Embed Size (px)
Citation preview

POSTGRADUAAT ASO 2021
Vaatheelkunde

I
SPREKERS
09.00 – 09.30 Prof. Aerden Critical Limb Ischemia
09.30 – 10.00 Dr. Kerselaers Symptomatische Carotisstenose
10.00 – 10.30 Prof. Debing Buikaneurysma

I
CRITICAL LIMB ISCHEMIA
08-02-17
Titel van de presentatie
3
Definition
A limb with chronic, end-stage arterial occlusive disease, that is expected to
require amputation UNLESS successful revascularisation is performed.
- end-stage peripheral arterial disease (atherosclerotic disease)
- Fontaine 3-4 (restpain-tissue loss), or Rutherford 4-5-6 (restpain-minor/major tissue
loss)
- slow progression (years)
- usually uncontrolled CRF
- long history of revascularisations
- long occlusions (stenosis exclusively), multilevel disease (iliac/fem/pop/BTK),
collaterals+++, calcifications (CNI, DM, +80y)
- Ankle-Brachial Index <0.4

I
CAVE: CLI VS ACUTE ISCHEMIA VS DF
08-02-17
Titel van de presentatie
4
‘It’s all occluded arteries’
Acute ischemia CLI DF + PAD
pulselessness +++ +++ ++ (BTK)
pain +++ +++ 0
palor ++ + (<>Buerger test) 0
poikilothermia +++ + 0
paralysis +++ + 0
par/an-esthesia ++ 0 +++
non-healing wound 0 +++ (spontanous) +++ (trauma, neuropathy)
timing hours (acute) years weeks
flow interuption trombus, (plaque rupture) lesions lesions
trauma/aneurysm/embolism atherosclerosis (severe)
atherosclerosis

I 52/23/2021
CRITICAL LIMB ISCHEMIA ≠ DIABETIC FOOT ULCERATION!
Burn victim
25 sept
Progressive infection
3d3d

I2/23/2021 6
Archetype:dry, circumferential necrosismultiple area’s affectedsurroundings = nl‘far from the heart’

I1940 1945 1950 1955 1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010 2015 2020 2025
IKED-voet2003
M.E. Edmonds1986
Specialised diabetic foot clinic
Brewster1978
Aneurysm repair with synthetic graft
D.G. Armstrong1997
Charcot arthropathy
J. Kunlin1951
Autologous vein grafting
K. Van Acker2000
DFC in Belgium
Best & Murray1940
Heparin purification & use
J.C. Dos Santos1946
First endarterectomy
M. DeBakey1950
First carotidendarterectomy
B. Lipsky1991
Diabetic foot infections
C. Attinger2001
Foot angiosomes
C. Dubost1951
Aneurysm repair with homograft
Cassarella1988
BTK angioplasty
Mullan1980
First Carotid stenting
A. Bolia1990
Subintimal angioplasty
A. Boulton1986
Total Contact Cast
A. Grüntzig1977
First coronary angioplasty
Burke1986
PTFE prothese
L. Graziani2003
Endovascular feasibility in DF
J. Parodi1991
Aneurysm exclusion with endograft
C. Dotter1964
First PTA
E. Faglia2005
Endovascular First for DF
St. Vincent Declaration1989
Reduce Major Amputation by 50%
V.A. Alexandrescu2008
Angiosome-guided revascularization
Open, Reconstructive Vascular Surgery
Endovascular Techniques
Diabetic Foot Pathofysiology
2/23/2021 7

