Embed Size (px)
Citation preview

ANNALS OF SURGERYAugust 1959 No. 2
Postamputation Radiographic Evidence for Small ArteryObstruction in Arteriosclerosis
EDWARD A. EDWARDS, M.D.**
From the Department of Surgery, Peter Bent Brigham Hospital, and the Departmentof Anatomy, Harvard Medical School, Boston
Introduction
IN SPITE of the general assertion thatarteriosclerosis does not affect small arteriesin nondiabetics, it is commonplace to findocclusion of both named and unnamedsmall arteries and arterioles in the toes or
feet amputated from such individuals. Evenin diabetes, where small artery involvementis recognized as a common finding, no sys-
tematic study of this involvement is avail-able. Dible 2 has indeed studied the largernamed arteries of the foot in arteriosclerosis,and found partial or complete obstructionhere in about 25 per cent of cases, a fre-quency roughly one-third that of obstruc-tion at tibial and femoral levels.
It was the purpose of the study here re-
ported to extend these observations to thesmaller vessels of the foot and toes, to de-termine the pattern of occlusion in diabetic
* Submitted for publication September 8, 1958.** Senior Associate in Surgery, Peter Bent
Brigham Hospital, and Associate Clinical Professorof Anatomy, Harvard Medical School.
Read at the Annual Meeting of the Massachu-setts Medical Society, Boston, May 21, 1958.
Aided by grant No. H-2661 from the NationalInstitutes of Health.
and nondiabetic limbs, and to lay a founda-tion for further pathologic and clinicalanalysis of obstruction to the arteries of thetoes and heel.
Postamputation angiography was themethod employed, since it allows a rapidsurvey of the entire arterial tree of theamputated part. The mercury and bariumsulphate emulsion of Reiner, Rodriguez,and Jimenez 7 was the medium used. It isstrongly opaque, fills the smallest arteriesand probably arterioles quite easily, anddoes not pass the capillary bed. Histologicstudy of the injected part is not hindered.Mr. Rudolph Cumberbatch of the HarvardMedical School, class of 1959, gave tech-nical assistance in the trial of the mediumin animals.
Material and MethodThirteen arteriosclerotic lower limbs have
been studied. They comprise a fair sam-
pling of arteriosclerosis serious enough tolead to amputation. The age of the patientsranged from 57 to 89. Six were women,
seven men. Four patients were diabetic.Diabetes was ruled out in the other patientsby repeated blood and urine examinations.
177
Vol. 150

EDWARDS Annals of SurgerAugust 1959
MED. PLRNT)qP
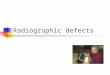
FIG. 1. Relatively normal vessels from a 69-year-old woman with iliac embolism and femoralarteriosclerotic occlusion. Arrows indicate occluded arteries.
In two patients the ischemic problem arose
after arterial embolism, peripheral arterio-sclerosis being mild in one instance, severe
in the other. In all instances arterioscleroticocclusion was known to exist at one or more
sites in the iliac, femoral, or popliteal ar-
teries.Four lower and two upper extremities of
young individuals were also studied withthe same technic. These were all amputated
178

