-
7/30/2019 Post Natal Pulmonary Adaptations
1/14
Respiratory Physiology & Neurobiology 158 (2007) 190203
Postnatal cardiopulmonary adaptations to high altitude
Luis Huicho a,b,c,
a Departamento Acad emico de Pediatra, Universidad Nacional
Mayor de San Marcos, Lima, Perub Universidad Peruana Cayetano
Heredia, Lima, Peru
cInstituto de Salud del Nino, Lima, Peru
Accepted 1 May 2007
Abstract
Postnatal cardiopulmonary adaptations to high altitude
constitute a key component of any set of responses developed to
face high altitude
hypoxia. Such responses are required ultimately to meet the
energy demands necessary for adequate functioning at cell and
organism level.After a brief insight on general and cardiopulmonary
comparative studies in growing and adult organisms, differences and
possible explanations
for varying cardiopulmonary pathology, pulmonary artery
hypertension, persistent right ventricular predominance and
subacute high altitude
pulmonary hypertension in different populations of children
living at high altitude are discussed. Potential long-term
implications of early chronic
hypoxic exposure on later diseases are also presented. It is
hoped that this review will help the practicing physician working
at high altitude
to make informed decisions concerning individual pediatric
patients, specifically with regard to diagnosis and management of
altitude-related
cardiopulmonary pathology. Finally, plausibility and the
knowledge-base of public health interventions to reduce the risks
posed by suboptimal or
inadequate postnatal cardiopulmonary responses to high altitude
are discussed.
2007 Elsevier B.V. All rights reserved.
Keywords: Cardiopulmonary adaptations; High altitude;
Postnatal
1. Introduction
Animals living in diverse settings but facing hypoxia/anoxia
as a common factor constitute ideal models for studying dif-
ferent response patterns (Hochachka and Lutz, 2001). In
brief,
one fundamental lesson learned from comparative studies in
organisms naturally or experimentally exposed to low oxygen
is that there are species able to withstand hypoxia (hypoxia
tolerant) and species that are not equipped to face success-
fully the hypoxic challenge for achieving optimal
functioning
and survival (hypoxia sensitive). Hypoxia-tolerant and
hypoxia-
sensitive are terms used for referring to these two categories
of
animal species (Hochachka and Lutz, 2001). These two cate-
gories of animals are also referred to as genetically
adapted
and non-genetically adapted species to high altitude hypoxia
(Monge and Leon-Velarde, 1991). We will use both set of
terms interchangeably throughoutthe review, although the
genes
accounting for the different strategies developed by both
groups
Correspondence address: Batallon Libres de Trujillo227, LI 33,
Lima,Peru.
Tel.: +51 1 93481121; fax: +51 1 3190019.
E-mail address: [email protected].
of species have not been entirely demonstrated and thereforethe
first classification is probably more cautious, as it may
include both genetic and functional changes. The responses
to
hypoxia assessed in such comparative studies range from the
whole organism to sub-cellular and molecular responses. They
include at least the following levels, as proposed by
Hochachka
et al. (1998): regulation of hypoxic ventilatory response
(HVR)
by carotid body chemoreceptors, oxygen sensors at pulmonary
vasculature that regulate the hypoxic vasoconstrictor
response
and the ventilation-perfusion matching, oxygen sensors in
other
tissues involved in the activation of the vascular
endothelial
growth factor and thus the angiogenesis especially in the
heart
and probably in the brain, and oxygen sensors in the kidney
and
liver involved in an enhanced erythropoietin expression.
Finally,
there are tissue-specific oxygen sensing and signal
transduction
pathways that lead to metabolic reorganization at least in
part
by altering the expression rates of hypoxia-sensitive genes
for
metabolic enzymes and metabolic transporters.
At the sub-cellular and molecular level, the metabolic effi-
ciency of genetically adapted animals is higher than that of
non-genetically adapted ones. There are several mechanisms
by
which hypoxia-tolerant animals resolve the challenges posed
by hypoxic environments, but metabolic arrest and stabilized
1569-9048/$ see front matter 2007 Elsevier B.V. All rights
reserved.
doi:10.1016/j.resp.2007.05.004
mailto:[email protected]://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.resp.2007.05.004http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.resp.2007.05.004mailto:[email protected]
-
7/30/2019 Post Natal Pulmonary Adaptations
2/14
L. Huicho / Respiratory Physiology & Neurobiology 158 (2007)
190 203 191
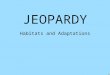
Fig. 1. From the cell to the organism: several fundamental
features of cells tolerant to hypoxia and of cells sensitive to
hypoxia-implications of programming and of
modifying factors on resulting overall organism-level responses
(successful adaptation or non-adaptation). Modified from Hochachka
(1986). AMS: acute mountain
sickness; HAPE: high altitude pulmonary edema; HACE: high
altitude cerebral edema; CMS: chronic mountain sickness, CSHAPH:
chronic symptomatic high
altitude pulmonary hypertension.
membrane functions appear to be the most effective
strategies
for extending tolerance to hypoxia (Hochachka, 1986).
Depend-
ing on whether the organism is tolerant or sensitive to
hypoxia,
early exposure to chronic hypoxia and intervention of risk
fac-
tors may alter to a varying degree early programming events
at
the cellular level and lead to a final successful or
non-successful
pattern of adaptation at the organism level (Fig. 1).A
conceptual summary of the relationships between time
and physiological responses to hypoxia and the ancestral
phys-
iological phenotype as a phylogenetic adaptation to
hypobaric
hypoxia is seen in Fig. 2. This conceptual model of
responses
was taken from Hochachka et al., who discussed them in
detail
in several reviews (Hochachka, 1986; Hochachka et al., 1998;
Rupert and Hochachka, 2001a, 2001b). We added concepts
most likely present in Hochachkas propositions but not
explic-
itly included in his model, namely: (1) the determinant role
of
the genetic background, which leads ultimately to an
adaptive
or non-adaptive set of responses to hypoxia, (2) the
potential
role of important modifying factors (life style, environmen-
tal and indoor pollution, and chronic respiratory diseases),
and
(3) the notion of programming, that is, the possible
long-term
indirect effects that poverty, malnutrition and other
environmen-
tal agents can exert on the responses to hypoxia in the
fetal
and early postnatal vulnerable periods of life. Programming
and modifying/risk factors were incorporated in the model as
important modulators of different steps from signal
transductiononwards. All such modifying effects can change
substantially
the genetic expression of both acute and long-term
responses.
Acute responses to hypoxia occur instantaneously with the
hypoxic exposure, whereas adjustments requiring hours to
days
are termed acclimatory responses or acclimation. We also
included the concept of long-term responses to imply that
they
can take the whole life of an individual. Only acute and
acclima-
tory responses are possible within a given generation.
However,
all components of the cascade of responses can change
through
evolutionary time (genetic adaptation), changes that involve
genetic alterations. Andean, Tibetan and Ethiopian
populations
show three different patterns of adaptation to high altitude
-
7/30/2019 Post Natal Pulmonary Adaptations
3/14
192 L. Huicho / Respiratory Physiology & Neurobiology 158
(2007) 190203
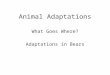
Fig. 2. Relationship between time of exposure to hypoxia and
physiological responses. Acute responses are those occurring
instantaneously with the hypoxic
exposure. Adjustments requiring some fraction of the life of
organisms are termed acclimatory responses and they were extended
here to so-called long-term
responses to imply that they can take the whole life of an
individual. Only acute and acclimatory responses are possible
within a given generation. All components
of the cascade can change through evolutionary time
(phylogenetic adaptation or genetic adaptation), changes that
involve genetic alterations. Andean, Tibetan and
Ethiopian human populations are includedas examples of
differentpatterns of adaptation to highaltitude hypoxia. Besides
genetic adaptationas a resultingsuccessful
set of responses, acute and long-term non-adaptive strategies
resulting in several conditions are included. Programming and
modifying/risk factors were incorporated
as important modulators of different steps from signal
transduction onwards. Modified from Hochachka et al. (1998). AMS:
acute mountain sickness; HAPE:
high altitude pulmonary edema; HACE: high altitude cerebral
edema; CMS: chronic mountain sickness; CSHAPH: chronic symptomatic
high altitude pulmonary
hypertension.
hypoxia and therefore show different phenotypes of SaO2 and
eryhtropoiesis. Besides genetic adaptation as a successful
set
of responses, we included acute and long-term non-adaptive
strategies resulting in several conditions. The resulting
acute
non-adaptive responsesinclude acutemountainsickness(AMS),
high altitude pulmonary edema (HAPE), and high altitude
cere-
bral edema (HACE). On the other hand, non-adaptive responses
to long-term exposure may lead to chronic mountain sickness
(CMS)and chronic symptomatic high altitude pulmonary hyper-
tension (CSHAPH).
Studies on Andean, Tibetan andEthiopian high altitude
popu-lations have revealed different patterns of adaptation to
hypoxia.
Andean natives show erythrocytosis and hypoxemia, and may
also develop pulmonary artery hypertension (Monge, 1978;
Winslow and Monge, 1978). Moreover, CMS may result from
an excessively enhanced erythropoietin response (Monge,
1978;
Winslow and Monge, 1978). Tibetans show consistently low
oxygen saturation and lack of enhanced erythropoiesis
(Beall,
2000, 2006). Recently, in Ethiopia, a third successful
pattern
of human adaptation to high altitude hypoxia that contrasts
with
both the Andean and the Tibetan patterns was described(Beall
et
al., 2006). In Ethiopian native residents at 3530 m, 1486
years
of age, without evidence of iron deficiency,
hemoglobinopathy,
or chronic inflammatory conditions, they found that
hemoglobin
concentration and arterial oxygen saturation were within the
ranges of sea level populations, despite the ambient hypoxia
(Beall et al., 2002). The understanding of the underlying
mech-
anisms leading to these differences is not complete.
