Embed Size (px)
Citation preview

POST CABG CHALLENGES
Petros S. Dardas, MD, FESC
St Lukes’ Hospital
Thessaloniki, GREECE

• PROCTOR
– TAVI (MEDTRONIC)
– ROTABLATION (BOSTON)

The future: treat native coronariesinstead of SVGs?

CASE 1
• 68 MALE
• 2015 CABG
– LIMA LAD
– RIMA BIG IM
– SVG RCA
• 4 MONTHS LATER: INCREASING ANGINA

LHC• 100% LIMA LAD distally
• SEVERE STENOSIS DISTAL RIMA –IM
• 100% SVG RCA
1ST PCI • NATIVE RCA
• DISTAL RIMA - IM

1st PCI
RCA pre RCA post

1st PCI
RIMA pre RIMA post

2ND PCI
• RETROGRADE OSTIAL LAD CTO

2ND PCI
Pre 1 Pre 2

2ND PCI
Pre 3 1.5 mm balloon LMS-Cx

2ND PCI
ENHANCER RX LMS CXENHANCER RX CONFIANZA PRO -LAD

2ND PCI
TURNPIKE LP –de-escalation GAIA II GAIA II in false lumen

2ND PCI
RETROGRADE INJECTION THROUGH TURNPIKE

2ND PCI
SION inability to cross SION BLACK

2ND PCI
SION BLACK DIAGONALREVERSE CART GAIA II unable to cross

2ND PCI
REVERSE CART GAIA II unable to cross REVERSE CART PILOT 200

2ND PCI
PILOT succesfull RG3 externalization

2ND PCI
ENHANCER RX PROXIMAL LADENHANCER RX GAIA II unable to cross distally

2ND PCI
ENHANCER RX BIFURCATION LAD SEPTAL
ENHANCER RX GAIA II SUCCESFULL REENTRY TRUE LUMEN

2ND PCI
BMU true lumen LAD ballooning

2ND PCIFINAL

CASE 2
• 44 male
• Familial hyperlipidemia
• 2006:
– PCI distal RCA, ostial IM
• 2008:
– RIMA LAD

• 2 years h/o increasing SOB – stable angina
• TH SCAN: – severe inferolateral reversible defect
• LHC: – Patent RIMA
– Patent IM stent
– Long heavily calcified proximal mid RCA CTO
– Bridging collaterals – small epicardial collateral from CX

PRE

TURNPIKE SPIRAL – MIRACLE 6 –unable to cross CONFIANZA PRO 12 proximal cap

DEESCALATION MIRACLE 6 PILOT 200

GAIA II

BIG HEMATOMA

FIELDER XT - KNUCKLE

MIRACLE 12 STING RAY BALLOON

STING RAY BALLOON COAXIAL

STING RAY WIRE various attempts

PILOT 200 various attempts

PILOT 200 distally BHW distally

FINAL

CASE 3GRAFT FAILURE - PCI OF NATIVE
DISEASE
• HEAVILY CALCIFIED LESIONS-increased use of Rotablation

63 male – CABG x3 – blocked grafts –heavy calcification of native vessels
Severe LMS – prox LAD calcified disease Blocked LIMA

63 male – CABG x3 – blocked grafts –heavy calcification of native vessels
Rota 1.25 mm Rota 1.5 mm

63 male – CABG x3 – blocked grafts –heavy calcification of native vessels
FINAL 1 FINAL 2

63 male – CABG x3 – blocked grafts –heavily calcified extremely tortuous
superdominant RCA

MOTHER IN CHILD IN GRAND CHILD TECHNIQUE
6 FR GUIDEZILLA INSIDE 8 FR GUIDEZILLA
ADVANCE THE SYSTEM AS A WHOLE UNIT

MOTHER IN CHILD IN GRAND CHILD TECHNIQUE
6 FR GUIDEZILLA INSIDE 8 FR GUIDEZILLA 1.5 mm balloon cannot cross

ROTAWIREROTA 1.25 MM difficult to negotiate the bend

ROTA 1.25 mm 140000 rpm ROTA 1.25 mm 180000 rpm

ROTA 1.5 mm ROTA 2.0 mm

Post rotaMOTHER in CHILD in GRANDCHILD with balloon anchoring

MOTHER in CHILD in GRANDCHILD STENT CROSSING

63 male – CABG x3 – blocked grafts –heavy calcification of native vessels
FINAL RESULT

