Embed Size (px)
Citation preview
31-Jul-17
1
Acne in the Post-Adolescent Female
DR SHOBHAN MANOHARAN
General and Laser Dermatologist
Brisbane Skin and Westside Dermatology
dd
DISCLOSURES
Allergan
Endymed
Inova
Leo
L’Oreal
Avita
Syneron Candela
Cynosure
Post Adolescent Female Acne
5
Acne Vulgaris: One of the Most Common Global Skin Diseases1
1. Tan & Bhate. Br J Derm 2015. 2. Smith et al. Am J Clin Nutr 2007. 3. Collier et al. J Am Acad Dermatol 2008
• Estimated to affect 9.4% of the global population, making it the eighth most prevalent disease worldwide1
• In Western populations2:• 79–95% of the adolescent
population• 40–54% of individuals older than 25• 12% of women and 3% of men by
middle age
• In adults, acne may have persisted since adolescence, be late-onset, or recurrent3
69%
43%
20%
12%
67%
51%
35%
26%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pe
rce
nta
ge W
ith
Acn
e
Age (by Decade)
Men
Women
P < .0001
P < .0001
P = .0073
P = .5617
Teens 20s 30s 40s
N = 1013
Prevalence of Acne Reported By Age Group3
Adapted from Collier et al 2008
6
Acne Is Common, But Not Trivial
1. Williams et al. Lancet. 2012; 2. Collier et al. JAAD. 2008; 3. Jacob et al. JAAD. 2001;4. Yin and McMichael. Am J Clin Dermatol. 2014; 5.Silverberg. Cutis. 2013; 6. Kelly. Cosmetic Dermatol. 2003; 7. Del Rosso and Kircik. J Drugs Dermatol. 2013; 8. Taylor et al. JAAD. 2002; 9. Davis and Callender. J ClinAesthet Dermatol. 2010; 10. Williams et al. Lancet. 2012; 11. Collier et al. J Am Acad Dermatol. 2008
• May lead to scarring
• Affects up to 20% of teenagers1
• Risk increases with longer acne duration2
• More common in patients with skin of colour4-6
• May cause dyschromia
• Persistent (post-inflammatory) erythema4,5,7
• Persistent (post-inflammatory) hyperpigmentation4,5,8
• May affect self-esteem10,11
• Even mild disease can have notable impact in some patients

31-Jul-17
2
Pathophysiology
Types of lesions
“Blocked” follicle NoduleInflamed follicleMicrocomedone
Pustule
Gollnick H et al. J Am Acad Dermatol 2003; 49: S1- S37 and Galderma Data on File
Open
Comedone
“Blackhead
”
Closed
Comedone
“Whitehead”
10
Classical View of Acne Pathophysiology1-3
1. Del Rosso and Kircik. J Drugs Dermatol. 2013; 2. Williams et al. Lancet. 2012; 3. Tanghetti. J Clin Aesthet Dermatol. 2013.
Normal –appearing skin • Increased androgens/ androgen sensitivity
• Increased sebum production
• Abnormal keratinocyte proliferation
• P. acnes proliferation
• Inflammation
Microcomedone
Non-inflammatory lesions(Open and closed comedones)
Resolution/scarring/dyschromia
Inflammatory lesions(Papules/pustules/nodules/cysts)
