Embed Size (px)
Citation preview
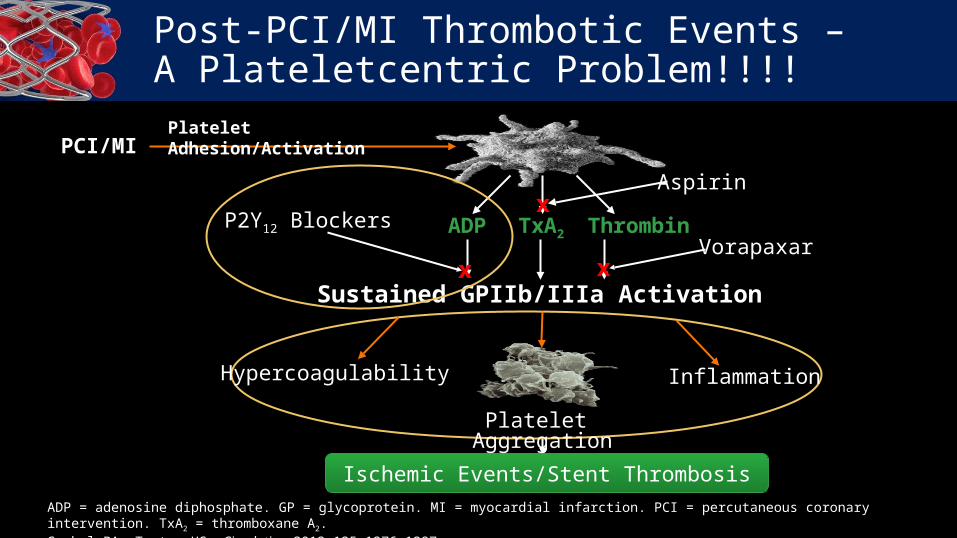
Post-PCI/MI Thrombotic Events – A Plateletcentric Problem!!!!
ADP = adenosine diphosphate. GP = glycoprotein. MI = myocardial infarction. PCI = percutaneous coronary intervention. TxA2 = thromboxane A2.Gurbel PA, Tantry US. Circulation. 2012;125:1276-1287.
Ischemic Events/Stent Thrombosis
PCI/MIPlatelet Adhesion/Activation
Platelet Aggregation
Hypercoagulability Inflammation
ThrombinADP TxA2
Sustained GPIIb/IIIa Activation
P2Y12 Blockers
xVorapaxar
x
Aspirinx
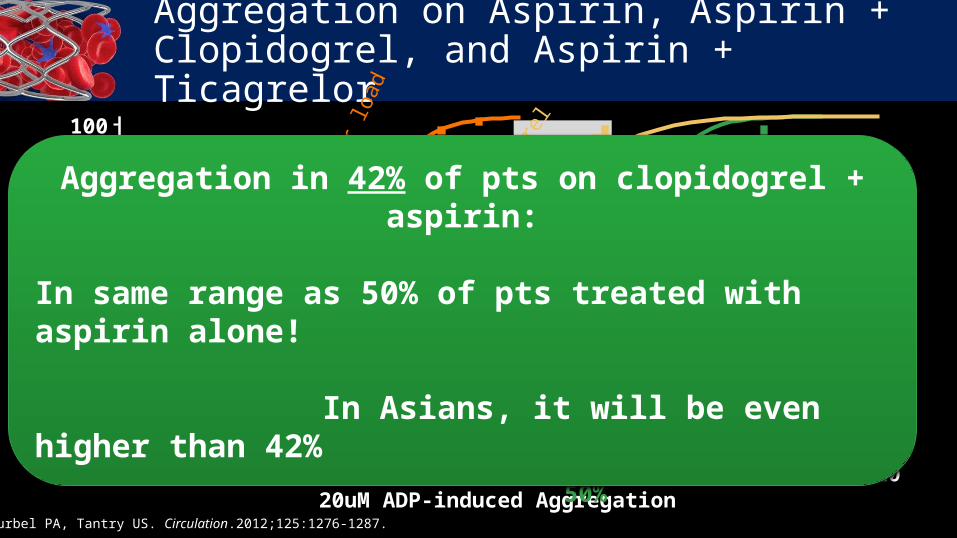
Gurbel PA, Tantry US. Circulation.2012;125:1276-1287.