I
RECENT CLI STUDIES
Biagioni RB, Nasser F, Matielo MF, Burihan MC, Brochado Neto FC, Ingrund JC, Sacilotto R.
Comparison of Bypass and Endovascular Intervention for Popliteal Occlusion with the
Involvement of Trifurcation for Critical Limb Ischemia. Ann Vasc Surg. 2020 Feb;63:218-226
Altreuther M, Mattsson E. Long-Term Limb Salvage and Amputation-Free Survival After
Femoropopliteal Bypass and Femoropopliteal PTA for Critical Ischemia in a Clinical Cohort.
Vasc Endovascular Surg. 2019 Feb;53(2):112-117
Dayama A, Tsilimparis N, Kolakowski S, Matolo NM, Humphries MD. Clinical outcomes of
bypass-first versus endovascular-first strategy in patients with chronic limb-threatening
ischemia due to infrageniculate arterial disease. J Vasc Surg. 2019 Jan;69(1):156-163
Mustapha JA, Katzen BT, Neville RF, Lookstein RA, Zeller T, Miller LE, Nelson TR, Jaff MR.
Propensity Score-Adjusted Comparison of Long-Term Outcomes Among Revascularization
Strategies for Critical Limb Ischemia. Circ Cardiovasc Interv. 2019 Sep;12(9)
08-02-17
Titel van de presentatie
8
Bypass vs Endovascular revascularization

I 92/23/2021

I 102/23/2021

I
ENDOVASCULAIR VS OPEN HEELKUNDE
Endovasculair Open heelkunde
+ - + -
anesthesie locale algemene- of locoregionale
incisies geen wondinfectie en littekens
bloed verlies geen onvermijdelijk
contrast allergienefrotoxisch
bestraling
minimaal
patency goed (iliacaal) matig (SFA)slecht (BTK)
goed (ATK)matig (BTK)
slecht indien langebypass en prothese
bypass geen vene PTFE/Dacron
hospitalizatie kort lang
arteriëlesegmenten: multiple of onbereikbaar
ja nee
redo gemakkelijk moeilijk (distalerelandingszone)
2/23/2021 11

I
ENDOVASCULAIR VS OPEN HEELKUNDE
Endovasculair Open heelkunde
+ - + -
anesthesie locale algemene- of locoregionale
incisies geen wondinfectie en littekens
bloed verlies geen onvermijdelijk
contrast allergienefrotoxisch
bestraling
minimaal
patency goed (iliacaal) matig (SFA)slecht (BTK)
goed (ATK)matig (BTK)
slecht indien langebypass en prothese
bypass geen vene PTFE/Dacron
hospitalizatie kort lang
arteriëlesegmenten: multiple of onbereikbaar
ja nee
redo gemakkelijk moeilijk (distalerelandingszone)
DM = immunosuppressieulcus = ingangspoort voorinfectie (CAVE prothese)
patency loss ≠ ulcer recurrencewondgenezing ± 3-6 maand
multilevel disease: meerderearteriële segmenten kunnentegelijkertijd behandeld worden
ulcus recidieven zijn ZEER frequent
Femoro-distale bypass: 1m lange vene zeldenbeschikbaar
2/23/2021 12

I
OPEN/BYPASS SURGERY
- low surgical/anesthesiological risk (‘the fit elder’)
- maximalization of patency required
- large tissue defect (wound): months of healing required
- rest pain: patency loss = reoccurance of pain
- involvement of common femoral and deep femoral artery
- multi-level disease, long occlusions of SFA and popliteal P2-3
- excellent landing/receptor arterial segment with outflow to correct angiosome
- venous conduit available
- all other: ENDOVASCULAR FIRST/ONLY (+ REDO)
08-02-17
Titel van de presentatie
13
when is open surgery the optimal revascularization mode?

I
COMPOUND PATENCY
08-02-17
Titel van de presentatie
14
SFA - Full Metal Jacket
10/6/2020
1/2/2021

I
ENDOVASCULAR REVASCULARIZATION
- minimal invasive (morbidity, mortality)
- local anesthesia
- minimal blood loss
- no surgical wounds
- multiple target vessels (BTK), simultaneous revascularization
- redo perfectly doable (patency bypass > PTA = false debate)
- low(er) patency = acceptable (small wounds) (DCB/DES to the rescue?)
- ankle and foot arteries (bypass = no option)
- full occlussions (no landing zone required) (bypass = no option)
08-02-17
Titel van de presentatie
15
when is endovascular the optimal revascularization mode?