P. acnes = Propionibacterium acnes
Four primary causes of acne1
1. Thiboutot D et al. J Am Acad Dermatol 2009; 60 : S1–50.
Propionibacterium acnes (P acnes) follicular
colonisation
Sebum production by sebaceous gland
Alteration in keratinisation process
Inflammation and immune response
HORMONE MODULATED
12
Normal-Appearing skin
Inflammation
Evolving View of Acne Pathophysiology:Inflammation Plays Key Role Throughout1,2
1. Del Rosso and Kircik. J Drugs Dermatol. 2013; 2. Tanghetti. J Clin Aesthet Dermatol. 2013.
Scar formation
Normal-appearing
skin
Dyschromia
Lesions Resolution
Subclinical inflammation
Papules, pustules,
or nodules
Micro-comedones
Open or closed
Comedones

31-Jul-17
3
Key features of acne vulgaris:
A chronic inflammatory dermatosis
Closed comedones (whiteheads) and open comedones (blackheads)
• Mainly comedones, with an occasional small inflamed papule or pustule
MILD ACNE
• Comedones and more numerous papules and pustules, with lesions confined to the face
MODERATE ACNE
Moderate – Severe acne•Comedones, inflammatory lesions•Extensive involvementtrunk and limb
Moderate acne•Comedones•Inflammatory lesions-papules and pustules•Primarily face
MODERATE TO SEVERE ACNE
• Numerous comedones, papules and pustules, spreading to the upper trunk with an occasional cyst or nodule
• Numerous painful nodular lesions on the face, neck and upper trunk
SEVERE ACNE

31-Jul-17
4
• Approach is multifactorial, targeting multiple pathogenic factors:• Sebum production
• Alteration of the keratinisation process
• P. acnes
• Inflammation
• Therapeutic goals:• Resolve existing lesions
• Prevent scarring
• Teaching to cope with psychological stress resulting from acne
Principles of acne treatmentInvestigations
• Microbial
• Endocrinological
Microbial
• In non-responders
• In sudden flares
• Rapid nodules
• Long term antibiotic usage – oral and topical
Endocrinologic
In post-pubertal females with
• Infrequent menses
• Hirsuitism
• Androgenetic alopecia
• Infertility
• PCOS
• Clitormegaly
• Truncal obesity
Tests
• Free and Total Testosterone
• DHEA-S
• Androstenedione
• LH, FSH
• Eostrogen, progesterone
• Sex hormone binding globulin
• prolactin
31-Jul-17
5
First Line Therapy - GP
Oral antibiotics – doxy, mino (50bd); erythromycin (ees ii bd)
Topical retinoids (differin, epiduo)
Topical benzyl peroxide
Topical Dapsone (Aczone)
Topical abs (duac, eryacne)
OCP (yaz, yasmin, diane)
Spironolactone
Diet
Skin care regime
BASIC SKIN CARE
• Soap free cleanser
• Light moisturiser
• Light, non-comadogenic sunscreen
• Mineral makeup
Recommendations
• Low gi
• Dairy esp skim milk may exacerbate acne
Oral Antibiotics
• Tetracyclines – doxy, mino
• Erythromycin
• Bactrim
• Moderate to severe, with inflammation
• Limit to 3 months
• Use in combination with topical retinoid
• Rotation therapy
• Flare management
M.S.
20 year old swim teacher
Mild acne over a few years
Initially on Eryacne
Then put on doxycycline for 18 months
Sudden flare of skin

31-Jul-17
6
Gram Negative Folliculitis
Long-term continuous tetracycline use
Swabs
Pseudomonas aeruginosa
Consider in non-responsive acne, or acne that flares suddenly in monomorphic form
My Mx
Pred 50
Ciprofloxacin 500mg bd
See back in 1wk with bloods for roac
Roac 20/d
Topical Antibiotics
• Erythromycin
• Clindamycin/Benzyl Peroxide
• Largely for spot treatment
• Not to be used as monotherapy – risk of bacterial resistance
• Combine with BP/retinoid
Topical Dapsone 7.5% (Aczone)
ACZONE® (dapsone) 7.5% w/w Topical gel: A Product for the Topical Treatment of Acne
• Once-daily dosing1
• Proven efficacy and tolerability1,2
• Studied in large pivotal trials
used for a topical acne drug2
• 4340 acne patients studied2
• 100% had moderate acne1,3
• Features a pump design1
1. ACZONE® Gel 7.5% w/w topical gel Australian Approved Product Information. 2. Thiboutot DM et al. J Clin Aesthet Dermatol2016; 9(10): 18-27. 3. Eichenfield MD et al. J Drugs in Dermatol 2016; 15(8) 962-69

31-Jul-17
7
Study objective:
• To assess the safety and efficacy of dapsone 7.5% versus vehicle control administered topically once daily for 12 weeks in patients with acne vulgaris
End Points
• Co-primary:
– Global Acne Assessment Score (GAAS) success at week 12
– Mean reduction in inflammatory and noninflammatory lesion counts at week 12
• Secondary:
– Mean reduction in total lesions at week 12
– Percent reduction at week 12 for total, inflammatory, and noninflammatory lesion counts
Patients:
• ≥ 12 years of age with 20 to 50 inflammatory lesions and 30 to 100 noninflammatory lesions on the face at screening and baseline and with a score of 3 (moderate) on the GAAS
Study Design: Two Multicenter, Randomized,Double-blind, Vehicle-controlled, Parallel-group Studies1,2
1. ACZONE® 7.5% w/w Topical Gel Australian Approved Product Information; 2 Thiboutot DM et al. J Clin Aesthet Dermatol 2016; 9(10): 18-27..
QD = once daily; R = 1:1 randomization.
