Embed Size (px)
Citation preview

Eur Radiol (2010) 20: 1651–1656DOI 10.1007/s00330-009-1704-z GASTROINTESTINAL
Perry J. PickhardtSteven M. WiseDavid H. Kim
Received: 11 September 2009Accepted: 12 November 2009Published online: 13 January 2010# European Society of Radiology 2009
Positive predictive value for polyps detected
at screening CT colonography
Abstract Purpose: To determine thepositive predictive value (PPV) forpolyps detected at CT colonography(CTC). Methods: Assessment of 739colorectal lesions ≥6 mm detectedprospectively at CTC screening in479 patients was performed. By-polypPPV was analyzed according to small(6–9 mm) versus large (≥10 mm) size;morphology (sessile/pedunculated/flat); diagnostic confidence level(3 = most confident, 1 = leastconfident); and histology. By-patientPPV was analyzed at various polypsize thresholds. Results: By-polypPPV for CTC-detected lesions≥6 mm, 6–9 mm, and ≥10 mm was91.6% (677/739), 90.1% (410/451),and 92.7% (267/288), respectively(p=0.4). By-polyp PPV according tosessile, pedunculated, flat, and mass-like morphology was 92.5%(441/477), 96.5% (139/144), 77.7%(73/94), and 97.6% (40/41), respec-tively (p<0.0001 for flat versus
polypoid morphology). By-polypPPV according to diagnostic confi-dence level was 94.7% (554/585) forhighest (= level 3), 83.5% (106/127)for intermediate (= level 2), and63.0% (17/27) for lowest (= level 1)confidence (p<0.0001 for levels-2/3versus level-1). By-patient PPV at6-mm, 8-mm, 10-mm, and 30-mmpolyp size thresholds was 92.3%(442/479), 93.0% (306/329), 93.1%(228/245), and 97.4% (38/39),respectively. Conclusion: Theoverall per-polyp and per-patient PPVfor lesions ≥6 mm was 92% forCTC screening. Increased diagnosticconfidence and polypoid (non-flat)morphology correlated with a higherPPV, whereas small versus largepolyp size had very little effect.
Keywords CT colonography . Virtualcolonoscopy . Colorectal cancerscreening . Polyps
Introduction
CT colonography (CTC) has been shown in recent clinicalvalidation and comparison trials to be comparable to opticalcolonoscopy (OC) for the screen detection of advancedneoplasia [1–3]. Broad consensus among radiologists onthe general application of CTC as a clinical tool has beenachieved [4, 5]. To function as a clinically efficacious andcost-effective screening tool, CTC must not only be sensi-tive for lesion detection, but also demonstrate a reasonablylow false-positive rate [6–8]. In contrast to validation trialswhere OC is performed in all subjects [1, 3], including those
with negative CTC results, the sensitivity and specificity ofCTC (relative to OC) cannot be measured in clinicalpractice. The reason for this is that negative CTC cases arenot referred to OC and thus cannot be stratified into true-negative versus false-negative results. However, becauseboth true-positive and false-positive CTC results can betracked in clinical practice, the positive predictive value(PPV) of CTC screening can be obtained and will likelybe an important quality assurance measure going for-ward. The purpose of this study was to determine thePPV of our CTC screening program for the detection ofrelevant colorectal lesions (≥6 mm), and to assess the
P. J. Pickhardt (*) . S. M. Wise .D. H. KimDepartment of Radiology,University of Wisconsin Schoolof Medicine and Public Health,E3/311 Clinical Science Center, 600Highland Ave.,Madison, WI, 53792-3252, USAe-mail: [email protected].: +1-608-2639028Fax: +1-608-2630140

influence of lesion size, morphology, and diagnosticconfidence on the PPV.
Material and methods
This Health Insurance Portability and Accountability Act(HIPAA)-compliant study was approved by our institu-tional review board (IRB); the need for signed informedconsent was waived due to the retrospective nature ofassessment. A total of 5,124 consecutive ambulatoryadults (2,792 women and 2,332 men) underwent CTCscreening at a single medical center over a 52-monthinterval. The mean age of this screening population was56.9 years.
