-
tia ie
ABItetetiaforvidphacicreacifoothethafruleg(iedafisnooiltioundofatinenfulnizthehededucreintheaotameheapopJ
A1599-1611.
POIttetCa
poofinfatpoAmetibafatdiewhteifatfatgetna
RulatreThsisin(SFan35accaninplewibopromaompocreacichnic acid
(ALA), and increasing con-sumption of fish, particularly fatty
total fat, SFA, TFA, monounsatu-rated fatty acids (MUFA), and
n-6and n-3 PUFA for healthy individu-als. The endpoints used to
determine
oncauetaimcuvaassmesivlatinfldopotioR
aneathebrispeeaproemtioEva ucluingagIn(DNugu
FATFaetaFawhch(SFA), one double bond (MUFA), ormore than one
double bond (PUFA),
from the methyl terminus of the fattyacid as n-6 or n-3 fatty
acids. MUFAfound in the diet are largely n-9 fattyacids, with small
amounts of n-7 fatty0002-8223/07/10709-0016$32.00/0d
2risks and benefits are based largely acids. The Figure presents
the struc-oi: 10.1016/j.jada.2007.07.024
007 by the American Dietetic Association Journal of the AMERICAN
DIETETIC ASSOCIATION 1599SITION STATEMENTis the position of the
American Die-ic Association and the Dietitians ofnada that dietary
fat for the adult
fish. This paper evaluates the evi-dence of benefits and adverse
effects(or lack thereof) of dietary fatty acidsto issue dietary
recommendations for
and the configuration of the doublebonds (cis or trans). In
addition,PUFA are further classified based onthe position of the
first double bondfrom thPosition of the
Dieti
STRACTis the position of the American Di-tic Association (ADA)
and Dieti-ns of Canada (DC) that dietary fatthe adult population
should pro-e 20% to 35% of energy and em-asize a reduction in
saturated fattyds and trans-fatty acids and an in-ase in n-3
polyunsaturated fattyds. ADA and DC recommend ad-based approach for
achievingse fatty acid recommendations;t is, a dietary pattern high
inits and vegetables, whole grains,umes, nuts and seeds, lean
protein, lean meats, poultry, and low-fatiry products), fish
(especially fattyh high in n-3 fatty acids), and use
ofnhydrogenated margarines ands. Implicit to these recommenda-ns
for dietary fatty acids is thatsaturated fatty acids are the
pre-minant fat source in the diet. Thesety acid recommendations are
madethe context of a diet consistent withergy needs (ie, to promote
a health-body weight). ADA and DC recog-e that scientific knowledge
abouteffects of dietary fats on human
alth is incomplete and take a pru-nt approach in recommending a
re-ction in those fatty acids that in-ase risk of disease, while
promotingake of those fatty acids that benefitlth. Registered
dietitians play a piv-l role in translating dietary recom-ndations
for fat and fatty acids intolthful dietary patterns for
differentulation groups.m Diet Assoc. 2007;107:e assocAmerican
Dieteticns of Canada: D
pulation should provide 20% to 35%energy and emphasize a
reductionsaturated fatty acids and trans-ty acids, and an increase
in n-3lyunsaturated fatty acids. Theerican Dietetic Association and
Di-tians of Canada recommend a food-sed approach for achieving
thesety acid recommendations; that is, at high in fruits and
vegetables,ole grains, legumes, nuts, lean pro-n (ie, lean meats,
poultry, and low-dairy products), fish (especially
ty fish high in n-3 fatty acids), to-her with the use of
nonhydroge-ted margarines and oils.
ecommendations for the intakeof dietary fat and fatty acidshave
been made for healthy pop-
tions as well as for prevention andatment of chronic disease
(1-12).e guidance issued generally is con-tent in recommending a
decreasethe intake of saturated fatty acidsA) and trans-fatty acids
(TFA),d in recommending 20% or 25% to% of energy from fat. This can
beomplished by a reduction in SFAd TFA, which results in a
decreaseenergy intake, or by partial or com-te replacement of SFA
and TFAth unsaturated fatty acids and car-hydrates or to a lesser
extent withtein within the recommendationsde for macronutrients.
Recent rec-mendations also recognize the im-rtance of n-3 fatty
acids. An in-ase in n-3 polyunsaturated fattyds (PUFA) can be
attained byoosing fats and oils high in -linole-iationADA
REPORTSAssociation andtary Fatty Acidslipid and lipoprotein
responses be-se they respond to changes in di-ry fatty acids and
because they areportant risk factors for cardiovas-lar disease
(CVD). Moreover, ele-ted biomarkers of inflammation areociated with
CVD and numeroustabolic disorders that are respon-e to dietary fat
(13). Research re-ing the role of dietary fatty acids toammatory
and immune disorderses not suggest that among healthypulations,
different recommenda-ns are needed for fat and fatty
acid.ecommendations for dietary fat
d fatty acids for treatment of dis-se or clinical practice are
outsidescope of this paper. However, a
ef discussion of the relationship ofcific fatty acids to
different dis-ses/conditions is provided when ap-priate. For those
with hyperlipid-ia, the American Dietetic Associa-ns (ADAs) updated
Hyperlipidemiaidence Analysis Library (14) providesseful Guide for
Practice, which in-des recommendations for modify-dietary fatty
acid intakes for man-
ing hyperlipidemia/dyslipidemia.addition, Dietitians of
Canadas
Cs) Practice-based Evidence intrition service provides
practiceidance (15).
S IN THE FOOD SUPPLYtty acids are the major form of di-ry fat
(mainly as triglycerides).tty acids are classified based onether or
not the fatty acid carbonain contains no double bonds
-
turlogsouthethenuS
amvegucSFandosteoiloil
F
SL l a
ic fMPS cho
Mc
enreary
tr
Pn
n
Figlipo
ADA REPORTS
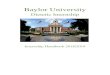
160e of different fatty acids, their bio-ical actions, and
common foodrces. Humans are unable to syn-size n-6 or n-3 fatty
acids, thusse fatty acids are essential dietarytrients.FA are
present in relatively highounts in animal fats and tropicaletable
oils. Meat and dairy prod-ts contribute approximately 60% ofA in
the diet in the United Statesd Canada. Animal fats contain
pre-minantly palmitic acid (16:0) andaric acid (18:0). Tropical
vegetables, such as palm kernel and coconut
atty acid classification Structure
aturated fatty acidsauric acid C12:0yristic acid C14:0almitic
acid C16:0tearic acid C18:0
onounsaturated fatty acidsis-configurationPalmitoleic acid
C16:1Oleic acid C18:1
ans-configurationElaidic acid C18:1
Vaccenic acid C18:1
olyunsaturated fatty acids-6 fatty acidsLinoleic acid C18:2
Arachidonic acid C20:4
Conjugated linoleic acid C18:2 (vari
-3 fatty acids-linolenic acid C18:3
Eicosapentaenoic acid C20:5Docosapenteonoic acid
C22:5Docosahexaenoic acid C22:6
ure. Fatty acids in the food supplystrucprotein.s, contain high
amounts of lauric res
0 September 2007 Volume 107 Number 9d myristic acid. SFA are
formed byustrial hydrogenation (addition ofdrogen atoms to
unsaturated bondsating saturated bonds) of vegeta-oils. Fully
hydrogenated fats areh in stearic acid.artial hydrogenation results
information of a large number of
sitional and geometric isomers ofnaturally occurring cis-fatty
ac-
. A major TFA in industrially hy-genated oils is elaidic acid
(t9-18:although many other trans-
mers are formed. TFA are presentruminant meat and milk fats as
a
Biological actions
Raises total, LDLa, and HDLb cholesteroincreases some
hemostatic/thrombotthat promote thrombosis
Does not increase total, LDL, and HDL
Decreases total and LDL cholesterol whsubstituted for saturated
fat and dectotal cholesterol compared with dietacarbohydrate
Raises total and LDL cholesterol similasaturated fat, decreases
HDL vs satuand raises the total-to-HDL ratio mosaturated fat;
induces systemic inflaand endothelial dysfunction
Not established
Decreases total and LDL cholesterol
Precursor for eicosanoids (prostaglandithromboxanes,
leukotrienes)
) Anti-cancer properties, decreases bodygrowing animals
Decreases cardiovascular risk throughmechanisms including
platelet functiinflammation endothelial cell functioncompliance,
arrhythmia
Decreases risk of sudden death througmechanisms including
platelet functiendothelial cell function, arterial comand
arrhythmia and has beneficial enervous system development and
he
, function, and common food sources. LDLult of biohydrogenation
of unsat- fatated fatty acids in the rumen. Thejor TFA in ruminant
meat andlk is vaccenic acid (t11-18:1), withaller amounts of other
TFA.UFA are present in vegetable,
t, and seed oils, as well as in meatsd dairy products. The major
dietaryFA is oleic acid (18:1n-9). Oleicd is present in high
amounts inve oil, canola oil, mid-oleic sun-wer oil, and other mid-
and high-ic vegetable oils, peanuts, pista-ios, almonds, and
avocados. PUFAfound in vegetable, nut, and seed
s with the amounts of n-6 and n-3
Common food sources
ndactors
Coconut oilButter fat, coconut oilMost fats and oils
lesterol Most fats and oils, cocoabutter, fully
hydrogenatedvegetable oils
sesSome fish oils, beef fatMost fats and oils, nuts,
seeds, avocados
ed fat,o thanation
Partially hydrogenatedvegetable oils
Butterfat, meat
Liquid vegetable oils, nuts,seeds
Meat, poultry, fish, eggs
in Butterfat, meat
tiple
rterial
Flaxseed, canola oil,soybean oil, walnuts
ultiple
ncets on