I
ENDOVASCULAR
08-02-17
Titel van de presentatie
16
Emerging technologies• Paclitaxel
• Cryotherapy
Intima Hyperplasia
• Intravascular Lithotripsy
• Scoring Balloons
Plaque Rupture
• Arterectomy devices
• Laser
Tunnelisaztion
• Biodegradable
• DES
• Sirolimus
• Paclitaxel
Stents

I
PACLITAXEL / DCB
IMPACT- DEEP BTK trial
Konstantinos Katsanos: meta-analysis of 2018 (28 RCTs*) and 2019 (8 RCTs):
‘higher mortality and limb loss, dose dependant’
FDA: stop!
initial industry response: suspicious
08-02-17
Titel van de presentatie
17
*Katsanos K, Spiliopoulos S, Kitrou P, Krokidis M, Karnabatidis D. Risk of Death Following Application of Paclitaxel-Coated Balloons and Stents in the Femoropopliteal Artery of the Leg: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Am Heart Assoc. 2018 Dec 18;7(24)

I
MEDIACALCINOSIS (ARTERIAL WALL CALCIFICATION)
2/23/2021 18
diabetesrenal failureoctogenarians

I
CLI REVASCULARISATION
1. ‘Aorta+Iliac/Femoral/FemPop/2xTibial+Peroneal’
Ankle and Foot arteries are equally important
CT-angio protocol irrelevant when foot pulses are ABSENT
2. ‘Indirect revascularization of wrong angiosome =
OK’
Direct revascularization
3. ‘First: repair inflow (iliac, femoral)’
Flow-limiting leasions are usually BTK
4. ‘Incomplete opening of full length occlusion =
collateral recruitment’
Provide pulsatile flow towards wound region (inflammatory
blush)
08-02-17
Titel van de presentatie
19
Misconceptions / New Insights

I
CLI REVASCULARISATION
1. ‘Aorta+Iliac/Femoral/FemPop/2xTibial+Peroneal’
Ankle and Foot arteries are equally important
CT-angio protocol irrelevant when foot pulses are ABSENT
2. ‘Indirect revascularization of wrong angiosome =
OK’
Direct revascularization
3. ‘First: repair inflow (iliac, femoral)’
Flow-limiting leasions are usually BTK
4. ‘Incomplete opening of full length occlusion =
collateral recruitment’
Provide pulsatile flow towards wound region (inflammatory
blush)
Titel van de presentatie
Misconceptions / New Insights
08-02-
17
Titel van de presentatie2
0
BTK:- Diabetics- Octogenarians- Renal Failure

I08-02-17
Titel van de presentatie
21

I
CLI REVASCULARISATION
1. ‘Aorta+Iliac/Femoral/FemPop/2xTibial+Peroneal’
Ankle and Foot arteries are equally important
CT-angio protocol irrelevant when foot pulses are ABSENT
2. ‘Indirect revascularization of wrong angiosome =
OK’
Direct revascularization
3. ‘First: repair inflow (iliac, femoral)’
Flow-limiting leasions are usually BTK
4. ‘Incomplete opening of full length occlusion =
collateral recruitment’
Provide pulsatile flow towards wound region (inflammatory
blush)
08-02-17
Titel van de presentatie
22
Misconceptions / New Insights
“An angiosome is a block of tissue
that is fed by one source artery”
Taylor GI, Palmer JH. The vascular territories
(angiosomes) of the body: experimental study and clinical
applications. Br J Plast Surg. 1987;40(2):113–141.