Bowel preparation the evening before CTC screeningconsisted of a saline laxative (2 doses of 296 ml magne-sium citrate or 1–2 doses of 45 ml sodium phosphate) andoral contrast agents (250 ml 2% w/v barium sulfate and60 ml diatrizoate [Gastroview, Covidien]). Bowel disten-tion for CTC was achieved with automated carbon dioxidedelivery (PROTOCO2L, Bracco Diagnostics), except foran early subset of 419 patients who underwent room airinsufflation. Supine and prone acquisitions were obtainedwith 8- or 16-channel multi-detector CT scanners (Light-Speed Series, GE Healthcare), with 1.25-mm collimation,kVp of 120, 50–75 mAs or modulated tube current withnoise index set at 50 and mA range of 30–300 mA, and1-mm reconstruction interval. For cases with inadequatesegmental distention in the same location on both supineand prone positioning, an additional decubitus view wasalso obtained—typically right lateral decubitus positionto optimize sigmoid distention.
Prospective CTC study interpretation for polyp detectionwas performed using a dedicated workstation (V3D Colon,Viatronix). The studies were read by a one of five abdominalradiologists, all with extensive experience in CTC inter-pretation (>500 cases). A hybrid 3D and 2D polyp detectionapproach was used, with 2D correlation to confirm softtissue composition of all suspicious lesions. Lesion mea-surement was performed using combined 2D and 3Dassessment in a manner that has been previously described[9]. For all polyps measuring ≥6 mm, the lesion size,morphology, segmental location, and diagnostic confidencelevel were prospectively recorded.
Polyp size was categorized as small for 6–9 mm lesionsand large for all lesions measuring 10 mm or greater.Lesion morphology was characterized as sessile, pedun-culated, flat, or mass-like. Pedunculated lesions had adefinable stalk of attachment separate from the polyp head.Flat lesions are a subset of sessile polyps that have aplaque-like morphology and generally measure 3 mm orless in height (and always measure less than half as tall aswide) [10, 11]. Masses were defined as ≥3 cm and weresubclassified as carpet lesions when relatively flat todistinguish them from polyps, annular, or semi-annular
masses. Polyp location was scored according to the sixsegments: cecum, ascending, transverse, descending, sig-moid, and rectum. Diagnostic confidence was prospec-tively assigned by the interpreting radiologist using apreviously validated three-point scale [12], ranging fromhighest confidence (= level 3) to lowest confidence (= level1), with level-2 confidence being intermediate. Diagnosticconfidence scoring is somewhat subjective. However, atypical level-3 lesion would be composed of homogeneoussoft tissue attenuation and its site of attachment to thebowel wall would remain fixed in position between supineand prone. In comparison, a typical level-1 confidencefinding might be fairly subtle, associated with suboptimalpreparation or distention, and perhaps clearly identified ononly one view.
According to our diagnostic algorithm, all patients withpolyps ≥6 mm detected at CTC screening were offeredsame-day OC for polypectomy, unless contraindicated by apatient factor such as anticoagulation therapy. In addition,patients with one or two small (6–9 mm) polyps were givenan alternative option of short-term CTC surveillance. Theinclusion criterion for this study consisted of all CTC-detected lesions ≥6 mm that underwent subsequent OCevaluation. Lesion measurement at OC was performedusing visual comparison against an open forceps, calibratedguidewire, or other endoscopically inserted device. Forlesion matching at CTC and OC, a standard algorithm wasapplied that required concordance for both lesion size(within 50%) and location (same or adjacent segment) [3].For most patients, polyp matching was very straightfor-ward. For any case where the matching was difficult orambiguous (e.g., multiple lesions of varying sizes), anadditional consensus review was performed for reconcilia-tion, consisting of two or more experienced CTCradiologists. Any fixed and focal mucosal-based anatomicabnormality called at OC was considered a potentialcandidate for matching with CTC (assuming appropriatesize and location), regardless of end histology (e.g.,adenomatous, hyperplastic, normal mucosa, juvenile,inflammatory, lymphoid, etc.). Some matching lesionssuch as venous blebs, were not biopsied, whereas someother matching lesions were fulgurated or could not beretrieved. Adherent stool was always considered a false-positive result.