POSTAMPUTATION RADIOGRAPHIC EVIDENCE
for proximal nonvascular disease. Their ves-sels were presumably normal, and the filmsoffer confirmation of the pattern of the ar-teriosclerotic occlusions.Most of the limbs were injected within an
hour or two after amputation. The terminalradicles were somewhat less well shownwhen injection was delayed one or moredays. A cannula was inserted distally in thedorsalis pedis artery if that was patent. Ifnot, the posterior tibial was employed. Inthree instances where both were occluded,the perforating peroneal could be can-nulated.
Flushing out the vessels by means ofabout 100 cc. of normal saline solution im-proved the visualization of the finestbranches. After this maneuver a tourniquetwas placed below the amputation wound,and 6 to 14 cc. of the opaque medium wereinjected. The injection was made with an
ordinary glass syringe. No manometer wasused, but the pressure was judged to befrom 200 to 300 mm. Hg. Small extravasa-tions occurred occasionally, and large ac-
cumulations followed the use of a volumeof medium beyond that mentioned.
Results
Normal AnatomyA good perfusion of the arteries both
proximally and distally was obtained, with-out regard to the artery cannulated. Micro-scopic examination showed filling of ex-
tremely fine arteries as well as some of thearterioles. The capillaries were not filled,and none of the medium entered the veins.Major pedal arteries. Some of the fea-
tures of the arterial pattern are better seenin the wider vessels of the adult than in theslender ones of the child. It may thereforebe useful to turn directly to the film of a
patient whose pedal vessels were only min-imally diseased (Fig. 1).Three arteries-the anterior and posterior
tibial, and the peroneal-constitute thesources of the pedal circulation. As has
been mentioned elsewhere,4 one of thesemay preponderate over the other. In thisinstance we see the most frequent pattern.The dorsalis pedis is large, and perforatesthe first metatarsal space to join the lateralplantar branch of the posterior tibial toform the plantar arch. The medial plantarhas smaller and less direct connections withthe arch. The peroneal bends backward, itsimage crossing that of the posterior tibial.A perforating branch ordinarily proceedsforward above the ankle, but is uncertainhere. The dorsalis pedis may normally belacking or minute, according to Huber, in12 per cent.5 In these cases its place is gen-erally taken by the perforating branch ofthe peroneal, which may, however, branchrepeatedly over the dorsum of the foot.Distally the peroneal artery, often calledthe posterior lateral malleolar, is bold andterminates in peroneal calcaneal branches.
Calcaneal circulation. The lateral por-tion of the heel is supplied partly by theperoneal calcaneal branches, and partly bythe lateral tarsal, arising from the dorsalispedis. The branches of the peroneal andlateral tarsal course approximately in thelong axis of the foot, anastomosing in thecalcaneal rete.The medial portion of the heel is sup-
plied by several medial calcaneal arteries,arising from the proximal part of the lateralplantar. One or more of these may arisefrom the posterior tibial itself, or from theposterior lateral malleolar branch of thatvessel. The medial calcaneal arteries branchrepeatedly as they radiate from their originsto the calcaneal rete.
Digital circulation. The vessels of thisarea are shown in Figures 2 and 3 of a"normal" specimen amputated from a 17-year-old boy. Some of the detail to be de-scribed is based on stereoscopic study ofthis specimen.Both plantar and dorsal vessels exist, of
which the plantar are much the wider andlonger. The digital supply stems mainlyfrom the plantar arch, and to a lesser de-
Volume 150Number 2 179

Annals of SurgeryAugust 1959
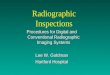
Fic. 2. Digital circula-tion in a limb from a 17-year-old boy amputatedfor congenital deformityof the femur. The dorsalispedis and lateral plantararteries are narrowed bythe proximal tourniquet.
gree from the dorsalis pedis and plantararteries proximal to the arch. Four largeplantar metatarsal arteries are seen, eachdividing distally into plantar digital arteriesfor the contiguous borders of adjacent toes.Special arteries exist for the free bordersof the first and fifth digits. The medialdigital I arises from the first metatarsal; thelateral digital V is a separate branch fromthe plantar arch.The two plantar digital arteries supply-
ing a single toe are usually of unequal size.
The "preponderant" artery bifurcates at theproximal part of the terminal tuft to con-
stitute its major supply, the "diminutive"partner joining its border of the tuft by fineand numerous branches.The great toe is the seat of two quite con-
stant large transverse anastomoses. Theproximal is constituted by the branching ofthe medial digital I from the first meta-tarsal; the distal lies across the proximalphalanx. In addition this specimen showsa "circumferential" artery which is more
180 EDWARDS