Although
it is plausible that they are due to genetic differences in
the
strategies for facing hypoxia, the genes involved, their
transmis-
sion patterns and their distribution among and within
different
populations are not clear (Beall et al., 2002; Brutsaert,
2001).
The effect of environmental factors other than hypoxia and
the
interaction of hypoxia with genetic variables on the patternsof
adaptation are aspects also waiting for further clarification
(Moore, 2001; Rupert and Hochachka, 2001a, 2001b).
In the following sections we will discuss whether there
are similar population differences in developmental
cardiopul-
monary adaptation patterns to high altitude hypoxia. We will
offer first a brief physiological overview on
cardiopulmonary
responses to hypoxia, particularly on the reactivity of the
pulmonary artery. We will then discuss from a comparative
perspective the responses of growing and adult organisms,
and
follow this with a discussion of cardiopulmonary responses
in
human infants andchildrenliving at high altitude.In thefinal
sec-
tions we will comment on the possible long-term effects of
early
-
7/30/2019 Post Natal Pulmonary Adaptations
4/14
L. Huicho / Respiratory Physiology & Neurobiology 158 (2007)
190 203 193
hypoxic exposure on the health status in later life and
whether
there is a sound knowledge-base for drawing clinical and
health
policy recommendations regarding exposure of children to
life
at high altitude.
2. Comparative cardiopulmonary responses to high
altitude hypoxia in developing and adult organisms
2.1. Physiological significance of cardiopulmonary
responses to hypoxia
A particular challenge that hypoxic exposure presents to the
lungs is that they should overcome any existing limitation
to
gas exchange so as to ensure that blood equilibrate
completely
with alveolar oxygen pressure. Three physiological
mechanisms
that may act as limiting factors to an efficient gas
exchange
have been described: intrapulmonary shunts, diffusion
limita-
tions and ventilation to perfusion heterogeneity (Scheid and
Piiper, 1997; Skovgaard and Wang, 2006). Pulmonary vascular
reactivity is fundamental in the reduction of the ventilation
toperfusion heterogeneity by means of a constrictive response
that
is variable from species to species. Hypoxic pulmonary vaso-
constriction (HPV) is considered a widely conserved adaptive
vasomotor response to alveolar hypoxia, which distributes
pul-
monary blood flow to optimally ventilated lung segments by a
process of vasoconstriction whichspecifically involves the
small
muscular pulmonaryarteries (Moudgil et al., 2005).
Itthusmedi-
ates ventilation-perfusion matching by reducing shunt
fraction
optimizing in this waysystemic oxygenpressure (Moudgil et
al.,
2005). On exposure to hypoxia, the primary site of
vasoconstric-
tion is the precapillary muscular pulmonary and low alveolar
oxygen leads to constriction of the pulmonary vasculature
inbirds and mammals which elevates resistance to pulmonary
blood flow and leads to a rise in pulmonary arterial blood
pres-
sure (Skovgaard and Wang, 2006; Moudgil et al., 2005). In
the systemic vessels, in contrast, hypoxia dilates most
systemic
arteries in both animals and humans. These differing
responses
of pulmonary and systemic arteries to hypoxia indicate that
HPV,
although modulatedby the endothelial cells, cannot be
explained
by endocrine or paracrine vasoconstrictors that have concor-
dant effects on the pulmonary and systemic circulation such
as
endothelin and leukotrienes (Moudgil et al., 2005). It is
believed
that the restricted occurrence of HPV to intrapulmonary
arteries
reflects the localization of the molecular apparatus that
mediates
HPV, namely the mitochondrial redox sensor and the
effectors(O2-sensitive K
+ channels in pulmonary artery smooth muscle
cells) to the resistance pulmonary arteries (Moudgil et al.,
2005).
This seductive hypothesis should be verified through the
con-
duction of studies aimed at developing organ-specific
designs
for assessing in different species developmental responses
to
hypoxia within the framework of an overall, integrative con-
ception of adaptation. Also, the hypothesis paves the way
for
focusing the study of hypoxic adaptive responses of animals
and humans exposed chronically to high altitude hypoxia on
the
mitochondrial level in pulmonary artery smooth muscle cells,
and also for understanding better the genetic aspects of
such
responses. Fig. 3 shows a diagrammatic summary of the cas-
cade of responses elicited at pulmonary vasculature level
when
organisms are challenged by hypoxia. The genetic background
provides the basis of the response, although pulmonary
vascu-
lar reactivity resulting from hypoxia sensing may be
modified
by programming during early intrauterine or extrauterine
life
periods. This leads to successful long-term vascular
pulmonary
adaptation or to non-adaptive long-term responses that can
be
ultimately manifested in chronic and symptomatic high
altitude
pulmonary hypertension.
2.2. Cardiopulmonary responses in young organisms
There is a paucity of research performed on cardiopulmonary
responses to high altitude hypoxia in growing animals. A
com-
prehensive review made on physiological adaptations to high
altitudein1991(Mongeand Leon-Velarde, 1991) concludedthat
animals tolerant to hypoxia such as guinea-pigs, when
studied
during growth, show a lower degree of ventricular
hypertrophy
and pulmonary artery hypertension than growing rats, consid-
ered hypoxia-sensitive animals. Unfortunately, the prenatal
andpostnatal time-course of such responses in humans is
fundamen-
tally unknown, though there are critical periods during
prenatal
and early postnatal growth. If growing organisms are exposed
to certain factors such as under-feeding during these
critical
periods, they may be programmed for later development of
dis-
eases such as ischemic heart disease, diabetes, hypertension,
and
stroke (Barker, 2002).
As for the more general problem of early exposure to diverse
agentsduring critical periods of lung developmentand
thesubse-
quent risk of developing cardiorespiratory diseases later in
life,
as well as the underlying molecular mechanisms, this is a
largely
neglected area and more uncertainties than definitive
answersstill prevail (Massaro and DeCarlo Masaro, 2004). Fig. 4
depicts
the different stages of human lung development and shows
pre-
sumably vulnerable periods that may be affected by exposure
to
several agents including hypoxia. There are clearly
compelling
examples of late consequences of early events, such as
intrauter-
ine and postnatal exposure to parental tobacco smoking and
later risk in adulthood for more respiratory symptoms,
poorer
lung function, and increased risk for obstructive pulmonary
dis-
ease (Hafstrom et al., 2005; Harding et al., 2000; Maritz et
al.,
2005; Svanes et al., 2004). A recent publication by Le Cras et
al.
(2004) synthesized divergent studies about transforming
growth
factor-alpha (TGF-) pointing to its overexpression in
important
developmental and adult pulmonary diseases and showed thatbrief
overexpression of TGF- by the lung, if produced when
the gas-exchange saccules of the architecturally immature
lung
are beingsubdivided (septated)to form alveoli, permanently
dis-
rupts septation. Their results support the existence of a
critical
period for septation and for the formation of the pulmonary
vas-
culature and provide additional evidence that early events
can
influence laterlung anatomy, lung function,and the
development
of lung disease. Importantly, this work also points to the
impact
early events have on the subsequent development of lung
disease
and adds to our still poor understanding of the molecular
basis
of this effect (Svanes et al., 2004). Of interest, in all
species
studied so far septation, whether prenatal or postnatal,
occurs
-
7/30/2019 Post Natal Pulmonary Adaptations
5/14
194 L. Huicho / Respiratory Physiology & Neurobiology 158
(2007) 190203
Fig. 3. Pulmonary vasculature set of responses in conditions of
chronic exposure to hypoxia. A hierarchical approach is proposed
where the genetic endowment is
determinant in the way organisms respondto hypoxia at the
pulmonary vasculature level. Earlyexposure to chronic hypoxiaand
participationof modifying/risk factors
may significantly alter the responses, which may therefore lead
to increased or normal pulmonary vasculature resistance and
pressure, successful or inadequate blood
flow redistribution to optimally ventilated lung regions,
reduction or inadequately persistent shunt fractions, improvement
or not in ventilation-perfusion matching,
and eventually to maintenance or not of optimum systemic oxygen
pressure. The global resulting responses may signify a successful
long-term pulmonary adaptation
or a non-adaptive set of responses leading to chronic
symptomatic high altitude hypertension. NO: nitric oxide; ET-1:
endothelin-1; LKs: leukotrienes; CSHAPH:
chronic symptomatic high altitude pulmonary hypertension; PAP:
pulmonary artery pressure.
during a period when the organisms blood concentration of
its
major glucocorticosteroid hormone is low; septation ends as
the
glucocorticosteroid concentration rises (Massaro and DeCarlo
Masaro, 2004). Administration of a glucocorticosteroid to ratsor
mice during the period of septation, when the concentration of
corticosteroids in the bloodis normally low, impairs
spontaneous
septation and the development of the pulmonary vasculature,
resulting in pulmonary hypertension (LeCras et al., 2000).
Peri-
natal exposure to hypoxia may also affect septation and pave
the
way for later development of pulmonary hypertension (Blanco
et al., 1991; Massaro et al., 1990). However, most
experimen-
tal evidence on vulnerable periods comes currently from
animal
studies, and we should therefore be cautious in
extrapolating
those results to human lung development, as the critical
peri-
ods seem to vary from species to species and in addition
there
are gender differences. Moreover, the time-period of
vulnera-
bility is still nebulous for several specific phases of human
lung
development and more research is needed before we can derive
sound recommendations on early preventive interventions. We
will be back with this issue later in the review describingmore
evidence pointing to possible associations between events
occurring early in life and the risk of developing specific
lung
disorders.