Fish oil, algaeFish oil, algaeFish oil, algae
ow-density lipoprotein; HDLhigh-densityanindhycreblehigP
thepotheidsdro1),isoin
urmamismM
nuanMUaciolifloolechareoil
r toratre smm
ns,
ants fat
mulon,, a
h mon,pliaffecalth
ture lty acids varying greatly. The major
-
dielin(18thehigflo3nn-3seewapreamandit(adALcucelacieican6npaereasetachjorpoC
PUcuammiCLt11onLAclafooinglabanamanexelabingingtioT
diebleThtrienalenofKeintvidfating
FATThporthawhantriAm1TFTh(AHdabe1trivenmethaDiaSFprobenulimonareenintinhigtertakT
Gumediseta0.6PUmemavidmaeqfataleinfatyeayeag/dtha(12ab0.5potha10whtio
LAdieT
thainttheconetaofristiotheCotio(21tifiomweabpeMetrianmgwodupuThcenmawhwearseracorbragtwciatio
ADAciADgrointtotiointiocabbuprotoopagendreintom
ADA REPORTStary PUFA are the 18-carbon n-6oleic acid (LA) and
the n-3 ALA. LA:2n-6) is the parent fatty acid ofn-6 fatty acids
and is present inh amounts in soybean, corn, saf-wer, and sunflower
oils. ALA (18:-3) is the parent fatty acid of thefatty acids and is
highest in flax-d, canola and soybean oils, andlnuts. -Linoleic
acid (18:3n-6) issent in foods in very smallounts, except for
evening primrosed borage oils. The desaturation (ad-ion of double
bonds) and elongationdition of carbon atoms) of LA andA to longer
carbon chain PUFA oc-rs in phytoplankton and animalls. LA is
elongated to arachidonicd (ARA), and ALA is converted
toosapentaenoic acid (EPA; 20:5n-3)d docosahexaenoic acid (DHA;
22:-3) animal cells. Fish and seafood,rticularly fatty fish such as
mack-l, herring, salmon, tuna, and trout,well as oysters, are the
richest di-ry sources of the n-3 longer carbonain PUFA, EPA, and
DHA. The ma-dietary sources of ARA are meat,
ultry, and eggs.onjugated linoleic acids (CLA) areFA in which
the double bonds oc-r on adjacent carbons. Smallounts of CLA are
present in thelk and meat of ruminants. A majorA is cis-9, trans-11
18:2, termed c9,18:2, which has one trans- and
e cis-bond, compared to the all cis-, which is c9,c12 18:2. CLA
are notssified as TFA for the purpose ofd labeling, or in
regulations relat-to TFA in Canada. The trans-fateling rules in the
United Statesd Canada do not differentiateong TFA from ruminant
animalsd industrial hydrogenation, but dompt conjugated dienes
(CLA) fromeling. Thus, all trans fats, includ-ruminant trans fats,
but exclud-CLAs, are included on the Nutri-
n Facts label, regardless of origin.he fatty acid composition of
commontary fats and oils are presented in Ta-1 (available at
www.adajournal.org).e USDepartment of Agricultures Nu-nt Data
Laboratory (16) and the Ca-dian Nutrient File (17) provide excel-t
resources on the nutrient contentfoods, including fatty acids.
Theep It Managed database (18) is aneractive software program that
pro-es information about the n-3 and n-6ty acid content of 9,000
food serv-
s. theTY ACID RECOMMENDATIONSe Dietary Reference Intake (DRI)
re-t on macronutrients recommendedt SFA and TFA be as low as
possibleile consuming a diet that providesadequate intake of all
essential nu-ents (12). The Dietary Guidelines forericans 2005 (9)
recommended0% of calories from SFA, and thatA consumption be as low
as possible.e American Heart AssociationsA) Diet and Lifestyle
Recommen-
tions recommended that SFA intake7% of calories, and that TFA
be% of calories (5). Likewise, the Nu-tion Recommendations and
Inter-tions for Diabetes 2007 (1) recom-nd that SFA be 7% of
calories andt TFA be minimized. The Canadianbetes Association
recommended thatA be10% of calories and that use ofcessed foods
containing SFAandTFAlimited
(http://www.diabetes.ca/Files/tritional_guide_eng.pdf). The upperit
of 35% calories from fat was baseddata to show that higher fat
intakesassociated with a greater intake of
ergy and SFA. The lower limit for fatake was set tominimize the
increaseplasma triglyceride and decrease inh-density lipoprotein
(HDL) choles-ol levels that occurs with high in-es of
carbohydrates.he DRI report and the Dietaryidelines for Americans
2005 recom-nd an acceptable macronutrienttribution range of 5% to
10% di-ry energy from n-6 PUFA, and% to 1.2% of energy from n-3FA,
but did not set a Recom-nded Dietary Allowance or Esti-ted Average
Requirement for indi-ual fatty acids. The DRI report oncronutrients
(12) provided an Ad-uate Intake (AI) for n-6 and n-3ty acids, which
is an intake equiv-nt to the observed median intakethe United
States. The AI for n-6ty acids is 17 g/day for men 19 to 50rs, 12
g/day for women 19 to 50rs. The AI for ALA is 1.6 and 1.1ay for men
and women 19 to oldern 70 years of age, respectively). These
intakes are equivalent toout 5% to 6% energy from LA and% energy
from ALA. The DRI re-rt on macronutrients also notedt EPA and DHA
can provide up to% of total dietary n-3 fatty acids,ich is based on
median consump-n patterns for these fatty acids in
United States. Mean intakes of yea
September 2007 Journal ofand ALA are about 5% and 0.5% oftary
energy in Canada (19).his position paper emphasizest the AI are the
observed medianakes of n-6 and n-3 fatty acids forUS population,
and should not befused with the Recommended Di-ry Allowance or with
those intakesfatty acids that confer the lowestk of disease. For
primary preven-n of coronary heart disease (CHD),US Dietary
Guidelines Advisory
mmittee (20), AHA (5,6), the Na-nal Heart Foundation of
Australia), and the United Kingdom Scien-c Advisory Committee (10)
all rec-mend two servings of fish perek, preferably fatty fish,
providingout 450 to 500 mg EPA and DHAr day. The National Health
anddical Research Council (2006) Nu-ent Reference Values for
Australiad New Zealand recommend 610/day for men and 430 mg/day
formen for chronic disease risk re-ction
(http://www.nhmrc.gov.au/blications/synopses/_files/n35.pdf).e
National Academies (22) re-tly recommended that adolescentles,
adult males, and femaleso will not become pregnant, asll as adult
males and females whoe at risk of CVD consume two 3-ozvings of fish
per week. The reportknowledged that females who aremay become
pregnant or who areeastfeeding, and children up toe 12 may benefit
from consumingo 3-oz servings of seafood, espe-lly those with
higher concentra-ns of EPA and DHA.
A and DC Position on Fat and FattydsA and DC concur with other
expertups in recommending a dietary fatake for adults in the range
of 20%35% energy, emphasizing a reduc-n of SFA and TFA, and an
increasen-3 PUFA. These recommenda-ns for specific fatty acids are
appli-le to children over 2 years of age,t should be followed with
age-ap-priate total fat and energy intakessupport normal growth and
devel-ment. For children 1 to 3 years ofe, a total fat intake of
30% to 40% ofergy is recommended, and for chil-n 4 to 18 years of
age, a total fatake of 25% to 35% of energy is rec-mended. For
children under 2
rs of age, cows milk, if fed, should
the AMERICAN DIETETIC ASSOCIATION 1601
-
betiobahigtotD
egythecanfatteiateingsurefihiganraiResucartuteriHooveoftimrean-6toevionintme4%(32OrWotoNunaFatomeR
intaromalisofdisproeicceptoThfavdisverCoredhaint
chbeityglySosanthemaalslev(28A
ceprantri1.2ALisshbleundraofextwiF
conananwemaproDHanDHbeforpleabfecnoT
inmegutallowistPrFovirthetioviswhyouswbeelscushpo
canmapetiosmThAganronmekgwhyoutiothamawisutypforM
admebyanmaEPconronpo(45giotiosocconponaB
preinfclilesbresuenfroamme(46wosu0.2ofDH
FATWhrislipplalow
ADA REPORTS
160full-fat milk. The recommenda-ns for total fat for children
aresed on a gradual transition fromh-fat intakes during infancy to
theal fat recommendation for adults.ecreasing SFA and TFA is a
strat-for reducing the energy content ofdiet. Alternatively, SFA
and TFAbe replaced with unsaturated
ty acids, and/or carbohydrate, pro-n. Replacing SFA with
unsatur-d fat avoids the triglyceride-rais-effect when
carbohydrates are
bstituted for SFA. Complex and un-ned carbohydrates result in
aher fiber intake and can attenuate,d even prevent, the
triglyceride-sing effect of low-fat diets (23-25).placing SFA with
protein also re-lts in lower triglycerides than whenbohydrates are
used as the substi-e (26). MUFA avoid the HDL-low-ng effects of
diets high in n-6 LA.wever, uncertainty surrounds therall
risk-to-benefit of high intakesMUFA vs LA; consensus on the op-al
intake of LA has not beenched. The recommended range forPUFA in the
United States is 5%10% of energy (7-9,12) based ondence of
beneficial effects of PUFACVD and diabetes (27-31). Otherernational
groups have recom-nded lower intakes of n-6 PUFA ofto 8% [European
Commission
)], 5% to 8% (Food and Agricultureganization of the United
Nations/rld Health Organization [11]), 3%4% [The Japan Society for
Lipidtrition (33)], and 2% to 3% [Inter-tional Society for the
Study oftty Acids and Lipids (34)] of energymeet essential fatty
acid require-nts.ecommendations for lowering theake of n-6 PUFA
have centeredund concerns that high intakesy antagonize n-3 PUFA
metabo-m, contribute to an increased riskinflammatory, immune, and
otherorders associated with an excessduction of n-6 fatty
acidderivedosanoids, and may increase sus-tibility of tissue and
plasma lipidsoxidative modification (35,36).