I
CLI REVASCULARISATION
1. ‘Aorta+Iliac/Femoral/FemPop/2xTibial+Peroneal’
Ankle and Foot arteries are equally important
CT-angio protocol irrelevant when foot pulses are ABSENT
2. ‘Indirect revascularization of wrong angiosome =
OK’
Direct revascularization
3. ‘First: repair inflow (iliac, femoral)’
Flow-limiting leasions are usually BTK
4. ‘Incomplete opening of full length occlusion =
collateral recruitment’
Provide pulsatile flow towards wound region (inflammatory
blush)
08-02-17
Titel van de presentatie
23
Misconceptions / New Insights
art. peronealis
art. tibialis posterior
art. tibialis anterior

I
CLI REVASCULARISATION
1. ‘Aorta+Iliac/Femoral/FemPop/2xTibial+Peroneal’
Ankle and Foot arteries are equally important
CT-angio protocol irrelevant when foot pulses are ABSENT
2. ‘Indirect revascularization of wrong angiosome =
OK’
Direct revascularization
3. ‘First: repair inflow (iliac, femoral)’
Flow-limiting leasions are usually BTK
4. ‘Incomplete opening of full length occlusion =
collateral recruitment’
Provide pulsatile flow towards wound region (inflammatory
blush)
08-02-17
Titel van de presentatie
24
Misconceptions / New Insights
2/23/2021 24

I
BTK ARTERIAL SEGMENTS ARE PREDOMINANTLY
AFFECTED
2/23/2021 25

I
CLI REVASCULARISATION
1. ‘Aorta+Iliac/Femoral/FemPop/2xTibial+Peroneal’
Ankle and Foot arteries are equally important
CT-angio protocol irrelevant when foot pulses are ABSENT
2. ‘Indirect revascularization of wrong angiosome =
OK’
Direct revascularization
3. ‘First: repair inflow (iliac, femoral)’
Flow-limiting leasions are usually BTK
4. ‘Incomplete opening of full length occlusion =
collateral recruitment’
Provide pulsatile flow towards wound region (inflammatory
blush)
Titel van de presentatie
Misconceptions / New Insights

I
SPREKERS
09.00 – 09.30 Prof. Aerden Critical Limb Ischemia
09.30 – 10.00 Dr. Kerselaers Symptomatische Carotisstenose
10.00 – 10.30 Prof. Debing Buikaneurysma

Carotispathologie: indicaties en behandeling
Laura Kerselaers, kliniekhoofdVaatchirurgie UZ Brussel
Vrijdag 12 februari 2021ASO's 4de en 5de opleidingsjaar Algemene Heelkunde

I
BEROERTE MAJEUR GEZONDHEIDSPROBLEEM
1ste
oorzaak verworven handicap volwassenen
3de
oorzaak overlijden
Burden of stroke in Belgium (2015-SAFE):
Incidentie: 10.000 per jaar (↑ 39% te verwachten 2015-2035)
Kost: ong 400 miljoen/jaar
Ong 50 % overlijdt binnen het jaar
Ong 1/3 blijvende handicap

I
BEROERTE PLOTSE VERSTORING BLOEDVOORZIENING IN DE HERSENEN
Herseninfarct -ischemisch
(85%)
Hersenbloeding -hemorrhagisch(15%)
Klinisch geen onderscheid: beeldvorming nodig

I
BE FAST REMINDER OF STROKE SIGNS
B - BalanceIs the person suddenly having trouble with balance or coordination?
E – Eyes Is the person experiencing suddenly blurred or double vision or a sudden loss of vision in one or both eyes?
F - Face DroopingDoes one side of the face droop or is it numb? Ask the person to smile.
A- Arm Weakness Is one arm weak or numb? Ask the person to raise both arms. Does one arm drift downward?S - Speech DifficultyIs speech slurred, are they unable to speak, or are they hard to
understand? Ask the person to repeat a simple sentence like, “The sky is blue.” Is the sentence repeated correctly?T - Time to call 9-1-1If the person shows any of these symptoms, even if the symptoms go away,
call 9-1-1 and get them to the hospital immediately
Source: American Stroke Association