It would be particularly illuminating to have comparative
studies on the ontogenetic characteristics of
cardiopulmonary
responses to chronic high altitude hypoxia in
hypoxia-sensitive
and hypoxia-tolerant species. They offer the potential to
reveal
possible critical periods during early phases of cardiopul-
monary growth and development in conditions of hypoxia and
their relationship with adult fitness to hypoxia in general
and
with the risk of developing later persistent cardiopulmonary
pathology including symptomatic high altitude pulmonary
-
7/30/2019 Post Natal Pulmonary Adaptations
6/14
L. Huicho / Respiratory Physiology & Neurobiology 158 (2007)
190 203 195
Fig. 4. Prenatal and postnatal periods of lung development and
the notion of critical periods. Rectangles with black areas denote
greater vulnerability (critical
periods) whereas those with grey areas denote lower
vulnerability. Programming is more likely to occur during critical
periods leading thus to various diseases later
during infancy, childhood or adulthood. Proposed period times of
vulnerability of specific stages of lung development to diverse
agents are only approximations
and some of them may not be fully applicable to human beings.
Gender variations also occur. Critical periods may include prenatal
phase, postnatal phase or both
intrauterine and extrauterine phases. Vertical and oblique
arrows on different developmental lung stages indicate modulatory
effects of diverse molecules, such as
growth factors. AB: antibiotics; IGF: insulin-like growth
factor; EGF: epidermal growth factor; TGF-: transforming growth
factor .
hypertension. Such studies may also identify potential
targets
for proving therapeutic options and for implementing
preventive
interventions.
2.3. Cardiopulmonary response in adult organisms
In contrast, studies on cardiopulmonary responses to hypoxia
in adult animals are numerous. For a detailed discussion of
the issue we refer the reader to a comprehensive review pub-
lished in 2001 (Tucker and Rhodes, 2001). In that review,
the
authors distinguish the findings in animals indigenous to
low
altitude from those in animals native to high altitude. Two
patterns of cardiopulmonary response have been consistently
shown in low altitude animals. Species such as sheep and
goat
show a hypo-responsive pattern characterized by low thick-ness
of the pulmonary vessels, absent or mild pulmonary artery
hypertension, and mild to moderate right ventricular
hypertro-
phy. Hyper-responder animals such as cows show comparatively
higher thickness of pulmonary arteries, moderate to severe
pul-
monary hypertension and marked rightventricular
hypertension.
In addition,animals native to high altitude such as yaks,
camelids
(llamas, alpacas, guanacos) and rodents and lagomorphs
(guinea
pigs, viscachas, pikas) show consistently less variable,
attenu-
ated pulmonary hypertensive responses with little pulmonary
vascular hypertrophy and right ventricular hypertrophy. This
attenuated response is also apparent among human high alti-
tude populations, particularly in Tibetan populations. In brief,
it
seems that medial pulmonary artery thickness predicts the
pul-
monary vascular response to high altitude (Tucker and
Rhodes,
2001).
These findings strongly suggest that the cardiopulmonary
responses to high altitude hypoxia are genetically driven.
This
does not deny at all the influence of geneenvironment inter-
actions or the role of developmental adaptation, whose
relative
importance in the context of a successful adaptation as
compared
to the purely genetic influence needs to be studied.
3. Humans: cardiopulmonary changes in high altitude
infants and children
A basic auxiologic concept universally accepted is that
chil-
dren need an adequate environment to reach an
optimum,unrestricted growth and development. Accordingly, there is
a
justified concern on the potential influence of high
altitude
hypoxia on growth and development of children living in such
settings. Ultimately, oxygen availability to tissues should be
the
minimal needed for matching the metabolic demands of a grow-
ing organism. Alternatively, an increased metabolic
efficiency
in face of limited oxygen availability is a plausible
overcoming
strategy. Since cardiovascular and respiratory systems
constitute
key steps in the oxygen cascade they deserve a particular
con-
sideration in a review on their responses in children living
under
hypoxic conditions. We will focus here on studies performed
in
children with long-term exposure to high altitude.
-
7/30/2019 Post Natal Pulmonary Adaptations
7/14
196 L. Huicho / Respiratory Physiology & Neurobiology 158
(2007) 190203
From a more specific perspective,we examine howcardiopul-
monary development occurs in children resident at high
altitude
andhow this mayinfluencethe risk of persistence of fetal
circula-
tory patterns (patent foramen ovale and patent ductus
arteriosus),
as well as of symptomatic pulmonary hypertension with con-
sequent right-heart failure. These concerns are reflected in
the
published literature (Alzamora Castro et al., 1960; Khoury
and
Hawes, 1963; Hurtado Gomez and Calderon, 1965; Lin and Wu,
1974; Miao et al., 1988; Sui et al., 1988).
3.1. Cardiopulmonary transitional changes in the high
altitude infant
In a comprehensive review of early postnatal transitional
cardiopulmonary changes in infants living at high altitude
it
was emphasized there that the immediate postnatal period is
a
dynamic one, with continuous developmental changes in virtu-
ally every aspect of the cardiopulmonary system (Niermeyer,
2003). Such changes involve alveolar structure, pulmonary
blood flow, circulatory patterns, central nervous system
controlof breathing, regulation by peripheral chemoreceptors,
inputs
from metabolic rate and thermoregulation, hemoglobin synthe-
sis, and modulators of oxyhemoglobin binding. Within seconds
after birth,the lungs fillwith air, pulmonarybloodflow
increases,
and fetal shunts through the foramen ovale and ductus
arteriosus
close. The respiratory system is challenged by a rapid
increase
in metabolic rate and by the gradual resetting of the
carotid
chemoreceptors from fetal to postnatal PaO2 values, while
the
final steps in structural maturation of the alveolar gas
exchange
units take place. Oxygen is crucial in modulating this series
of
events and, subsequently, birth into a hypoxic high altitude
envi-
ronment has not only short-term impact but also implicationsthat
may extend throughout the life-span.
The availability of oxygen influences profoundly the nature
and intensity of the developmental cardiopulmonary changes
that occur in the perinatal period from fetus to newborn
infant.
Such changes are clearly different at high altitude from
those
occurring at sea level and include differences in oxygen
arterial
saturation, breathing patterns and maturation of respiratory
con-
trol reflexes, and velocity of regression of fetal
characteristics
of the pulmonary vasculature. Various differences in
transitional
changes vary not only with postnatal age and altitude, but
also
among populations living in different high altitude settings,
sug-
gesting an important influence of genetic adaptation on
perinatal
physiology. Exposure to chronic high altitude hypoxia during
theperinatal transition also results in apparent lifelong
alterations in
respiratory reflex responses and pulmonary vasoreactivity.
Dis-
ruption of the normal process of cardiopulmonary transition
can
result in symptomatic high altitude pulmonary hypertension.
It
is also very likely that the high altitude hypoxia may
interact
synergistically with hypoxemia due to acute respiratory
infec-
tions in young infants still undergoing transition, contributing
in
this way to infant mortality at high altitude (Lozano,
2001).
3.1.1. Arterial oxygen saturation
Arterial oxygen saturation (SaO2) decreases with increasing
altitude, but this decrease is not linear. The SaO2 of infants
at
high altitude depends on several variables, including the
ambient
oxygen pressure, age of infants, state of awakening,
feeding,
respiratory rate and pattern, oxygen hemoglobin affinity,
and
reactivity of the pulmonary vessels. In addition, SaO2 shows
population variations that may be reflecting differing
genetic
adaptation to high altitude.
At 3100 m, saturation in awakening infants is significantly
higher than those in active or quiet sleep. It is variable
with
feeding, tending to be intermediate between wakefulness and
sleep. This pattern is similar with further altitude increase,
and at
3658 m in Lhasa, the highest saturations occur in the first 2
days
after birth, followed by a decline in the first week
(Niermeyer
et al., 1995). Tibetan newborn infants show consistently
higher
oxygen saturations than Han infants, although they reside at
the
same altitude in Lhasa. In the first 2 days after birth, SaO 2
aver-
ages 90% to 94% in the Tibetans and 86% to 92% in the Han.
During infancy, Tibetan infants maintain fairly constant
values
in all states, while Han infants show a progressive decline
during
sleep through 4 months (Niermeyer et al., 1995). Andean
infants
between 2 and 5 months show at a similar altitude (3750 m)
val-uesroughly lowerthan Tibetaninfants, with averagesof 88 3%
(Reuland et al., 1991). In El Alto, Bolivia (4018 m) infants
have
a mean SaO2 of 86.9% overall and a mean of 87.8% during the
awake state (Gamponia et al., 1998). At 4540m in Peru,
SaO2values range from 57% to 75% in infants from 30 min to 72 h
of age (Gamboa and Marticorena, 1971) and from 74% to 81%
during infancy and childhood (Sime et al., 1963). These
values
show a wide range, and thus some caution is warranted before
deriving conclusions on normal values in different high
altitude
settings.
As remarked previously, in addition to altitude and post-
natal age, SaO2 variations are related to other factors such
asbehavioral state or activity and population group. Moreover,
oxygen hemoglobin affinity also influences SaO2 values, and
oxygen hemoglobin affinity in turn depends on proportion of
fetal hemoglobin, 2,3 DPG, PCO2, pH and temperature. It has
been reported that the proportion of fetal hemoglobin (HbF)
in
high altitude newborn infants is higher than that of their
sea
level counterparts (Ballew and Haas, 1986). When differences
were assessed between different populations living at high
alti-
tude on the Andean plateau, lower proportions of HbF were
demonstrated among high altitude residents of native Aymara
andQuechua versus mestizo background, andover25% of native
infants showed a predominance of adult hemoglobin (HgbA)
in cord blood (Galarza Guzman, 1988). The advantage of HbFin
high altitude newborns may depend on how adequate is the
delivery of oxygen to the tissues during fetal life.