A matched lesion (CTC–OC concordance) was con-sidered a CTC true positive, whereas a CTC false positivelacked a matching correlate at OC. The CTC positivepredictive value (PPV) was defined as = (CTC TP)/(CTCTP + CTC FP). True-positive versus false-positive matcheswere assessed by-polyp in terms of lesion size, morphology,diagnostic confidence, and histology. PPVon a per-patientbasis required at least one matching lesion at OC for apatient to be considered a true positive. Per-patient PPVwas assessed at 6-mm, 8-mm, 10-mm, and 30-mm polypsize thresholds. The false-positive rate (FPR) was definedas 1−PPV.
1652
Statistical analysis
Fisher’s exact test was used to assess for statisticalsignificance between predictive values according to thecategories of lesion size, morphology, and diagnosticconfidence. A p value <0.05 was considered to bestatistically significant.
Results
From the entire screening cohort of 5,124 subjects under-going CTC, a total of 639 patients had at least one lesion≥6 mm, corresponding to a test positive rate of 12.5%. Ofthese 639 patients with 958 total lesions ≥6 mm, 160patients with 219 polyps undergoing CTC surveillancewere excluded from further analysis, leaving a study cohortof 479 patients with 739 lesions ≥6 mm that were evaluatedby OC.
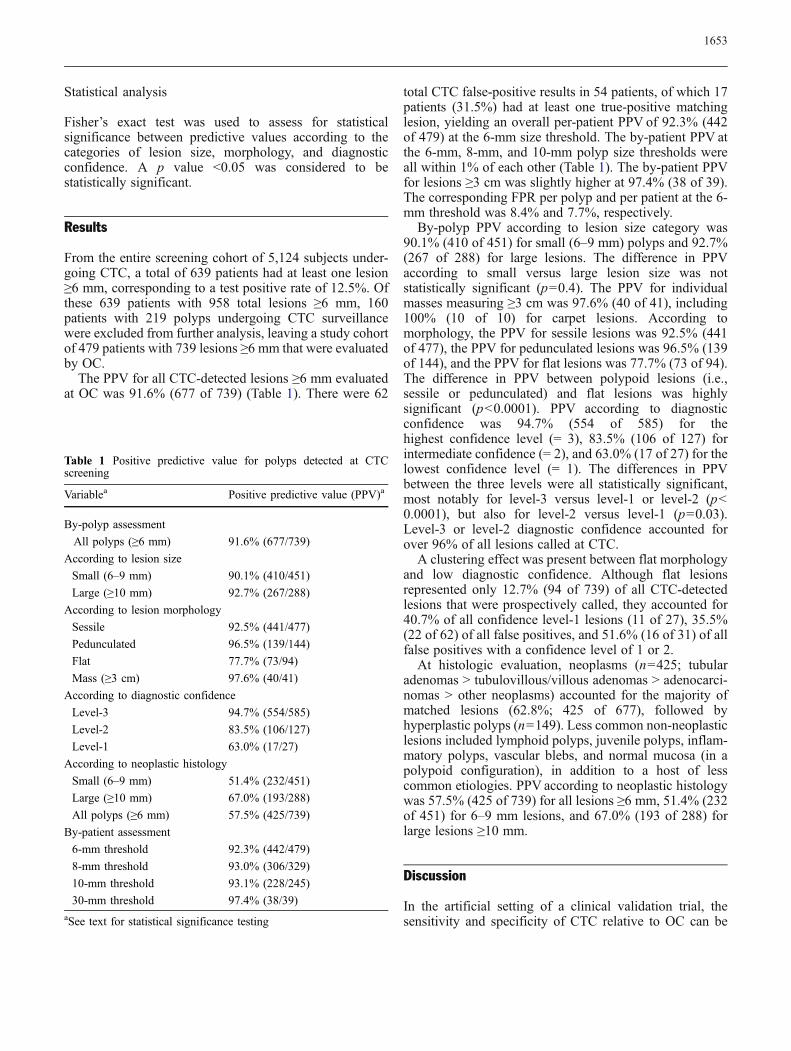
The PPV for all CTC-detected lesions ≥6 mm evaluatedat OC was 91.6% (677 of 739) (Table 1). There were 62
total CTC false-positive results in 54 patients, of which 17patients (31.5%) had at least one true-positive matchinglesion, yielding an overall per-patient PPV of 92.3% (442of 479) at the 6-mm size threshold. The by-patient PPV atthe 6-mm, 8-mm, and 10-mm polyp size thresholds wereall within 1% of each other (Table 1). The by-patient PPVfor lesions ≥3 cm was slightly higher at 97.4% (38 of 39).The corresponding FPR per polyp and per patient at the 6-mm threshold was 8.4% and 7.7%, respectively.