I
2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in
collaboration with the European Society for Vascular Surgery (ESVS). Document covering
atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper
and lower extremity arteries. Endorsed by: the European Stroke Organization (ESO).
Eur J Vasc Endovasc Surg (2018) 55, 305e368
Questions and Answers on Diagnosis and Management of Patients with Peripheral
Arterial Diseases: A Companion Document of the 2017 ESC Guidelines for the Diagnosis
and Treatment of Peripheral Arterial Diseases, in collaboration with the European
Society for Vascular Surgery (ESVS) Endorsed by: the European Stroke Organisation
(ESO).
Eur J Vasc Endovasc Surg (2018) 55,
457e464
Management of Atherosclerotic Carotid and Vertebral Artery Disease: 2017 Clinical
Practice Guidelines of the European Society for Vascular Surgery (ESVS). A.R. Naylor a,
J.-B. Ricco a, G.J. de Borst a, S. Debus a, J. de Haro a, A. Halliday, et al.
Eur J Vasc Endovasc Surg (2018) 55, 3e81

I
AETIOLOGY OF CAROTID TERRITORY ISCHAEMIC STROKE
The principal causes of ischaemic, carotid territory stroke are
thromboembolism from ICA or MCA (25%),
small vessel intracranial disease (25%),
cardiac embolism (20%),
other specified rarer causes (5%),
and unknown causes despite investigation (25%).
Overall, about 10 -15% of all strokes follow thromboembolism
from a previously asymptomatic ICA stenosis >50%.

ICopyrights apply

I
CASE 1
A 76-year-old male is referred 48 hours after a transient ischaemic attack in the territory of the left carotid artery.
He presented a recurrent episode of transient aphasia two hours prior to admission. He is not currently taking any medication. The duplex ultrasound scan (DUS) reveals a 60% stenosis of the left internal carotid artery (ICA) and non-stenotic plaques in the right ICA.

I
CASE 1
Onderscheid symptomen carotisstenose:
–> asymptomatisch vs symptomatisch (< 6ma)
Onderscheid symptomatologie:
-> AF (ipsi) – TIA – stroke (contra)
Q1. Do you plan any further carotid imaging?
>DUS – CTA - MRA
>CAS –> aortic arch
Q2. How would you manage the patient?
>CEA? - CAS? – BMT?
>Timing?

I

I
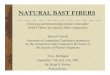
METHODS FOR MEASURING CAROTID ARTERY STENOSIS SEVERITY.
23-2-202138

I11/10
/201239
PreSSUB
Stroke = Time is brain
Neurologist: IVTL < 4,5u after onsetInterventional radiologist: Trombectomy major vesselocclusion <24h
Goals: door to needle: < 30 min (< 15 min bij de routines)door to groin: < 60 min
CEA – CAS - BMT = Prevention of strokeremove – cover – stabilize plaque

I
TIMING CEA
Stroke-in-evolution, Crescendo TIAs : urgent
TIA, minor stroke: asap (within 2 weeks)
Patients with a significant neurological deficit (modified Rankin > 3), with an area
of infarction exceeding one-third of the MCA territory and those who have altered
consciousness should not undergo CEA until significant neurological improvement
has occurred.
11/10
/2012PreSSUB 40

I
CASE 3
A 62-year-old man is referred for a left carotid bruit. He is asymptomatic and smokes tobacco regularly. DUS found a 70% left ICA stenosis. His medical history includes a transient ischaemic aphasia seven years earlier and a thyroidectomy complicated by right recurrent laryngeal nerve (RLN) palsy.
Further investigations reveal that the left carotid lesion is predominantly echolucent and there is evidence of an old ‘silent’ infarction in the left parietal hemisphere.

I
CASE 3
Q6. Should the 70% asymptomatic left ICA stenosis be treated?
• Optimal medical therapy
• Smoking cessation and assistance.
• Carotid revascularization
Q7. What should be the revascularization strategy: CEA or CAS?