Differences in adult SaO2 values found among different adult
populations native to high altitude have also been shown
among
Tibetan and Han neonates born to women resident at high
alti-
tude.Tibetan infants displayedhigher SaO2 andbirth weight
and
lower hemoglobinconcentrationthan Hannewborns(Niermeyer
et al., 1995). These findings reflect likely genetic differences
in
the degree of adaptation to high altitude hypoxia of Tibetan
and Han populations. Hypoxia may have operated distinctly
in these populations through genetic modification of regula-
tors of pulmonary vascular reactivity and blood flow such as
-
7/30/2019 Post Natal Pulmonary Adaptations
8/14
L. Huicho / Respiratory Physiology & Neurobiology 158 (2007)
190 203 197
nitric oxide production, which is known to be under genetic
control (Marsden et al., 1993; Pearson et al., 2001).
Pulmonary
vascular reactivity may in turn modify the SaO2.
Alternatively,
direct effects on genes accounting for oxygen saturation may
have operated distinctly in different populations (Beall,
2006).
It seems that oxygen saturation has no heritability in the
Andean
natives, but does among Tibetans where an autosomal domi-
nant major gene for higher oxygen saturation has been
detected
(Weiss, 1993). Women estimated with high probability to have
high oxygen saturation genotypes have more surviving chil-
dren than those estimated with high probability to have the
low
oxygen saturation genotype. These findings suggest that
ongo-
ing natural selection favoring greater reproductive success
is
increasing thefrequency of thehigh saturation alleleat this
major
gene locus (Beall et al., 1994, 1997, 2004). This is
interesting
given the amount of mobility and cross-breeding that occurs
nowadays.
3.1.2. Ventilation and pulmonary function
For a detailed discussion on the development of
ventilatorycontrol in infants, the reader is referred to a recently
pub-
lished review (Cohen and Katz-Salamon, 2005). The
ventilation
control is related to the function of the peripheral
chemorecep-
tors, which are the bodys principle O2 (hypoxia) sensors.
The
HVR of newborn infants is well known. It consists of an ini-
tial and transient peripherally mediated increase in
ventilation,
which quickly returns to baseline or even below (Cohen et
al.,
1997). The fall in ventilation during sustained hypoxia, is
due
to hypoxic depression of chemoreception, which has
peripheral
and central components. With advancing age, the initial
tran-
sient increase in ventilation becomes sustained for longer
and
the hypoxic depression becomes less dramatic, although
devel-opment is slow and the biphasic response persists in some
form
into adulthood (Easton et al., 1988; Cohen et al., 1997). Of
note,
hypometabolism is known to occur on exposure to hypoxia in
newborns, but infants at high altitude maintain metabolic
rate
with no major alterations in ventilation (Mortola et al.,
1992).
Neonates gestated and born at high altitude (3850m) show
a similar biphasic HVR as neonates born at a lower altitude
(800 m), that is, initial increase in ventilation, followed by a
sus-
tained decrease that may persist beyond the termination of
the
hypoxic stimulus (Lahiriet al., 1978). Of note, when infants
born
at high altitude experienced a prolonged exposure to 3850 m,
resting ventilation did not increase or decrease as compared
with sea level infants. Developmental control of ventilation
isalso influenced by early exposure to hypoxia. Thus it has
been
shown that the mature hyperbolic curve of the HVR is delayed
in rats raised at high altitude as compared with rats growing
at
sea level (Joseph et al., 2000). Interestingly, infants native
to
La Paz (4000 m), showed deeper and slower respiratory
pattern
and greater oxygen extraction than infants native to Santa
Cruz
(500m)(Mortola et al., 1992). However, in this study, there
were
no differences in pulmonary ventilation, oxygen consumption,
or carbon dioxide production between the two groups.
Pulmonary development at the level of gas exchange units is
also influenced by perinatal exposure to hypoxia. In rat
models,
the velocity of lung volume increase is slower, there is a
delayed
septation of gas exchange saccules, the gas exchange surface
area is blunted, and there is an accelerated thinning of the
alve-
olar walls (Massaro et al., 1989). These changes may
constitute
the underlying mechanisms of pulmonary anatomic and func-
tional changes observed in infants and children living at
high
altitude and exposed to hypoxia in early periods of
development.
3.1.3. Pulmonary artery pressure
Infants born at high altitude display in general a constric-
tive arterial pulmonary response to ambient hypoxia which
is related to an increased thickness of the muscular layer
in the pulmonary vessels. This vasoconstriction leads in
turn
to right ventricular hypertrophy. These characteristics have
been studied through electrocardiographic,
echocardiographic,
hemodynamic and histopathologic studies in children
gestated,
born and resident at high altitude settings. How long the
increased pulmonary artery and the right ventricular pattern
predominate has been shown to vary at different altitudes.
Infants studied in Mexico (2240 m) through echocardiog-
raphy showed slightly elevated pulmonary artery pressures at1530
days (Victoria-Oliva et al., 1996). In Leadville, Colorado
(3100m), echocardiography showed that pulmonary artery pres-
sure showed normal to moderately elevated values during the
neonatal period that normalized completely by 24 months of
age (Niermeyer et al., 1993). All these infants had received
supplementary oxygen immediately after birth that may have
modified the pulmonary artery pressure response verified
later
in infancy. Healthy infants in La Paz (37004000 m) showed a
gradual decrease of pulmonary artery pressure as determined
by echocardiography (Niermeyer et al., 2002). An echocar-
diographic comparative study revealed that right ventricular
anterior wall of infants native to La Paz (3600 m) was
greaterthan that of infants native to Santa Cruz (300 m),
difference
that persisted through the first year of extrauterine life; by
con-
trast, low altitude infants showed a significant decrease of
wall
thickness by the end of the first month of life ( Aparicio et
al.,
1991).
Heart catheterization has also been performed for assess-
ing the pulmonary artery pressure response. Neonates born in
Morococha, Peru (4540 m), showed pulmonary artery pressure
values close to systemic blood pressures when alveolar PO2was
about 50 mm Hg, values that persisted for 72 h after birth.
Interestingly, the pulmonary artery pressure showed an
inverse
correlation with SaO2 and administration of 100% oxygen to
some infants led to a fall of pressure to values near normal
forsea level (Gamboa and Marticorena, 1971).
The electrocardiographic findings also point to similar pat-
terns of persistence of increased pulmonary artery pressure
and
right ventricular preponderance, again being the time-course
of
such changes dependent on the age of infants and on the
altitude
of residence (Marticorena, 1983).
Another avenue of evidence for developmental artery pul-
monary pressure response came from histopathologic studies
performed in Peruvian infants. The histologic pattern of the
pulmonary artery trunk at various altitudes ranging from sea
level to 4540 m showed a delayed changed from the aortic to
adult structure. Infants born at sea level display a
transitional
-
7/30/2019 Post Natal Pulmonary Adaptations
9/14
198 L. Huicho / Respiratory Physiology & Neurobiology 158
(2007) 190203
pattern by 6 months and an adult pattern by 2 years of age,
whereas residents above 3440 m may show persistence of an
aortic (high-pressure) pattern into the preschool years
(Saldana
and Arias-Stella, 1963a, 1963b).
As for high altitude-related structural heart abnormalities,
echocardiography measurements performed in infants aged
from 2 weeks to 6 months in La Paz (37004000 m) revealed
persistence of an anatomically patent foramen ovale in 75%
through 3 months and 44% through 6 months ( Niermeyer et
al., 2002). None of these infants showed a clinically
significant
shunting. However, other studies in school-age children in
Tibet
(Miao et al., 1988) and Peru (Alzamora Castro et al., 1960)
have
identified an increased prevalence of symptomatic patent
ductus
arteriosus and patent foramen ovale with increasing altitude
of
residence.
Finally, there is evidence that high altitude interacts with
acute respiratory infections, particularly in young infants
and
children, aggravating the hypoxemia and increasing thus the
risk
of death (Reuland et al., 1991; Onyango et al., 1993; Lozano
et al., 1994; Dyke et al., 1995; Duke et al., 2001;
Lozano,2001). Consequently, it has been proposed that SaO2
moni-
toring through an extensive use of pulse oximetry should be
investigated and implemented for avoiding severe hypoxemia
and death in high altitude infants and children with acute
respi-
ratory infections (Duke et al., 2002; Huicho, 2003). The use
of
pulse oximetry monitoring would also be a more efficient
strat-
egy for detecting hypoxemia and risk of death at high
altitude
than clinical signs (Reuland et al., 1991; Duke et al.,
2002).
In summary, increased pulmonary arterial pressure and right
ventricular preponderance persist at altitudes above 4000 m
well
beyond infancy in Andean populations. Because these find-
ings have not been related to clinical signs, they have
beenconsidered as adaptive responses to high altitude hypoxia.
How-
ever, these changes have also been described in infants in
La
Paz, Leadville and Lhasa who developed symptomatic acute or
subacute pulmonary hypertension (Khoury and Hawes, 1963;
Hurtado Gomez and Calderon, 1965; Sui et al., 1988;
Niermeyer
et al., 1998). Thus, caution should be exercised before con-
sidering asymptomatic pulmonary hypertension as a universal
adaptive response.