0 20 40 60 80 100 12020uM ADP-induced Aggregation
100
80
60
40
20
0
Cu
mu
lati
ve F
req
uen
cy (
%)
42%
50%
Asp
irin
75-1
00 m
g Q
D
8 hr
s po
st-6
00 m
g cl
opid
ogre
l
Aggregation on Aspirin, Aspirin + Clopidogrel, and Aspirin + Ticagrelor
8 hr
s po
st-1
80 m
g tic
agre
lor l
oad
Aggregation in 42% of pts on clopidogrel + aspirin:
In same range as 50% of pts treated with aspirin alone!
In Asians, it will be even higher than 42%
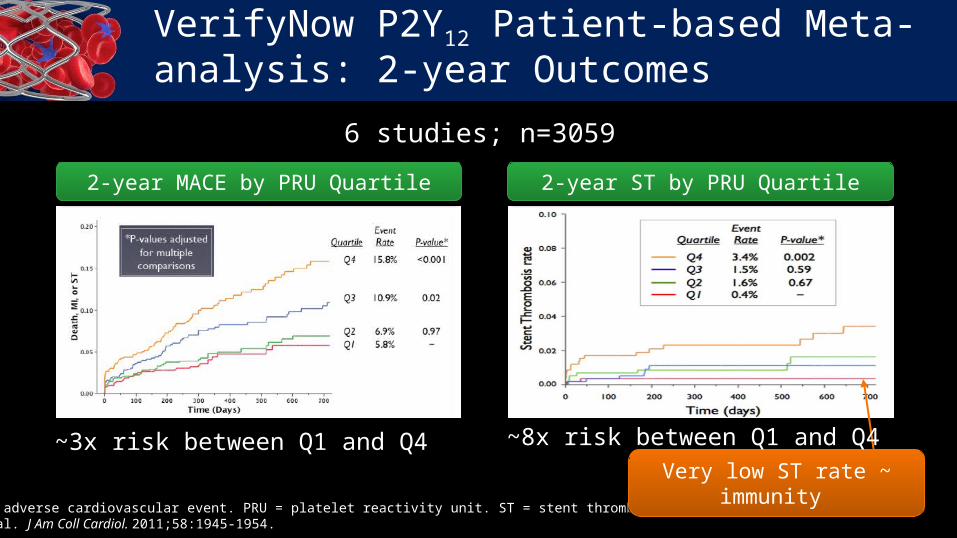
2-year MACE by PRU Quartile
MACE = major adverse cardiovascular event. PRU = platelet reactivity unit. ST = stent thrombosis. Brar SS, et al. J Am Coll Cardiol. 2011;58:1945-1954.
2-year ST by PRU Quartile
Very low ST rate ~ immunity
6 studies; n=3059
~3x risk between Q1 and Q4 ~8x risk between Q1 and Q4
VerifyNow P2Y12 Patient-based Meta-analysis: 2-year Outcomes
Gurbel PA, et al. J Am Coll Cardiol. 2007;50:1822-1834. Gurbel PA, et al. Am Heart J. 2010;160:346-354. Campo G, et al. J Am Coll Cardiol. 2011;57:2474-2483. Jeong YH, et al. Presented at: European Society of Cardiology Congress 2011; August 27-31, 2011; Paris, France. Gurbel PA, et al. Thromb Haemost. 2011;106:263-264. Sibbing D, et al. Thromb Haemost 2010;103:151-159. Sibbing D, et al. J Thromb Haemost. 2010;8:250-256.