us, ALA, EPA, and DHA, whichorably affect risk of CVD and
othereases (37), could be affected ad-sely by high n-6 fatty acid
intakes.nsensus on the beneficial effect ofucing LA intakes on
human healths not been reached (38). Higher LA
akes can play an important role in (w
2 September 2007 Volume 107 Number 9olesterol-lowering (39), may
haveneficial effects on insulin sensitiv-(40), and may reduce
plasma tri-cerides in some individuals (41).me n-6 fatty
acidderived eico-oids also have important effects inresolution of
inflammation and
rkers of CVD and CVD events areo lowest in individuals with
highels of both n-6 and n-3 fatty acids,42).DA and DC concur with
the ac-table macronutrient distributionge of the DRI report on
macronu-ents (12) for ALA, which is 0.6% to% of energy. The median
intake ofA in the United States and Canada0.5% energy. The intake
of TFAould be reduced to as low as possi-. SFA should be replaced
with cis-saturated fat or complex carbohy-tes to maintain a total
fat intake20% to 35% of energy. To a limitedent, SFA calories can
be replacedth protein.ish and Shellfish. ADA and DCsider that n-3
PUFA from fish areimportant part of a healthful diet,d recommend
two servings perek, preferably fatty fish. Approxi-tely 8 oz of
cooked fish per weekvides about 500 mg/day EPA andA. For vegans who
do not consumey preformed sources of EPA andA, additional research
is needed
fore recommendations can be madethese fatty acids, including
sup-ments. It is important to note thesence of reported adverse
health ef-ts in this population that consumesfish.he presence of
some contaminantsfish, including dioxins and methylrcury, has
raised concern. Federalidelines for avoiding
environmen-contaminants in fish should be fol-ed (the US Food and
Drug Admin-ration and the Environmentalotection Agency (43);
Canadianod Inspection Agency (44)]. The En-onmental Protection
Agency andUS Food and Drug Administra-
n have issued a joint consumer ad-ory for pregnant women, womeno
could become pregnant andng children not to eat shark,ordfish, king
mackerel, or tilefishcause of their higher mercury lev-. Up to 12
oz per week of low-mer-ry fish are recommended, such asrimp, canned
light tuna, salmon,llock, and catfish. As albacore
hite) tuna has more mercury than terned light tuna, these risk
groupsy eat up to 6 oz of albacore tunar week. These same
recommenda-ns apply to young children, butaller portions should be
served.e Canadian Food Inspectionency, different from the US Foodd
Drug Administration and Envi-mental Protection Agency, recom-nds a
maximum intake of 0.20 g//day for pregnant women, womeno could
become pregnant, andng children. A report from the Na-nal Academies
(22), which statest pregnant women or women whoy become pregnant
should staythin Federal advisories for con-mption of specific fish
and seafoodes, and state/regional advisorieslocally caught fish.any
of the fish noted in federal
visories as containing high levels ofrcury are not commonly
consumedCanadian women and children,
d other fish not noted in the reportsy contain methyl mercury.
TheA and DHA content of commonlysumed fish and amounts of
envi-mental contaminants has been re-rted by Mozaffarian and Rimm).
Adherence with federal (and re-nal) advisories on fish consump-n
will help achieve the benefits as-iated with fish and
seafoodsumption without increasing ex-sure to environmental
contami-nts.reast Milk. Human milk is theferred source of nutrition
for allants under 6 months of age, unlessnically contraindicated.
Infantss than 1 year of age who are notastfed should be fed human
milkbstitutes that contain at least 4%ergy from LA and 0.75%
energym ALA, which are the minimumounts of LA and ALA recom-nded in
formulas for term infants), and both DHA and ARA. Formen who wish
to use a humanmilkbstitute, DHA should be at least% of total fatty
acids and the levelARA should not be lower thanA.
TY ACIDS AND HEALTHile many factors contribute to thek of CHD,
the important lipid andoprotein risk factors includesma (or serum)
total cholesterol,-density lipoprotein (LDL) choles-
ol, HDL cholesterol, triglycerides,
-
anterliplipmasesingmoestovecengiemeon
SFAEppotak(27shchcrelesmg53cre0.0difacihaingwhefftermythecauterSFindme
MUOlles(7,hyideinvlesstutes22suterchtha(49T
an
InaciofanlevbrecanaciginC
MUrecn-6rectheomtiograEvBloTrthariehigpaingesdie(64hu
TFAHiciarisdefatdehaofofterdecreLDTFtersmenflawhTF(74E
poallanCliMUmethu
ruthaisC
fatincangenertthapaC-g/dstrCLsitmedadustuThabdieefihigmerecpaF
rivduplewisombySFadgieSF
PUTh(AimEaLAtorityincpoCVanordtheroltheinchan-6uteWe
ADA REPORTSd the ratio of total to HDL choles-ol. Despite the
significance of lipid/oprotein risk factors, many non-id factors,
including inflammatoryrkers, are also important for as-sing CHD
risk (47). Thus, target-multiple risk factors holds the
st promise for attaining the great-reduction in disease risk.
More-r, because inflammation plays atral role in many diseases,
strate-s to reduce elevated inflammatorydiators may have beneficial
effectsmany other diseases.
idemiologic studies have shown asitive association between the
in-e of SFA and the incidence of CHD,48,49), and clinical studies
haveown that SFA raise total and LDLolesterol (40,50). For every 1%
in-ase in energy from SFA, LDL cho-terol levels increase by 1.3 to
1.7/dL (0.034 to 0.044 mmol/L) (51-), and HDL cholesterol levels
in-ase by 0.4 to 0.5 mg/dL (0.010 to13 mmol/L) (54). Individual
SFAfer in their effects (55,56). Lauricd (12:0) and myristic acid
(14:0)ve a greater total cholesterol rais-effect than palmitic acid
(16:0),
ile stearic acid (18:0) has a neutralect on total, LDL, or HDL
choles-ol (53,54,57). Lauric acid, but notristic or palmitic acid,
decreasestotal-to-HDL cholesterol ratio be-se of an increase in HDL
choles-ol (54). Foods contain mixtures ofA, thus, selecting foods
based onividual SFA content is not recom-nded.
FAeic acid lowers total and LDL cho-terol when it replaces
SFA8,12,58). When compared to carbo-drate, MUFA decrease
triglycer-s, increase HDL cholesterol, and isersely related to
total-to-HDL cho-terol ratio. A meta-analysis ofdies with
individuals with diabe-showed that high-fat diets with
% to 33% energy from MUFA re-lted in lower plasma total
choles-ol, verylow-density-lipoproteinolesterol, and triglyceride
levelsn did low-fat, high-carbohydrate% to 60% energy) diets
(59).he association between MUFA
d risk of cancer is inconsistent (60). mesome studies, food
sources of oleicd were associated with a lower riskbreast cancer
(61,62), but meta-alysis found that tissue oleic acidels were
positively associated withast cancer (63). Because oleic acidbe
synthesized in vivo, tissue oleicd is not necessarily of dietary
ori-.urrent recommendations forFA were derived by
consideringommendations for SFA, TFA, andand n-3 PUFA, then
deriving a
ommendation for MUFA based onamount needed to obtain the
rec-mended intake of total fat. Na-nal Cholesterol Education Pro-m
Expert Panel on Detection,aluation, and Treatment of Highod
Cholesterol in Adults (Adulteatment Panel III) recommendst MUFA not
exceed 20% of calo-s. There is an increasing trend forher MUFA in
many foods, due inrt to use of fats with higher MUFAplace of TFA.
Some evidence sug-ts an adverse effect of high MUFAts on
atherosclerosis in animals), but this has not been observed
inmans.
gh intakes of TFA have been asso-ted with an increase in the
relativek of coronary artery disease, CHDath rate, and risk of
fatal and non-al myocardial infarction, and sud-n death (27,65-70).
Clinical trialsve shown a dose-dependent effectTFA over the range
of 0.5% to 10%energy in increasing LDL choles-ol levels (12).