By-polyp PPV according to lesion size category was90.1% (410 of 451) for small (6–9 mm) polyps and 92.7%(267 of 288) for large lesions. The difference in PPVaccording to small versus large lesion size was notstatistically significant (p=0.4). The PPV for individualmasses measuring ≥3 cm was 97.6% (40 of 41), including100% (10 of 10) for carpet lesions. According tomorphology, the PPV for sessile lesions was 92.5% (441of 477), the PPV for pedunculated lesions was 96.5% (139of 144), and the PPV for flat lesions was 77.7% (73 of 94).The difference in PPV between polypoid lesions (i.e.,sessile or pedunculated) and flat lesions was highlysignificant (p<0.0001). PPV according to diagnosticconfidence was 94.7% (554 of 585) for thehighest confidence level (= 3), 83.5% (106 of 127) forintermediate confidence (= 2), and 63.0% (17 of 27) for thelowest confidence level (= 1). The differences in PPVbetween the three levels were all statistically significant,most notably for level-3 versus level-1 or level-2 (p<0.0001), but also for level-2 versus level-1 (p=0.03).Level-3 or level-2 diagnostic confidence accounted forover 96% of all lesions called at CTC.
A clustering effect was present between flat morphologyand low diagnostic confidence. Although flat lesionsrepresented only 12.7% (94 of 739) of all CTC-detectedlesions that were prospectively called, they accounted for40.7% of all confidence level-1 lesions (11 of 27), 35.5%(22 of 62) of all false positives, and 51.6% (16 of 31) of allfalse positives with a confidence level of 1 or 2.
At histologic evaluation, neoplasms (n=425; tubularadenomas > tubulovillous/villous adenomas > adenocarci-nomas > other neoplasms) accounted for the majority ofmatched lesions (62.8%; 425 of 677), followed byhyperplastic polyps (n=149). Less common non-neoplasticlesions included lymphoid polyps, juvenile polyps, inflam-matory polyps, vascular blebs, and normal mucosa (in apolypoid configuration), in addition to a host of lesscommon etiologies. PPV according to neoplastic histologywas 57.5% (425 of 739) for all lesions ≥6 mm, 51.4% (232of 451) for 6–9 mm lesions, and 67.0% (193 of 288) forlarge lesions ≥10 mm.
Discussion
In the artificial setting of a clinical validation trial, thesensitivity and specificity of CTC relative to OC can be
Table 1 Positive predictive value for polyps detected at CTCscreening
Variablea Positive predictive value (PPV)a
By-polyp assessment
All polyps (≥6 mm) 91.6% (677/739)
According to lesion size
Small (6–9 mm) 90.1% (410/451)
Large (≥10 mm) 92.7% (267/288)
According to lesion morphology
Sessile 92.5% (441/477)
Pedunculated 96.5% (139/144)
Flat 77.7% (73/94)
Mass (≥3 cm) 97.6% (40/41)
According to diagnostic confidence
Level-3 94.7% (554/585)
Level-2 83.5% (106/127)
Level-1 63.0% (17/27)
According to neoplastic histology
Small (6–9 mm) 51.4% (232/451)
Large (≥10 mm) 67.0% (193/288)
All polyps (≥6 mm) 57.5% (425/739)
By-patient assessment
6-mm threshold 92.3% (442/479)
8-mm threshold 93.0% (306/329)
10-mm threshold 93.1% (228/245)
30-mm threshold 97.4% (38/39)aSee text for statistical significance testing
1653

calculated, assuming that all patients undergo bothprocedures. However, in actual clinical practice, theseperformance measures cannot be obtained because onlypositive CTC cases are referred to OC for polypectomy,precluding assessment of the false-negative and true-negative rates. Performance measures that can be obtainedin routine clinical CTC practice include the test positiverate, the false-positive rate (FPR), and the positivepredictive value (PPV). Therefore, these values willnecessarily become important parameters for programquality metrics and for comparison with other clinicalprograms.