Vehicle gel (n = 2178) QD; R
0 2 41 8 12Dapsone gel(n = 2162) QD; R
TotalPatientsN = 4340
Randomized1
Weeks
Pivotal Clinical Data:Efficacy and Safety
Pooled Analysis of Pivotal Trial Data
Clinical Success: Percentage of ACZONE® (dapsone) 7.5% w/w gel Patients With GAAS of 0 or 1 at Week 12
* as assessed by the investigator
1. ACZONE® 7.5% w/w Topical Gel Australian Approved Product Information; 2. . Thiboutot DM et al. J Clin Aesthet Dermatol 2016; 9(10): 18-27.
.
Patients Achieved Success at Week 12 With a Score of 0 or 1 on the Global Acne Assessment
Score (GAAS) Scale1,2
30%
644 21%
4600%
20%
40%
60%
80%
100%
Total
AC
ZO
NE
®7.5
% P
erc
en
tag
e o
f Pa
tie
nts
Ac
hie
vin
g G
AA
S S
uc
ce
ss
ACZONE
Vehicle
P < .001
ACZONE® (dapsone) 7.5% w/w gel (n = 2162)
Vehicle (n = 2178) GAAS Scale2, *
0 = none
1 = minimal
2 = mild
3 = moderate
4 = severe
Effect of Once-Daily Application of ACZONE® (dapsone) 7.5% w/w Topical gel
1. Data on file, Allergan, 2016; Study Photos.
Actual, unretouched photos of an ACZONE® 7.5% w/w Topical Gel patient.1 Individual
results may vary.
Lesion Count Reductions
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%
0 1 2 3 4 5 6 7 8 9 10 11 12
Mea
n P
erce
nta
ge R
edu
ctio
nFr
om
Bas
elin
e
Week
Aczone Vehicle
(29.2) ACZONE® 7.5% w/w Topical gel
(29.7) Vehicle
-48.1%
(-13.9)
-54.6%
(-15.8)
P < .001
ACZONE® (dapsone) 7.5% w/w gel (n = 2162)
Vehicle (n = 2178)
Study design: Pooled analysis of 4,340 patients in 2 identical, 12-week, multicenter, randomized, double-blind, vehicle-controlled,parallel-group studies.
P<0.01
P<0.001
P<0.001
Adapted from Thiboutot 2016
Inflammatory Lesion Count Reduction At Week 121,*
1. Thiboutot DM et al. J Clin Aesthet Dermatol 2016; 9(10): 18-27.
31-Jul-17
8
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%
0 1 2 3 4 5 6 7 8 9 10 11 12
Me
an
Pe
rce
nta
ge
Re
du
ctio
n
Fro
m B
ase
line
Week
Aczone
Vehicle
(46.8) ACZONE® 7.5% w/w Topical gel
(47.6) Vehicle
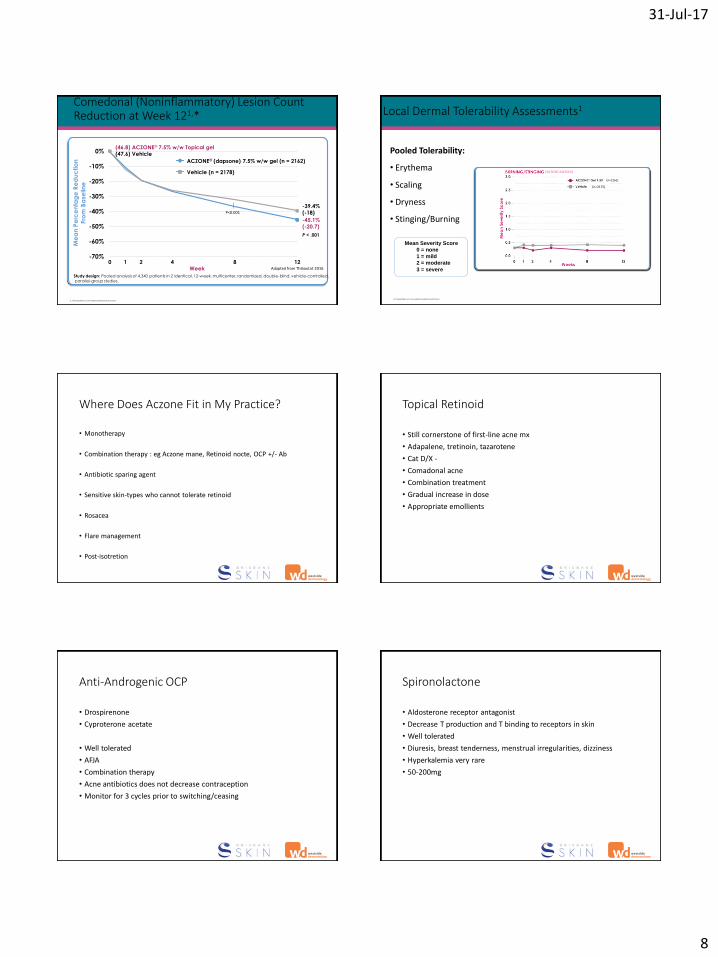
-39.4%
(-18)
-45.1%
(-20.7)
P < .001
ACZONE® (dapsone) 7.5% w/w gel (n = 2162)
Vehicle (n = 2178)
