Embed Size (px)
Citation preview

Postoperative Care of thePostoperative Care of the
Cardiac Surgical PatientCardiac Surgical Patient
Timothy A. Denton, M.D.
High Desert Heart Institute
Victorville, CA
Outline
• Overview of surgical patients• Cardiac Surgery Knowledge base• Intraop issues• Postop Issues• Systems of care
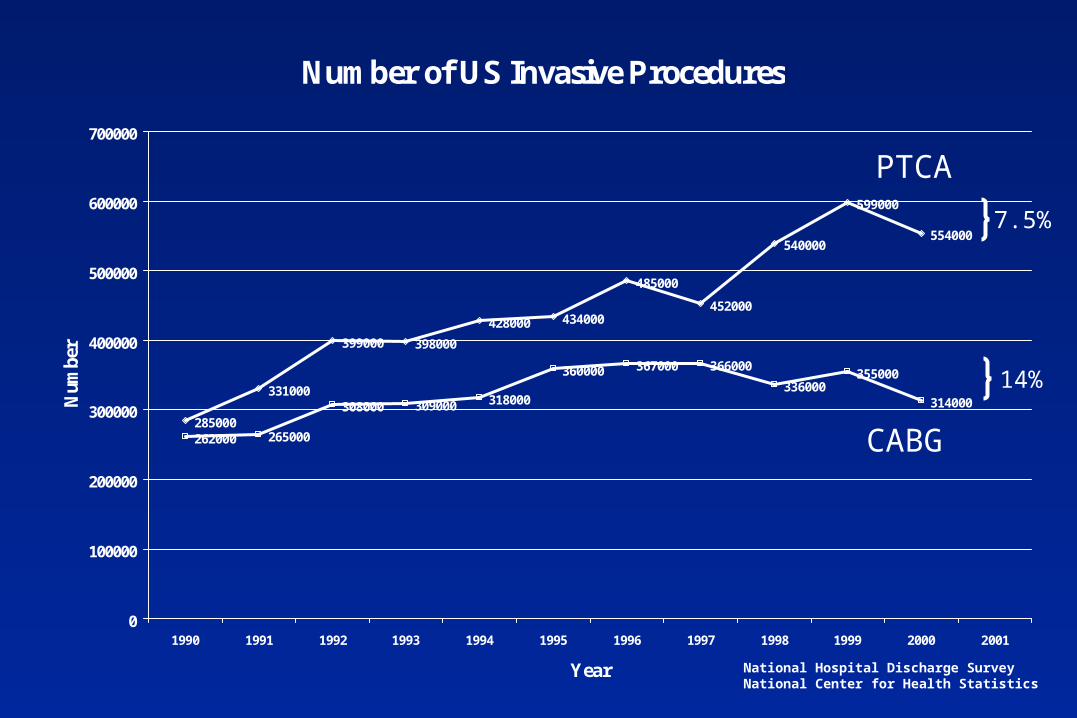
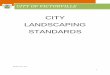
Number of US Invasive Procedures
285000
331000
399000 398000
428000 434000
485000
452000
540000
599000
554000
262000 265000
308000 309000 318000
360000 367000 366000
336000355000
314000
0
100000
200000
300000
400000
500000
600000
700000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Year
Num
ber
National Hospital Discharge SurveyNational Center for Health Statistics
CABG
PTCA
7.5%
14%

STS Rates of Cardiac Surgeries (2000)
CABG82%
Valve9%
CABG+Valve9%
CABG
Valve
CABG+Valve

CSMC Rates of Cardiac Surgeries (2001)
CABG47%
Valve25%
CABG+Valve28%
CABG
Valve
CABG+Valve
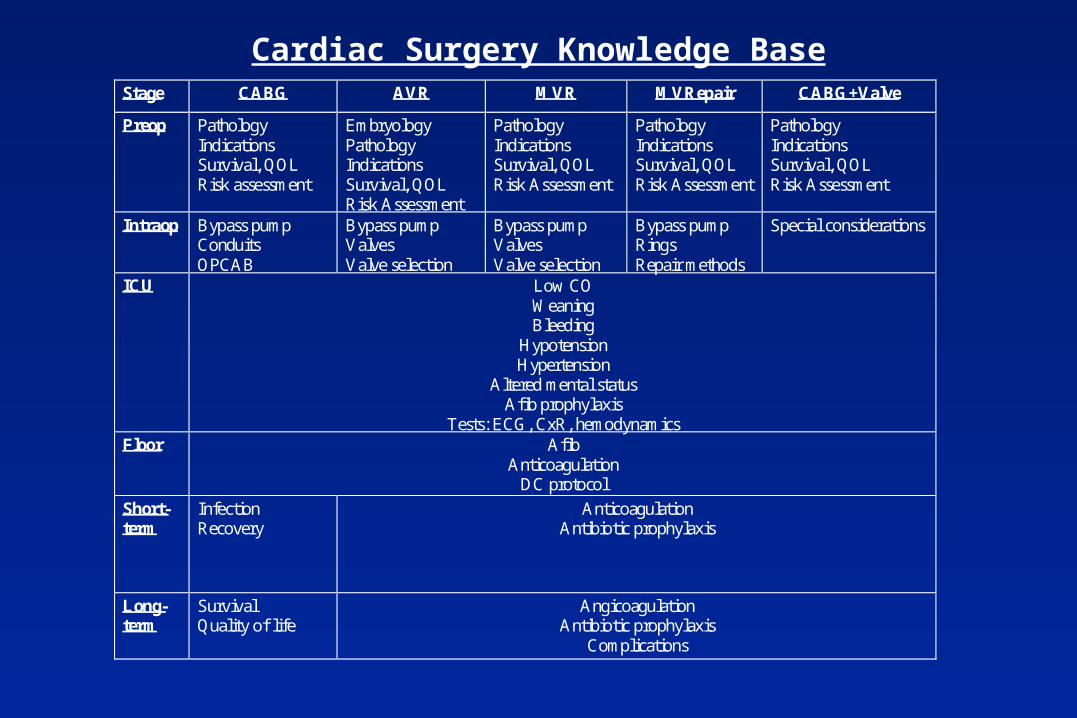
Cardiac Surgery Knowledge BaseStage CABG AVR MVR MVRepair CABG+Valve
Preop PathologyIndicationsSurvival, QOLRisk assessment
EmbryologyPathologyIndicationsSurvival, QOLRisk Assessment
PathologyIndicationsSurvival, QOLRisk Assessment
PathologyIndicationsSurvival, QOLRisk Assessment
PathologyIndicationsSurvival, QOLRisk Assessment
Intraop Bypass pumpConduitsOPCAB
Bypass pumpValvesValve selection
Bypass pumpValvesValve selection
Bypass pumpRingsRepair methods
Special considerations
ICU Low COWeaningBleeding
HypotensionHypertension
Altered mental statusAfib prophylaxis
Tests: ECG, CxR, hemodynamicsFloor Afib
AnticoagulationDC protocol
Short-term
InfectionRecovery
AnticoagulationAntibiotic prophylaxis
Long-term
SurvivalQuality of life
AngicoagulationAntibiotic prophylaxis
Complications

Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol

John Gibbon’s First Pump-Oxygenator
1935 - Cat bypass for 26 minutes
1953 - Cecelia Bavolek ASD repair
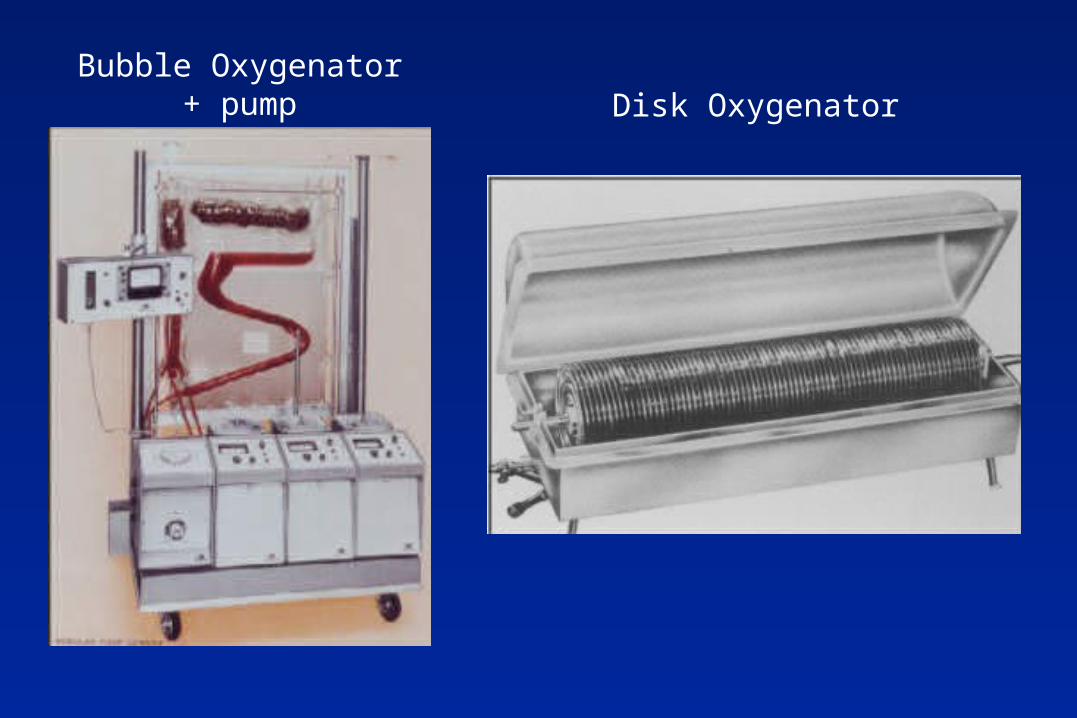
Disk OxygenatorBubble Oxygenator
+ pump
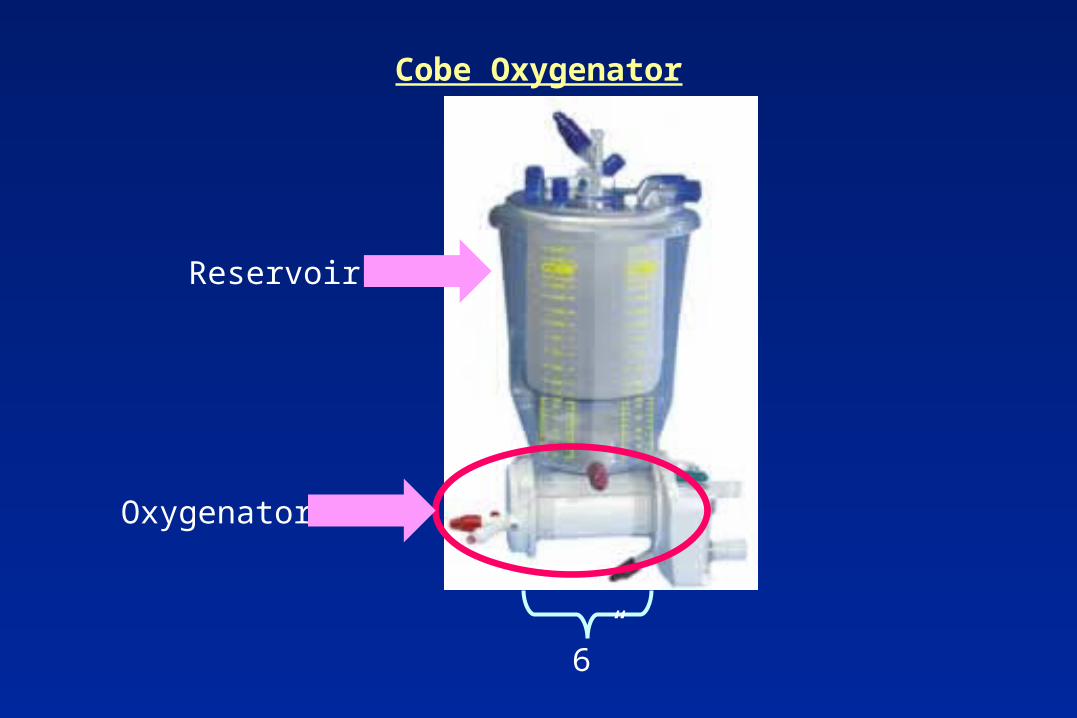
Cobe Oxygenator
Reservoir
Oxygenator
6”
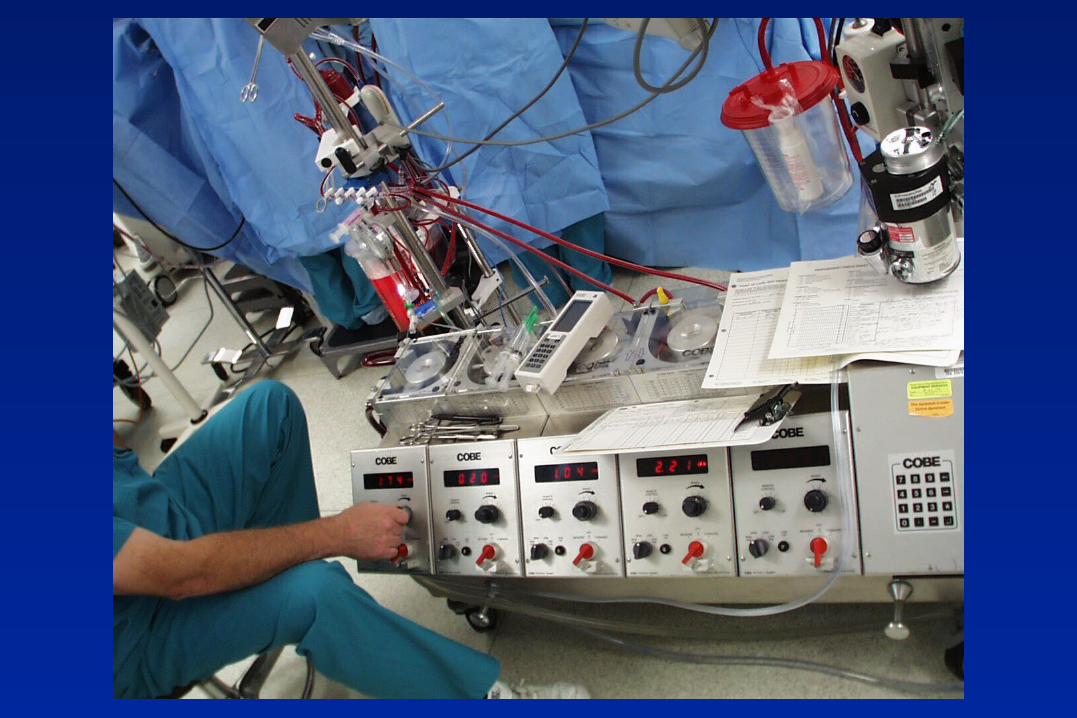