Our results demonstrate a very high PPV for our clinicalscreening program, indicating strong concordance betweenpositive findings at CTC and subsequent evaluation at OC.PPV for all CTC-detected non-diminutive polyps was 92%for individual lesions, as well as at the patient level,corresponding to false-positive rates of less than 10%. Toour knowledge, this is the largest study investigating PPVfor CTC-detected polyps. Perhaps most noteworthy is thefact that these PPV values are substantially increasedcompared with the two large published multi-center CTCscreening trials [1, 3]. In the Department of Defense (DoD)screening trial [3], the per-patient PPV was 41% at the6-mm threshold, similar to the PPV of 40% in the sub-sequent ACRIN trial [1]. However, it must be noted thatthese values are lowered in part by the fact that onlyneoplastic lesions (adenomas and cancers) were con-sidered as a true-positive result. When all matched lesionsare included, regardless of histology, the 6-mm per-patientPPV in the DoD trial increased to 59% [13], still wellbelow our current results. Similarly, the IMPACT trial,which evaluated a symptomatic cohort, reported a per-patient PPV of 61.9%, but this result was derivedspecifically for identifying patients with at least onadvanced neoplasm—not all lesions ≥6 mm [14].
One could reasonably question whether we are now justcalling the more obvious lesions at CTC, perhaps account-ing for the high PPV. This concern for the possibility of falsenegatives in our CTC screening program was actually theimpetus behind our previous study comparing the rates ofadvanced neoplasia detection at CTC versus OC screening[2]. In this study, we found that CTC screening actually ledto the removal of more advanced neoplasms, the main targetfor colorectal screening and prevention, despite the fact thatonly 8% of adults screened by CTC were referred to OC. Inaddition, the test positive rates for CTC and OC weresimilar at both the 6-mm (13%) and 10-mm (4–5%) sizethresholds. These data are very reassuring and suggest thatCTC screening is achieving a very high sensitivity andspecificity in clinical practice. It is important to note thatalthough a small subset of patients may elect to undergoCTC surveillance of small polyps, this does not directlyaffect the PPV for 6–9 mm lesions since these cases are notconsidered. Rather, it merely changes the relative propor-tion of small and large lesions going to OC. Because PPV
does not appear to significantly vary between small andlarge polyps, the overall PPV is also not substantiallyaffected.
When patients with a positive CTC are sent to OC, thereare sometimes additional lesions found at OC that were notreported at CTC. However, in our experience, over 70% ofthese additional lesions are diminutive in size (5 mm orsmaller) [15], which are generally not reported at CTC[5, 16]. A number of these diminutive polyps can beidentified at prospective CTC, but we do not individuallycharacterize and catalogue these lesions. However, in thesetting of larger co-existing lesions, we may incidentallymention their likely presence to the endoscopist. In terms ofhistology, over 70% of all additional polyps seen at OC thatwere not called at CTC are hyperplastic in our experience[15]. Furthermore, less than 3% of additional lesions haveproven to be large adenomas, without any additionalcancers uncovered to date.
We evaluated several factors in order to determine theireffect on PPV. Both polyp morphology and diagnosticconfidence had a strong influence on PPV, whereas smallversus large lesion size did not. The uniform PPV resultsfor small and large lesions at both by-polyp and by-patientassessments are striking and reinforces how continuedimprovements in CTC technique and interpretation haveimproved performance down to the 6-mm size threshold.Perhaps not surprisingly, a polypoid morphology (i.e.,sessile or pedunculated) was associated with a significantlyhigher PPV compared with flat lesions. A higher diagnosticconfidence by the interpreting radiologist was also asso-ciated with a significantly higher PPV. Similar trends werenoted in the DoD trial [12]. Importantly, although flatlesion morphology and low diagnostic confidence tendedto cluster together, they both accounted for a small minorityof each classification schema. In addition, although true flatlesions are less conspicuous at both CTC and OC, theyactually tend to be much less histologically aggressivecompared with polypoid lesions in our screening popula-tion [11]. Perhaps the common misperception that flatlesions are more ominous than sessile or pedunculatedpolyps has resulted in a tendency to overcall subtlepotential flat lesions at CTC. Alternatively, it is alsopossible that some unmatched CTC-detected flat lesionsare being missed at subsequent OC. In contrast, large flatmasses (carpet lesions) had a high concordance at CTC–OCevaluation.