3.2. Later cardiopulmonary changes in high altitude
children and adolescents
In Peruvian children living at the same altitude in
Tintaya,Marquiri, and Nunoa (4100 m), but having different
degrees
of genetic admixture and different nutritional and socioeco-
nomic conditions, we showed substantially higher height and
weight in those with better nutrition and socioeconomic con-
dition (Pawson et al., 2001). This finding is suggestive of
a
relatively minor influence of high altitude hypoxia on
physical
growth in face of relatively advantageous socioeconomic
condi-
tions (Pawson et al., 2001). Interestingly, Nunoa children,
with
predominant Quechua ancestry, showed higher arterial oxygen
saturation values and lower heart rate than the other two
groups,
predominantly mestizo, findings suggestive of a better
degree
of adaptation in Nunoa children (Huicho et al., 2001). Fur-
ther studies are needed that compare SaO2 in Andean, Tibetan
and Ethiopian children. They should carefully assess
potential
modifying factors such as migration patterns to lower
altitudes,
frequency of early respiratory conditions, indoor pollution,
and
nutritional and socioeconomic status.
Physical growth and functional development of the respira-
tory system seem to follow a pattern different from that in
sea
level children and adolescents. Anatomic and functional
studies
showedthat thethorax andrespiratorysystem display an
acceler-
ated growth and maturation in high-altitude children
(Frisancho,
1976; Frisancho, 1969; Mueller et al., 1978). Also, children
with
a genetic ancestry suggestive of long-term exposure to high
alti-
tude seem to have higher chest dimensions relative to
stature
and higher respiratory functional measurements than children
of
European ancestry living at high altitude (Greksa, 1986,
1988;
Greksa et al., 1987, 1988; Stinson, 1985).
As it has been shown in infants, several
electrocardiographic,
vectorcardiographic, hemodynamic and histopathologic studies
in children and adolescents living at high altitude have
shown
persistent hypertrophy of the pulmonary artery muscular
layer,asymptomatic pulmonary artery hypertension and a related
right
ventricular hypertrophy. As we already mentioned above,
these
characteristics persist well beyond infancy and extend into
late
childhood, particularly in children living at extreme
altitudes
(Marticorena, 1983; Penaloza et al., 1960, 1961, 1964). A
recent
study in healthy Tibetan and Han children aged 712 years
also showed a high prevalence of ECG abnormalities consis-
tent with right heart strain in both groups, with no
difference
between the two ethnic groups or sexes. Children were
studied
at two altitudes at 3500 and 4500m. These results contrast
with
other reports showing higher rates of chronic altitude sickness
in
Han Chinese children. The authors conclude that other
studiesshowing higher observed rates of symptomatic chronic
altitude
sickness in Han Chinese children suggest that
extracardiologic
factors play a role in the pathogenesis of the disease. They
nev-
ertheless acknowledge limitations of their study, including
small
sample size and the low sensitivity of the electrocardiogram
in
the detection of right ventricular strain (Hulme et al.,
2003).
Overall, all the above research on developmental cardiopul-
monary responses in children living at high altitude show
consistently a prolonged right ventricular predominance
beyond
infancy and a concomitant persistence of asymptomatic pul-
monary artery hypertension, characteristics that seem to
reflect
an adaptive set of strategies in Andean and Tibetan children
liv-
ing at high altitude. However, the description of
symptomatichigh altitude pulmonary hypertension and of
altitude-related
structural heart abnormalities in different populations of
chil-
dren living in Bolivia, Leadville and Lhasa (Hurtado Gomez
and Calderon, 1965; Khoury and Hawes, 1963; Niermeyer et
al., 1998; Sui et al., 1988; Niermeyer et al., 2002; Miao et
al.,
1988; Alzamora Castro et al., 1960) strongly suggest the
exis-
tence of differing pulmonary artery pressure response
patterns
to high altitude hypoxia among different populations. This
is
similar to the erythropoietic and SaO2 responses, which show
different patterns in Andean, Tibetan and Ethiopian
populations.
In some populations the absence of a delayed regression of
an increased pulmonary artery pressure and right ventricular
-
7/30/2019 Post Natal Pulmonary Adaptations
10/14
L. Huicho / Respiratory Physiology & Neurobiology 158 (2007)
190 203 199
preponderance may be indicating a better adaptation to high
altitude, whereas in those populations with a slower change
to
adult patterns or even absence of such transition, the
responses
may be indicating a lower degree of adaptation. We can
advance
the hypothesis that, similarly to what has been described in
adult
populations, different patterns of adaptation to high altitude
are
probably present in relation to the pulmonary artery
response
in Andean, Tibetan and Ethiopian children. We need further
research to confirm this hypothesis and also to identify the
time-period of the occurring changes. Furthermore, factors
such
as genetic admixture, patterns of migration to lower
altitudes,
outdoor and indoor pollution, nutritional and socioeconomic
conditions were not adequately addressed or they were com-
pletely absent in most of the above cited studies. Thus
there
is a legitimate concern on whether the pattern of cardiopul-
monary responsesis consistently similar whensuch factors
differ
among different study populations of children. These factors
may act to modify the pulmonary artery pressure response to
hypoxia. Further studies aimed at assessing the possible
influ-
ence of these conditions on developmental
cardiopulmonaryresponses of different high altitude children
populations are
warranted.
In this regard, we recently studied preschool and school-
aged children resident at 4100 m in Tintaya, Peru (Huicho et
al.,
2005; Huicho and Niermeyer, 2006, 2007). Our broad objective
was to correlate clinical assessments with anatomic and
physio-
logic cardiovascular findings. Other specific objectives
included
the determination of prevalence of pathologic
cardiopulmonary
findings and of prevalence of symptomatic high altitude pul-
monary hypertension. We took advantage of an existing mining
settlement that comprised 150 families, with 336 children.
The
study population also facilitated exploration of genetic and
envi-ronmental factors such as admixture, patterns of exposure
to
altitude, and duration of residence at high altitude. We
admin-
istered a structured questionnaire to every selected family
for
obtaining information on surnames of children, parents, and
grandparents and on language(s) spoken in the household as
indicators of ethnic origin. Questions also covered the
alti-
tude of birth for each child and altitude of residence prior
to
arrival at Tintaya, duration of residence in Tintaya, and
typi-
cal annual pattern of movement. Problems during the
perinatal
period were sought, as were childhood health problems, with
particular emphasis on cardiorespiratory ailments and
chronic
conditions. The responses to altitude change, level of
activ-
ity at high altitude, and environmental smoke exposure werealso
assessed. Subsequently, all children underwent a complete
physical examination, anthropometry, oxygen saturation mea-
surements, hemoglobin determination, electrocardiography and
echocardiography. We found that most children showed at
least
some degree of high altitude ancestry, based on analysis of
maternal and paternal surnames and the surnames of maternal
and paternal grandparents. Our schoolchildren showed also a
high mobility pattern to lower altitudes, most of them
traveled
to lower altitude during summer vacation and winter break
each
year. They enjoyed furthermore a good nutritional status and
lived in favorable housing conditions. In those children, we
did
not find evidence of pulmonary artery hypertension out of
the
context of heart structural abnormalities. The prevalence of
such
abnormalities was also similar to that of sea level.
Controlling
for potential confounding factors that may influence
echocardio-
graphic and electrocardiographic measurements including sex,
nutritional status, chest dimensions, pulse oximetry,
hemoglobin
concentration, ethnicity, length of residence at high altitude,
or
parental history of exposure to high altitude, did not reveal
a
consistent influence of such variables.
Our findings clearly differ from previous studies. Several
explanations may be offered for these discrepant results.
Most
children showed at least some degree of high altitude
genetic
pattern through patronymic evaluation. This trait may have
con-
ferred them a genetic adaptive advantage, although this
cannot
explain completely the absence of pulmonary hypertension. In
addition, other factors such as the frequent descent to
lower
altitudesmay have attenuated theeffectsof hypoxia on
thedevel-
opment of cardiopulmonary system. Although we were not able
to assess completely whether the outdoor and indoor
pollution
influences developmental pattern, it is plausible that
pollution
can affect important periods of the cardiopulmonary develop-ment
process. It is known that indoor pollution is a risk factor
for respiratoryinfections, and thuswe can speculatethat
frequent
presentation of such illnesses may impair the setting of
adaptive
cardiopulmonary responses in early life. Our study
population
enjoyed unusually good outdoor andindoor conditions for a
high
altitude mining settlement. Finally, we acknowledge the need
to
perform studies that adequately assess the real role of
pollution
and of the prevalence of respiratory infections on the
patterns
of cardiopulmonary development through comparative observa-
tion of high altitude children living under different degrees
of
exposure to pollutants.
4. Symptomatic high altitude pulmonary hypertension
The previous findings on cardiopulmonary responses to high
altitude in infants and children are clearly relevant to the
risk of
development of high altitude-related cardiopulmonary pathol-
ogy in general and more specifically of a clinical condition
called high altitude pulmonary hypertension. There are
several
reports of the latter in the literature and all have been
described
in infants, children and adults resident at altitude (Grover et
al.,
1966; Hurtado Gomez and Calderon, 1965; Khoury and Hawes,
1963; Lin and Wu, 1974; Sui et al., 1988; Wu et al., 1998;
Wu
and Miao, 2002; Wu et al., 2003). The hallmark of the
condition
is the presence of pulmonary artery hypertension and it is
associ-ated with several clinical features. A recent consensus
statement
on high altitude diseases defines high altitude pulmonary
hyper-
tension as a clinical condition occurring in children and
adults
resident above 2500m and characterized by a mean pulmonary
artery pressure above 30 mm Hg or a systolic pulmonary
artery
pressure above 50 mm Hg, right ventricular hypertrophy,
heart
failure, moderate hypoxemia and the absence of excessive
ery-
throcytosis (Leon-Velarde et al., 2005). There has been some
confusion in the literature and several terms have been
histori-
cally used, including chronic mountain sickness of the
vascular
type, high altitude heart disease, hypoxic cor pulmonale,
infant
subacute mountain sickness, pediatric high altitude heart
dis-
-
7/30/2019 Post Natal Pulmonary Adaptations
11/14
200 L. Huicho / Respiratory Physiology & Neurobiology 158
(2007) 190203
ease, and adult subacute mountain sickness (Leon-Velarde et
al., 2005).