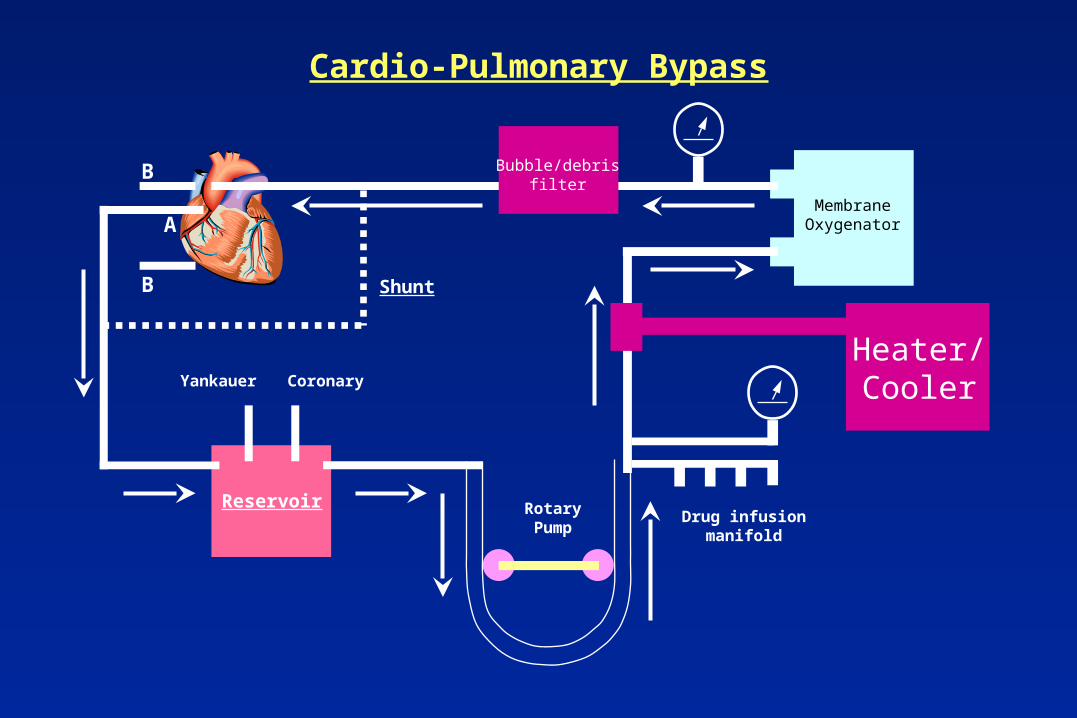
Cardio-Pulmonary Bypass
Reservoir
A
B
B
Heater/Cooler
Drug infusionmanifold
MembraneOxygenator
RotaryPump
Yankauer Coronary
Bubble/debrisfilter
Shunt
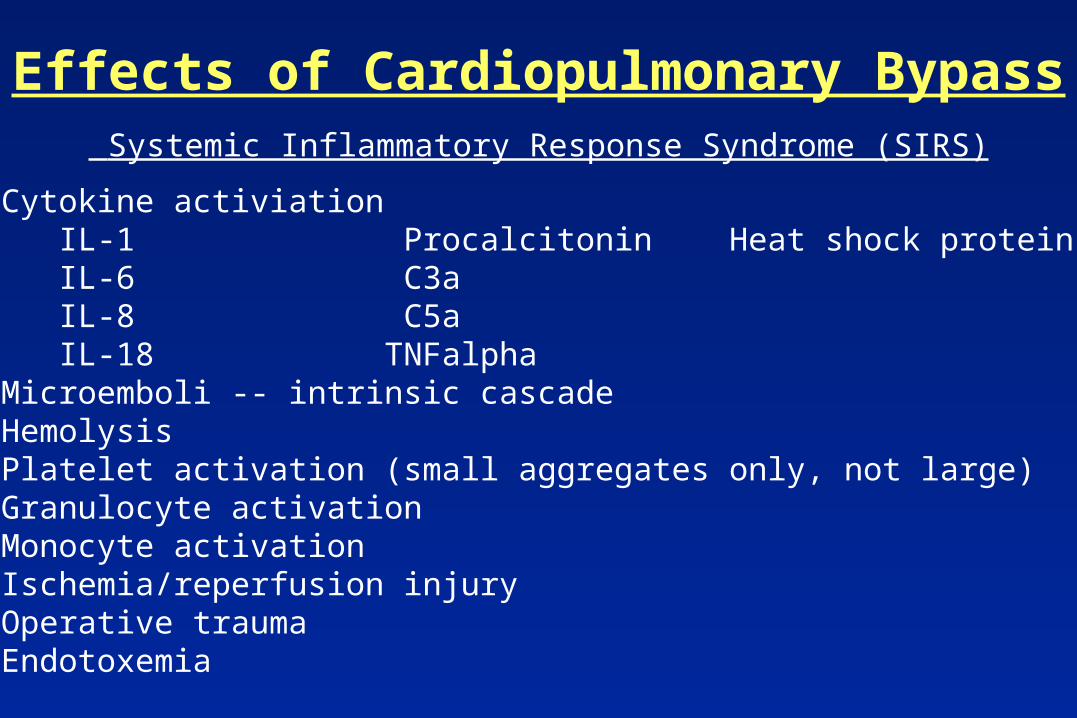
Effects of Cardiopulmonary Bypass
• Cytokine activiationIL-1 Procalcitonin Heat shock protein 70IL-6 C3aIL-8 C5aIL-18 TNFalpha
• Microemboli -- intrinsic cascade• Hemolysis• Platelet activation (small aggregates only, not large)• Granulocyte activation• Monocyte activation• Ischemia/reperfusion injury• Operative trauma• Endotoxemia
Systemic Inflammatory Response Syndrome (SIRS)
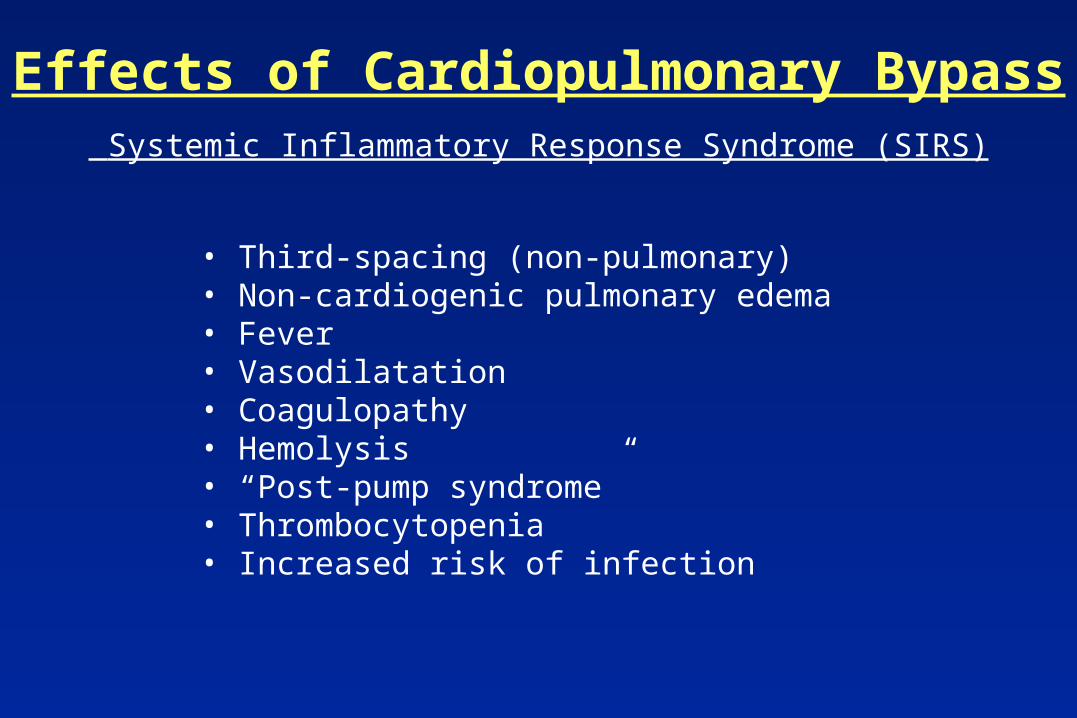
Effects of Cardiopulmonary Bypass
• Third-spacing (non-pulmonary)• Non-cardiogenic pulmonary edema• Fever• Vasodilatation• Coagulopathy• Hemolysis• “Post-pump syndrome”• Thrombocytopenia• Increased risk of infection
Systemic Inflammatory Response Syndrome (SIRS)
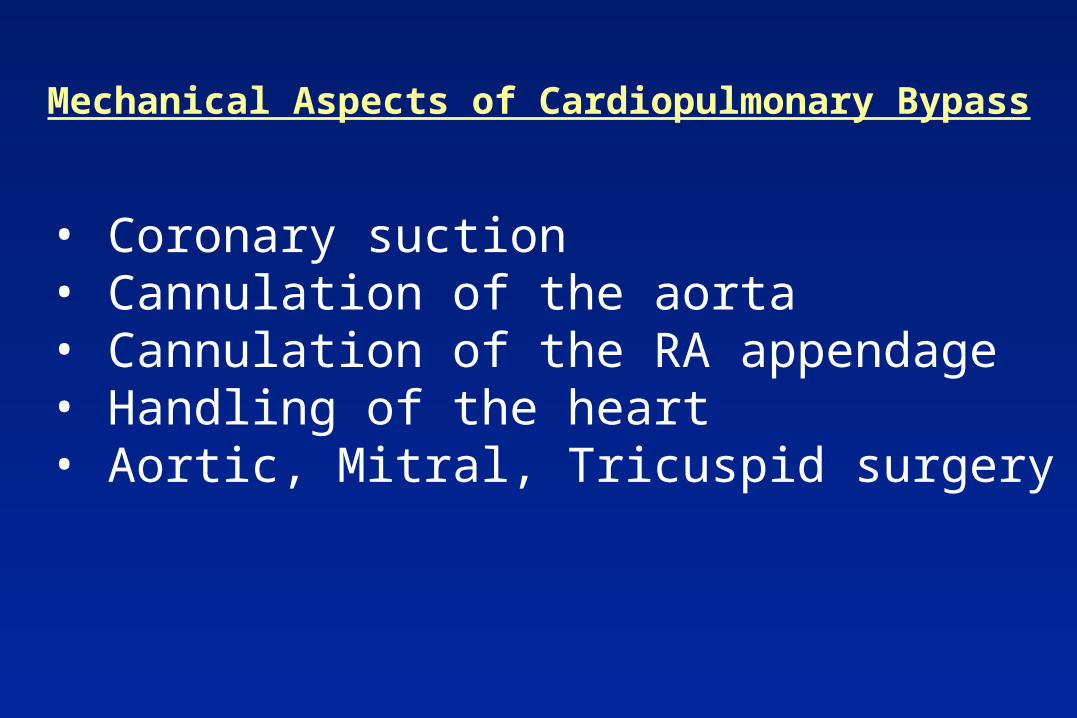
• Coronary suction• Cannulation of the aorta• Cannulation of the RA appendage• Handling of the heart• Aortic, Mitral, Tricuspid surgery
Mechanical Aspects of Cardiopulmonary Bypass
• Heparin• Anesthesia• Protamine
Chemical Effects of Cardiac Surgery
• Hypothermia
Other Effects of Cardiopulmonary Bypass
Off-Pump Coronary Bypass Surgery

