Embed Size (px)
Citation preview

ERS Annual Congress Vienna
1–5 September 2012
Postgraduate Course 13 AirPROM: patient-specific modelling and systems
biology living labs workshop
Saturday, 1 September 2012 14:00–17:30
Room: Schubert 5
Thank you for viewing this document. We would like to remind you that this material is the
property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
© 2012 by the author

The need and potential of patient-specific modelling
Prof. Christopher E. Brightling Institute for Lung Health
Glenfield Hospital LE3 9QP Leicester
United Kingdom [email protected]
Aims 1. Define the current approaches to phenotyping airways disease 2. Describe what is meant by scales of disease 3. Describe our current knowledge of immunopathology across the scales of disease using
asthma as an exemplar 4. Discuss the shortcomings of our current approaches to clinical integration of multi-scale data 5. Propose how systems biology and computational multi-scale modelling might add value to our
understanding of disease and its potential in stratified/personalized medicine Summary The airways diseases asthma and chronic obstructive pulmonary disease affect over 400 million people world-wide and cause considerable morbidity and mortality. Airways disease costs the European Union in excess of €56 billion per annum. Current therapies are inadequate due to our incomplete understanding of the pathophysiology of these diseases and our lack of recognition of the enormous disease heterogeneity, such that our current ‘one size fits all’ approach is inappropriate. We need to fully characterise this heterogeneity in order to identify the ‘right target’ for the ‘right patient’ and measure the ‘right outcome’. To achieve this goal we need sufficient tools to predict disease progression or response to current or future therapies. Current diagnostic criteria based on the presence of airflow obstruction and symptoms do not integrate the complex pathological changes occurring within the lung, do not define different airway inflammatory patterns, nor do they define different physiological changes or differences in structure as can be defined by imaging. Over recent years there has been interest in describing this heterogeneity and using this information to sub-group patients into airway disease phenotypes. Most approaches to phenotyping have considered disease at a single scale and have not integrated information from different scales (e.g. organ-whole person, tissue-organ, cell-tissue and gene-cell) of disease to provide multi-dimensional phenotypes. Integration of disease biology with clinical expression is critical to improve understanding of this disease. When combined with bio-statistical modelling, this information may lead to identification of new drug targets, new end-points for clinical trials and targeted treatment for subgroups of airway disease patients. It is hoped this will ultimately improve COPD outcomes and represent a move towards personalised medicine. In this review, we will consider these aspects of multi-dimensional phenotyping in more detail. References
1. Barker B, Brightling CE. Phenotyping the Heterogeneity of Chronic Obstructive Pulmonary Disease Clinical Science in press 2012
2. Brightling CE, Gupta S, Gonem S, Siddiqui S. Lung damage and airway remodelling in severe asthma. Clin Exp Allergy. 2012;42(5):638-49
3. Walker C, Gupta S, Hartley R, Brightling CE Computed tomography scans in severe asthma: utility and clinical implications Curr Opin Pulm Med. 2012;18(1):42-7.
4. Bousquet J, Anto JM, Sterk PJ, Adcock IM, Chung KF, Roca J, Agusti A, Brightling C, et al. Systems medicine and integrated care to combat non-communicable disease. Genome Med. 2011 6;3(7):43.
5

5. Gonem S, Desai D, Siddiqui S, Brightling C. Evidence for phenotype-driven treatment in asthmatic patients. Curr Opin Allergy Clin Immunol. 2011;11(4):381-5.
6. Brightling CE, Gupta S, Hollins F, Sutcliffe A, Amrani Y. Immunopathogenesis of severe asthma Curr Pharm Des. 2011;17(7):667-73.
7. Siddiqui S, Brightling C. Magic bullets: the new goal for asthma Am J Respir Crit Care Med. 2009; 180(5):383-4.
6