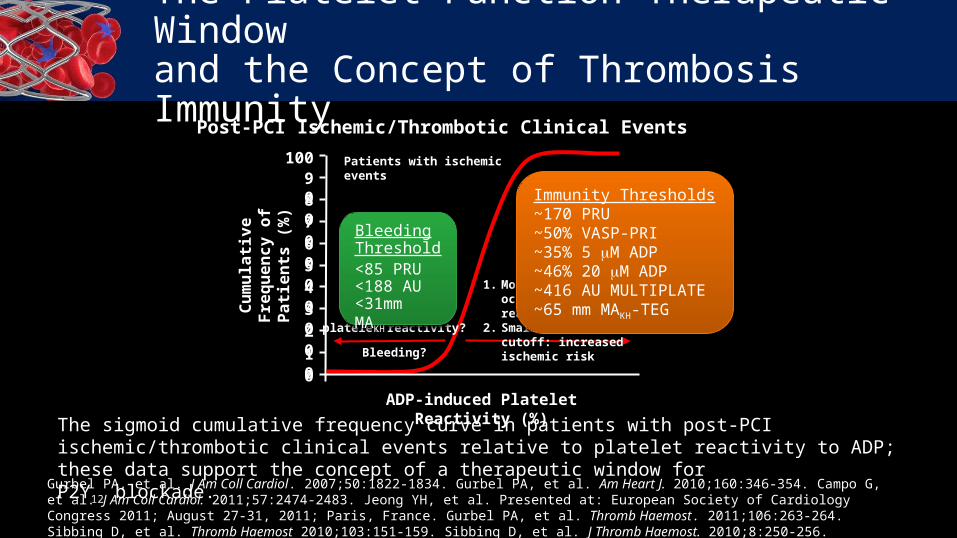
The Platelet Function Therapeutic Window and the Concept of Thrombosis Immunity
The sigmoid cumulative frequency curve in patients with post-PCI ischemic/thrombotic clinical events relative to platelet reactivity to ADP; these data support the concept of a therapeutic window for P2Y12 blockade.
Post-PCI Ischemic/Thrombotic Clinical Events
Cu
mu
lati
ve
Fre
qu
en
cy
o
f P
ati
en
ts (
%)
ADP-induced Platelet Reactivity (%)
010
2030405060708090
100
Too lowplatelet reactivity?
Bleeding?
1. Most ischemic events occur above a platelet reactivity cutoff
2. Small increase above cutoff: increased ischemic risk
Patients with ischemic events
Bleeding Threshold
<85 PRU<188 AU<31mm MAKH
Immunity Thresholds~170 PRU~50% VASP-PRI~35% 5 M ADP~46% 20 M ADP~416 AU MULTIPLATE~65 mm MAKH-TEG
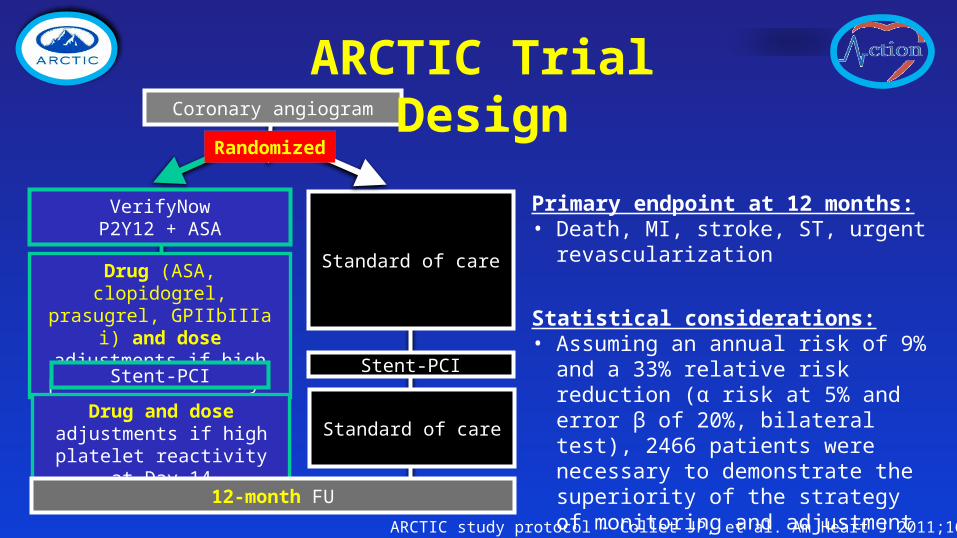