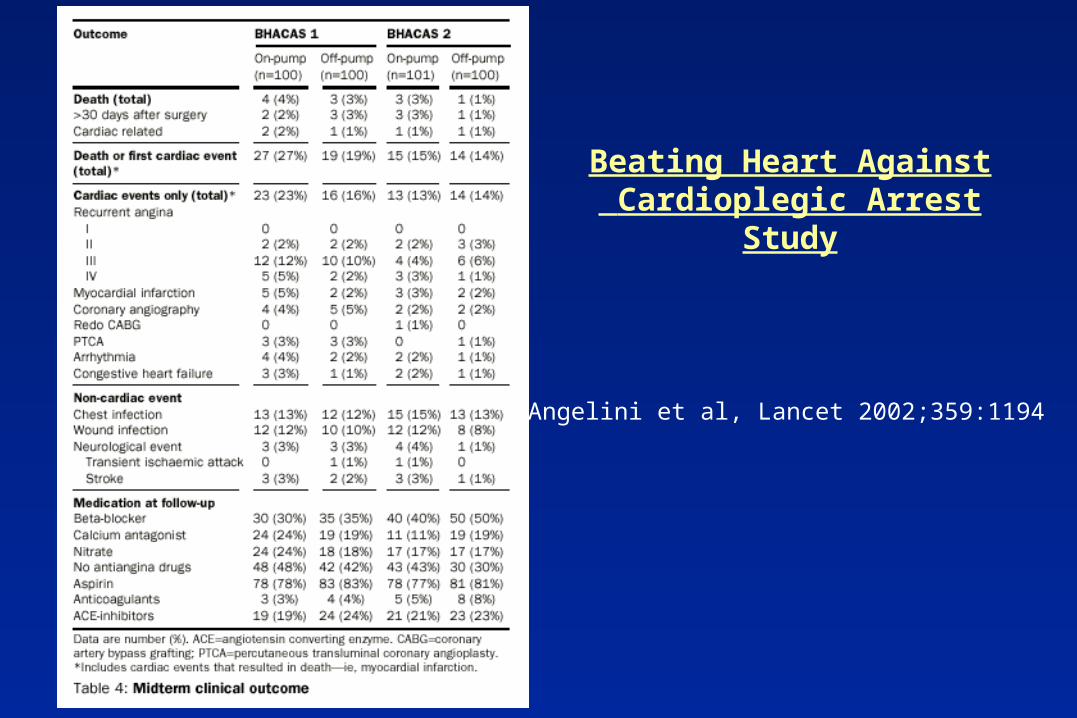
Beating Heart Against Cardioplegic Arrest Study
Angelini et al, Lancet 2002;359:1194
Beating Heart Against Cardioplegic Arrest Study
Angelini et al, Lancet 2002;359:1194
Minimally Invasive Cardiac Surgery
OPCABEasier recovery?Fewer complications?Cheaper?Good anastomoses?
Small ScarCosmesis
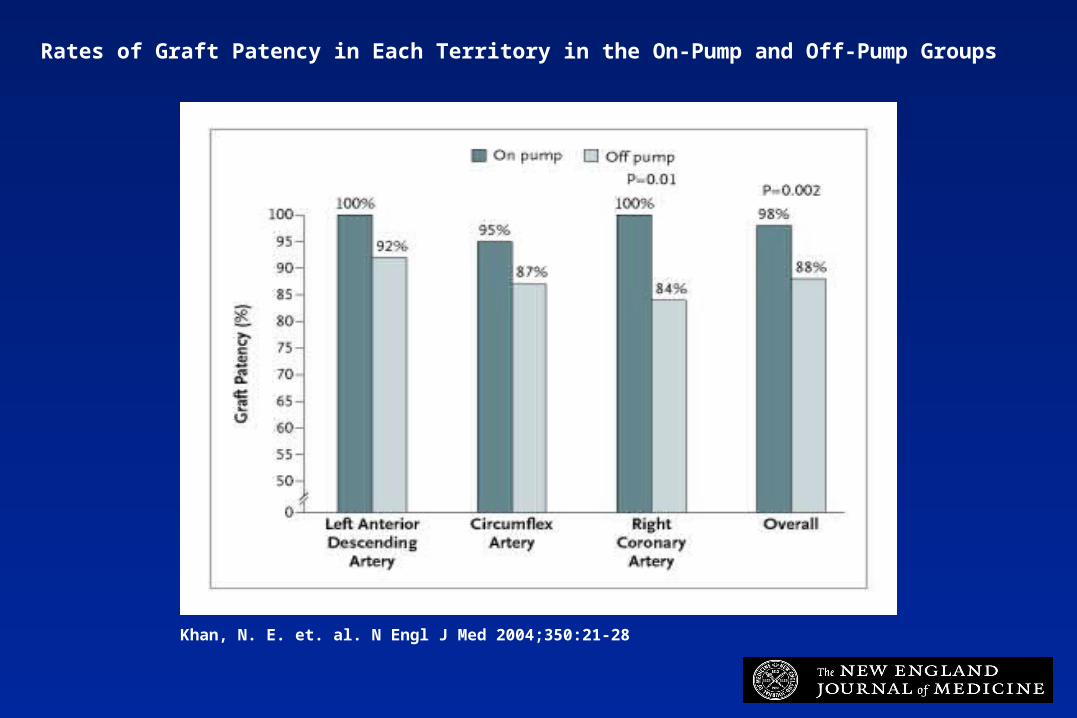
Khan, N. E. et. al. N Engl J Med 2004;350:21-28
Rates of Graft Patency in Each Territory in the On-Pump and Off-Pump Groups
Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol
Conduits• Saphenous vein• IMA• Radial• Artificial• Other
lesser saphenousarm veinsgastroepiploicinferior epigastric

Patency of Various Conduits
2-3 weekspost-op
Endo et al. Circulation 2001;104:2164
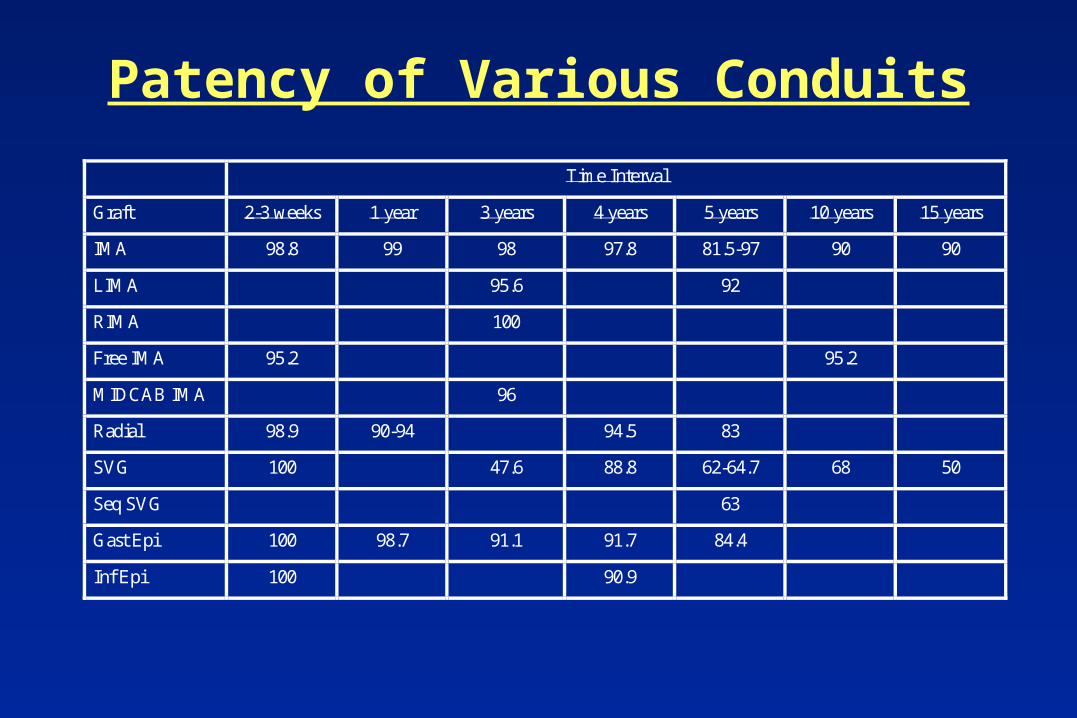
Patency of Various Conduits
Time Interval
Graft 2-3 weeks 1 year 3 years 4 years 5 years 10 years 15 years
IMA 98.8 99 98 97.8 81.5-97 90 90
LIMA 95.6 92
RIMA 100
Free IMA 95.2 95.2
MIDCAB IMA 96
Radial 98.9 90-94 94.5 83
SVG 100 47.6 88.8 62-64.7 68 50
Seq SVG 63
Gast Epi 100 98.7 91.1 91.7 84.4
Inf Epi 100 90.9

RA Background
•Long-term patency from 83-96%•Radial artery used in 50% of all CABG’s
at CSMC•Anecdotal complaints of sensory abnormalities
and rare complaints of hand weakness
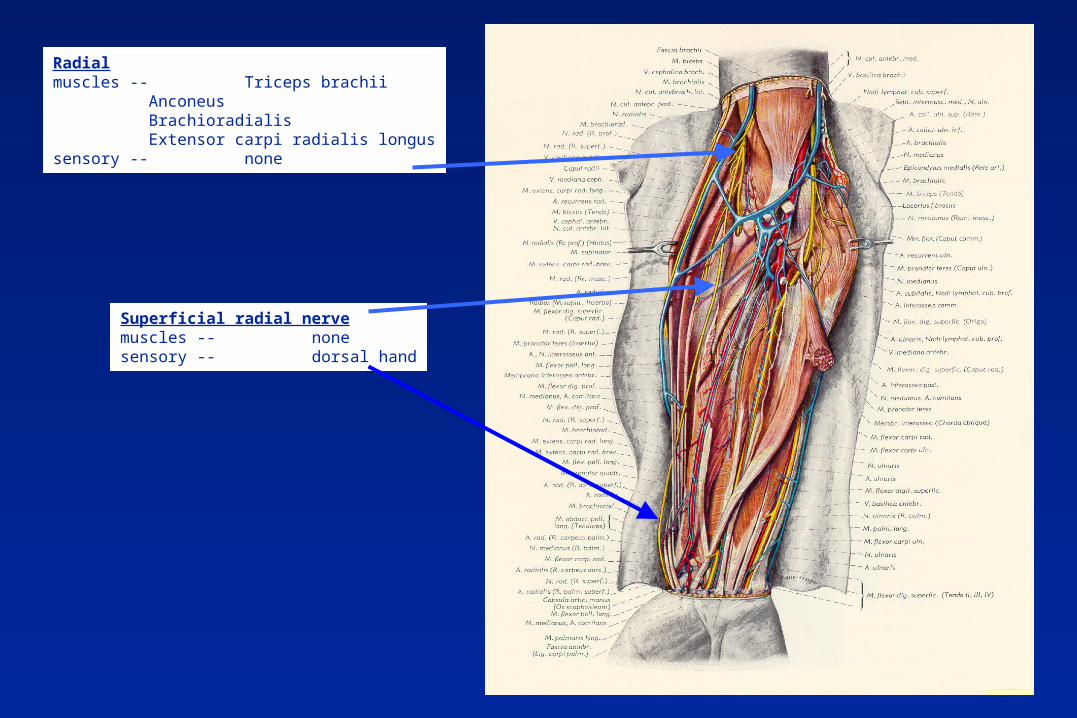
Radialmuscles -- Triceps brachii
AnconeusBrachioradialisExtensor carpi radialis longus
sensory -- none
Superficial radial nervemuscles -- nonesensory -- dorsal hand

Path ofRadial Nerve
in the Forearm
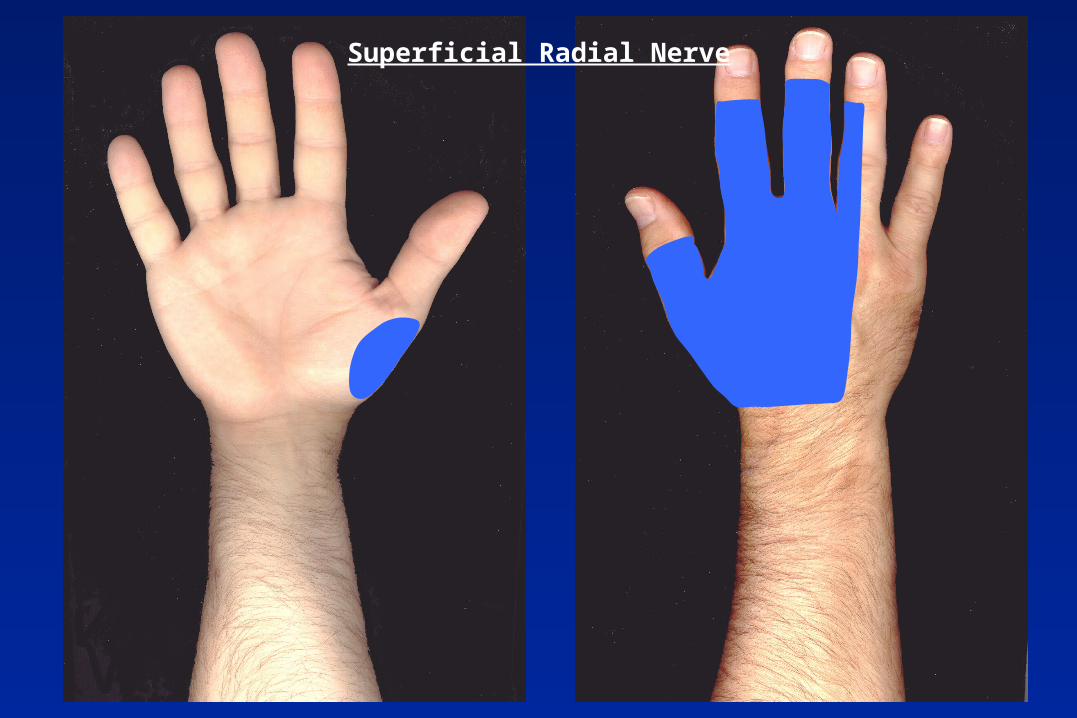
Superficial Radial Nerve
Patient Population
•2/20/96 to 12/31/99•All patients with radial arteries•Compared to patients without
radial arteries over sametime period.