Comedonal (Noninflammatory) Lesion Count Reduction at Week 121,*
1. ThiboutotDM et al. J Clin Aesthet Dermatol 2016; 9(10): 18-27.
.
P<0.001
Adapted from Thiboutot 2016
Study design: Pooled analysis of 4,340 patients in 2 identical, 12-week, multicenter, randomized, double-blind, vehicle-controlled,parallel-group studies.
Local Dermal Tolerability Assessments1
Pooled Tolerability:
• Erythema
• Scaling
• Dryness
• Stinging/Burning
1. ThiboutotDM et al. J Clin Aesthet Dermatol 2016; 9(10): 18-27.
.
Mean Severity Score
0 = none
1 = mild
2 = moderate
3 = severe
(n=2175)
(n=2161)
(PATIENT ASESSED)
Where Does Aczone Fit in My Practice?
• Monotherapy
• Combination therapy : eg Aczone mane, Retinoid nocte, OCP +/- Ab
• Antibiotic sparing agent
• Sensitive skin-types who cannot tolerate retinoid
• Rosacea
• Flare management
• Post-isotretion
Topical Retinoid
• Still cornerstone of first-line acne mx
• Adapalene, tretinoin, tazarotene
• Cat D/X -
• Comadonal acne
• Combination treatment
• Gradual increase in dose
• Appropriate emollients
Anti-Androgenic OCP
• Drospirenone
• Cyproterone acetate
• Well tolerated
• AFJA
• Combination therapy
• Acne antibiotics does not decrease contraception
• Monitor for 3 cycles prior to switching/ceasing
Spironolactone
• Aldosterone receptor antagonist
• Decrease T production and T binding to receptors in skin
• Well tolerated
• Diuresis, breast tenderness, menstrual irregularities, dizziness
• Hyperkalemia very rare
• 50-200mg
31-Jul-17
9
Second Line Therapies – When to refer?
Unresponsive to first line agents
Truncal acne
Evidence of early scarring
Darker skin types