PG13 Patient specific modelling and systems biology living labs workshop-
‘The need and potential of patient specific modelling’
Professor Chris BrightlingInstitute for Lung Health, Leicester, UK
Conflicts of Interest
• AirPROM- EU FP7 6 industry partners, SMEs– www.airprom.european-lung-foundation.org/
• COPD MAP- MRC/ABPI 4 Pharma Partners
• Research Funding and Consultancy– Roche/ Genentech– AstraZeneca/ MedImmune– Novartis– GlaxoSmithKline– Chiesi
The need and potential of patient specific modeling
• 400 million people affectedwith asthma world-wide
•COPD third leading causeof death by 2030
• Airway disease costs EU>56 billion Euros/annum
7

The need and potential of patient specific modeling
• Validated models topredict airways diseaseprogression and response totreatment
• Platform to translatepatient-specific tools
• Personalised managementof airways disease.
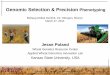
Asthma UK Asthma Audit 1999
191 209319
634
3793
152
305 310
1,1331,200
1,000
800
600
400
200
0% 2.5/17 8/ 32 8/ 18 5/ 7 1.5/ 1
Stage I II III IV V
Esti
mat
ed t
otal
cos
t of
trea
tmen
t pe
r pe
rson
(£) Exacerbations
No exacerbations
Towards Personalised Medicine
Traditional Asthma Classification
•Extrinsic / Intrinsic asthma Rackemann 1927
•Occupational asthma
•Exercise induced asthma
•Catamenal asthma
Aetiology
Patterns of Variable Airflow Obstruction•Turner-Warwick 1977- Brittle asthma- The morning dipper- Irreversible asthma
•Ayres 1998- Types 1 & 2 brittle asthma
Pathology•Pavord 1999, Wenzel1999, Green 2002- Eosinophilic Vs Non-eosinophilic
•BTS
•ATS Refractory
•ERS ‘Difficult’ asthma
•GINA
•NAEPP III
Severity/Control
•No uniformity•Descriptive•Focus on few dimensions of disease
8

Unravelling Complexity
“If you can not measure it, you can not improve it”.
Lord Kelvin
Unravelling Complexity
High Resolution Complex Phenotyping
Resolution
SymptomsSignsLung function
What is a Phenotype?
A phenotype is any observablecharacteristic that results from thegenetic background as well as theinfluence of environmental factors andpossible interactions between the two.
9

AIRWAY DISEASE
CHRONIC INFLAMMATION
Pathology
AIRFLOW OBSTRUCTION
AIRWAY HYPERRESPONSIVENESS
Physiology
SYMPTOMS
EXACERBATIONS
Clinical Expression
Airway Disease Domains
Inflammatory Phenotypes
BrightlingChest 2006;129(5):1344-8 COPD Asthma Normal
Sp
utu
m eo
sin
oph
ils (
%)
Brightling et al. Lancet 2000
Green et alLancet 2002
Asthma
Variable Airflow Obstruction
Allergy
Eosinophilic airway inflammation
Symptoms
- PEF Variability
- Modified JACS - Atopic status (SPT)
- Induced sputum
Demographics BMI
- Age of onset- Gender
Phenotyping Heterogeneity
PC20
10

Summary
INFLAMMATION PREDOMINANTLate onset
Greater proportion of malesFew daily symptoms
Concordant disease
Discordant Inflammation
Discordant Symptoms
OBESE FEMALE NON EOSINOPHILIC
High symptom expression
EARLY SYMPTOM PREDOMINANTNon-eosinophilic
Normal BMIHigh symptom expression
Refractory Asthma
Eos Inflammation
Sym
pto
ms
Haldar et al 2008 AJRCCM
Summary
INFLAMMATION PREDOMINANTLate onset
Greater proportion of malesFew daily symptoms
Discordant Inflammation
Discordant Symptoms
OBESE FEMALE NON EOSINOPHILIC
High symptom expression
EARLY SYMPTOM PREDOMINANTNon-eosinophilic
Normal BMIHigh symptom expression
Eos Inflammation
Sym
pto
ms
Haldar et al 2008 AJRCCM
Refractory Asthma
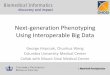
120
100
80
60
40
20
0
Severe exacerbations (cumulative
number)
0 1 2 3 4 5 6 987 10 11
Time (months)
12
‡p=0.01
1 asthma admission
6 asthma admissions
PhenotypeOutcomes at 12
monthsStudy Group Sig
Symptom predominant
Clinical Protocol
N=7
Sputum management
N=4
Change in ICS Dose
+1428.57 -400 0.022
Severe exacerbation frequency
5.43 2.50 0.198
Number commenced on OCS
6 (85.7%)
0 -
Cluster Specific Outcomes
11