Standard of care
VerifyNow P2Y12 + ASA
Drug (ASA, clopidogrel, prasugrel, GPIIbIIIa i) and dose adjustments if high
platelet reactivity
Coronary angiogram
Stent-PCI
Randomized
Standard of careDrug and dose adjustments
if high platelet reactivity at Day 14
12-month FU
Stent-PCI
ARCTIC Trial Design
Primary endpoint at 12 months:• Death, MI, stroke, ST, urgent
revascularization
Statistical considerations:• Assuming an annual risk of 9% and a
33% relative risk reduction (α risk at 5% and error β of 20%, bilateral test), 2466 patients were necessary to demonstrate the superiority of the strategy of monitoring and adjustment
ARCTIC study protocol - Collet JP, et al. Am Heart J 2011;161:5-12
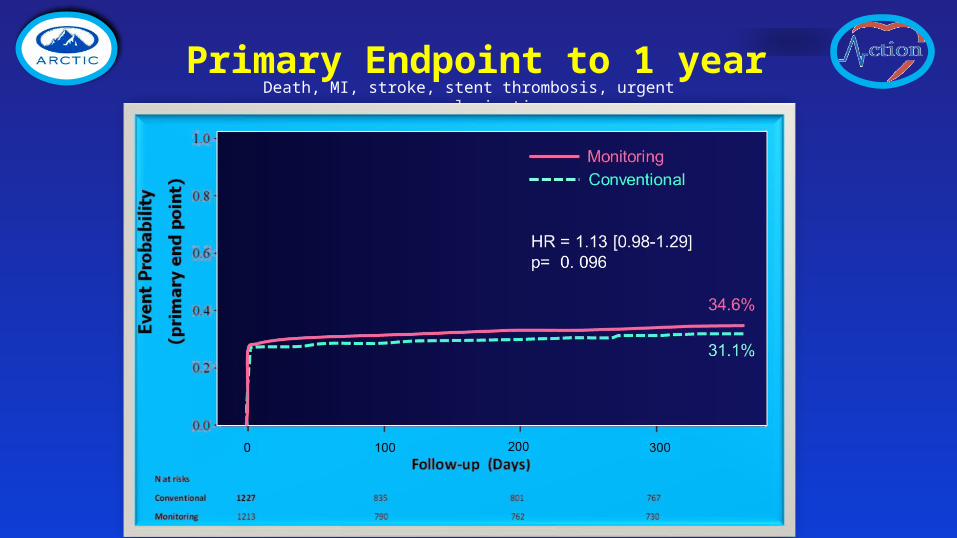
Primary Endpoint to 1 yearDeath, MI, stroke, stent thrombosis, urgent revascularization
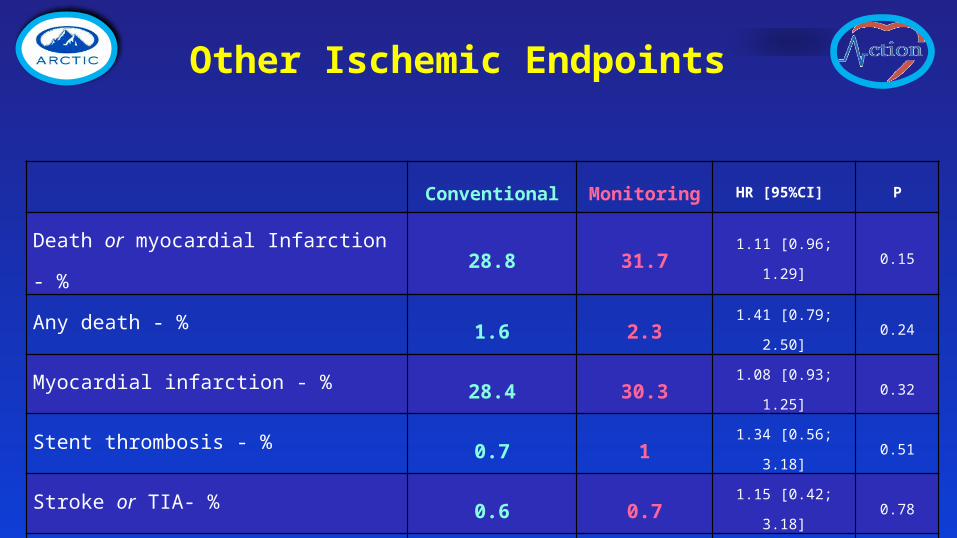