POSTAMPUTATION RADIOGRAPHIC EVIDENCE
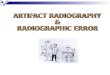
FIG. 3. Tracing
of the arteries seen RNSTOM0/5 _in Figure 2.
PLRNT/I <d
METTRTqRSRL
DOR5. PEDIS -
perfectly formed than in other subjects.The terminal tuft constitutes the only con-
stant gross anastomosis between the twodigital arteries of the four lesser toes. Thetwo arteries are, however, connected bynumerous fine transverse twigs which may
occasionally exist as a major connectionacross one or another phalanx. This is par-
ticularly true of the fifth toe (Fig. 2).The dorsal circulation is similar in its
proximal portions. The dorsalis pedis, di-rectly, or through an arctuate artery run-
ning across the middle of the dorsum, givesrise to slender dorsal metatarsal arterieswhich communicate with the plantar ar-
teries via posterior and anterior perforatingarteries situated at the proximal and distalends, respectively, of the intermetatarsalspaces. Huber found the arcuate artery per-
fectly formed in only half of his specimens.In the others the dorsal nietatarsals arose
from the plantars by continuatioin of theanterior perforating arteries. In instanceswhere the perforatiing peroneal replaces thedorsalis pedis, it supplies dorsal metatarsalbranches.
METPT/7RSPL
-LIlT PLPNTqR
PLPNTQR PPCH
The dorsal metatarsals bifurcate into ex-ceedingly slender dorsal digital arteries,which except in the great toe are usuallylost as distinct vessels before reaching theterminal tufts. Special dorsal digital arteriesto the free borders of the first and fifth toesare inconstant. Unusually they may replacethe corresponding vessels of plantar origin.
Diseased ExtremitiesGood perfusion was obtained in most
parts of the extremities, although the fluidoften had to pass through circuitous routesto bypass multiple obstructions. Truly gan-grenous parts did not fill, and this was alsotrue of some toes in which agglutinativethrombosis had apparently occurred. Ex-travasations were fairly common, especiallyabout areas of necrosis. In two cases therewas arteriovenous shunting with lack ofdistal perfusion. This will be described indetail below.Major pedal arteries. The existence of
hiigh arterial occlusion in all the limbs has
been mentioned. In all except that of thepatient with iliac embolism and femoral
Volume 150Number 2 181

Annals of SurgeryAugust 1959
FIG. 4. A. Tracing offilm from a 60-year-olddiabetic woman with deepulcer of the heel. A faintdorsalis pedis pulse waspresent. Dotted lines in-dicate occluded arteries.B. Enlarged radiograph toshow calcaneal circula-tion. Arrows indicate oc-cluded arteries.
arteriosclerosis, serious occlusion was alsodemonstrated at multiple levels in bothtibial and the peroneal arteries. This isshown by the search for a patent arterycapable of being cannulated. The dorsalispedis was found adequate in five cases, theposterior tibial in five, and the perforatingperoneal in three. In only two cases was a
second artery sufficiently patent to havebeen cannulated. Extensive occlusions were
the rule, and the distal continuity of thecannulated artery was usually interrupted,often for long spans. The tarsal and plantar
arteries and the plantar arch were frequentsites of occlusion.While all four diabetic limbs showed ex-
tremely diffuse disease, similar degrees ofinvolvement were evident in most of thenondiabetic cases.
Calcaneal circulation. Except for thecase shown in Figure 1, the heel in all othercases was deprived of one or two of itssource arteries. In only one case was it cer-
tain that the peroneal was the sole source
remaining. A fairly direct connection existedbetween the lateral tarsal and the peroneal
182 EDWARDS