In Conclusion…
• Various challenges post CABG
• Require expertise in:
– Various CTO techniques
– Rotablation
– Complex high risk PCI

Rotablation in the extremies: Mechanical support assisted
unprotected left main stem rotationalatherectomy
Petros Dardas, MD, FESC
St Luke’s Hospital
Thessaloniki, GREECE

History
Past medical history• Male 61 years old,
hypertensive, non diabetic with moderate kidney disease
• 1997 Aortic Valve replacement- metallic (bicuspid aortic stenosis)
• 1997 Valvular Heart Failure (EF=35%)
• 2009 PCI Left Anterior Descending
• 2011 ICD implantation for primary prevention (EF=25%)
Cause of hospitalization
• Heart Failure Decompensation: peripheral edema + dyspnoea
• Electrical Storm: 3 ICD therapies for VF
• ECHOCARDIOGRAPHY:
– EF=15%
– Metallic Aortic Valve: normal function
– Mitral Valve: moderate to severe regurgitation

EF=15%

CORONARY ANGIOGRAPHYRCA: normal AVR: normal

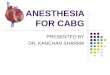
CORONARY ANGIOGRAPHYsevere heavily calcified distal LMS ostial LAD ostial CX (MEDINA
1,1,1)

Coronary angiography
• OPTIONS:– CABG – declined by surgeons
STS score >10– PCI – Rotablation without
support– PCI – Rotablation with
mechanical support
• DECISION– PCI – Rotablation with
mechanical support– IABP: Inadequate support– IMPELLA: Non applicable (AVR)
ECMO

ECMO
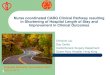
• Percutaneous femoral cannulation of both the common femoral vein (24 Fr cannula) and artery (18 Fr cannula with added distal leg perfusion branch)
• the circuit was connected to a third generation (magnetically levitated) centrifugal pump (Centrimag, Levitronix) and to a long term (low pressure) membrane oxygenator (Medtronic)
• cardiopulmonary support with flows up to
5.5 l/min

PILOT 50 LAD - FINECROSS IVUS CANNOT CROSS
PTCA: Rotablation LAD, CX, CULOTTE technique

ROTAWIRE THROUGH FINECROSS ROTABURR 1.25mm 140000rpm
PTCA: Rotablation LAD, CX, CULOTTE technique

ROTABURR 1.5mm 140000rpm POST ROTA LAD
PTCA: Rotablation LAD, CX, CULOTTE technique

ROTABURR 1.5 mm CX 140000rpm POST ROTA CX
PTCA: Rotablation LAD, CX, CULOTTE technique

STENT LAD DEPLOYED FINAL KISSING
PTCA: Rotablation LAD, CX, CULOTTE technique

PTCA: Rotablation LAD, CX, CULOTTE technique
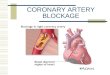
• FINAL POT 4.5 BALLOON 26 Atm

PTCA: Rotablation LAD, CX, CULOTTE techniqueFINAL RESULT

PTCA: Rotablation LAD, CX, CULOTTE techniqueFINAL IVUS RESULT

• Day 1: patient completely dependent on ECMO –pressure tracing direct line – iv inotropes
• Day 5: ECMO removed – full recovery
• Day 8: patient discharged – NYHA I – EF 35%
• Mitral Regurgitation improved grade II

PRE 15% POST 35%
EF

Conclusions (I)
• High Risk PCI is feasible if facilitated by Mechanical Circulatory Support
• IABP remains the old fashioned gold-standard• ECMO is indicated for life threatening pulmonary
or cardiac failure, when any other forms of treatment have been failed
• ECMO provides full hemodynamic support although at the expense of a higher complication rate due to the increased invasiveness of the procedure in the femoral vessels and the presence of an oxygenator which increases the inflammatory response

Conclusions (II)
• Identification of high risk patients who most likely will benefit from Mechanical Circulatory Support is crucial
• Type of Mechanical Circulatory Support depends on:
– Left Ventricular - circulatory status
– type and duration of procedure» rotablation in heavily calcified tandem lesions, where any
other method of percutaneous intervention would have failed with detrimental effect for these particular patients