Results
Symptom N/total ProportionAny abnormality 169/560 30.1%Thumb strength 31/559 5.5%Sensation abnormality Dorsum Palm
101/55977/55971/559
18.1%13.8%12.7%
Other Abnormality 43/558 6.3%Improvement 101/560 18.0%
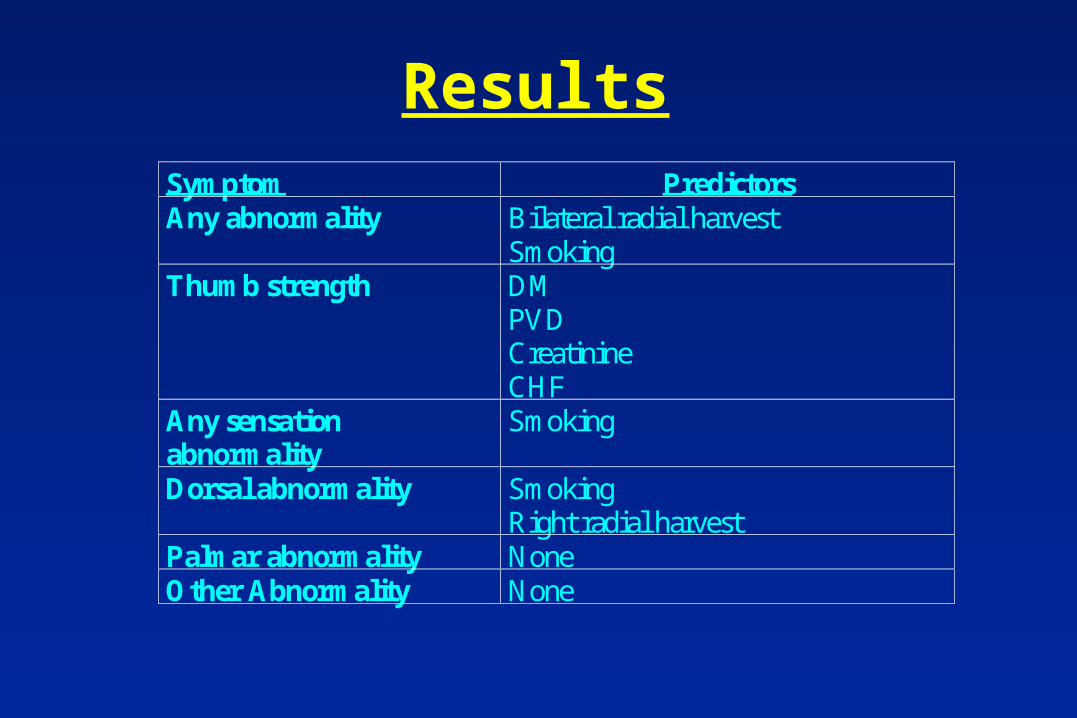
ResultsSymptom PredictorsAny abnormality Bilateral radial harvest
SmokingThumb strength DM
PVDCreatinineCHF
Any sensationabnormality
Smoking
Dorsal abnormality SmokingRight radial harvest
Palmar abnormality NoneOther Abnormality None
Problems
•Usually, thumb strength complaintsvia Flexor pollicus longusMOTOR MEDIAN NERVE
•Most palmar sensation abnormalitiesSENSORY MEDIAN NERVE

Results
Sensory AbnormalityLocation
ThumbWeakness
No ThumbWeakness
P value
Palmar Only 16.1% (5/31) 3.8% (20/528) 0.003Dorsal Only 6.5% (2/31) 5.6% (29/528) 0.97Both Palmar and Dorsal 35.5% (11/31) 6.6% (35/528) <0.001
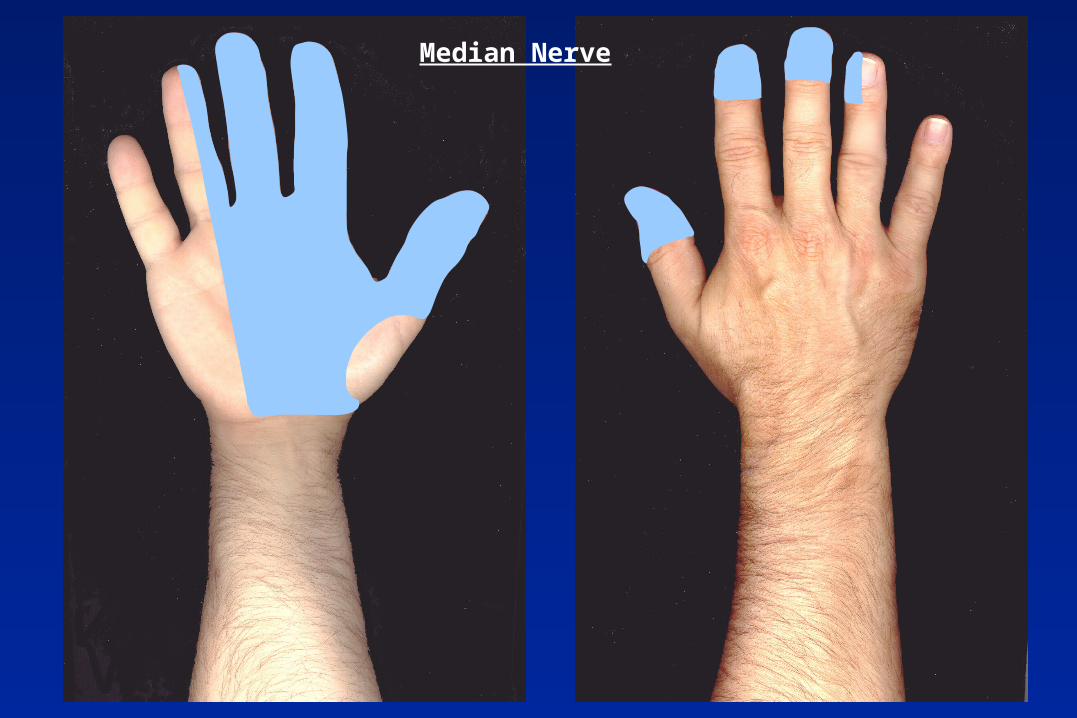
Median Nerve
Problems
Data support median nerve damage
• Palmar abnormalities• Thumb weakness• Statistical associations
What is the mechanism of median damage?
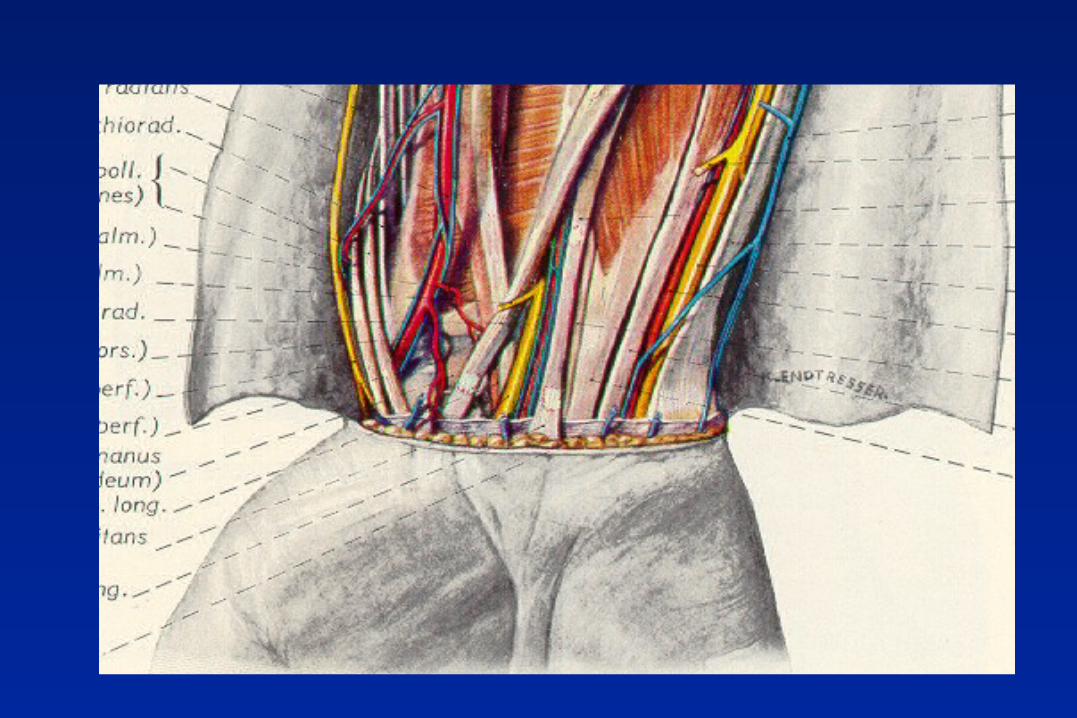
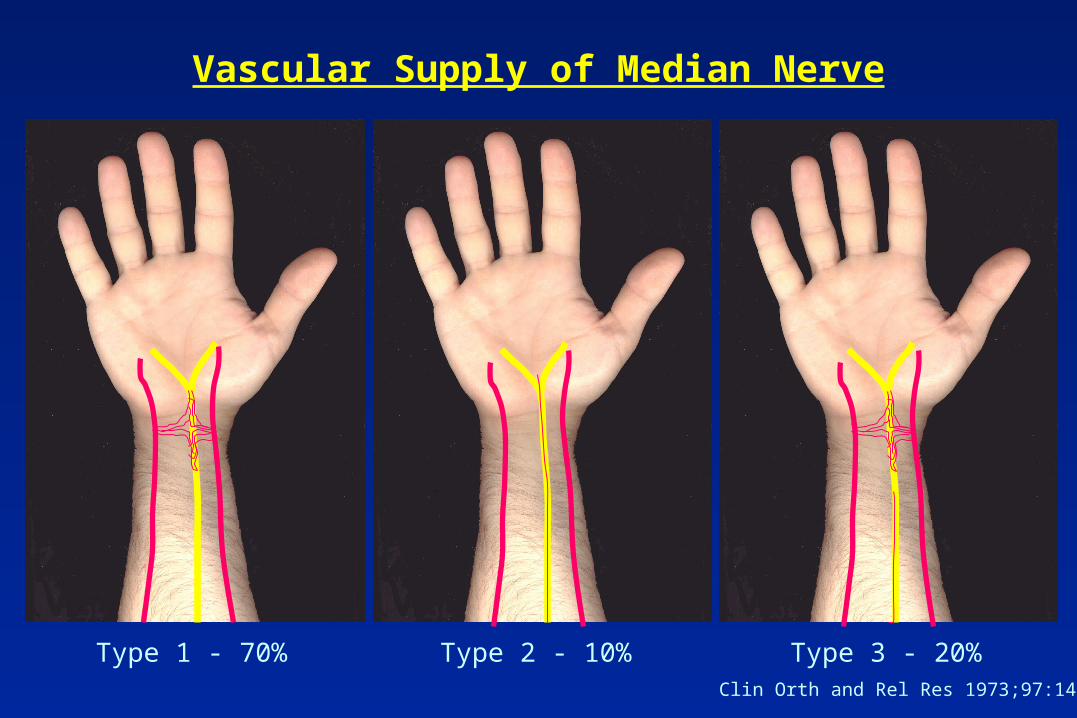
Vascular Supply of Median Nerve
Type 1 - 70% Type 2 - 10% Type 3 - 20%Clin Orth and Rel Res 1973;97:144

Summary
•Clear evidence for radial nerve damage•Clear evidence for median nerve damage•Vascular disease contribution to damage
Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol

What is this?
RA = 20
PAD = 24
No Y descent
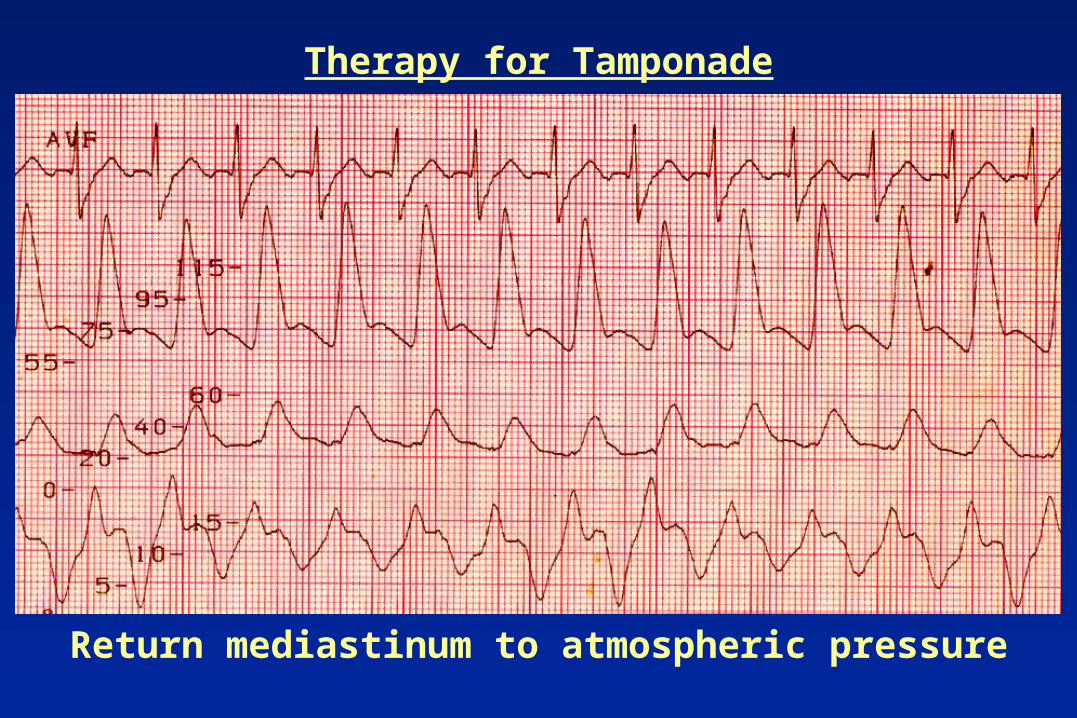
Therapy for Tamponade
Return mediastinum to atmospheric pressure