V'olume 150Number 2
POSTANIPUTATION RADIOGRAPHIC EVIDENCE 183
-_ I ,~~~~~~~~~~~~~~~ ~~~~~~~~1||i..I:.|
FIG. 5. A and B. Digital circulation from same case as Figure 4. C. Schema of the proximal arterial status.Occluided vessels are shown barred.
arteries when one of these was obstructed,but the connection between the laterallyplaced and the medial calcaneal arterieswas reticular and fine.
Obstruction, usually extensive, was alsoquite regularly seen in the medial calcanealarteries, both in the diabetic and nondia-betic feet (Fig. 4, 6).
Digital circulation. Here, as in the cal-caneal territory, extensive obstructions werequite the rule, many nondiabetic feet show-ing a degree of involvement equal to thatseen in the diabetic. Obstruction involvedthe plantar arch, many of the dorsal andplantar metatarsals, the special border ar-teries of the first and fifth toes, and thetransverse anastomoses of the first (Fig. 5,7). The other digital arteries wvere occludedinfrequiently; and, except as a terminalevent, obstructions, when found, were aptto be localized,
Arteriovenous shunting. In two limbs,one from a diabetic man, the perfusing fluidpassed into the veins. In both instancessevere ischemia had followed an unsuccess-ful attempt at femoro-popliteal reconstruc-tion. In neither instance had sympathec-tomy been performed. The perforatingperoneal existed as the only source arterywhich could be cannulated. It should berecalled that this artery was similarly usedin a third case in which such shunting didnot occur. Likewise, the two cases exhibitedno other features which were recognized asunique.
In both instances the shlunting was prob-ably via numerous arteriovenous communi-cations in the tarsal and ankle regions (Fig.8). For the most part, the excessive opacityof the films precludes identification of allresponsible communications; but two suchchannels may be recognized in Figure 9.

Annals of SurgeryAugust 1959
FIG. 6. A. Tracing offilm from a 72-year-oldnondiabetic man with dif-fuse ischemia of entirefoot, and ulcers of thetoes. B. Enlarged radio-graph to show calcanealcirculation.
The physiologic consequences of theshunting are suggested by the failure ofadequate perfusion distal to the location ofthe communications.
Discussion
The similarity of findings in the diabeticand nondiabetic limbs is noteworthy, butthis is probably due in large part to the factthat only limbs coming to amputation were
studied. The findings do not negate thegeneral observation that nondiabetic ar-
teriosclerosis in particular may, in an in-dividual case, be quite well localized tosome high level of the arterial tree.A pathologic examination of some of the
sttudied extremities confirms the occlusionof arteries where indicated by the radio-graph. Further study is contemplated toelucidate the nature and mechanism of thesmall artery involvement. The obstructionsmay be due to local arteriosclerosis, butthere is a distinct possibility that athero-sclerosis at higher levels (such as the tibial)
184 EDWARDS
Af-
.;e

Volume 150Number 2
POSTAMPUTATION RADIOGRAPHIC EVIDENCE 185
F;~~~~'A ItJ ?SMiL
FIG. 7. A and B. Digital circulation from same case as Figure 6. The paucity of arteriolarfilling in the toes correlated with clinical evidence of red cell agglutinations. C. Schema ofthe proximal arterial status.
may be responsible, through distal throm-bosis, microembolism, or even through themore frequently encountered lesion of in-timal proliferation. That such proliferationwill develop distal to a point of narrowingin the arterial tree was proposed by Thomain 1911.9 Experimental evaluation of thistheory is planned.The richness of artery ramification dis-
closed in the radiographs does not provethe adequacy of the blood supply. The pathof blood supply in these cases was inter-rupted at several levels. At each level, theanastomotic connections, which are almostinvariably narrower than the occluded ves-sel, cause a reduction in pressure and flowaccording to the law of Poiseuille-that is,the flow is proportionate to the fourthpower of the radius of each vessel. The flow
suffers a further progessive lowering as itcrosses the anastomotic connections of eachsubsequent and more distal obstruction.The flow is still more reduced by the ex-cessive length of the collateral networktransversed, through the friction existingbetween the blood and the vessel wall.
It has been emphasized in previous re-ports 3 4that the circulation of some partsof a limb may be sufficiently circumscribedas to make it possible for ischemia to de-velop in that part out of proportion to thestate of the limb as a whole. The presentstudy indicates that this is true for theheel or the toes. Their soft tissue mass,moreover, is specially adapted to withstandpressure, with a structure quite distinctfrom subcutaneous tissue in general. This