Second Line Therapies
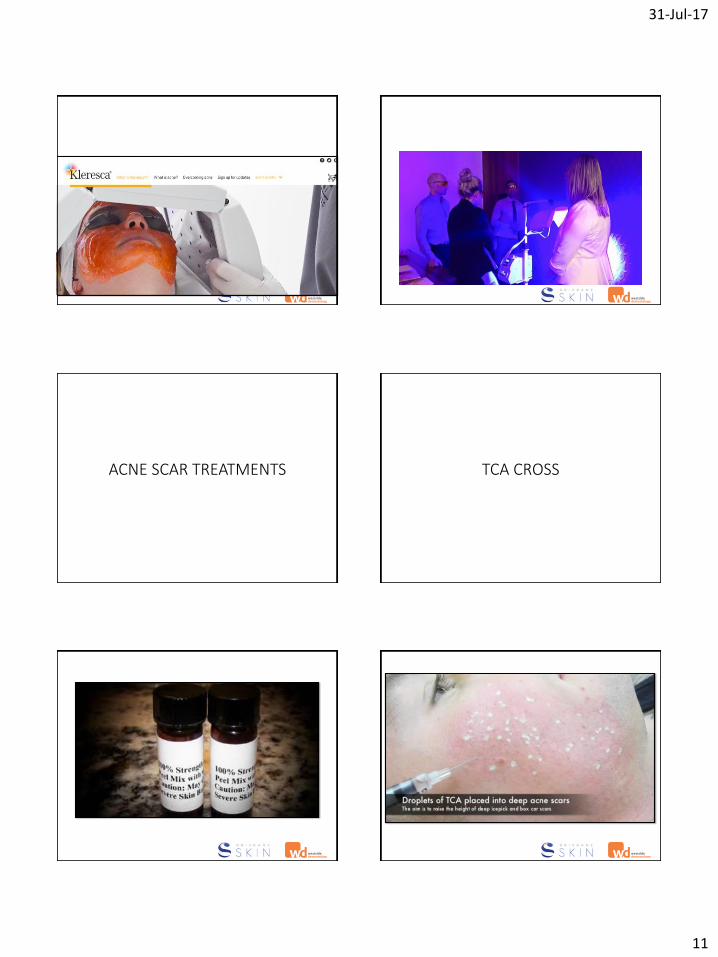
Chemical peels
Laser and Light treatments
Comadonal Extractions
Isotretionoin
Oral Isotretinoin
Indicated in:
Nodular acne and severe variants
Not responding to other therapy
Scarring + postinflammatory hyperpigmentation
Darker skin types – lower threshold
Acne excoriae
• Pregnancy category X
• 1 month wash-out only
• Often combination on commencement to reduce flares – Abs, Pred, Aczone
• 6-12 mth Rx – longer in some, esp if Hx of PCOS
• Baseline and f/u ELFTs, Chol, TG
• Low dose routine often favoured – less SES, higher compliance, similar efficacy in most acne
PHYSICAL THERAPIES FOR ACNE

31-Jul-17
10
31-Jul-17
11
ACNE SCAR TREATMENTS TCA CROSS
31-Jul-17
12
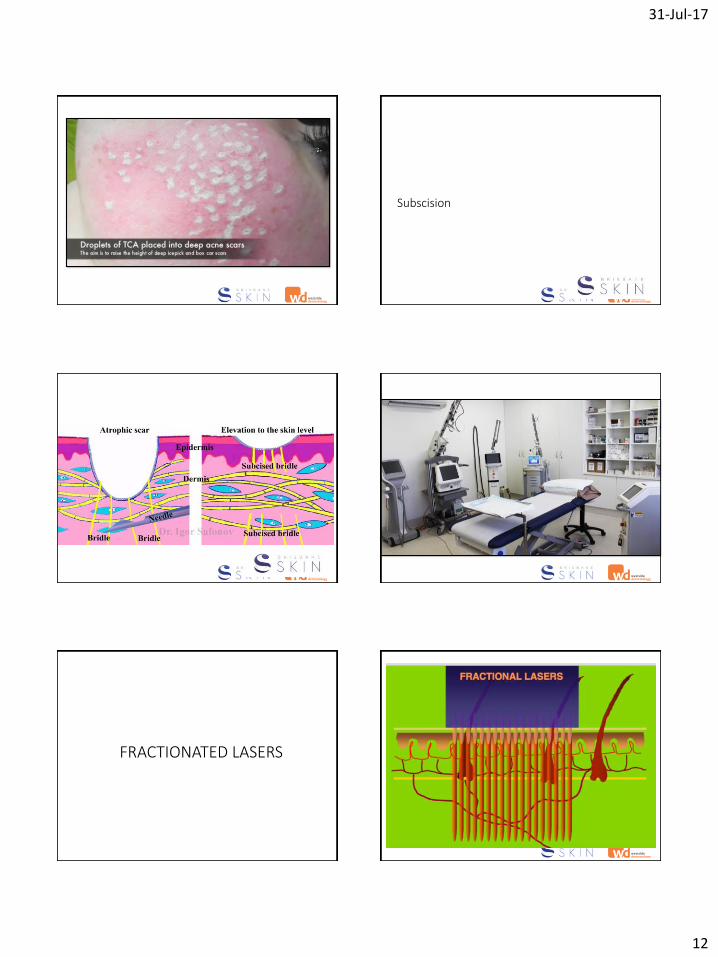
Subscision
FRACTIONATED LASERS

31-Jul-17
13
Benefits of Fractionation
• Less discomfort
• Less downtime, quicker heal
• Ability to penetrate deeper than with fully ablative settings.
• Ability to treat darker skin-types (IV-VI)
• Less complications (PIH and scarring)
• Ability to treat off the face (neck, chest, arms)
RADIOFREQUENCY
ABLATIVE LASER ReCell
31-Jul-17
14
ReCell
• The ReCell Autologous Cell Harvesting Device creates an epithelial suspension which can be used to promote repigmentation and wound healing.
• FTSG or SSG processed into a non-cultured autologous suspension containing multiple skin cell phenotypes, including melanocytes.
• Immediate application to a wound bed, typically
prepared using dermabrasion or ablative laser.
• Removes need for wet lab.
FILLERS

31-Jul-17
15
Newstead I Manly I North Lakes