Differential Diagnosis ofLow Cardiac Output/Hypotension
• Tamponade• Tamponade• Tamponade• Tamponade• Hypovolemia• LV dysfunction / infarction• Hemorrhage
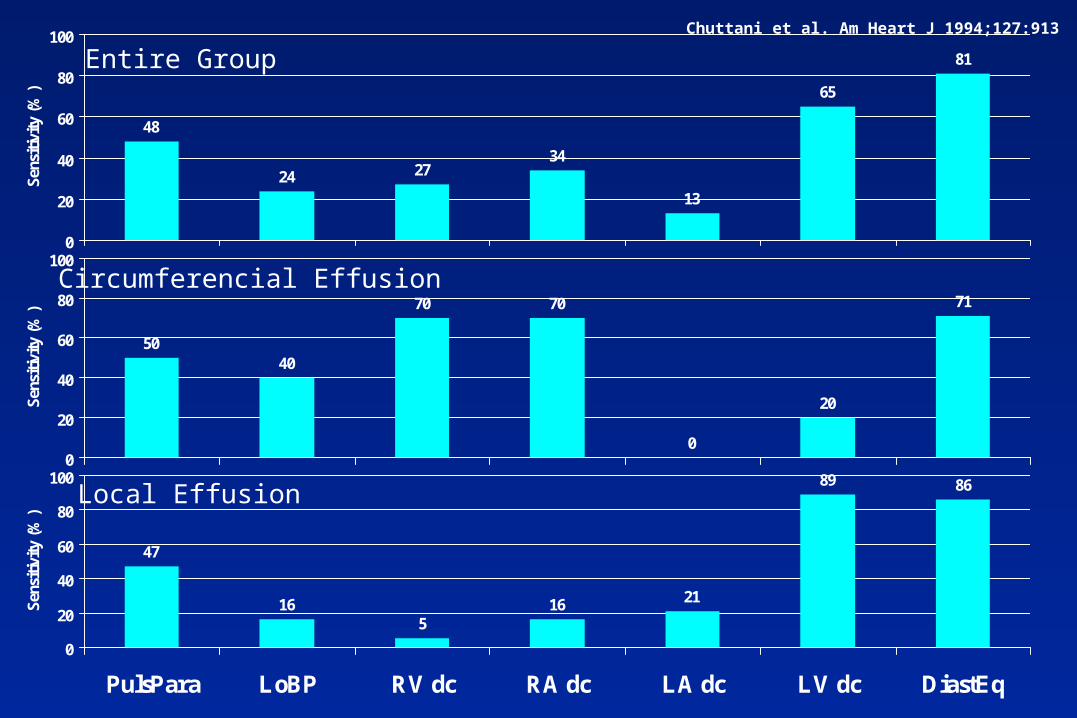
Chuttani et al. Am Heart J 1994;127:913
48
24 2734
13
65
81
0
20
40
60
80
100S
ensi
tivi
ty (
%)
5040
70 70
0
20
71
0
20
40
60
80
100
Sen
siti
vity
(%
)
47
165
16 21
89 86
0
20
40
60
80
100
PulsPara LoBP RV dc RA dc LA dc LV dc DiastEq
Sen
siti
vity
(%
)
Entire Group
Circumferencial Effusion
Local Effusion
Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol
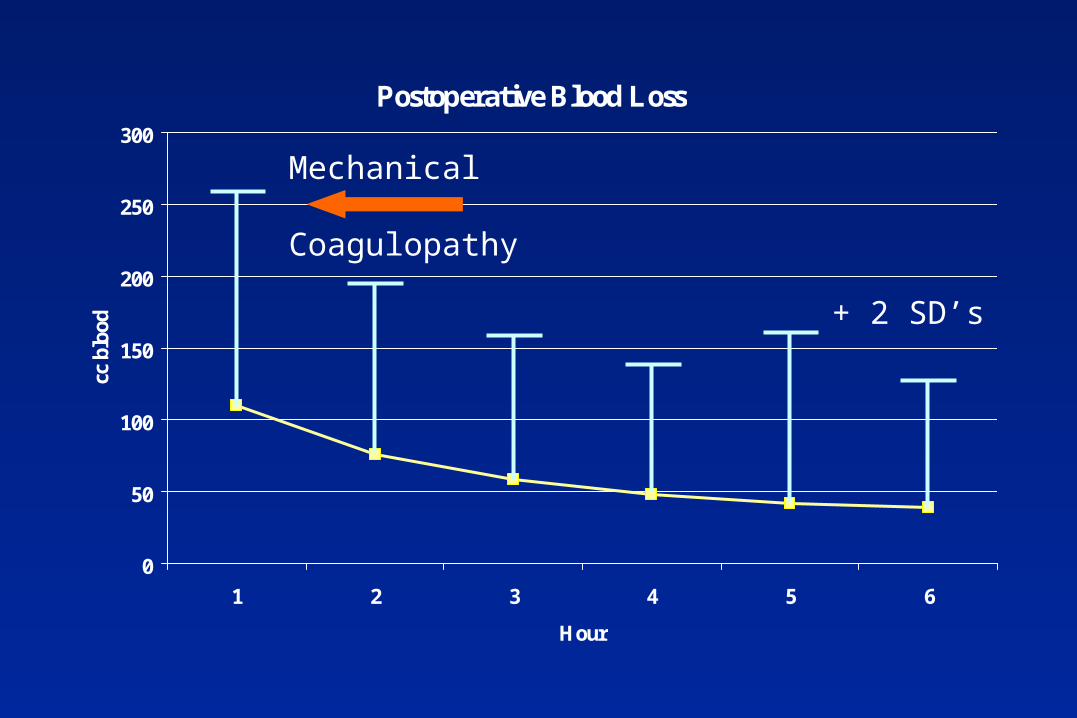
Postoperative Blood Loss
0
50
100
150
200
250
300
1 2 3 4 5 6
Hour
cc b
lood + 2 SD’s
Mechanical
Coagulopathy
Etiology
• Mechanical• Coagulopathy
HeparinCoumadinAntiplatelet agentsTemperatureLow platelet count (rare)Poor platelet function
Therapy
• MechanicalReturn to surgery
• CoagulopathyCorrect PT (FFP 2 or more units)Correct PTT (Protamine 20-40 mg)Correct PFA (DDAVP 20-40 units)Correct Platelet count (platelets)Empiric therapy
Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol
Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol

Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol
Cardiac Arrhythmias following PneumonectomyNEJM 1943;229:356-359
•When was cardiac surgery started?•When was bypass started?•When was ECG monitoring started?
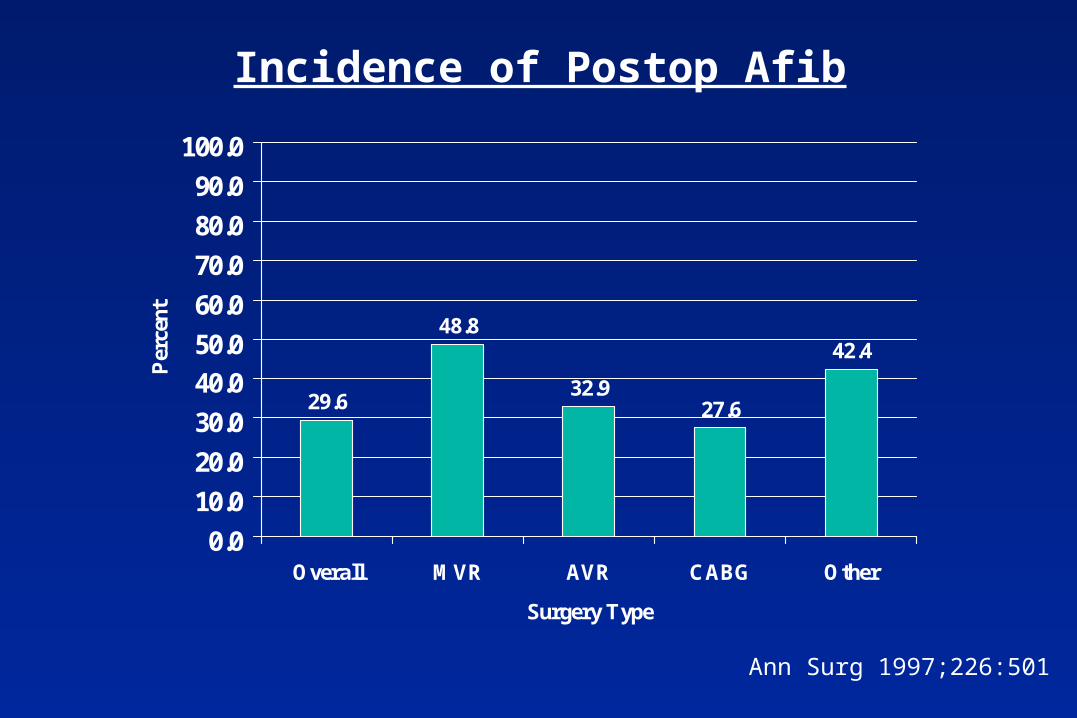
Incidence of Postop Afib
Ann Surg 1997;226:501
29.6
48.8
32.927.6
42.4
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Overall MVR AVR CABG Other
Surgery Type
Per
cent
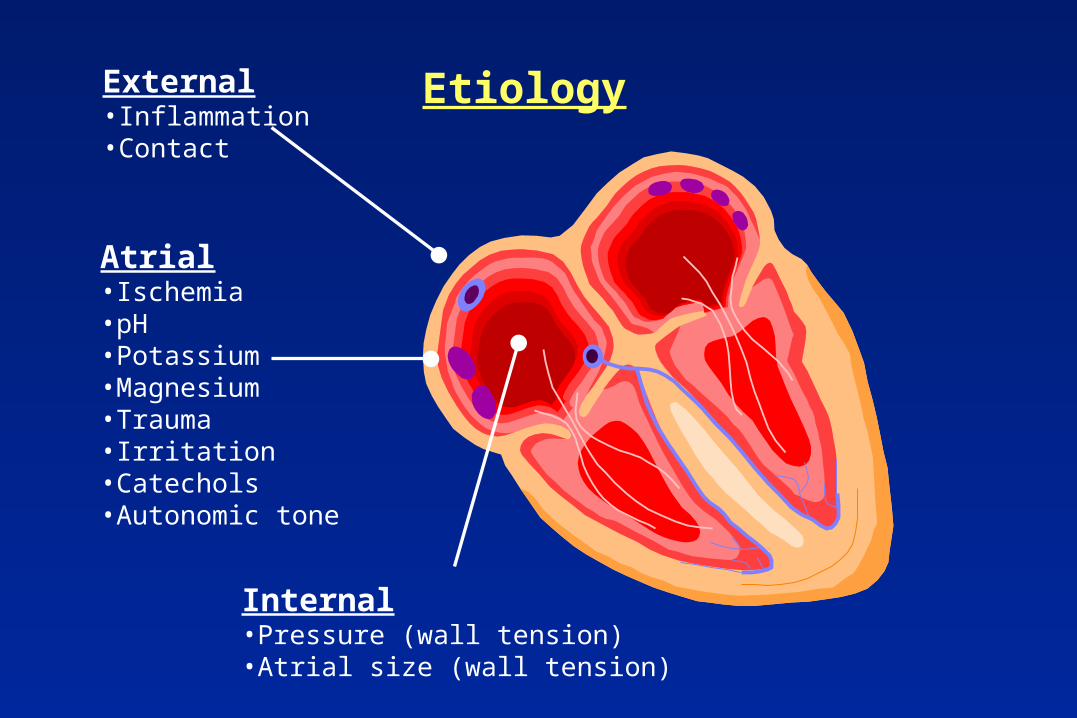
EtiologyExternal•Inflammation•Contact
Internal•Pressure (wall tension)•Atrial size (wall tension)
Atrial•Ischemia•pH•Potassium•Magnesium•Trauma•Irritation•Catechols•Autonomic tone