Conventional Monitoring HR [95%CI] P
Death or myocardial Infarction - % 28.8 31.7 1.11 [0.96; 1.29] 0.15
Any death - % 1.6 2.3 1.41 [0.79; 2.50] 0.24
Myocardial infarction - % 28.4 30.3 1.08 [0.93; 1.25] 0.32
Stent thrombosis - % 0.7 1 1.34 [0.56; 3.18] 0.51
Stroke or TIA- % 0.6 0.7 1.15 [0.42; 3.18] 0.78
Urgent revascularization - % 4.2 4.5 1.06 [0.73; 1.55] 0.76
Other Ischemic Endpoints
Conventional Monitoring HR [95%CI] P
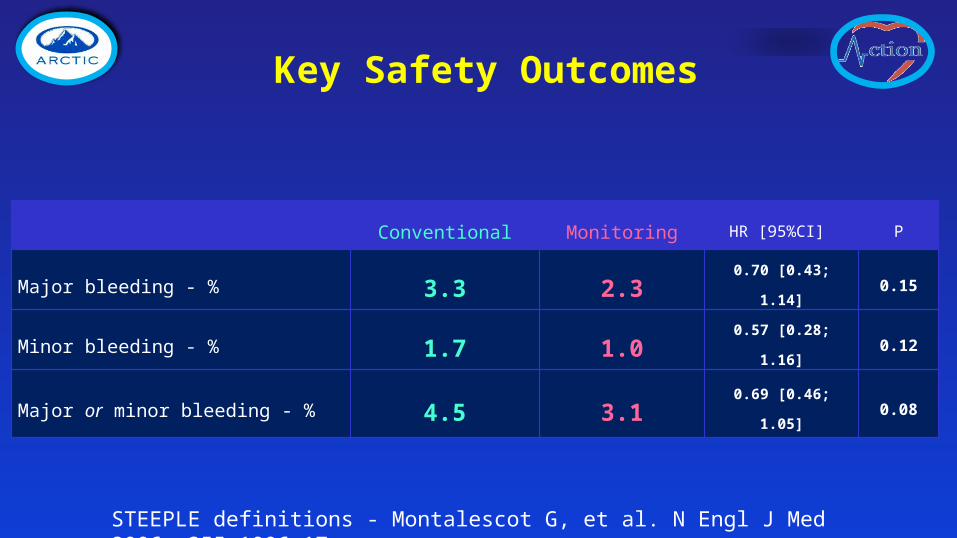
Major bleeding - % 3.3 2.3 0.70 [0.43; 1.14] 0.15
Minor bleeding - % 1.7 1.0 0.57 [0.28; 1.16] 0.12
Major or minor bleeding - % 4.5 3.1 0.69 [0.46; 1.05] 0.08
Key Safety Outcomes
STEEPLE definitions - Montalescot G, et al. N Engl J Med 2006; 355:1006–17
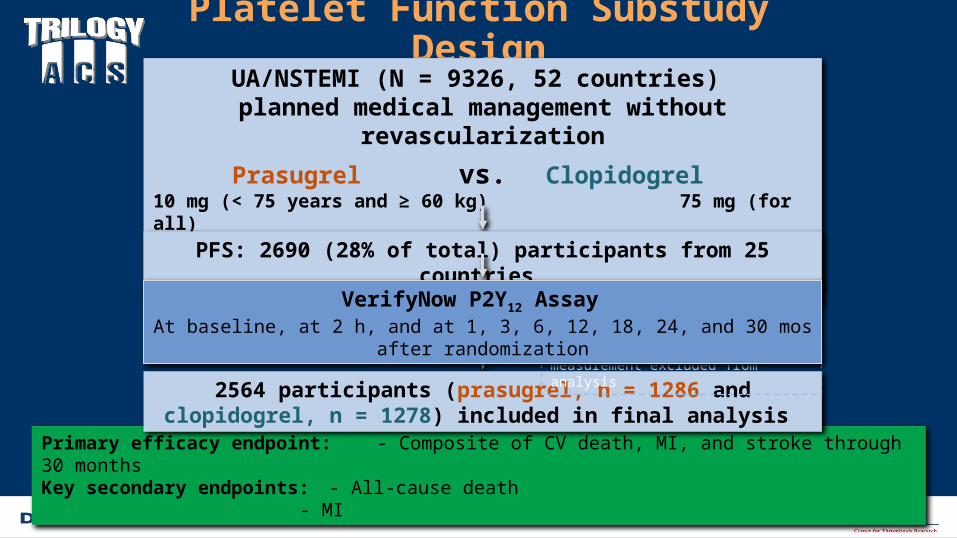
Platelet Function Substudy DesignUA/NSTEMI (N = 9326, 52 countries)