The consensus statement did not provide information on the
prevalence of high altitude disease and listed some risk
fac-
tors, includingprevious pulmonaryarterial hypertension,
history
of persistent excessive pulmonary vasoconstriction in
response
to hypoxia, and hypoxemia during sleep (Leon-Velarde et al.,
2005). An adequate assessment of prevalence requires the
study
of samples with known denominator. Unfortunately, most stud-
ies referring to high altitude disease in children did not
provide
this substantial information. Similarly, the determination of
risk
factors ideally needs cohort studies or casecontrol studies
ade-
quately controlled for bias, and we have not found such
studies
in the reviewed literature.
It seems from the above discussed studies that symptomatic
high altitude pulmonary hypertension is (1) a potentially
life-
threatening condition presenting in infants, children and
even
adults with risk factors and(2) that subjects without high
altitude
genetic ancestry may be more susceptible. Among populations
with some degree of genetic admixture, the pre-existence
ofpulmonary artery hypertension may be an important risk
factor.
The role of other factors such as indoor pollution,
pre-existing
respiratory conditions such as asthma, particularly if not
con-
trolled, and migration patterns to low altitudes, requires
further
study.
5. Possible long-term implications of early
cardiopulmonary patterns of growth and development
at high altitude
A series of papers on the pediatric origins of adult lung
diseases has recently been published that include general
devel-opmental issues and specific lung problems arising in
infancy,
childhood and adulthood, which are associated with early
pre-
natal or postnatal exposure to different agents (Eber and
Zach,
2000; Holt and Sly, 2000; Le Souef, 2000; Robinson, 2000;
Sly,
2000; Stick, 2000; von Mutius, 2000). Additional
epidemiolog-
ical studies showed that exposure to factors that restrict
fetal
growth, lead to low birth weight, or interfere with early
postna-
tal growth, can alter lung development and have later
adverse
effects on lung function and respiratory health. Major
causal
factors include reduced nutrient and oxygen availability,
nico-
tine exposure via maternal tobacco smoking and preterm
birth,
each of which can affect critical stages of lung development
(Hafstrom et al., 2005; Harding et al., 2000; Maritz et al.,
2005;Svanes et al., 2004).
Similarly, experimental studies have demonstrated that these
environmental insults can permanently alter lung structure
and
hence lung functions, increasing the risk of respiratory
illness
and accelerating the rate of lung aging (Harding et al.,
2000;
Maritz et al., 2005). A fetus is able to mount a
proliferative
response to a common allergic trigger (beta-lactoglobulin,
house
dustmite, etc.) asearly as22 weeks of pregnancy (Fig.4).
Mater-
nal exposure to allergens influences self-IgG production
which
modulates the allergen exposure of the fetus resulting in
either
primary sensitization of T cells or tolerance to the
allergen.
Atopic mothers create a more Th2-orientated environment for
the developing fetus than non-atopic mothers (Warner, 1999).
Thus early manipulation of the maternal immune response
during pregnancy, either by reducing self-exposure to
environ-
mental allergens or controlling her allergic reactions, may be
a
method of preventing later development of allergic disease
in
infants (Warner, 1999) (Fig. 4). Early postnatal antibiotic use
in
the first 6 months of life preceded the manifestation of
wheeze
but not eczema or allergic sensitization during the first 2
years
of life (Kummeling et al., 2007) (Fig. 4). However, there is
still
incomplete understanding of the molecular and cellular
mecha-
nisms by which these factors adversely affect lung
development
and whether such effects can be blocked or reversed (Maritz
et al., 2005). The role of early postnatal respiratory
infections
such as bronchiolitis and pneumonia in the later development
of chronic respiratory diseases including asthma and chronic
obstructive pulmonary disease is somewhat contradictory and
needs further investigation (Stick, 2000).
Chronic hypoxia is an attractive model that can be used in
animals for performing comparative studies on whether
hypoxia
modifies the programming events in the fetus and the newbornand
whether it influences on the risk of developing cardiopul-
monary conditions in later periods of life. In fact, cohort
and/or
casecontrol studies in humans may also reveal the ways by
which chronic hypoxia operates on early periods of lifefor
deter-
mining later cardiopulmonary clinical conditions in human
high
altitude populations, as well as the underlying molecular
mech-
anisms. Demonstration of critical periods of cardiopulmonary
growth and development that are vulnerable to chronic
hypoxia
may lay the basis for developing early preventive
interventions
related to lifelong permanence at high altitude.
6. Clinical and public health implications: is the
evidence strong enough?
Thestrength of the available evidence is currently not
enough
for implementing sound clinical and health policy recom-
mendations for preventing and managing high altitude-related
conditions in children going to or already living at high
alti-
tude. However, the implication is that newcomers,
particularly
those of non-high altitude ancestry, may be at more risk of
developing symptomatic high altitude pulmonary hypertension.
Also, it seems that those infants and children with
pre-existing
pulmonary artery hypertension and those with an acute respi-
ratory infection should be cautioned against traveling to
highaltitude, particularly against a rapid ascent. In addition, it
seems
advisable to recommend supplementary oxygen to infants and
children living at high altitude and suffering from an acute
respi-
ratory infection, particularly pneumonia, when values of SaO2are
lower than those considered normal for the altitude of res-
idence. Pneumonia is known to lead to hypoxemia and it very
likely aggravates any pre-existing high altitude hypoxia.
Normal
SaO2 values published for infants and children living at sea
level
are clearly not applicable to children living at different
altitudes
and thus further investigation is warranted for identifying
cut-
off SaO2 values below which supplementary oxygen should be
mandatory (Duke et al., 2002; Huicho, 2003).
-
7/30/2019 Post Natal Pulmonary Adaptations
12/14
L. Huicho / Respiratory Physiology & Neurobiology 158 (2007)
190 203 201
References
Alzamora Castro, V., Battilana, G., Abugattas, R., Sialer, S.,
1960. Patent ductus
arteriosus and high altitude. Am. J. Cardiol. 5, 761763.
Aparicio, O.O., Romero Gutierrez, F., Harris, P., Anand, I.,
1991. Echocardiog-
raphy shows persistent thickness of the wall of the right
ventricle in infants
at high altitude. Cardioscience 2, 6369.
Ballew, C., Haas, J.D., 1986. Hematologic evidence of fetal
hypoxia among
newborn infants at high altitude in Bolivia. Am. J. Obstet.
Gynecol. 155,
166169.
Barker,D.J.P. (Ed.), 2002. Fetaland Infant Originsof Adult
Disease.BMJ Books,
London.
Beall, C.M., 2000. Tibetan and Andean patterns of adaptation to
high-altitude
hypoxia. Hum. Biol. 72, 201228.
Beall, C.M., 2006. Andean, Tibetan, and Ethiopian patterns of
adaptation to
high-altitude hypoxia. Integr. Comp. Biol. 46, 1824.
Beall, C.M., Blangero, J., Williams-Blangero, S., Goldstein,
M.C., 1994. A
major genefor percent of oxygensaturation of arterial hemoglobin
in Tibetan
highlanders. Am. J. Phys. Anthropol. 95, 271276.
Beall, C.M., Decker, M.J., Brittenham, G.M., Kushner, I.,
Gebremedhin, A.,
Strohl, K.P., 2002. An Ethiopianpatternof human adaptation to
high-altitude
hypoxia. Proc. Natl. Acad. Sci. 99, 1721517228.
Beall, C.M., Song, K., Elston, R.C.,Goldstein,M.C., 2004. Higher
offspring sur-
vival among Tibetan women withhigh oxygen saturation genotypes
residing
at 4000 m. Proc. Nat. Acad. Sci. 101, 1430014304.
Beall, C.M., Strohl, K., Blangero, J., Williams-Blangero, S.,
Brittenham, G.M.,
Goldstein, M.C., 1997. Quantitative genetic analysis of arterial
oxygen sat-
uration in Tibetan highlanders. Hum. Biol. 69, 597604.
Blanco, L.N.,Massaro,D., Massaro,G.D., 1991. Alveolarsize,
number, and sur-
face area: developmentally dependent response to 13% O2. Am. J.
Physiol.
Lung. Cell. Mol. Physiol. 261, L370L377.
Brutsaert, T.D., 2001. Limits on inferring genetic adaptation to
high altitude in
Himalayan and Andean populations. High Alt. Med. Biol. 2,
211225.
Cohen, G., Malcolm, G., Henderson-Smart, D., 1997. Ventilatory
response of
the newborn infant to mild hypoxia. Pediatr. Pulmonol. 24,
163172.
Cohen, G., Katz-Salamon, M., 2005. Development of chemoreceptor
responses
in infants. Respir. Physiol. Neurobiol. 149, 233242.
Duke, T., Mgone, J., Frank, D., 2001. Hypoxemia in children with
severe pneu-monia in Papua New Guinea. Int. J. Tuberc. Lung Dis. 5,
511519.
Duke, T., Blaschke, A.J., Sialis, S., Bonkowsky, J.L., 2002.
Hypoxaemia in
acute respiratory and non-respiratory illnesses in neonates and
children in a
developing country. Arch. Dis. Child. 86, 108112.
Dyke, T., Lewis, D., Heegaard, W., Manary, M., Flew, S., Rudeen,
K., 1995.
Predicting hypoxiain children withacute lower respiratory
infection: a study
in the highlands of Papua New Guinea. J. Trop. Pediatr. 41,
196201.
Easton, P.A., Slykerman, L.J., Anthonisen, N.A., 1988. Recovery
of the venti-
latory response to hypoxia in normal adults. J. Appl. Physiol.