Relative to SFA, TFAcrease HDL cholesterol and in-ase the TC-to-HDL
cholesterol andL-to-HDL cholesterol ratios (54).A also increases
other coronary ar-y disease risk factors, such asall dense LDL,
postprandial lipids,dothelial function, and systemic in-mmatory
mediators (71-73), all ofich may contribute to the effect ofA on
CHD mortality and morbidity,75).vidence of no relationship and
a
sitive association between industri-y produced TFA and cancer
(76-79)d diabetes (80) has been reported.nical studies with the
major transFA (vaccenic acid) in ruminantats and milks have not
been done;s, evidence to support a recom-
ndation for the intake of fat from EP
September 2007 Journal ofminant meats and dairy productst
differs from those based on SFAinsufficient.LA, in ruminant meat
and dairys, have unique biological effects,luding decreased fat
deposition,d anticarcinogenic, antiathero-ic, and immune-modulating
prop-ies (81). There is some evidencet CLA supplements (3 g/day)
im-ir insulin sensitivity (82), increasereactive protein [t10,c12
CLA, 3.4ay (83)], and increase oxidativeess and insulin resistance
[c9,t11A, 3 g/day (84)] in those with obe-y and metabolic syndrome.
Supple-ntation with about 2 g CLA pery may reduce milk fat
secretionring lactation (85), although otherdies have not confirmed
this (86).ese doses are above those attain-le from usual foods;
thus, whethertary CLA provides any health ben-t is not clear.
Consumption ofher-fat dairy and red meats as aans to increase CLA
intake is notommended because of the accom-nying increase in
SFA.oods containing industrially de-ed TFA should be minimized.
Re-cing TFA in some foods, for exam-, pastry that requires solid
fat,thout increasing SFA is complex. Ine foods, TFA have been
removedreplacement with fats higher inA. The current
recommendationsvise that TFA replacement strate-s not result in a
higher TFA andA (87).
FAe n-6 (LA and ARA) and the n-3LA, EPA, and DHA) fatty acids
areportant in many aspects of health.rly studies focused on diets
rich inin reducing plasma lipid risk fac-s and CVD morbidity and
mortal-(31). More recently, there has beenreased understanding of
the im-rtance of n-3 fatty acids in reducingD risk, in neurological
function,d in inflammatory and immune dis-ers. ALA, EPA, and DHA
differ inir metabolic and physiologicales, and the relative
importance ofdifferent n-3 fatty acids remains
ompletely understood. Concerns been raised that a high
dietary:n-3 fatty acid ratio may contrib-to many diseases
associated withstern diets. Because the intake of
A and DHA are much lower than
the AMERICAN DIETETIC ASSOCIATION 1603
-
foranicatheScreaofwhcreetaplaintcenvermibyinacicauachofforingALdasolacin
alsenplaan43fecPrchmafrobysimlesmuchboantotchcreto-alsmeanastiotypStutiogluCotheganuint
inshigbeT
n-6canrebanimhaanancluintofcerFothePUstocreinincfar(33relCHdifH
beoftor(10LDoxifroMUtosucreanerninenoftherentoconacctioiscrewitofavincrediebeernis
cretiothaareinfln
inaverconcia(10theintasseveanThStucrewiinffatNuthaALristhothecarsuwienlesoftie(11conofin(11M
thaprotioiesassprolenALofdeevebinpro(952.1pointInHeterfro
ADA REPORTS
160LA and ALA, increases in EPAd DHA intake that have
physiolog-l effects do not substantively alterdietary n-6:n-3 fatty
acid ratio.
ientific consensus has not beenched on whether current intakesLA
are too high, and it is unclearether associations between an
in-ased risk of disease and high di-ry n-6:n-3 fatty acid ratios
are ex-ined by high n-6, low n-3 fatty acidakes, or effects of
their ratio. Re-t studies have suggested that con-sion of ALA into
EPA is not deter-ned by the ratio of LA to ALA, butthe absolute
amounts of ALA or LAthe diet (88). Use of n-6/n-3 fattyd ratios is
also problematic be-se an identical ratio can beieved with very
different amountseach fatty acid class (89). There-e, because of
the difficulty in apply-one ratio across diets varying inA, EPA,
and DHA, the recommen-tions in this paper focus on the ab-ute
intakes of n-6 and n-3 fattyds.-6 Fatty Acids. Early clinical
tri-found that 13% to 21% dietary
ergy from PUFA decreased totalsma cholesterol by 13% to 15%,d
decreased CHD events by 25% to%, although there was a lack of ef-t
on all-cause mortality (90-92).edictive equations based onanges in
blood cholesterol esti-ted that an increase of 1% energym PUFA
reduces total cholesterol0.9 mg/dL (0.023 mmol/L), while ailar
intake of SFA raises total cho-terol by approximately twice asch
(51,52). PUFA increase HDLolesterol when substituted for
car-hydrate, although less than SFAd MUFA (54). Because PUFA
loweral cholesterol and increase HDLolesterol, the net effect is a
de-ase in the total-to-HDL and LDL-HDL cholesterol ratios. PUFA
mayo have beneficial effects on glucosetabolism and insulin
resistanced, hence, on type 2 diabetes (80,93),suggested by the
inverse associa-n of vegetable fat and PUFA withe 2 diabetes in the
Nurses Healthdy (80) and the inverse associa-n between PUFA and
fasting bloodcose levels in the Italian Ninemmunities Study (94).
However,Canadian Diabetes Association
ve a D-level evidence rating to thetrition recommendation for
PUFA
ake of 10% of energy because of tai
4 September 2007 Volume 107 Number 9ufficient clinical evidence
thath LA has beneficial effects in dia-tes (95).he possibility that
high intakes ofPUFA may increase the risk ofcer, gallstones,
CHDmortality, ce-ral infarction, hyperinsulinemia,d subsequent
insulin resistance, ormune and inflammatory disorderss been raised
(33,35,96-99). Meta-alysis of 16 case-control studiesd seven major
cohort studies con-ded that it is unlikely that a highake of LA
substantially raises riskbreast, prostate, or colorectal can-(96).
The Health Professionals
llow-Up Study showed that men inhighest vs lowest quintile
of
FA intake had a lower risk of gall-ne formation (100). In
contrast, in-ased LA intake from 1950 to 2000Japan has been
associated with anreased morbidity from cerebral in-ction and
ischemic heart disease,97,98). Similarly, there is a
linearationship between n-6 PUFA andD mortality among populations
inferent countries (101).igh intakes of n-6 PUFA have
en proposed to increase productionproinflammatory and
proaggrega-y eicosanoids derived from ARA2), and increase
susceptibility ofL and tissue lipids high in LA todative
modification (103). LDLm subjects consuming LA-rich vsFA-rich diets
is more susceptibleoxidative modification (35). Con-mption of oils
high in LA has in-ased in the United States, Canada,d other
countries following West-ized diets (104), with an increaseLA
intakes from about 3% dietaryergy in the 1930s to current
intakesabout 5% to 6% dietary energy inUnited States and Canada.
Cur-t evidence does not support a needincrease LA intakes in
individualssuming LA at the lower end of theeptable macronutrient
distribu-n range. However, whether benefitattained by recommending
a de-ase in LA intakes for individualsth intakes above the median
of 5%6% energy is unclear. One positionors a decrease in the intake
of LAfavor of MUFA and ALA. A de-ase in LA would also reduce
thetary ratio of LA to ALA, which hasen suggested to be too high in
West-diets (105). An alternate position
that current intake of LA be main-
ned, and that n-3 fatty acids in- ofased. In support of the
latter posi-n, recent studies have suggestedt n-6 and n-3 fatty
acids togetherassociated with the lowest level ofammation
(28,42).-3 Fatty Acids. ALA, the predom-nt dietary n-3 fatty acid,
is con-ted to EPA and DHA, although theversion of ALA to EPA and
espe-lly to DHA is very low in humans6-110). Epidemiologic studies
inUnited States reported that ALA
akes of 0.53 to 2.8 g per day wereociated with a reduced risk of
CVDnts, fatal ischemic heart disease,d all-cause mortality
(111-113).e Health Professionals Follow-Updy reported that a 1%
energy in-ase in ALA intake was associatedth a 40% lower risk of
myocardialarction, after adjustment for totalintake (69), while
results from therses Health Study (114) foundt women in the lowest
quintile ofA intake had a 38% to 40% lowerk of sudden cardiac death
thanse in the highest two quintiles. InLyon Diet Heart Study,
postmyo-dial infarction patients who con-med a Mediterranean-style
dietth 0.81% energy from ALA, 8.3%ergy from SFA and 217 mg/day
cho-terol had a 50% to 70% lower riskrecurrent heart disease than
pa-nts consuming an AHA step 1 diet5). Recent epidemiologic
studiestinue to support a beneficial effectdietary ALA on CVD,
particularlythe presence of a low fish intake6).eta-analysis have
raised concernt ALA may increase the risk ofstate cancer (117).