planned medical management without revascularization
Prasugrel vs. Clopidogrel 10 mg (< 75 years and ≥ 60 kg) 75 mg (for all)5 mg (≥ 75 years; < 75 years and < 60 kg)
Aspirin ≤ 100 mg (strongly recommended) for allPFS: 2690 (28% of total) participants from 25 countries
Primary efficacy endpoint: - Composite of CV death, MI, and stroke through 30 monthsKey secondary endpoints: - All-cause death
- MI
2564 participants (prasugrel, n = 1286 and clopidogrel, n = 1278) included in final analysis
126 without valid PRU measurement excluded from analysis
VerifyNow P2Y12 Assay At baseline, at 2 h, and at 1, 3, 6, 12, 18, 24, and 30 mos after randomization
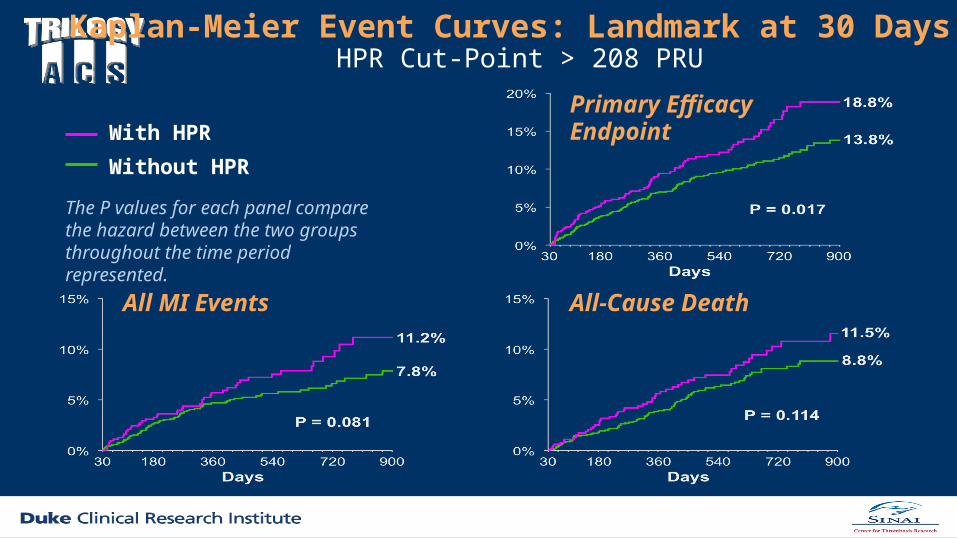
Kaplan-Meier Event Curves: Landmark at 30 Days HPR Cut-Point > 208 PRU
The P values for each panel compare the hazard between the two groups throughout the time period represented.