64, 521528.
Eber, E., Zach, M.S., 2000. Paediatric origins of adult lung
disease: long term
sequelae of bronchopulmonary dysplasia (chronic lung disease of
infancy).
Thorax 56, 317323.
Frisancho, A.R., 1976. Growth and development at highaltitude.
In: Baker, P.T.,
Little, M.A. (Eds.), Man in the Andes. A Multidisciplinary Study
of High-
altitude Quechua. Dowden and Hutchinson, Stroudsburg, PA, pp.
180207.Frisancho, A.R.,1969. Human growth and pulmonary functionof
a highaltitude
Peruvian Quechua population. Hum. Biol. 41, 365379.
Galarza Guzman, C.M., 1988. Hemoglobinas en recien nacidos
ciudad de La
Paz altura 3600 m. Commun. Rapida Instit. Boliv. Biolog. Alt. 2,
316.
Gamboa, R., Marticorena, E., 1971. Presion arterial pulmonar en
recien nacidos
en las grandes alturas. Arch. Instit. Biolog. Andina 4,
5566.
Gamponia, M.J., Babaali, H., Yugar, F., Gilman, R.H., 1998.
Reference values
for pulse oximetry at high altitude. Arch. Dis. Child. 78,
461465.
Greksa, L.P., 1986. Chest morphology of young Bolivian
high-altitude residents
of European ancestry. Hum. Biol. 58, 427443.
Greksa, L.P., 1988. Effect of altitude on the stature, chest
depth and forced
vital capacity of low-to-high altitude migrant children of
European ancestry.
Hum. Biol. 60, 2332.
Greksa, L.P., Spielvogel, H., Caceres, E., Paredes-Fernandez,
L., 1987. Lung
function of young Aymara highlanders. Ann. Hum. Biol. 14,
533542.
Greksa, L.P., Spielvogel, H., Paz-Zamora, M., Caceres, E.,
Paredes-Fernandez,
L., 1988. Effect on the lung function of high altitude residents
of European
ancestry. Am. J. Phys. Anthropol. 75, 7785.
Grover, R.F., Vogel, J.H., Voigt, G.C., Blount Jr., S.G., 1966.
Reversal of high
altitude pulmonary hypertension. Am J Cardiol. 18, 928932.
Hafstrom, O., Milerad, J., Sandberg, K.L., Sundell, H.W., 2005.
Cardiorespi-
ratory effects of nicotine exposure during development. Respir.
Physiol.
Neurobiol. 149, 325341.
Harding, R., Cock, M.L., Louey, S., Joyce, B.J., Davey, M.G.,
Albuquerque,C.A.,Hooper, S.B.,Maritz, G.S.,2000. The compromised
intra-uterine envi-
ronment: implications for future lung health. Clin. Exp.
Pharmacol. Physiol.
27, 965974.
Hochachka, P.W., 1986. Defense strategies against hypoxia and
hypothermia.
Science 231, 234241.
Hochachka, P., Gunga, H.C., Kirsch, K., 1998. Our ancestral
physiological phe-
notype: and adaptation for hypoxia tolerance or for
enduranceperformance?
Proc. Natl. Acad. Sci. 95, 19151920.
Hochachka, P.W., Lutz, P.L., 2001. Mechanism, origin, and
evolution of anoxia
tolerance in animals. Comp. Biochem. Physiol. B: Biochem. Mol.
Biol. 130,
435459.
Holt, P.G., Sly, P.D., 2000. Paediatric origins of adult lung
diseases: Prevention
of adult asthma by early intervention during childhood:
potential value of
new generation immunomodulatory drugs. Thorax 55, 700703.
Huicho, L., 2003. Hypoxaemia in children: abnormal values may be
mislead-ing. Arch. Dis. Child. 88, 364.
Huicho, L., Muro, M., Pacheco, A., Silva, J., Gloria, E.,
Marticorena, E., Nier-
meyer, S., 2005. Cross-sectional study of echocardiographic
characteristics
in healthy children living at high altitude. Am. J. Hum. Biol.
17, 704
717.
Huicho, L., Niermeyer, S., 2006. Cardiopulmonary pathology among
children
resident at high altitude in Tintaya, Peru: a cross-sectional
study. High Alt.
Med. Biol. 7, 168179.
Huicho, L., Pawson, I.G., Leon-Velarde, F., Rivera-Chira, M.,
Pacheco, A.,
Muro, M., Silva, J., 2001. Oxygen saturation and heart rate in
healthy
school children and adolescents living at high altitude. Am. J.
Hum. Biol.
13, 761770.
Huicho, L., Niermeyer, S., 2007. Cross-sectional study of
electrocardiographic
pattern in healthy children resident at high altitude. Am. J.
Phys. Anthropol.
133, 879886.
Hulme, C.W., Ingram, T.E., Lonsdale-Eccles, D.A., 2003.
Electrocardiographic
evidence for right heart strain in asymptomatic children living
in Tibeta
comparative study between Han Chinese and ethnic Tibetans.
Wilderness
Environ. Med. 14, 222225.
Hurtado Gomez, L., Calderon, R.G., 1965. Hipoxia de altura en la
insuficiencia
cardiaca del lactante. Bolet. Soc. Boliv. Pediatr. IX, 1123.
Joseph, V., Soliz, J., Pequignot, J., Sempore, B., Cottet-Emard,
J.M., Dalmaz,
Y., Favier, R., Spielvogel, H., Pequignot, J.M., 2000. Gender
differentiation
of the chemoreflex chemoreflex during growth at high altitude:
functional
and neurochemicalstudies. Am. J. Phys. Regul. Integrative Comp.
Biol. 278,
R806R816.
Khoury, G.H., Hawes, C.R., 1963. Primary pulmonary hypertension
in children
living at high altitude. J. Pediatr. 62, 177185.
Kummeling, I., Stelma, F.F., Dagnelie, P.C., Snijders, B.E.,
Penders, J., Huber,
M., van Ree, R., van den Brandt, P.A., Thijs, C., 2007. Early
life exposure to
antibiotics and the subsequent development of eczema, wheeze,
and allergic
sensitization in the first 2 years of life: the KOALA Birth
Cohort Study.
Pediatrics 119, e225e231.
Lahiri, S., Brody, J.S., Motoyama, E.D., Velasquez, T.M., 1978.
Regulation
of breathing in newborns at high altitude. J. Appl. Physiol. 44,
673
678.
Le Cras, T.D., Markham, N.E., Morris, K.G., Ahrens, C.R.,
McMurtry, I.F.,
Abman, S.H., 2000. Neonatal dexamethasone treatment increases
the risk
for pulmonary hypertension in adult rats. Am. J. Physiol. Lung
Cell. Mol.
Physiol. 278, L822L829.
Le Cras, T.D., Hardie, W.D., Deutsch, G.H.,Albertine,
K.H.,Ikegami, M., Whit-
sett,J.A., Korfhagen, T.R., 2004. Transientinduction of TGF-
disrupts lung
morphogenesis, causing pulmonary disease in adulthood. Am. J.
Physiol.
Lung Cell. Mol. Physiol. 287, L718L729.
-
7/30/2019 Post Natal Pulmonary Adaptations
13/14
202 L. Huicho / Respiratory Physiology & Neurobiology 158
(2007) 190203
Leon-Velarde, F., Maggiorini, M., Reeves, J.T., Aldashev, A.,
Asmus, I.,
Bernardi,L., Ge, R.L.,Hackett, P., Kobayashi, T., Moore,
L.G.,Penaloza, D.,
Richalet, J.P., Roach, R., Wu, T., Vargas, E., Zubieta-Castillo,
G., Zubieta-
Calleja, G., 2005. Consensus statementon chronic andsubacute
highaltitude
diseases. High Alt. Med. Biol. 6, 147157.
Le Souef, P.N., 2000. Paediatric origins of adult lung diseases:
tobacco related
lung diseases begin in childhood. Thorax 55, 10631067.
Lozano, J.M., 2001. Epidemiology of hypoxaemia in children with
acute lower
respiratory infection. Int. J. Tuber. Lung Dis. 5,
496504.Lozano, J.M., Steinhoff, M., Ruiz, J.G., Mesa, M.L.,
Martinez, N., Dussan, B.,
1994. Clinical predictors of acute radiological pneumonia and
hypoxaemia
at high altitude. Arch. Dis. Child. 71, 323327.
Lin, C.P., Wu, T.Y., 1974. Clinical analysisof 286cases of
pediatrichigh altitude
heart diseases. Chin. Med. J. 54 (Engl suppl to No. 6),
99100.
Maritz, G.S., Morley, C.J., Harding, R., 2005. Early
developmental origins of
impaired lung structure and function. Early Hum. Dev. 81,
763771.
Marsden,P.A., Heng, H.H.Q., Scherer,S.W., Stewart,R.J.,
Hall,A.V., Shi,X.M.,
Tsui, L.C., Schappert, K.T., 1993. Structure and chromosomal
localization
of the human constitutive endothelial nitric oxide synthase
gene. J. Biol.
Chem. 268, 1747817488.
Marticorena, E.A., 1983. Observaciones desde el nacimiento hasta
los 14 anos
de edad, en alturas comprendidas entre los 3730m y 4710msnm y
sus impli-
cancias en la adultez y enfermedad. Arch. Instit. Biol. Andina
12, 2650.
Massaro, G., DeCarlo Masaro, G., 2004. Critical period for
alveologenesis andearly determinants of adult pulmonary disease.
Am. J. Physiol. Lung Cell.
Mol. Physiol. 287, 715717.
Massaro, G.D., Olivier, J., Massaro, D., 1989. Short-term
perinatal 10% O2
alters postnatal development of lung alveoli. Am. J. Physiol.