Nine observa-nal studies (four prospective stud-and five
nonprospective studies)essed the relationship betweenstate cancer
incidence or preva-ce, and intake or blood levels ofA, and reported
an increased riskprostate cancer (1.70; 95% confi-nce interval:
1.12 to 2.58). How-r, in prospective studies, the com-ed estimate
of relative risk forstate cancer incidence was 1.32% confidence
interval: 0.80 to8). A subsequent study also re-rted no association
between ALAake and prostate cancer risk (118).addition, subjects in
the Lyon Dietart Study who consumed a Medi-ranean diet with 0.8% of
energym ALA did not have increased risk
prostate cancer (119). Most evi-
-
deALE
decrefibofstudethipaofepStaofdeiscmgofDHfatmemoassitystrfisAerapreratpotalpoE
posocanconanrecexprecevefro11suananD
sysanshfatblosevtempotioorcog(13Fr
inph47allthenitlesweinZuuaabnoW
raptiorecfathefer
PRThvelattfattiocondielacPUthrtanALbydeTFhahefrobioacinothaUnothbrasombreposuverA
DHwiTFsumehigbean
intofsinfooT
pe10ALARabinffraapme(15shdonaothcreinfbrepolevscosu(15Sturepqudremo34naerstioT
poDHunCethevelDHterwo(16twanextingwhwefislonmospiwetiocomfanoth
ADA REPORTSnce suggests no adverse effect ofA and risk of
prostate cancer.PA and DHA reduce risk of sud-
n cardiac death, possibly by in-asing the threshold for
ventricularrillation, which is a leading causesudden death
(120,121). Recentdies in patients with implantedfibrillators,
however, caution thats effect may not be present in thistient
population (122). The intakeEPA and DHA from fish in
fiveidemiologic studies in the Unitedtes associated with the lowest
riskcoronary events, including CHDath, primary cardiac arrest,
andhemic heart disease death was 496per day (123-127). A daily
intakeapproximately 500 mg EPA andA is equivalent to about 8 oz
ofty fish per week. Other recentta-analyses reported that five orre
servings of fish per week wasociated with a lower CHD mortal-(128)
and a lower incidence of
oke (129) when compared with noh or fish less than once per
month.recent systematic review of the lit-ture of primary and
secondaryvention studies with 1 year du-ion with fish or fish oils
also re-rted reduced rates of all-cause mor-ity, cardiac and sudden
death, andssibly stroke (130).pidemiologic studies have re-
rted that high fish intakes are as-iated with a reduced risk of
breastd colorectal cancer (131), which issistent with evidence that
EPAd DHAmay reduce markers of colo-tal cancer (60,131,132) and
reduceression of genes involved in colo-tal cancer cell growth
(133). How-r, a recent review of 20 cohortsm seven countries that
evaluateddifferent types of cancer found nobstantial association
between plantd marine-derived n-3 fatty acidsd incidence of cancer
(134).HA is important in the nervoustem, including the retina.
Clinicald epidemiologic studies haveown that low dietary intakes of
n-3ty acids and low plasma or redod cell DHA are associated
witheral neurological and visual sys-problems (135-137). Three
recent
pulation studies found an associa-n between higher intakes of
DHAEPA and DHA and lower risk ofnitive decline or verbal
fluency8-140). Men and women in the
amingham Heart Study who were higthe top quartile of plasma
phos-atidylcholine DHA levels had a% reduction in risk of
developing-cause dementia (138). Likewise, inAtherosclerosis Risk
in Commu-
y Study (140), higher plasma cho-teryl ester levels of EPA and
DHAre associated with a lower declineverbal fluency. Similarly, in
thetphen Elderly Study (139), individ-ls who consumed fish had
consider-ly less 5-year cognitive decline thannconsumers.hile
research in these areas isidly increasing, sufficient informa-n is
as yet unavailable to suggestommendations for dietary n-3ty acids
with respect to mentalalth or visual problems that are dif-ent from
those based on CVD.
EGNANCY, LACTATION, AND INFANCYe importance of DHA in neural
de-opment and function has focusedention on the importance of n-3ty
acids during pregnancy, lacta-n, and infancy. Observational
andtrolled clinical studies show thattary PUFA during pregnancy
andtation influences the transfer ofFA across the placenta andough
breast milk (141,142). Impor-t questions are whether dietaryA can
provide sufficient amountsconversion through the
elongation-saturation pathway, and whetherA from hydrogenated n-6
mayve adverse effects on the mother orr infant. An intake of 2%
energym the n-6 LA prevents clinical andchemical signs of essential
fattyd deficiency in infants (143), andevidence is available to
suggestt LA intakes are inadequate in theited States or Canada. On
theer hand, the lower blood lipid andin levels of DHA in infants
fede formulas lacking DHA than inast-fed infants (144,145) raises
thessibility that inadequate dietarypplies of n-3 fatty acids can
ad-sely influence infant development.n inverse association of TFA
withA in newborn infant blood andth growth has been reported, andA
may be deposited in infant tis-es or converted to other
unusualtabolites (146-148). TFA levels ash as 18% of milk fatty
acids haveen reported in the United Statesd Canada (149-151), which
is
her than in Europe, where dietary tio
September 2007 Journal ofakes of TFA are lower (148). LevelsTFA
in human milk have decreasedce the introduction of trans-fatd
labeling (148,152).he conversion of ALA to DHA ap-
ars to be very low in humans (107-9). Newborn infants can
convertA to EPA and DHA, and LA toA, and there is no evidence of
met-olic immaturity in this pathway inancy (106,153,154). Although
thectional conversion of ALA to DHApears to be higher in women
thann, and increases during pregnancy5), intervention studies
haveown that increased intakes of ALAnot increase levels of DHA in
preg-nt women or infants (156). On theer hand, higher maternal DHA
in-ases the transfer of DHA to theant both before birth and viaast
milk after birth (142,157). Asitive association between bloodels of
DHA in infants and higherres on measures of neural and vi-al
maturation has been reported8-162). The Avon Longitudinaldy of
Parents and Children (163)orted that the verbal intelligenceotients
were higher among chil-n 6 months to 8 years of age ofthers who
consumed more than9 g seafood per week during preg-ncy than among
children of moth-who reported no seafood consump-n.he long-term
benefits of early ex-
sure to n-3 fatty acids (EPA andA) on later child development
arecertain (76,164-166). The Harvardnter for Risk Analysis
extrapolatedresults of studies on cognitive de-opment of infants
fed formula withA to suggest that increasing ma-nal DHA intake by
100 mg/dayuld increase child IQ by 0.13 points7). However, a linear
relation be-een DHA intake and IQ is unlikely,d nutrient
requirements cannot berapolated from formula to lactat-women.
Studies in Denmark in
ich women with low fish intakesre supplemented with 4.5 g/dayh
oil (equivalent to 1.3 g/day n 3ger carbon chain PUFA) for 4nths
after delivery found that de-te higher blood lipid DHA, therere no
advantages to visual matura-n, but passive vocabulary and
wordprehension were lower in the in-ts at 1 year of age (168,169).
Iner studies, maternal supplementa-
n with 200 mg/day DHA for the
the AMERICAN DIETETIC ASSOCIATION 1605
-
fireffbuopfanilawoeffnetivwameARbowapreing(17fisna
mebetiginfARtiaersstubeingsiotioinfanthesispreDHfanwirantiocludesivART
soumoabARrecfouARnokeARhupoefffanforDHcor
ROPRFATHEAThetiuaachpaingtioskalsset2),fer
T etetto tedb
To
S
M tota
n-
n-
n-
aTbNc2dT2DofweSfMgPhA
ADA REPORTS
160st 4 months of lactation also had noect on infant visual
maturation,t psychomotor, not mental, devel-ment test scores were
higher in in-ts at 30 months of age (170). Sim-rly, supplementation
of pregnantmen in Norway with fish oil had noect on early measures
of infantural maturation (158), but cogni-e development at 4 years
of ages increased (166). Fish oil supple-ntation in pregnancy may
reduceA in both mothers and their new-rn infants (171). Reduced
growths reported in three studies withterm infants fed formula
contain-DHA from fish oil without ARA2-175). The risks and benefits
ofh oil supplementation during preg-
able 2. Recommendations by the American Dital fat (for adults)
and saturated, monounsaturaased on a 2,000 calorie dietab
tal fatcd
20% of energy25% of energy30% of energy35% of energyFatty
acid/fatty acid class % of energy
FAe (as low as possible)3% of energy7% of energy10% of
energyUFAf (provides remaining fatty acids to meet8% of energy14%
of energy20% of energy25% of energy6 PUFAg (3% to 10% of energy)3%
of energy5% of energy7% of energy10% of energy3 PUFA-ALAh (0.6% to
1.2% of energy)0.6% of energy0.9% of energy1.2% of energy3
PUFAlong-chain PUFA
rans-fatty acids should be as low as possible.umbers are rounded
to nearest whole number.7 g oils recommendedUS Department of
Agriculture Foohe Acceptable Macronutrient Distribution Range for
total fa5% to 35% of energy for children 4 to 18 years. The
Acceptaietary Reference Intake is 5% to 10% energy from n-6
PUFAdeficiency, and intakes of n-6 fatty acids in the range of 3hen
the intake of n-3 fatty acids is at least 0.7% energy.FAsaturated
fatty acids.UFAmonounsaturated fatty acids.UFApolyunsaturated fatty
acids.LA-linolenic acid.ncy and lactation, or in infants as a
vis
6 September 2007 Volume 107 Number 9ans to increase infant DHA
ares unclear.lthough some epidemiologic andervention studies have
suggestedt higher intakes of EPA and DHAassociated with a small
increase
gestational length and reduced risksome pregnancy-associated
compli-ions (158,176,177), other studiesve not confirmed a benefit
ongth of gestation, preeclampsia,ampsia, or gestational hyperten-n
(158,171,178-181). Thus, currentdence does not support a
recom-ndation to increase EPA and DHAreduce risk of preterm
delivery orgnancy-associated complications.ince 1990, the impact of
formulastaining DHA or DHA plus ARA on
ic Association and Dietitians of Canada for, n-6, n-3, and
polyunsaturated fatty acids
Amount
44 g56 g67 g78 g
7 g16 g22 g
l fat)18 g31 g44 g56 g
7 g11 g16 g22 g
1.3 g2.0 g2.7 g500 mg
ide.30% to 40% of energy for children 1 to 3 years
andacronutrient Distribution Range provided by the 2002kes of 3%
energy from n-6 fatty acids prevents signs5% energy will support a
n-6:n-3 ratio of about 4:1ual maturation and neurodevelop- wwnt in
term and preterm infants hasen extensively studied. Some
inves-ators have shown benefits in termants fed formulas with DHA
andA, or DHA from birth, or after ini-l breastfeeding (182,183),
but oth-have not (184). However, most
dies assessed neurodevelopmenttween 6 and 24 months, an age
dur-which there is latency in expres-
n of minor neurological dysfunc-n (185). Evidence that
pretermants benefit from inclusion of DHAd ARA in formula fed
throughoutfirst year after birth is more con-
tent (184,186,187), and formula forterm infants now includes
bothA and ARA. Formulas for term in-ts with ARA and DHA are
alsodely available. One review of 6 of 10domized controlled trials
of addi-n of DHA and ARA to formula con-ded no substantial effect
on infantvelopment, and that more-expen-e formula with added DHA
andA is not necessary (188).he preferred and recommendedrce of
nutrition for infants under 6nths is human milk, and the
avail-ility of infant formulas containingA and DHA does not change
thisommendation. Some studies havend benefits of including DHA andA
in formulas for term infants, andadverse effects of feeding
mar-
ted infant formula containing bothA and DHA in amounts found
inman milk are known. Because ofssible benefits and lack of
adverseects, it is recommended that all in-ts who are not breastfed
be fed amula containing both ARA andA through at least the first
year ofrected age.