It is interesting that small (6–9 mm) versus large(≥10 mm) lesion size had relatively little impact on PPV.In the DoD trial, the overall per-patient PPV was 67% atthe 10-mm threshold, compared with 59% at the 6-mmthreshold [13]. However, in the ACRIN trial, there wasactually a decrease in per-patient PPV for larger adenomasizes, dropping to 23% at the 10-mm threshold, comparedwith 40% at 6 mm [1]. This paradoxical result from theACRIN trial is difficult to explain, but could potentially berelated to overcalling of large lesions in order to maintain a
1654

reasonable detection sensitivity. Regardless, the highperformance of CTC for small lesions in the currentstudy is likely multi-factorial, related in part to incrementalimprovements in bowel preparation, colonic distention,multi-detector CT scanners, and the CTC softwarecapabilities. Increased experience of the interpretingradiologists must also be considered as an importantpotential contributing factor. However, if quality initiativesin regards to training, technique, and performance resultsare uniformly applied, we believe that our results aregeneralizable to a wide variety of radiology practicesettings. Demanding a PPVof 90% is probably not realistic,as this concordance level is dependent upon excellentperformance at both CTC and OC, which may not alwaysbe attainable. Nonetheless, we believe a PPV on the orderof 70–80% is achievable, which is considerably higher thanthe published validation trials.
If the results for PPV in our clinical practice can bereproduced by others, this would have a dramatic impactupon the overall clinical efficacy and cost-effectiveness ofthis screening tool. Such information may help to convincelate-adopting physicians to consider CTC as a viablescreening option for their patients. Even though a numberof prior cost-effectiveness analyses have concluded thatCTC is cost-effective [17–19], the input assumptions forCTC performance were much more pessimistic comparedwith what we see in actual practice.
Because some discrepant (unmatched) lesions willactually represent colonoscopy misses and not CTCovercalls, the term “CTC–OC concordance rate” may bemore suitable than PPV. A CTC false-positive result wasdefined as any CTC-detected lesion without a matching OCcorrelate, which can result from either a CTC false positiveor an OC false negative. Even though the endoscopist isunblinded to the CTC results in clinical practice, there willstill be some real lesions that cannot be found at OC. In theDoD or ACRIN trials, such instances would have beenunavoidably mislabeled as CTC false positives. The overalleffect of these OC false-negative cases upon the CTC PPV
is probably relatively small. For all discordant cases, wereview the original CTC findings to determine if thefinding remains concerning for a possible OC falsenegative. In such cases, we generally arrange for a repeatCTC examination, with variable time interval that dependsupon the relative importance of the finding. We did notdirectly address this issue in the current study but plan tosystematically investigate this in a future project, after allfurther work-up has been completed. An additional poten-tial issue is difficulty in lesion matching between CTC andOC [20], but we have found this to be less problematic inclinical practice compared with the artificial trial setting,perhaps due in part to the unblinded nature of endoscopyfollowing positive CTC.
We have found that the prospective diagnostic con-fidence level of the interpreting radiologist is a usefulconsideration in clinical practice. For example, commu-nicating the possibility of a lower confidence level for agiven CTC-detected lesion to the endoscopist may preventan unnecessarily prolonged investigation if the lesioncannot be found. Alternatively, when we communicate ahigh diagnostic confidence level for a given CTC-detectedlesion, the endoscopist will be more motivated to prolongthe search. This is especially important for lesions locatedin relative blind spots for OC, most notably the back sidesof folds within the right colon [21].
In summary, the overall per-polyp and per-patient PPVwas 92% for non-diminutive CTC-detected lesions in ourclinical screening program. An increased diagnosticconfidence level and a polypoid (non-flat) morphologyboth correlated with a higher PPV, whereas small versuslarge polyp size had relatively little effect. If these resultscan be widely reproduced by other practices, CTC maybecome a more appealing primary screening option forpatients, referring physicians, and third-party payers.