J Thor CV Surg 1990;100:338
Predictors of Postop Afib
•Age•COPD•Preop beta blocker (+)•CRF
Rate of Afib per Decade
0102030405060708090
100
<40 40-49 50-59 60-69 >70
Decade
Per
cen
t
JAMA 1996;276:300
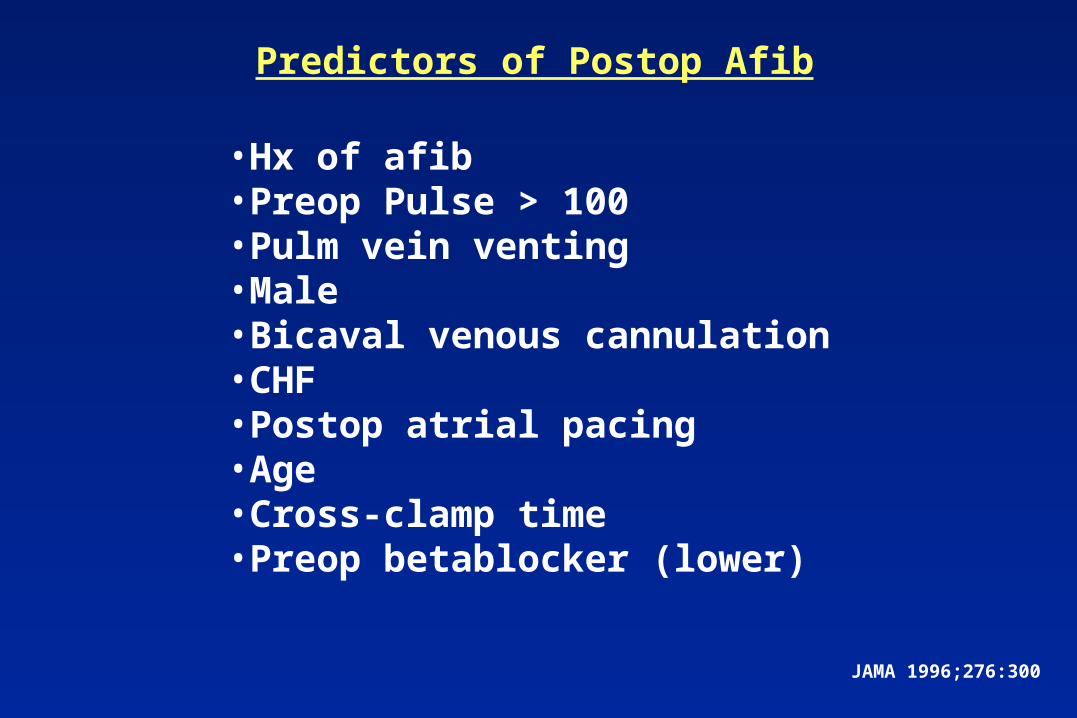
Predictors of Postop Afib
•Hx of afib•Preop Pulse > 100•Pulm vein venting•Male•Bicaval venous cannulation•CHF•Postop atrial pacing•Age•Cross-clamp time•Preop betablocker (lower)

Circ 1996;94:390
Predictors of Postop Afib
•Age•Male•HTN•IABP•Pneumonia•Prolonged ventilation•Return to ICU

Ann Thor Surg 1999;68:931-933
Does the Pump cause Afib?
•Retrospective•CABG (n=685)•Minimally invasive CABG (n=19)•TMLR (n=19)
36 37
5
0
10
20
30
40
50
60
70
80
90
100
CABG Off-Pump TMLR
Pos
t A
fib
Rat
e (%
)
P<0.01

J Thor CV Surg 1999;117:298
Does the Pump cause Afib?
•Retrospective•55 Off-pump vs control cohort
34
26
0
10
20
30
40
50
60
70
80
90
100
CABG Off-Pump
Pos
t A
fib
Rat
e (%
)
P=NS

Preventthe
Rhythm
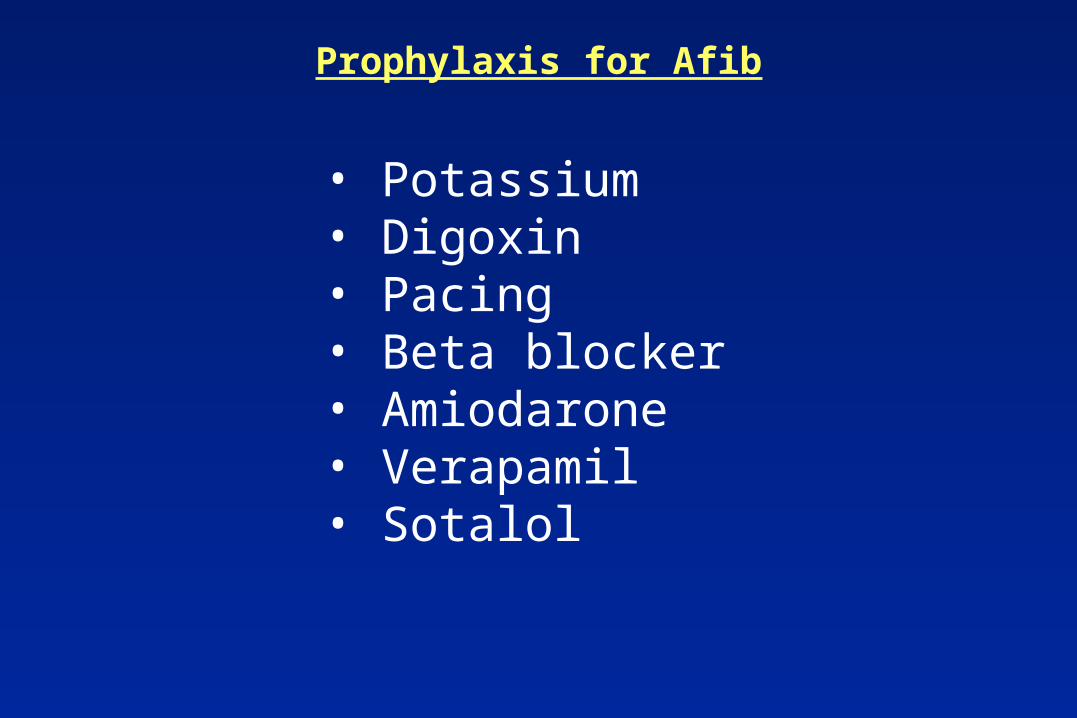
Prophylaxis for Afib
• Potassium• Digoxin• Pacing• Beta blocker• Amiodarone• Verapamil• Sotalol
Prog CV Dis 1989;31:367
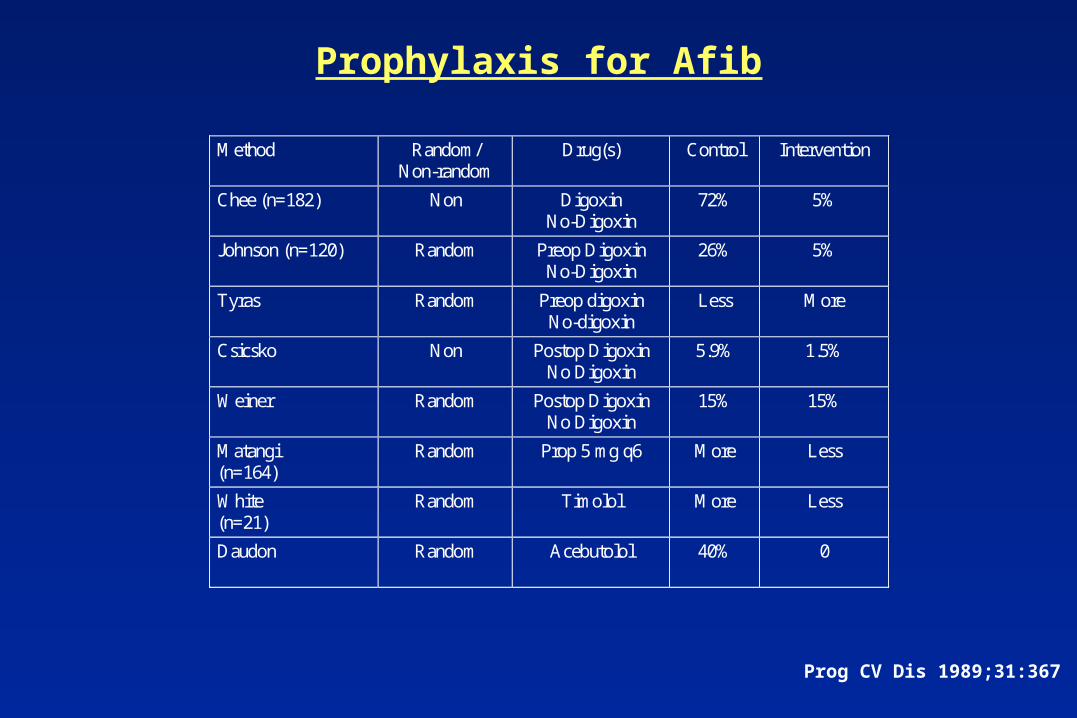
Prophylaxis for Afib
Method Random/Non-random
Drug(s) Control Intervention
Chee (n=182) Non DigoxinNo-Digoxin
72% 5%
Johnson (n=120) Random Preop DigoxinNo-Digoxin
26% 5%
Tyras Random Preop digoxinNo-digoxin
Less More
Csicsko Non Postop DigoxinNo Digoxin
5.9% 1.5%
Weiner Random Postop DigoxinNo Digoxin
15% 15%
Matangi(n=164)
Random Prop 5 mg q6 More Less
White(n=21)
Random Timolol More Less
Daudon Random Acebutolol 40% 0
Ann Thor Surg 1981;31:496
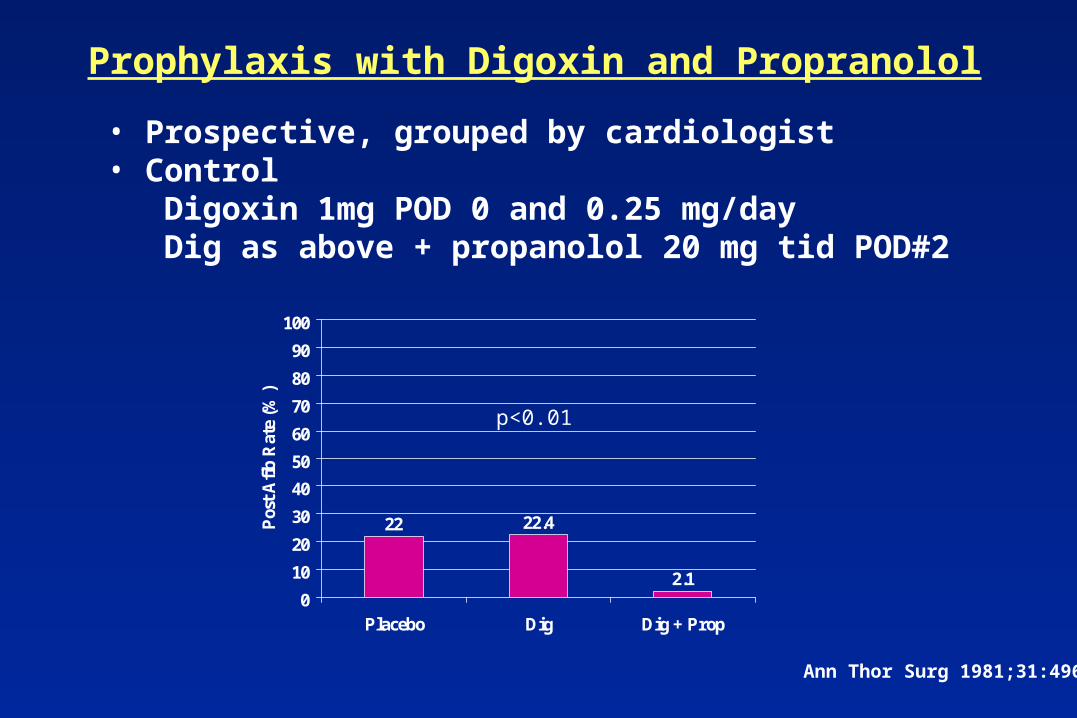
Prophylaxis with Digoxin and Propranolol
• Prospective, grouped by cardiologist• Control Digoxin 1mg POD 0 and 0.25 mg/day Dig as above + propanolol 20 mg tid POD#2
22 22.4
2.10
10
20
30
40
50
60
70
80
90
100
Placebo Dig Dig + Prop
Pos
t A
fib
Rat
e (%
)
p<0.01