LE OF FOOD AND NUTRITIONOFESSIONALS IN IMPLEMENTINGTY ACID
RECOMMENDATIONS FORLTHe special expertise of registered di-tians
(RDs) is important to individ-lize dietary recommendations toieve
optimal food-based dietarytterns. The complexity of translat-fat
and fatty acid recommenda-
ns requires the knowledge andills of food and nutrition
profession-. Once specific targets have beenfor total fat and fatty
acids (Tablethen the type and amount of dif-ent fats (Table 1,
available atmethuA
intthaareinofcathaleneclsioevimetopreS
con
d Gut isble M. Inta% tow.adajournal.org) to be included
-
togoabeguproeasuthethemealstioendieC
toingaciawresabetaFatratiothecomalsdieA
etatantopagPUcaleaingscitheetaqu
Ref1
2
3
4
5
6
7
8
9
10
11
12
13
14
16
17
18
19
20
21
22
23
24
25
26
27
28
29
ADA REPORTSmeet the total fat and fatty acidls in an
energy-controlled diet candetermined. For all fatty acids, theiding
philosophy is a food-based ap-ach. For individuals who do nott
fish, other options may be pur-ed, such as designer foods high inse
fatty acids, foods fortified withse fatty acids, or even supple-nts
(189). The RDs expertise iso needed to translate recommenda-ns for
fatty acids to the appropriateergy intake to achieve a
healthfultary pattern.onsumers lack knowledge on howuse the
Nutrition Facts labels, orredient lists to determine fattyd
contents, RDs must also beare that individuals vary in theirponse
to dietary fat and must bele to recommend appropriate di-ry fat
changes when necessary. Myts Translator, a calculator thatnslates
fat/fatty acid recommenda-ns into daily limits, is available
from
AHA at www.myfatstranslator.. Implicit in this is the need too
monitor adherence to food-basedtary recommendations.s RDs stay
abreast of current di-ry recommendations, it is impor-t that they
effectively respond toics where there is not yet scientificreement,
as is the case with n-6FA. Consequently, RDs will beled upon to
provide guidance in ar-s where the science is still emerg-. As
always, the evolution of theence-base brings clarity and formsbasis
for ongoing revisions in di-ry recommendations and conse-ent
dietary patterns.
erences. American Diabetes Association. Nutritionrecommendations
and interventions for di-abetes. A position statement of the
Ameri-can Diabetes Association. Diabetes Care.2007;30:S48-S65.
. De Backer G, Ambrosioni E, Borch-JohnsenK, Brotons C, Cifkova
R, Dallongeville J,Ebrahim S, Faergeman O, Graham I, Man-cia G,
Manger Cats V, Orth-Gomer K, PerkJ, Pyorala K, Rodicio JL, Sans S,
Sansoy V,Sechtem U, Silber S, Thomsen T, Wood D;Third Joint Task
Force of European andOther Societies on Cardiovascular
DiseasePrevention in Clinical Practice. Europeanguidelines on
cardiovascular disease pre-vention in clinical practice. Third
JointTask Force of European and Other Societ-ies on Cardiovascular
Disease Preventionin Clinical Practice. Eur Heart J.
2003;24:1601-1610.
. Priori SG, Aliot E, Blomstrom-Lundqvist C,Bossaert L,
Breithardt G, Brugada P,
Camm JA, Cappato R, Cobbe SM, Di Mario 15C, Maron BJ, McKenna
WJ, Pedersen AK,Ravens U, Schwartz PJ, Trusz-Gluza M,Vardas P,
Wellens HJ, Zipes DP; EuropeanSociety of Cardiology. Update of the
guide-lines on sudden cardiac death of the Euro-pean Society of
Cardiology. Eur Heart J.2003;24:13-15.
. Van de Werf F, Ardissino D, Betriu A, Cok-kinos DV, Falk E,
Fox KA, Julian D,Lengyel M, Neumann FJ, Ruzyllo W, Thy-gesen C,
Underwood SR, Vahanian A, Ver-heugt FW, Wijns W. Task Force on
theManagement of Acute Myocardial Infarc-tion of the European
Society of Cardiology.Management of acute myocardial infarctionin
patients presenting with ST-segment el-evation. The Task Force on
the Manage-ment of Acute Myocardial Infarction of theEuropean
Society of Cardiology. EurHeart J. 2003;24:28-66.
. Lichtenstein AH, Appel LJ, Brands M, Car-nethon M, Daniels S,
Franch HA, FranklinB, Kris-Etherton P, Harris WS, Howard B,Karanja
N, Lefevre M, Rudel L, Sacks F,Van Horn L, Winston M, Wylie-Rosett
J.American Heart Association NutritionCommittee, Diet and Lifestyle
Recommen-dations Revision 2006: A Scientific State-ment from the
American Heart AssociationNutrition Committee. Circulation.
2006;114:82-96.
. Kris-Etherton PM, Harris W, Appel LJ.AHA Scientific Statement:
Fish consump-tion, fish oil, omega-3 fatty acids and
car-diovascular disease. Circulation. 2002;106:2747-2757.
. National Cholesterol Education Program.Third Report of the
National CholesterolEducation Program (NCEP) Expert Panelon
Detection, Evaluation, and Treatment ofHigh Blood Cholesterol in
Adults (AdultTreatment Panel III) final report. NationalHeart, Lung
and Blood Institute, NationalInstitutes of Health. September 2002.
NIHPublication No. 02-5215.
. National Cholesterol Education Program(NCEP) Expert Panel on
Detection, Evalu-ation, and Treatment of High Blood Choles-terol in
Adults (Adult Treatment Panel III)final report. Circulation.
2002;106:3143-3421.
. US Department of Health and Human Ser-vices, US Department of
Agriculture. Di-etary Guidelines for Americans 2005.Available at:
http://www.healthierus.gov/dietaryguidelines/. Accessed July 10,
2007.
. UK Scientific Advisory Committee on Nu-trition. Advice on fish
consumption: Bene-fits and risks. April 2004. Available
at:http://www.sacn.gov.uk/pdfs/fics_sacn_advise_fish.pdf. Accessed
July 10, 2007.
. FAO/WHO Technical Report No. 916. Diet,Nutrition and the
Prevention of ChronicDiseases. Geneva, Switzerland: WorldHealth
Organization; 2003.
. Institute of Medicine. Dietary Reference In-takes for Energy,
Carbohydrate, Fiber, Fat,Fatty acids, Cholesterol, Protein and
AminoAcids. Washington, DC: National Acade-mies Press; 2002.
. Hotamisligil GS. Inflammation and meta-bolic disorders.
Nature. 2006;444:860-867.
. American Dietetic Association. Hyperlipid-emia Evidence
Analysis Library. Availableat:
http://ebg/adaevidencelibrary.com/template.cfm?templatebibliography&key224.
Ac-cessed October 15, 2005.. Dietitians of Canada. Practice-Based
Evi-
September 2007 Journal ofdence in Nutrition. Available at:
http://www.dieteticsatwork.com/pen. Accessed Janu-ary 14, 2007.
. US Department of Agriculture. NutrientData Lab. Available at:
http://www.nal.usda.gov/fnic/foodcomp/search/. AccessedJanuary 14,
2007.