257, L221
L225.
Massaro, G.D., Olivier, J., Dzikowski, C., Massaro, D., 1990.
Postnatal devel-
opment of lung alveoli: suppression by 13% O2 and a critical
period. Am.
J. Physiol. Lung Cell. Mol. Physiol. 258, L321L327.
Miao, C.Y., Li, W.X., Geng, D., Tao, L.A., Zuberbuhler, J.S.,
Zuberbuhler, J.R.,
1988. Effect of highaltitude on prevalence of congenital
heartdisease. Chin.
Med. J. (Engl). 101, 415418.
Monge, C., 1978. Acclimatization in the Andes, Reissued 1948
edition. The
Johns Hopkins Press, Baltimore.
Monge, C., Leon-Velarde, F., 1991. Physiological adaptation to
high altitude:
oxygen transport in mammals and birds. Physiol. Rev. 71,
11351172.
Moore, L.G., 2001. Human genetic adaptation to high altitude.
High Alt. Med.
Biol. 2, 257279.
Mortola, J.P., Frappell, P.B., Frappell, D.E., Villena-Cabrera,
N., Villena-
Cabrera, M., Pena, F., 1992. Ventilation and gaseous metabolism
in infants
born at high altitude,and their responses to hyperoxia. Am. Rev.
Respir. Dis.
146, 12061209.
Moudgil, R., Michelakis, E.D., Archer, S.L., 2005. Hypoxic
pulmonary vaso-
constriction. J. Appl. Physiol. 98, 390403.
Mueller, W., Yen, F., Rothhammer, F., Schull, F., 1978. A
multinational Andean
genetic and health program. VI. Physiological measurements of
lung func-
tion in an hypoxic environment. Hum. Biol. 50, 489513.
Niermeyer, S., 2003. Cardiopulmonarytransition in thehigh
altitudeinfant.High
Alt. Med. Biol. 4, 225239.
Niermeyer, S., Shaffer, E.M., Moore, L.G., 1998. Impaired
cardiopulmonary
transition at high altitude. Pediatr. Res. 43, 292A.
Niermeyer, S., Andrade, P., Vargas, E., Moore, L.G., 2002.
Prolonged postnatal
cardiopulmonary transition at 37004000 m. High Alt. Med. Biol.
3, 439.
Niermeyer, S., Yang, P., Shanmina, D., Zhuang, J., Moore, L.G.,
1995. Arterial
oxygen saturation in Tibetan and Han infants born in Lhasa,
Tibet. N. Engl.
J. Med. 333, 12481252.
Niermeyer, S., Shaffer, E.M., Thilo, E., Corbin, C., Moore,
L.G., 1993. Arterial
oxygenation and pulmonaryarterial pressure in healthy neonates
and infants
at high altitude. J. Pediatr. 123, 767772.
Onyango, F.E., Steinhoff, M.C., Wafula, E.M., Wariua, S., Musia,
J., Kitonyi, J.,
1993. Hypoxaemia in young Kenyan children with acute lower
respiratory
infection. BMJ 306, 612615.
Pawson, I.G., Huicho, L., Muro, M., Pacheco, A., 2001. Growth of
children in
two economically diverse Peruvian high-altitude communities. Am.
J. Hum.
Biol. 13, 323340.
Pearson, D.L., Dawling, S., Walsh, W.F., Haines, J.L.,
Christman, B.W., Bazyk,
A., Scott, N., Summar, M.L., 2001. Neonatal pulmonary
hypertension:
Urea-cycle intermediates,nitric oxide production, and
carbamoyl-phosphate
synthetase function. N. Engl. J. Med. 344, 18321838.
Penaloza, D., Arias-Stella, J., Sime, F., Recavarren, S.,
Marticorena, E.,
1964. The heart and pulmonary circulation in children at high
altitudes:
physiological, anatomical and clinical observations. Pediatrics
34, 568
582.
Penaloza, D., Gamboa, R., Dyer, J., Echevarria, M., Marticorena,
E., 1960. Theinfluence of high altitudes on the electrical activity
of the heart. I. Electro-
cardiographic and vectorcardiographic observations in the
newborn, infants,
and children. Am. Heart J. 59, 111128.
Penaloza, D., Gamboa, R., Marticorena, E., Echevarria, M., Dyer,
J., Gutierrez,
E.,1961. Theinfluence of high altitudeson theelectricalactivity
of theheart.
Electrocardiographic and vectorcardiographic observations in
adolescence
and adulthood. Am. Heart J. 61, 101115.
Reuland, D.S., Steinhoff, M.C., Gilman, R.H., Bara, M., 1991.
Prevalence and
prediction of hypoxemia in children with respiratory infections
in the Peru-
vian Andes. J. Pediatr. 119, 900906.
Robinson, P., 2000. Paediatric origins of adult lung disease:
Cystic fibrosis.
Thorax 56, 237241.
Rupert, J.L., Hochachka, P.W., 2001a. Genetic approaches to
understand-
ing human adaptation to altitude in the Andes. J. Exp. Biol.
204, 3151
3160.Rupert, J.L., Hochachka, P.W., 2001b. The evidence for
hereditary factors con-
tributing to high altitude adaptation in Andean natives: a
review. High Alt.
Med. Biol. 2, 235256.
Saldana, M., Arias-Stella, J., 1963a. Studies on the structure
of the pulmonary
trunk. I. Normal changesin theelastic configurationof thehuman
pulmonary
trunk at different ages. Circulation 27, 10861093.
Saldana, M., Arias-Stella, J., 1963b. Studies on the structure
of the pulmonary
trunk. II. The evolution of the elastic configuration of the
pulmonary trunk
in people native to high altitudes. Circulation 27,
10941100.
Scheid, P., Piiper, J., 1997. Vertebrate respiratory physiology.
In: Dantzler, W.H.
(Ed.), Comparative Physiology. Section 13, vol. 1. American
Physiological
Society, Oxford, New York, pp. 309356.
Sime, F., Banchero, N., Penaloza, D., Gamboa, R., Cruz, J.,
Marticorena, E.,
1963. Pulmonary hypertension in children born and living at high
altitudes.
Am. J. Cardiol. 11, 143149.
Skovgaard, N., Wang, T., 2006. Local control of pulmonary blood
flow and lung
structure in reptiles: implications for ventilation perfusion
matching. Respir.
Physiol. Neurobiol. 154, 107117.
Sly, P.D., 2000. Paediatric origins of adult lung disease:
introduction. Thorax
55, 585586.
Stick, S., 2000. Paediatric origins of adult lungdisease:
thecontribution of airway
development to paediatric and adult lung disease. Thorax 55,
587594.
Stinson, S., 1985. Chest dimensions of European and Aymara
children at high
altitude. Ann. Hum. Biol. 12, 333338.
Sui, G.J., Liu, Y.H., Cheng, X.S., Anand, I.S., Harris, E.,
Harris, P., Heath, D.,
1988. Subacute infantile mountain sickness. J. Pathol. 155,
161170.
Svanes, C., Omenaas, E., Jarvis, D., Chinn, S., Gulsvik, Burney,
P., 2004.
Parental smoking in childhood and adult obstructive lung
disease: results
from the European Community Respiratory Health Survey. Thorax
4,
295302.
Tucker, A., Rhodes, J., 2001. Roleof vascularsmoothmusclein
thedevelopment
of high altitude pulmonary hypertension: an interspecies
evaluation. High
Alt. Med. Biol. 2, 173189.
Victoria-Oliva, G., Mojarro-Rios, J., Alva-Espinosa, C.,
Villasis-Keever, M.,
Labarthe-Cabrera, J., Arellano-Penagos, M., Velasco-Jimenez, S.,
Alarcon-
Santos, S., Muro, R., Diaz-Arauzo, A., 1996. Ecocardiografia
Doppler en
recien nacidos con riesgo de hipertension arterial pulmonar.
Revista Mex.
Cardiol. 7, 2531.
von Mutius, E., 2000. Paediatric origins of adult lung disease:
paediatric origins
of adult lung disease. Thorax 56, 153157.
Warner, J.A., 1999. Primary sensitization in infants. Ann.
Allergy Asthma
Immunol. 83, 426430.
Weiss, K.M., 1993. Genetic variation and human disease. In:
Principles and
Evolutionary Approaches. Cambridge University Press,
Cambridge.
-
7/30/2019 Post Natal Pulmonary Adaptations
14/14
L. Huicho / Respiratory Physiology & Neurobiology 158 (2007)
190 203 203
Winslow, R.M., Monge, C.C., 1978. Hypoxia, Polycythemia, and
Chronic
Mountain Sickness. The Johns Hopkins Press, Baltimore.
Wu, T.Y., Miao, C.Y., 2002. High altitude heart disease in
children in Tibet.
High. Alt. Med. Biol. 3, 323325.
Wu, T.Y., Miao, C.Y., Lin, C., Ma, R., Yao, R., Lian, T., 1998.
Altitude illness
in children on the Tibetan plateau. In: Ohno, H., Kobayashi, T.,
Masuyama,
S., Nakashima, M. (Eds.), Progress in Mountain Medicine and High
Alti-
tude Physiology. Press Committee of the 3rd World Congress on
Mountain
Medicine and High Altitude Physiology, Matsumoto, Japan, pp.
195
200.
Wu, T.Y., Miao, C.Y., Wang, X., 2003. High altitude heart
disease in children in
Tibet. In: Viscor, G., Ricart, A., Leal, C. (Eds.), Health &
Height: Proceed-
ings of the 5th World Congress on Mountain Medicine and High
Altitude
Physiology. Universitat de Barcelona, Barcelona, Spain, pp.
291294.