I

I11/10
/201244
PreSSUB

I23-2-2021 45

I
TREATMENT CEA : PLAQUE REMOVAL
Type anesthesia
- AA vs LRA
23-2-202146

I
Fixatie hoofd en bovenste
ledematen
Arteriële bloeddrukmonitoring
Monitoring contralaterale
motoriek
Monitoring hogere
hersenfuncties (tellen)
Installatie Locoregionale anesthesie

I
TREATMENT CEA : PLAQUE REMOVAL
Type anesthesia
Classic vs eversion endarterectomy
23-2-202148

I
KLASSIEKE CEA
08-02-17 49

I
EVERSIETECHNIEK - RAITHEL
08-02-17 50
Indicaties:
• Kinking ACI
Voorwaarde Raithel:
• Geïsoleerde ACI aantasting
Nadeel:
• Shunting moeilijker

I
EVERSIE ENDARTERECTOMIE
08-02-17 51

I
TREATMENT CEA : PLAQUE REMOVAL
Type anesthesia
Classic vs eversion endarterectomy
Anteromediaal vs retrojugulair
23-2-202152

I
ANTEROMEDIAAL VS RETROJUGULAIR
Beasley et al.
Ann R Coll Surg
Eng 2008

I
TREATMENT CEA : PLAQUE REMOVAL
Type anesthesia
Classic vs eversion endarterectomy
Anteromediaal vs retrojugulair
Patch vs primary closure
23-2-202154

I
TREATMENT CEA : PLAQUE REMOVAL
Type anesthesia
Classic vs eversion endarterectomy
Anteromediaal vs retrojugulair
Patch vs primary closure
Shunt? No – routine - indication
- no shunt (?) when: stump-pressure, frontal lobe monitoring (EEG, NIRS), LRA
- circulus of Willis ok? Contralateral occlusion?
- shunt complications: dissection, air- of blood clot embolism
- increases operation difficulty
- false sense of security (no flow)
23-2-202155

I
CAROTID ARTERY STENTING : PLAQUE COVERING
• EPD (embolic protection device)
• Compared to CEA: more minor stroke perioperative, equal results at long term
• Indications
> hostile neck (redo surgery, tracheo, radiation neck, cervical kyphosis/obesity)
> Contralateral vocal cord paralysis
> lesion out-of-reach (under mandibula), or concomitant lesions in CCA
> unfit for anesthesia: very rare indication
23-2-202156

I
TECHNIEK – CAS (1/3)
26-04-2018
Techniek van carotid artery stenting
57
Via AFC
- Retrograad aanprikken AFC
- Plaatsen korte 7Fr. Sheat
- 0.035 voerdraad en catheter om ACC te catheteriseren tot ACE

I
TECHNIEK – CAS (2/3)
- Exchange naar stijve guidewire
- Opvoeren lange sheat tot in ACC
- Angiografie
- 0,014 voerdraad met Embolic Protection
Device op gemonteerd
- Voorzichtig tot voorbij letsel passeren
- Catheter terug trekken, EPD ter plaatse,
ruim voorbij stenose
26-04_2018
Techniek van carotid artery stenting
58
Via AFC

I
TECHNIEK – CAS (3/3)
- Zo nodig predilateren
- Stent positioneren en vrijzetten
- Postdilatereren, zacht niet
aandringen
- Controle angiografie
- Verwijderen van EPD nadat dit
terug dicht getrokken wordt in
catheter
- Verwijderen sheat mits closure
device of manuele compressie
08-02-17
Titel van de presentatie
59
Via AFC

IBest medical therapy
6023-2-2021
BEST MEDICAL THERAPY : PLAQUE STABILISATION
In secundaire preventie van CVA/TIA wordt aanbevolen:
Een geleidelijk te bereiken maar strikte
bloeddrukcontrole, waarbij ACEI en ARB de voorkeur
genieten.
Een absolute rookstop.
Een strikte controle van diabetes mellitus.
Toediening van een statine, ook bij borderline normale
cholesterolemie.