. Health Canada. Canadian Nutrient File.Available at:
http://www.hc-sc.gc.ca/fn-an/nutrition/fiche-nutri-data/index_e.html.
Ac-cessed January 14, 2007.
. KIM (Keep It Managed) Software Programfor omega-3 and omega-6
fatty acid contentof foods. Available at:
http://efaeducation.nih.gov/sig/kim1.html. Accessed January14,
2007.
. Health Canada. Available at:
http://www.hc-sc.gc.ca/fn-an/index_e.html. AccessedJanuary 14,
2007.
. US Department of Agriculture, US Depart-ment of Health and
Human Services. 2005Dietary Guidelines Advisory CommitteeReport.
Available at:
http://www.health.gov/dietaryguidelines/dga2005/report/. Ac-cessed
October 15, 2005.
. National Heart Foundation of Australia. Areview of the
relationship between dietaryfat and cardiovascular disease. Aust J
NutrDiet. 1999;56:S5-S22.
. Nesheim MC, Yackine AL. Seafood Choic-es: Balancing Benefits
and Risks. Washing-ton, DC: National Academies Press;
2007.Available at http://www.nap.edu/execsumm_pdf/11762.pdf.
Accessed January 14, 2007.
. Obarzanek E, Sacks FM, Vollmer WM,Bray GA, Miller ER 3rd, Lin
PH, KaranjaNM, Most-Windhauser MM, Moore TJ,Swain JF, Bales CW,
Proschan MA, DASHResearch Group. Effects on blood lipids of ablood
pressure-lowering diet: The DietaryApproaches to Stop Hypertension
(DASH)Trial. Am J Clin Nutr. 2001;74:80-89.
. Jenkins DJ, Kendall CW, Marchie A,Faulkner DA, Wong JMW, de
Souza R,Emam A, Parker TL, Vidgen E, LapsleyKG, Trautwein EA, Josse
RG, Leiter LA,Connelly PW. Effects of a dietary portfolioof
cholesterol-lowering foods vs lovastatinon serum lipids and
C-reactive protein.JAMA. 2003;290:502-510.
. Gardner CD, Coulston A, Chatterjee L,Rigby A, Spiller G,
Farquhar JW. The effectof a plant-based diet on plasma lipids
inhypercholesterolemic adults: A randomizedtrial. Ann Int Med.
2005;142:725-733.
. Appel LJ, Sacks FM, Carey VJ, ObarzanekE, Swain JF, Miller ER
3rd, Conlin PR,Erlinger TP, Rosner BA, Laranjo NM,Charleston J,
McCarron P, Bishop LM;OmniHeart Collaborative Research
Group.Effects of protein, monounsaturated fat,and carbohydrate
intake on blood pressureand serum lipids: Results of the Omni-Heart
randomized trial. JAMA. 2005;294:2455-2464.
. Hu FB, Stampfer MJ, Manson JE, Rimm E,Colditz GA, Rosner BA,
Hennekens CH,Willett WC. Dietary fat intake and the riskof coronary
heart disease in women.N EnglJ Med. 1997;337:1491-1499.
. Pischon T, Hankinson SE, Hotamisligil GS,Rifai N, Willett WC,
Rimm EB. Habitualdietary intake of n-3 and n-6 fatty acids
inrelation to inflammatory markers amongUS men and women.
Circulation. 2003;108:155-160.
. Tanasescu M, Cho E, Manson JE, Hu FB.
Dietary fat and cholesterol and the risk of
the AMERICAN DIETETIC ASSOCIATION 1607
-
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
ADA REPORTS
160cardiovascular disease among women withtype 2 diabetes. Am J
Clin Nutr. 2004;79:999-1005.
. Salmeron J, Hu FB, Manson JE, StampferMJ, Colditz GA, Rimm EB,
Willett WC.Dietary fat intake and risk of type 2 diabe-tes in
women. Am J Clin Nutr. 2001;73:1019-1026.
. Sacks FM, Katan M. Randomized clinicaltrials on the effects of
dietary fat and car-bohydrate on plasma lipoproteins and
car-diovascular disease. Am J Med 2002;113(suppl 9B):13S-24S.
. European Commission. Nutrition and dietfor healthy lifestyles
in Europe: Scienceand policy implications. Eurodiet CoreReport.
2001. Available at:
http://ec.europa.eu/health/ph_determinants/life_style/nutrition/report01_en.pdf.
AccessedJuly 10, 2007.
. Hamazaki T, Okuyama H. The Japan Soci-ety for Lipid Nutrition
recommends to re-duce the intake of linoleic acid. A reviewand
critique of the scientific evidence.World Rev Nutr Diet.
2003;92:109-132.
. International Society for the Study of FattyAcids and Lipids.
Adequate Intakes. Avail-able at:
http://www.issfal.org.uk/adequate-intakes.html. Accessed July 10,
2007.
. Reaven PD, Grasse BJ, Tribble DL. Ef-fects of
linoleate-enriched and oleate-en-riched diets in combination with
alpha-tocopherol on the susceptibility of LDLand LDL subfractions
to oxidative modi-fication in humans. Arterioscler
Thromb.1994;14:557-566.
. Calder PC. Polyunsaturated fatty acids andinflammation.
Prostaglandins Leukot Es-sent Fatty Acids. 2006;75:197-202.
. Akabas SR, Deckelbaum RJ. Summary of aworkshop on n-3 fatty
acids: Current statusof recommendations and future directions.Am J
Clin Nutr. 2006;83(suppl):1536S-1538S.
. Harris WS, Assad B, Poston C. Tissueomega-6/omega-3 fatty acid
ratio and riskfor coronary heart disease. Am J
Cardiol2006;98(4A):19i-26i.
. Ernst ND, Sempos CT, Briefel RR, ClarkMB. Consistency between
US dietary fatintake and serum total cholesterol concen-trations:
The National Health and Nutri-tion Examination Surveys. Am J Clin
Nutr.1997;66:965S-972S.
. Franz MJ, Bantle JP, Beebe CA, BrunzellJD, Chiasson JL, Garg
A, Holzmeister LA,Hoogwerf B, Mayer-Davis E, MooradianAD, Purnell
JQ, Wheeler M, American Di-abetes Association. Nutrition
principlesand recommendations in diabetes. DiabetesCare.
2004;27(suppl 1):S36-S46.
. Gardner CD, Kraemer HC. Monounsatu-rated versus
polyunsaturated dietary fatand serum lipids. A meta-analysis.
Arterio-scler Thromb Vasc Biol. 1995;15:1917-1927.
. Ferrucci L, Cherubini A, Bandinelli S, Bar-tali B, Corsi A,
Lauretani F, Martin A, An-dres-Lacueva C, Senin U, Guralnik JM.
Re-lationship of plasma polyunsaturated fattyacids to circulating
inflammatory markers.J Clin Endocrinol Metab. 2006;91:439-446.
. Food and Drug Administration, US Envi-ronmental Protection
Agency. What youneed to know about mercury in fish andshellfish.
EPA-823-R-04-005. March 2004.
Available at: http://www.cfsan.fda.gov/
8 September 2007 Volume 107 Number 9dms/admehg3.html. Accessed
July 10,2005.
. Health Canada. Advisory. Information onmercury levels in fish.
Available at:
http://www.hc-sc.gc.ca/ahc-asc/media/advisories-avis/2002/2002_41_e.html.
Accessed Janu-ary 14, 2007.
. Mozaffarian D, Rimm EB. Fish intake, con-taminants, and human
health. Evaluatingthe risks and benefits. JAMA.
2006;296:1885-1899.
. Raiten DJ, Talbot JM, Waters JH. Life Sci-ences Research
Office Report. Executivesummary of the report: Assessment of
nu-trient requirements for infant formulas.Available at:
http://www.nutritioninmedicine.com/PDF/Handouts/TermInfantHandout.pdf.
Accessed July 10, 2007.
. Willerson JT, Ridker PM. Inflammation asa cardiovascular risk
factor. Circulation.2004;109:II2-II10.
. Posner BM, Cobb JL, Belanger AJ, CupplesLA, DAgostino RB,
Stokes J 3rd. Dietarylipid predictors of coronary heart disease
inmen. The Framingham Study. Arch InternMed.
1991;151:1181-1187.
. Keys A. Coronary heart disease in sevencountries. Circulation.
1970;41:I1-I211.
. Schaefer EJ. Lipoproteins, nutrition, andheart disease. Am J
Clin Nutr. 2002;75:191-212.
. Keys A, Anderson JT, Grande F. Serumcholesterol response to
changes in the diet.IV. Particular saturated fatty acids in
thediet. Metabolism. 1965;14:776-787.
. Hegsted DM, McGandy RB, Myers ML,Stare EJ. Quantitative
effects of dietary faton serum cholesterol in man. Am J ClinNutr.
1965;17:281-295.
. Mensink RP, Katan MB. Effect of dietaryfatty acids on serum
lipids and lipopro-teins. A meta-analysis of 27 trials.
Arterio-scler Thromb. 1992;12:911-919.
. Mensink RP, Zock PL, Kester AD, KatanMB. Effects of dietary
fatty acids and car-bohydrates on the ratio of serum total toHDL
cholesterol and on serum lipids andapolipoproteins: A meta-analysis
of 60 con-trolled trials. Am J Clin Nutr. 2003;77:1146-1155.