PhenotypeOutcomes at 12
monthsStudy Group Sig
Inflammation predominant
Clinical Protocol
N=15
Sputum management
N=24
Change in ICS Dose +753.33 +241.67 0.22
Severe exacerbation frequency
3.53 0.38 0.002
Number commenced on OCS
2 (13.3%) 9 (37.5%) 0.167
Cluster Specific Outcomes
INFLAMMATION PREDOMINANTLate onset
Greater proportion of malesFew daily symptoms
OBESE FEMALE NON EOSINOPHILIC
High symptom expression
EARLY SYMPTOM PREDOMINANTNon-eosinophilic
Normal BMIHigh symptom expression
Refractory Asthma
Eos Inflammation
Sym
pto
ms
Specific Anti-eosinophil
Therapy
Right Patient, Right Target, Right Outcome
HaldarNEJM 2009
12

Airway geometry: response to mepolizumab
Siddiqui et alAllergy 2009
Haldar et al NEJM 2009
At Exacerbations:
Are there biological clusters?
Study Outline
Bafadhel et al AJRCCM 2011
13

Biological Clustering COPD Exacerbations
Factor
1 2 3
TNF α 0.80 -0.36
TNF R1 0.88
TNF R2 0.93
CCL13 0.82
CCL17 0.90
CXCL10 0.92
CXCL11 0.93
IL 1β 0.89 -0.36
IL 5 0.76
IL 6R 0.89
IL 8 0.83 Bafadhel et al AJRCCM 2011
Bacterial Exacerbation
IL1β 125pg/ml : 90% sensitive80% specific
AUC=0.89
Bacterial exacerbation if bacteria in stable state
OR 4.9 (2.4 to 9.9)
Predictors for Sputum Eosinophilia
AUC = 0.852% cut off 90% sensitivity, 60%
specificity
Eosinophilic exacerbationif eosinophilic in stable state
OR 2.7 (1.3 to 5.7)
14

At Exacerbations:
Can biomarkers direct therapy?
COPD Exacerbations: Targeted Therapy
Bafadhel et al AJRCCM 2012
Targeted Corticosteroid Therapy at Exacerbation
Bafadhel et al AJRCCM 2012
Health Status
Lung Function
Symptom Scores
15

Targeted Corticosteroid Therapy at Exacerbation
Bafadhel et al AJRCCM 2012
Complex Systems-homeokinesis
Clinical Exacerbation
Persistent disequilibrium
High risk
Day to day variation
Low risk
modulators
predictors
prevent
triggers
AirPROM‐ Airway Disease Predicting Outcomes
Through Patient Specific Computational Modelling
16

Large Airway: Structure-Function
Healthy Control
Severe Asthma
Large Airway: Structure-Function
CT Imaging Beyond Geometry
17

CFD: Therapeutic Response
Small Airway: Structure-FunctionSmall Airway Impedence
Ventilation Heterogeneity
Alveolar structure
Air Trapping
Inflammation
Small airway Domains
Air Trapping: Expiratory CT
18

Small airway obstruction in Asthma & COPD
Hogg et al NEJM 2004
Airway Remodelling
Immunopathology Asthma versus COPD
19

Gene Protein Cell Tissue Organ Patient
PATHOGENS
Bacteria/ Viruses/ Moulds
ALLERGENSPOLLUTION &
Physical Damage
Host SusceptibilityImpaired Innate immunity
TIME
The need and potential of patient specific modeling
Patient-Specific Multi-Scale Models
Benayoun 2003 AJRCCM
Politi J Thero Biol2010
ORMDL3Moffat NEJM 2010, Nature 2007
Cantero-Recaseus Hum Mol Gen 2010
Mahn 2009 PNAS
Personalised Healthcare / Target Identification
UP & Down the Scales
20

Acknowledgements
21

22