Acknowledgements Dr. Pickhardt and Dr. Kim are consultants forMedicsight and Viatrox and are co-founders of VirtuoCTC.
References
1. Johnson CD, Chen MH, Toledano AYet al (2008) Accuracy of CTcolonography for detection of largeadenomas and cancers. N Engl J Med359:1207–1217
2. Kim DH, Pickhardt PJ, Taylor AJ et al(2007) CT colonography versuscolonoscopy for the detection ofadvanced neoplasia. N Engl J Med357:1403–1412
3. Pickhardt PJ, Choi JR, Hwang I et al(2003) Computed tomographic virtualcolonoscopy to screen for colorectalneoplasia in asymptomatic adults. NEngl J Med 349:2191–2200
4. Taylor SA, Laghi A, Lefere P, HalliganS, Stoker J (2007) European society ofgastrointestinal and abdominal radiolo-gy (ESGAR): consensus statement onCT colonography. Eur Radiol 17:575–579
5. Zalis ME, Barish MA, Choi JR et al(2005) CT colonography reporting anddata system: a consensus proposal.Radiology 236:3–9
6. Mavranezouli I, East JE, Taylor SA(2008) CT colonography and cost-effectiveness. Eur Radiol. doi:10.1007/s00330-008-1058-y
7. Laghi A (2005) Virtual colonoscopy:clinical application. Eur Radiol 15Suppl 4:D138–141
8. Pickhardt PJ (2005) Virtualcolonoscopy: issues related toprimary screening. Eur Radiol 15:D133–D137
1655

9. Pickhardt PJ, Lee AD, McFarland EG,Taylor AJ (2005) Linear polyp mea-surement at CT colonography: in vitroand in vivo comparison of two-dimen-sional and three-dimensional displays.Radiology 236:872–878
10. Dachman AH, Zalis ME (2004) Qualityand consistency in CT colonographyand research reporting. Radiology230:319–323
11. Pickhardt PJ (2009) CT colonography:time for clinical implementation. NatRev Clin Oncol 6:187–188
12. Pickhardt PJ, Choi JR, Nugent PA,Schindler WR (2004) The effect ofdiagnostic confidence on theprobability of optical colonoscopicconfirmation of potential polypsdetected on CT colonography:prospective assessment in 1,339asymptomatic adults. AJR Am JRoentgenol 183:1661–1665
13. Pickhardt PJ (2005) Limitations ofvirtual colonoscopy - in response. AnnIntern Med 142:155–155
14. Regge D, Laudi C, Galatola G et al(2009) Diagnostic accuracy of com-puted tomographic colonography forthe detection of advanced neoplasia inindividuals at increased risk of colo-rectal cancer. JAMA 301:2453–2461
15. Cornett D, Barancin C, Roeder B et al(2008) Findings on optical colonoscopyafter positive CT colonography exam.Am J Gastroenterol 103:2068–2074
16. Pickhardt PJ (2007) Screening CTcolonography: how I do it. AJR Am JRoentgenol 189:290–298
17. Hassan C, Pickhardt P, Laghi A et al(2008) Computed tomographiccolonography to screen for colorectalcancer, extracolonic cancer, and aorticaneurysm. Arch Intern Med 168:696–705
18. Pickhardt PJ, Hassan C, Laghi A, ZulloA, Kim DH, Morini S (2007) Cost-effectiveness of colorectal cancerscreening with computed tomographycolonography: the impact of notreporting diminutive lesions. Cancer109:2213–2221
19. Vijan S, Hwang I, Inadomi J et al(2007) The cost-effectiveness of CTcolonography in screening for colorec-tal neoplasia. Am J Gastroenterol102:380–390
20. Liedenbaum MH, de Vries AH,Halligan S et al (2009) CTcolonography polyp matching:differences between experiencedreaders. Eur Radiol19:1723–1730
21. Pickhardt PJ, Nugent PA,Mysliwiec PA, Choi JR,Schindler WR (2004) Location ofadenomas missed by opticalcolonoscopy. Ann Intern Med141:352–359
1656