All MI Events All-Cause Death
Primary Efficacy Endpoint With HPR
Without HPR
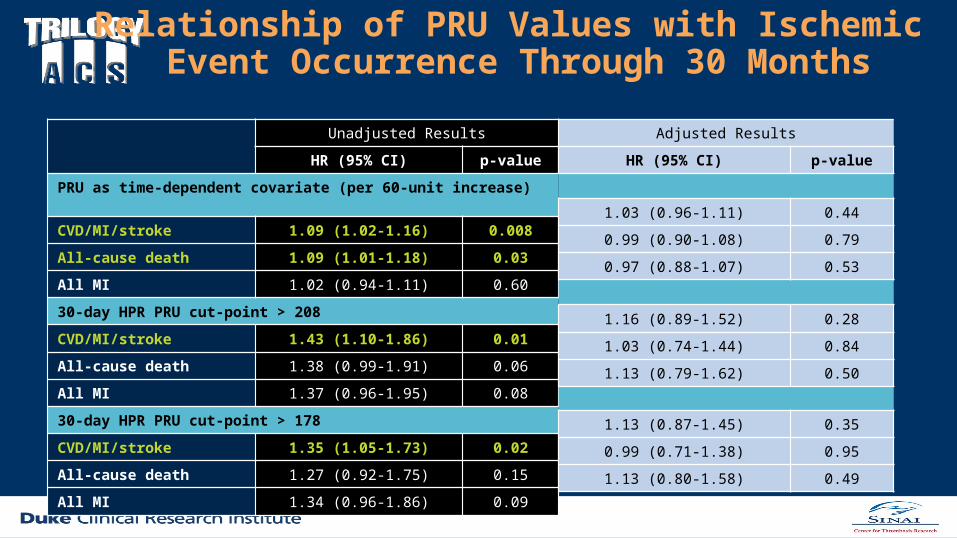
Relationship of PRU Values with Ischemic Event Occurrence Through 30 Months
Unadjusted Results
HR (95% CI) p-value
PRU as time-dependent covariate (per 60-unit increase)
CVD/MI/stroke 1.09 (1.02-1.16) 0.008
All-cause death 1.09 (1.01-1.18) 0.03
All MI 1.02 (0.94-1.11) 0.60
30-day HPR PRU cut-point > 208
CVD/MI/stroke 1.43 (1.10-1.86) 0.01
All-cause death 1.38 (0.99-1.91) 0.06
All MI 1.37 (0.96-1.95) 0.08
30-day HPR PRU cut-point > 178
CVD/MI/stroke 1.35 (1.05-1.73) 0.02
All-cause death 1.27 (0.92-1.75) 0.15
All MI 1.34 (0.96-1.86) 0.09
Adjusted Results
HR (95% CI) p-value
1.03 (0.96-1.11) 0.44
0.99 (0.90-1.08) 0.79
0.97 (0.88-1.07) 0.53
1.16 (0.89-1.52) 0.28
1.03 (0.74-1.44) 0.84
1.13 (0.79-1.62) 0.50
1.13 (0.87-1.45) 0.35
0.99 (0.71-1.38) 0.95
1.13 (0.80-1.58) 0.49





