EDWARDS Annals of SurgeryAugust 1959
4',
FIG. 8. Arteriovenous shunting in a limb from a 70-year-old nondiabetic man. There appearto be multiple open arteriovenous anastomoses in the tarsal region. The distal part of the footwas extremely ischemic and beginning to undergo necrosis, but frank gangrene was limitedto the toes.
has been well described for the heel byBlechschmidt.1
Clinically, ischemia of the heel or toepads results in their atrophy, with pain on
weight bearing. On examination, the partfeels flabby; and the underlying bone liesclose to the examining finger. Digital pres-
sure on the center of the heel leaves an
umbilicated appearance. Necrosis of thelimb is most often initiated in these parts.It is often preceded by cutaneous fissuring,the fissure overlying an area of infarct. Thesigns are more often seen when the specificarteries of the heel and toes are occludedthan when the disease is localized to higherarterial segments. Improvement of the cir-culatory status, especially by sympathec-tomy, is apt to restore much of the original
plumpness of the toes and, to a lesser de-gree, that of the heel.The demonstration of arteriovenous
shunting is among the few offered in thearteriosclerotic limb since Popoff's patho-logic demonstration of fibrosis and dilata-tion of the digital arteriovenous communi-cations in arteriosclerosis and Buerger's dis-ease.6 It has been shown that such shuntingdoes in fact exist during life.8
Conclusions
1. The smaller named and unnamed ar-
teries of the foot are the sites of extensiveocclusion in arteriosclerotic limbs Nvhichcome to amputation. The arteries involvedinclude the branches to both the medialand lateral parts of the heel, as well as the
186

Volume 150 POSTAMPUTATION RADIOGRAPHIC EVIDENCE 187Number 2
FIG. 9. A. Film fromsame case as Figure 8,showing detail of twoanastomoses ("anast.").B. Schema of the prox-inmal arterial status.
Jr\/_ Ai. I
FX.x1.
metatarsal arteries and those to the freeborders of the first and fifth toes. The otherdigital arteries are less frequently diseased.
2. There is no difference in the patternof occlusion between diabetic and nondia-betic feet. Occlusions were similarly aswidespread in most of the nondiabetic sub-jects as in the diabetic.
3. In two of 13 cases the postamputationinjection revealed arteriovenous shuntingtaking place at several sites in the tarsalarea. It is not known whether this phenom-enon existed in vivo.
References1. Blechschmidt, E.: Die Architektur des Fersen-
polsters. Morph. Jahr., 73:20, 1933.2. Dible, J. H.: The Pathology of Arteriosclerosis.
In Peripheral Vascular Disorders. Edited byMartin, P., R. B. Lynn, J. H. Dible and I.
Aird. Edinburgh, Livingstone, 1956.3. Edwards, E. A.: Localized Ischemis in the
Lower Extremities. G. P., 9:40, 1954.
4. Edwards, E. A.: The Anatomic Basis for Ische-mia Localized to Certain Muscles of the LowerLimb. Surg., Gynec. & Obst., 97:87, 1953.
5. Huber, J. F.: The Arterial Network Supplyingthe Dorsum of the Foot. Anat. Rec., 80:373,1941.
6. Popoff, N. W.: The Digital Vascular System.With Reference to the State of Glomus inInflammation, Arteriosclerotic Gangrene, Dia-betic Gangrene, Thromboangiitis Obliterans,and Supernumerary Digits, in Man. Arch.Path., 18:295, 1934.
7. Reiner, L., F. L. Rodriguez and F. A. Jimenez:An Injection Mass of Maximal Radiopacity forPostmortem Angiography. J. Mt. Sinai Hosp.,24:1139, 1957.
8. Ruberti, U. and Miani, A. Sindromi da deri-vazione artero-venosa della pianta del piedein corso di arteriopatia obliterante-AteneoParmense 1959.
9. Thoma, R.: Uber die Histomechanik des Gefiiss-systems und die Pathogenese der Angioskle-rose. Virchows Arch. f. path. Anat., 204:1,1911.