IBest medical therapy
6123-2-2021
BEST MEDICAL THERAPY : PLAQUE STABILISATION
Anti-aggregerende medicatie :
• Aspirin 75 à 160 mg/d bij asymptomatische stenose
• Aspirine + Clopidogrel 75mg bij TIA/minor stroke, na 3 weken
Clopidogrel in monotherapie verder
Anticoagulantia
• Bij voorkamerfibrillatie of cardiale emboligene pathologie
• In monotherapie !

I
QUESTION #1
SHOULD WE CONSIDER ANY INTERVENTION (CEA / CAS)
FOR ASYMPTOMATIC CAROTID PATIENTS?
ASYMPT STENOSE: REVASC VS BMT:
ECST-2, CREST-2
QUESTION #2
CEA VS CAS IN ASYMPT PATIENTS?
ACST-2
GUIDELINES: 2022
Two BIG questions in carotid research:

VRAGEN?

I
SPREKERS
09.00 – 09.30 Prof. Aerden Critical Limb Ischemia
09.30 – 10.00 Dr. Kerselaers Symptomatische Carotisstenose
10.00 – 10.30 Prof. Debing Buikaneurysma

I
CASUS
65
23-2-2021
Vrouw van 74 jaar vertoont sinds enkele weken vage abdominale pijnen en af en toe messtekende pijnen ter hoogte van de rug
Medische voorgeschiedenis Hysterectomie en ovariectomie Appendicectomie
Cardiovasculaire risicofactoren Actief tabagisme AHT hypercholesterolemie
Thuismedicatie Exforge 10/160mg 1x/dag Crestor 10 mg 1/dag

I
FYSIEK ONDERZOEK
66
23-2-2021
BD 135/85
Hartritme:102 per minuut, regelmatig
Normale vulling en hydratatie
BMI 28
Aa carotis +/+, geen souffle
Cor: S1 S2, geen souffle
Longen: zuivere auscultatie
Abdomen: pulsatiele massa, pijnlijk bij diepe palpatie
Pulsaties te voelen ter hoogte van arterie femoralis communis, poplitea,
dorsalis pedis en tibialis posterior

I67
23-2-2021

I
BIJKOMENDE ONDERZOEKEN
68
23-2-2021
Duplex

I
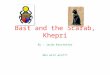
BIJKOMENDE ONDERZOEKEN: CTA
69
23-2-2021
Diameter: 7,2 cm

I 7023-2-2021
Diagnose:
Symptomatisch infrarenaal aorta
abdominalis aneurysma (contained
rupture)

I
BEHANDELING - INDICATIE
71
23-2-2021
Vrouw ≥ 5 cmMan ≥ 5,5 cmSnelgroeiende (≥ 1 cm/jaar)SacculairSymptomatische aneurysma

I
RUPTUUR
72
23-2-2021
Contained rupture Retroperitoneale bloeding Intraperitoneale bloeding
Pijn
HD stabiel
Normaal Hb
Pijn
Tachycardie
Normo- tot hypotensief
Daling Hb
Tachycardie
Hypotensief
Hypovolemische shock
Extreem laag Hb

I
BEHANDELING
73
23-2-2021
Ervaren team
Bloed en plasma bestellen
Cell saver
Hypotensieve hemostase
Anesthesie inductie start wanneer chirurgen steriel staan en patiënt afgedekt is

I
OPEN HERSTEL
74
23-2-2021

I 7623-2-2021

I 7723-2-2021

I 7823-2-2021

I79
23-2-2021

I 8023-2-2021

I 8123-2-2021

I 8223-2-2021

I83
23-2-2021

I 8423-2-2021

I 8523-2-2021

I 862/23/2021

I87
23-2-2021

I
ENDOLEAKS
88
23-2-2021

I 8923-2-2021
TYPE Ia Endoleak
Predictor = outside IFU

Ititel9023-2-2021
VASCULAR TEAM UZB