Am Heart J 1999;138:144
Amiodarone for Postop Afib Prophylaxis•Randomized, double-blind•Amiodarone 2 grams over 4 days preop
then continued for 7 days Placebo•CABG only
32.8
24.7
0
10
20
30
40
50
60
70
80
90
100
Placebo Amio
Pos
t A
fib
Rat
e (%
)
p=0.3
NEJM 1998;337:1785
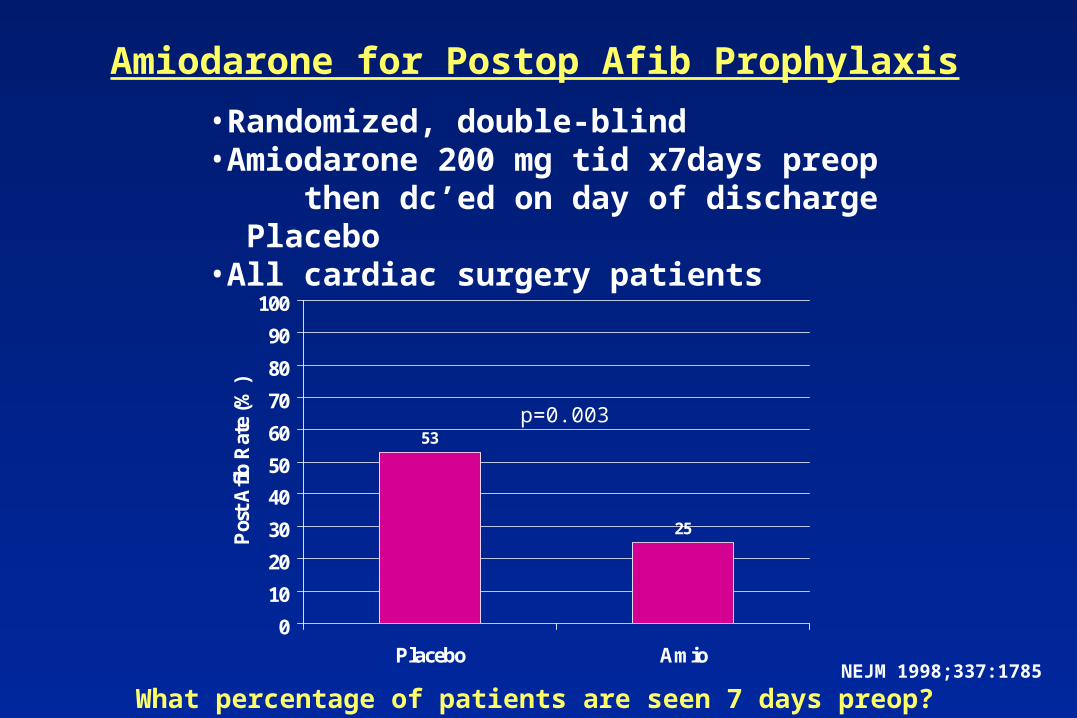
Amiodarone for Postop Afib Prophylaxis
•Randomized, double-blind•Amiodarone 200 mg tid x7days preop
then dc’ed on day of discharge Placebo•All cardiac surgery patients
53
25
0
10
20
30
40
50
60
70
80
90
100
Placebo Amio
Pos
t A
fib
Rat
e (%
)
p=0.003
What percentage of patients are seen 7 days preop?
JACC 1999;33:1981
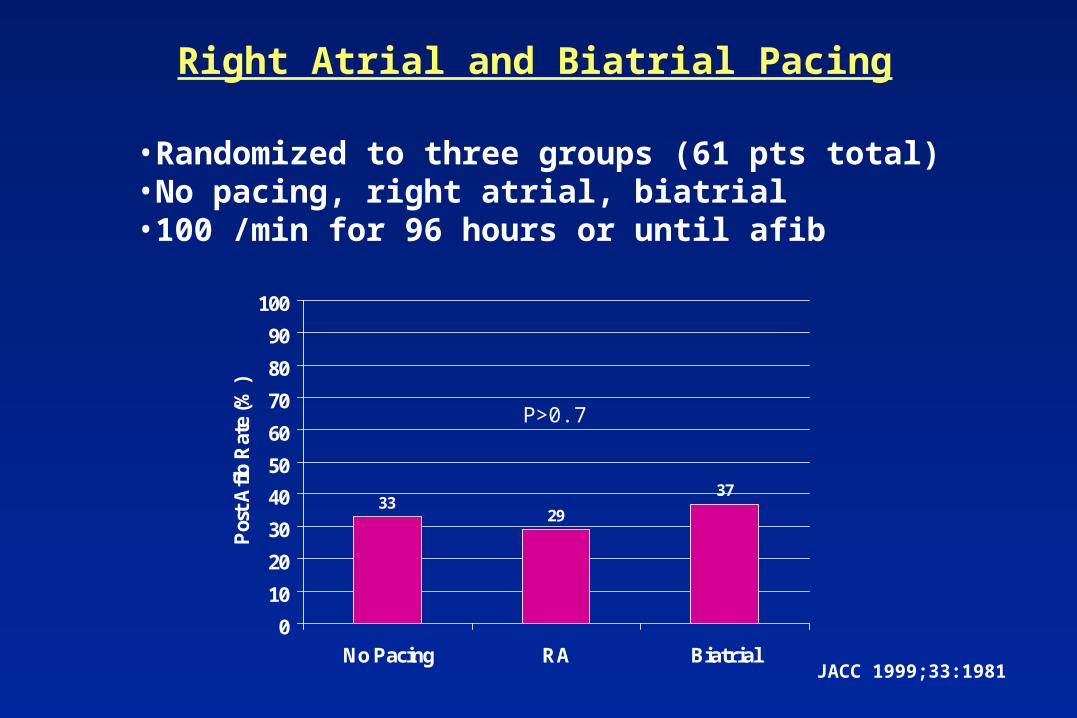
Right Atrial and Biatrial Pacing
•Randomized to three groups (61 pts total)•No pacing, right atrial, biatrial•100 /min for 96 hours or until afib
3329
37
0
10
20
30
40
50
60
70
80
90
100
No Pacing RA Biatrial
Pos
t A
fib
Rat
e (%
)
P>0.7

Ann Thor Surg 1985;39:336
Prophylaxis with Verapamil
•Double-blind, randomized•Verapamil 80 mg q6h vs placebo•Observed 7 days for afib•13% hypotension on verapamil
23
14
0
10
20
30
40
50
60
70
80
90
100
Placebo Verapamil
Pos
t A
fib
Rat
e (%
)
P=0.1
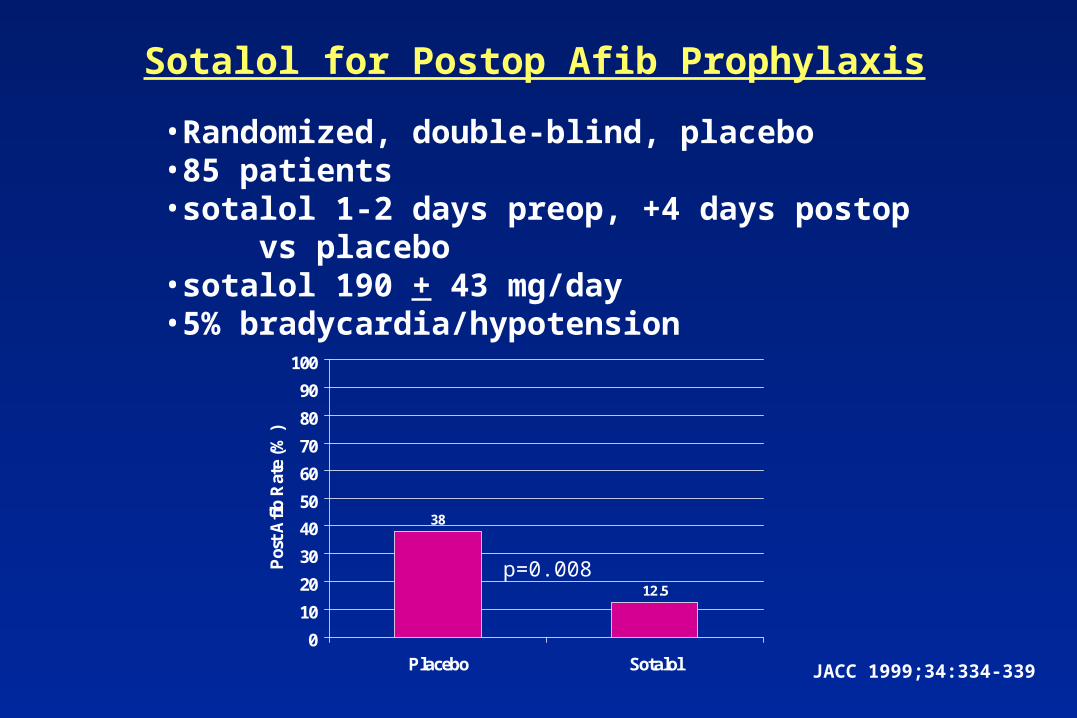
JACC 1999;34:334-339
Sotalol for Postop Afib Prophylaxis
•Randomized, double-blind, placebo•85 patients•sotalol 1-2 days preop, +4 days postop vs placebo•sotalol 190 + 43 mg/day•5% bradycardia/hypotension
38
12.5
0
10
20
30
40
50
60
70
80
90
100
Placebo Sotalol
Pos
t A
fib
Rat
e (%
)
p=0.008

Effect of Sot and Mag on Postop Afib
38
1412
2
0
10
20
30
40
50
60
70
80
90
100
Control Mag Sot Mag+Sot
Per
cent
Forlani S, et al. STS 38th Annual Meeting, 2001
Controlthe
AV node
Treatment of Postop Afib
Control the AV Node
• Beta blocker• Calcium channel blocker• Digoxin
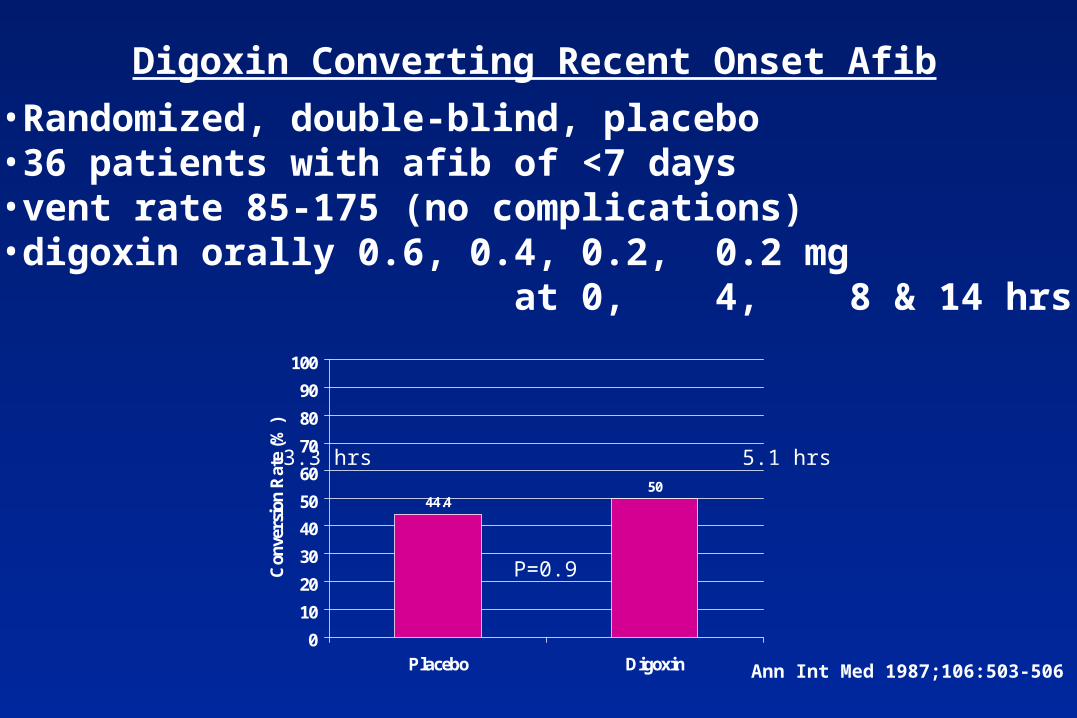
Ann Int Med 1987;106:503-506
Digoxin Converting Recent Onset Afib
•Randomized, double-blind, placebo•36 patients with afib of <7 days•vent rate 85-175 (no complications)•digoxin orally 0.6, 0.4, 0.2, 0.2 mg at 0, 4, 8 & 14 hrs
44.450
0
10
20
30
40
50
60
70
80
90
100
Placebo Digoxin
Con
vers
ion
Rat
e (%
)
3.3 hrs 5.1 hrs
P=0.9

Rate Control Therapy
Can J Cardiol 1998;14:1363-1366
•Observational study•59 patients post-CABG•Rate control with dig/verapamil•follow-up at 2-4 weeks•55/59 patients in NSR (93.2%)
Convertthe
Rhythm

Convert the Rhythm
• Electrical• Pharmacologic
procainamideamiodaronepropafenonesotalolibutilide

AJC 1999;84:345
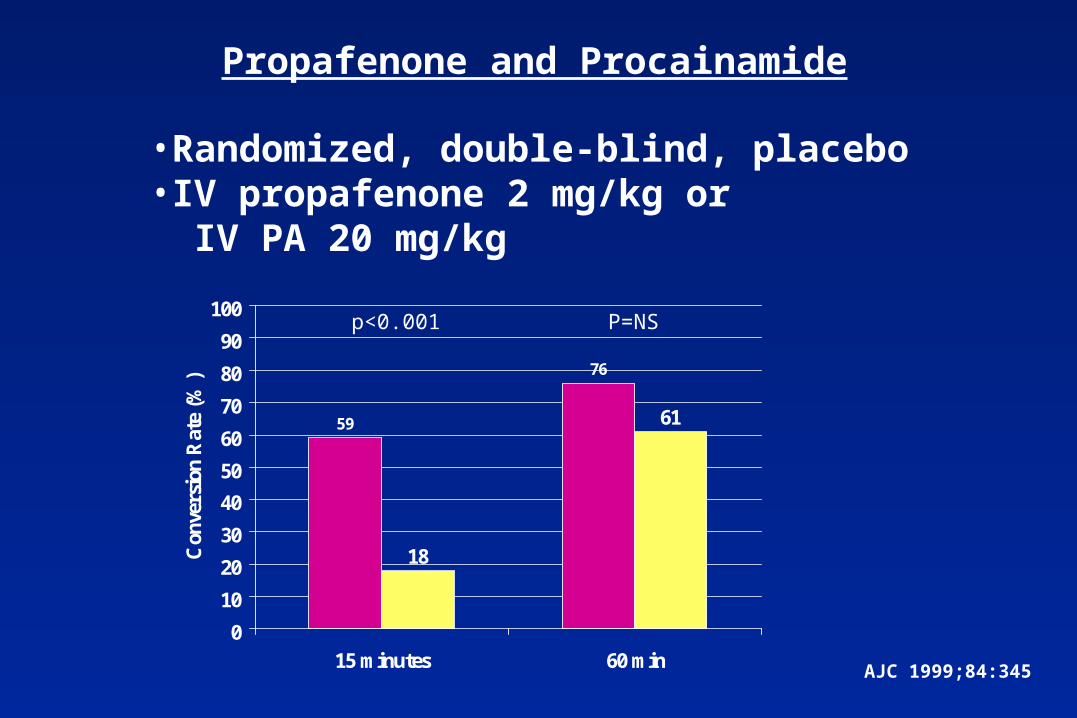
Propafenone and Procainamide
•Randomized, double-blind, placebo•IV propafenone 2 mg/kg or IV PA 20 mg/kg
59
76
18
61
0
10
20
30
40
50
60
70
80
90
100
15 minutes 60 min
Con
vers
ion
Rat
e (%
)
p<0.001 P=NS
Circ 1999;100:369
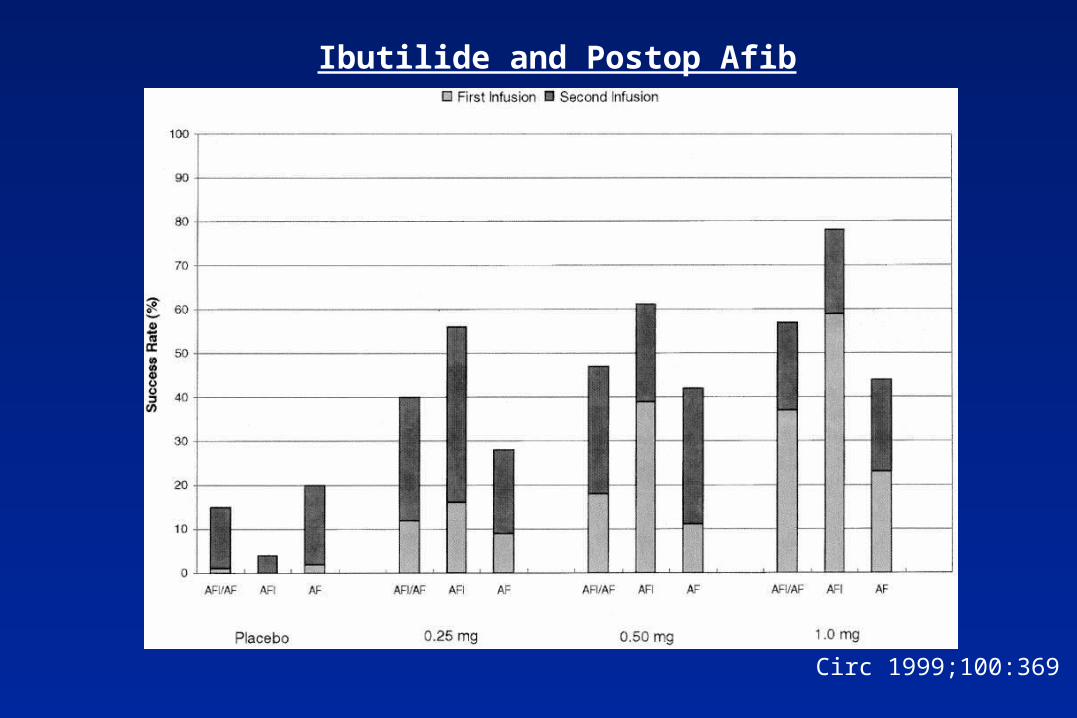
Ibutilide and Postop Afib
Ibutilide in Postop Afib
Circ 1999;100:369
•4 / 218 torsades (1.8%)•all in 1 mg group (5.6%)•3/4 had low EF
Our experience = 3 / 5 with torsades / VF
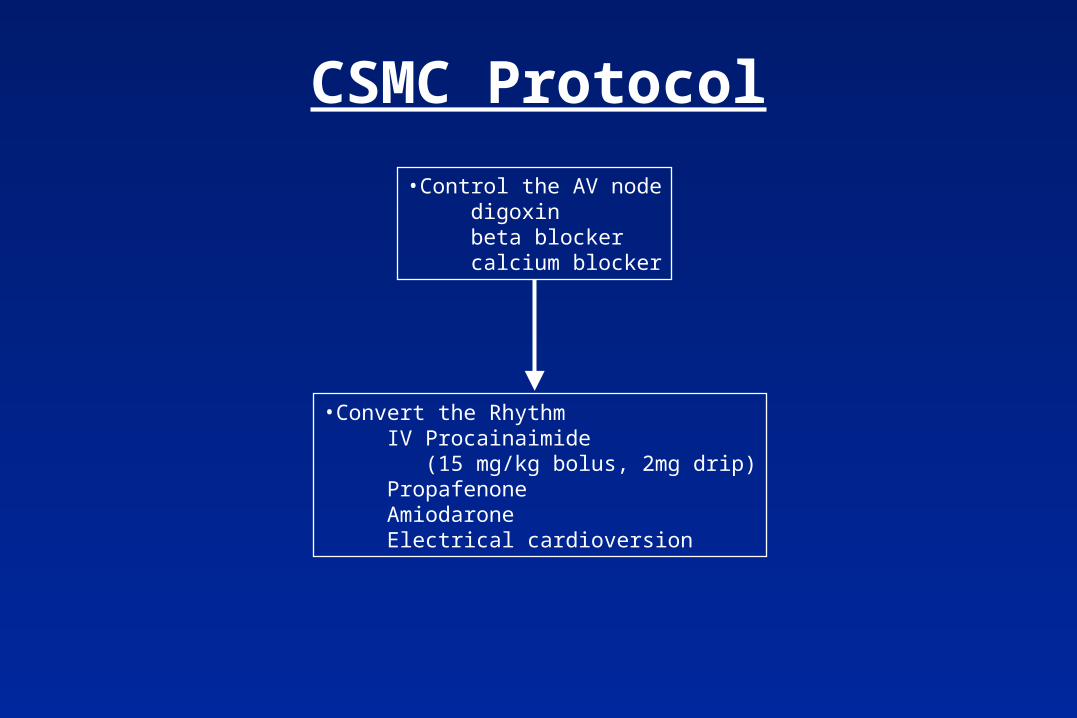
CSMC Protocol
•Control the AV node digoxin beta blocker calcium blocker
•Convert the Rhythm IV Procainaimide (15 mg/kg bolus, 2mg drip) Propafenone Amiodarone Electrical cardioversion

Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol
Anticoagulation
• Bioprosthetic valves/Ring RepairsINR = 2.0 for 12 weeks (unless contraindicated)“no rush” to INR of 2.0
• Mechanical valvesStart coumadin POD #3Pt leaves hospital at INR ~ 1.7Goal INR = 3.5
Outline
• Pump -- Off-pump• Conduits• Low cardiac output• Hypotension• Bleeding• Hypertension• Altered mental status• Afib prophylaxis -- afib• Anticoagulation• DC protocol
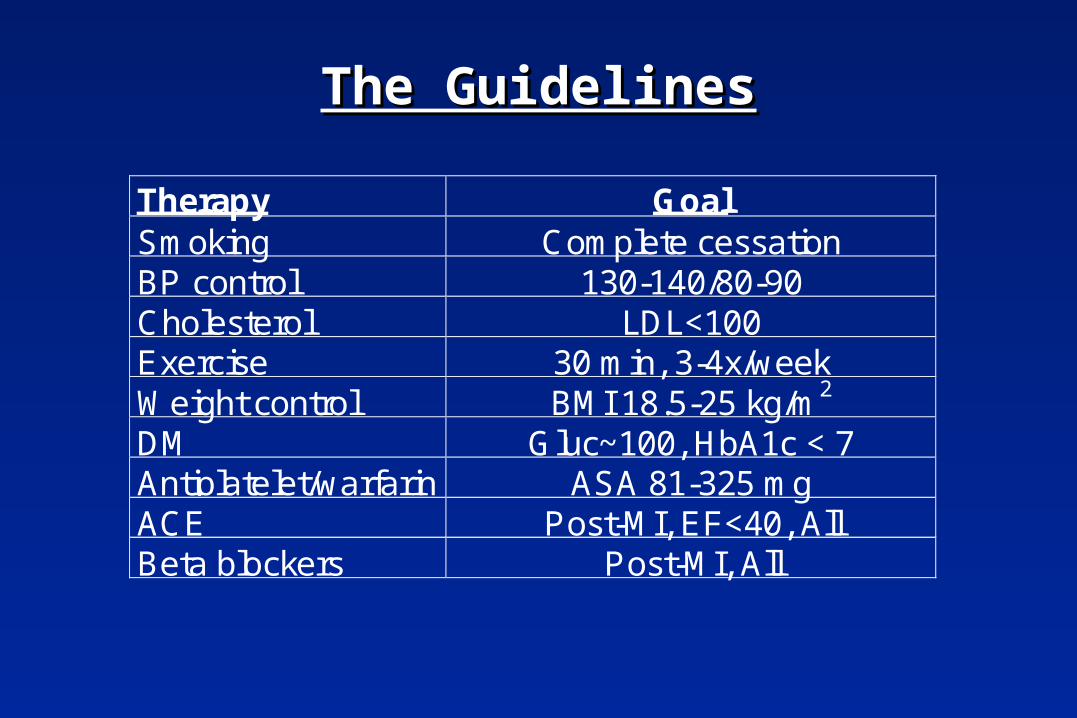
The GuidelinesThe Guidelines
Therapy GoalSmoking Complete cessationBP control 130-140/80-90Cholesterol LDL<100Exercise 30 min, 3-4x/weekWeight control BMI 18.5-25 kg/m2
DM Gluc~100, HbA1c < 7Antiplatelet/warfarin ASA 81-325 mgACE Post-MI, EF<40, AllBeta blockers Post-MI, All

How often do we provide these therapies?How often do we provide these therapies?
Therapy Rate ReferenceSmoking 48% Doescher J Fam Prac 2000;49;543
BP control 25% Berlowitz, NEJM 1998;339:1957Cholesterol 31.7% Fonarow Circ 2001;103:38
Exercise 19.1% MMWR 1998;47:91
Weight control 10.4% MMWR 1998;47:91DM 45% UKPDS AHJ 1999;138:353
Antiplatelet/warfarin 84% Rogers Circ 1994;90:2103ACE 75% (chf) J Gen Int Med 1997;12:563
Beta blockers 17.4% (iv) Rogers Circ 1994;90:2103PTCA (AMI) 30.3% Rogers Circ 1994;90:2103

Protocol in Cardiac Surgery• On discharge from the ICU -- ABC2D
aspirinbeta blockerconverting enzyme inhibitor (ACE)cholesterol-lowering agentdiabetes therapy and teaching
• Prior to discharge from the hospitalExerciseBMI recommendationsHTN therapy initiatedSmoking cessation
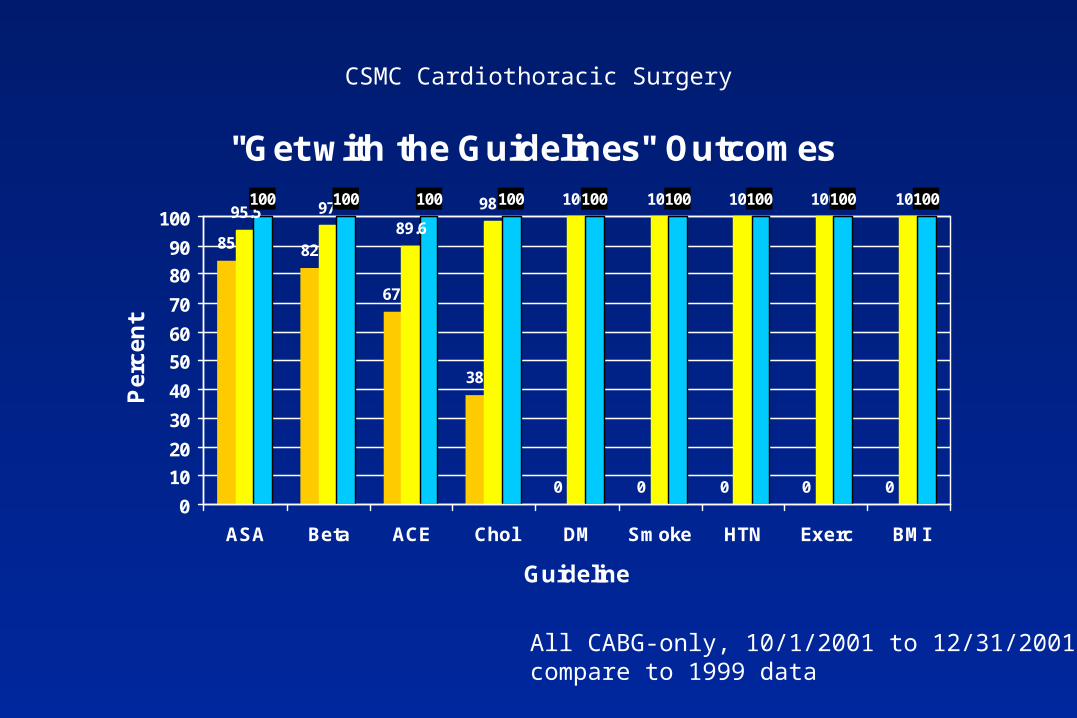
"Get with the Guidelines" Outcomes
85 82
67
38
0 0 0 0 0
95.5 9789.6
98.4 100 100 100 100 100100 100 100 100 100 100 100 100100
0
10
20
30
40
50
60
70
80
90
100
ASA Beta ACE Chol DM Smoke HTN Exerc BMI
Guideline
Pe
rce
nt
All CABG-only, 10/1/2001 to 12/31/2001compare to 1999 data
CSMC Cardiothoracic Surgery
Summary
• Fewer CABG, more valveand combinations
• Pump effects vs off-pump• Prophylaxis for postop
complications• “Systems of Care”
team speaks the same languageoptimal patient surgical and MEDICAL care
End