. Criqui MH, Golomb BA. Epidemiologic as-pects of lipid
abnormalities. Am J Med.1998;105:48S-57S.
. Castelli WP, Anderson K, Wilson PW, LevyD. Lipids and risk of
coronary heart dis-ease. The Framingham Study. Ann Epide-miol.
1992;2:23-28.
. Kris-Etherton PM, Yu S. Individual fattyacid effects on plasma
lipids and lipopro-teins: Human studies. Am J Clin
Nutr1997;65(suppl 5):1628S-1644S.
. Kris-Etherton PM. AHA Science Advisory:Monounsaturated fatty
acids and risk ofcardiovascular disease. Circulation.
1999;100:1253-1258.
. Garg A. High-monounsaturated-fat dietsfor patients with
diabetes mellitus: A meta-analysis. Am J Clin Nutr
1998;67(suppl):577S-582S.
. Nkondjock A, Shatenstein B, MaisonneuveP, Ghadirian P.
Assessment of risk associ-ated with specific fatty acids and
colorectalcancer among French-Canadians in Mon-treal: A
case-control study. Int J Epidemiol.2003;32:200-209.
. Kushi L, Giovannucci E. Dietary fat andcancer. Am J Med.
2002;113(suppl 9):63S-
70S.. Lipworth L, Martinez ME, Angell J, HsiehCC, Trichopoulos
D. Olive oil and humancancer: An assessment of the evidence.
PrevMed. 1997;26:181-190.
. Saadatian-Elahi M, Norat T, Goudable J,Riboli E. Biomarkers of
dietary fatty acidintake and the risk of breast cancer:
Ameta-analysis. Int J Cancer. 2004;111:584-591.
. Lada AT, Rudel LL. Dietary monounsatu-rated versus
polyunsaturated fatty acids:Which is really better for protection
fromcoronary heart disease? Curr Opin Lipidol.2003;14:41-46.
. Baylin A, Kabagambe EK, Ascherio A,Spiegelman D, Campos H.
High 18:2 trans-fatty acids in adipose tissue are associatedwith
increased risk of nonfatal acute myo-cardial infarction in Costa
Rican adults. JNutr. 2003;133:1186-1191.
. Lemaitre RN, King IB, Raghunathan TE,Pearce RM, Weinmann S,
Knopp RH, Co-pass MK, Cobb LA, Siscovick DS. Cellmembrane
trans-fatty acids and the risk ofprimary cardiac arrest.
Circulation. 2002;105:697-701.
. Pietinen P, Ascherio A, Korhonen P, Hart-man AM, Willett WC,
Albanes D, VirtamoJ. Intake of fatty acids and risk of
coronaryheart disease in a cohort of Finnish men.The
Alpha-Tocopherol, Beta-Carotene Can-cer Prevention Study. Am J
Epidemiol.1997;145:876-887.
. Kromhout D, Menotti A, Bloemberg B, Ara-vanis C, Blackburn H,
Buzina R, DontasAS, Fidanza F, Giampaoli S, Jansen A,Karvonen M,
Katan M, Nissinen A,Nedeljkovic S, Pekkanen J, Pekkarinen M,Punsar
S, Rasanen L, Simic B, Toshima H.Dietary saturated and trans fatty
acids andcholesterol and 25-year mortality from cor-onary heart
disease: The Seven CountriesStudy. Prev Med. 1995;24:308-315.
. Ascherio A, Hennekens CH, Buring JE,Master C, Stampfer MJ,
Willett WC.Trans-fatty acids intake and risk of myo-cardial
infarction. Circulation. 1994;89:94-101.
. Sun Q, Ma J, Campos H, Hankinson SE,Manson JE, Stampfer MJ,
Rexrode KM,Willett WC, Hu FB. A prospective study oftrans fatty
acids in erythrocytes and risk ofcoronary heart disease.
Circulation. 2007;115:1858-1865.
. Mozaffarian D, Rimm EB, King IB, LawlerRL, McDonald GB, Levy
WC. Trans fattyacids and systemic inflammation in heartfailure. Am
J Clin Nutr. 2004;80:1521-1525.
. Gatto LM, Sullivan DR, Samman S. Post-prandial effects of
dietary trans fatty acidson apolipoprotein(a) and cholesteryl
estertransfer. Am J Clin Nutr. 2003;77:1119-1124.
. Mauger JF, Lichtenstein AH, Ausman LM,Jalbert SM, Jauhiainen
M, Ehnholm C,Lamarche B. Effect of different forms ofdietary
hydrogenated fats on LDL particlesize. Am J Clin Nutr.
2003;78:370-375.
. Mozaffarian D. Trans fatty acidsEffectson systemic
inflammation and endothelialfunction. Atheroscler Suppl.
2006;7:29-32.
. Mozaffarian D, Katan MB, Ascherio A,Stampfer MJ, Willett WC.
Trans fatty acidsand cardiovascular disease. N Engl J
Med.2006;354:1601-1613.
. Bakker EC, Hys AJA, Kester ADM, Vles
JSH, Dubas JS, Blanco CE, Hornstra G.
-
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
ADA REPORTSLong-chain polyunsaturated fatty acids atbirth and
cognitive function at 7 y of age.Eur J Clin Nutr.
2003;57:89-95.
. Bakker N, Vant Veer P, Zock PL. Adiposefatty acids and cancers
of the breast, pros-tate and colon: An ecological study.EURAMIC
Study Group. Int J Cancer.1997;72:587-591.
. Kohlmeier L, Simonsen N, Vant Veer P,Strain JJ, Martin-Moreno
JM, Margolin B,Huttunen JK, Fernandez-Crehuet NavajasJ, Martin BC,
Thamm M, Kardinaal AF,Kok FJ. Adipose tissue trans fatty acidsand
breast cancer in the European Commu-nity Multicenter Study on
Antioxidants,Myocardial Infarction, and Breast Cancer.Cancer
Epidemiol Biomarkers Prev. 1997;6:705-710.
. Ip C, Marshall JR. Trans fatty acids andcancer. Nutr Rev.
1996;54:138-145.
. Hu FB, van Dam RM, Liu S. Diet and riskof type II diabetes:
The role of types of fatand carbohydrate. Diabetologia.
2001;44:805-817.
. Rainer L, Heiss CJ. Conjugated linoleicacid: Health
implications and effects onbody composition. J Am Diet Assoc.
2004;104:963-968.
. Moloney F, Yeow TP, Mullen A, Nolan JJ,Roche HM. Conjugated
linoleic acid supple-mentation, insulin sensitivity, and
lipopro-tein metabolism in patients with type 2diabetes mellitus.
Am J Clin Nutr. 2004;80:887-895.
. Riserus U, Basu S, Jovinge S, FredriksonGN, Arnlov J, Vessby
B. Supplementationwith conjugated linoleic acid causes
isomer-dependent oxidative stress and elevated C-reactive protein:
A potential link to fattyacid-induced insulin resistance.
Circula-tion. 2002;106:1925-1929.
. Riserus U, Vessby B, Arnlov J, Basu S.Effects of
cis-9,trans-11 conjugated linoleicacid supplementation on insulin
sensitiv-ity, lipid peroxidation, and proinflamma-tory markers in
obese men. Am J ClinNutr. 2004;80:279-283.
. Masters N, McGuire MA, Beerman KA,Dasgupta N, McGuire MK.
Maternal sup-plementation with CLA decreases milk fatin humans.
Lipids. 2002;37:133-138.
. Ritzenthaler KL, McGuire MK, McGuireMA, Shultz TD, Koepp AE,
Luedecke LO,Hanson TW, Dasgupta N, Chow BP. Con-sumption of
conjugated linoleic acid (CLA)-enriched cheese does not alter milk
fat orimmunity in lactating women. J Nutr.2005;135:422-430.
. Goyens PLL, Spilker ME, Zock PL, Katan,MB, Mensink RP.
Conversion of -linolenicacid in humans is influenced by the
abso-lute amounts of -linolenic acid and linoleicacid in the diet
and not by their ratio. Am JClin Nutr. 2006;84:44-53.
. Eckel RH, Borra S, Lichtenstein AH, Yin-Piazza SY.
Understanding the Complexityof Trans Fatty Acid Reduction in the
Amer-ican Diet. American Heart AssociationTrans Fat Conference
2006. Report of theTrans Fat Conference Planning Group.
Cir-culation. 2007;115:2220-2235.
. Harris WS, Poston WC, Haddock CK. Tis-sue n-3 and n-6 fatty
acids and risk forcoronary heart disease events. Arthroscle-rosis.
2007;193:1-10.
. Dayton S, Pearce ML, Hashimoto S, DixonWJ, Tomiyasu U. A
controlled clinical trial
of a diet high in unsaturated fat in prevent-ing complications
of atherosclerosis. Circu-lation. 1969;40(suppl II):1-63.
. Turpeinen O, Karvonen MJ, PekkarinenM, Miettinen M, Elosuo R,
Paavilainen E.Dietary prevention of coronary heart dis-ease: The
Finnish Mental Hospital Study.Int J Epidemiol. 1979;8:99-118.
. Leren P. The Oslo-Diet Heart Study: Eleven-year report.
Circulation. 1970;42:935-942.
. Xiao C, Giacca A, Carpentier A, Lewis GF.Differential effects
of monounsaturated,polyunsaturated and saturated fat ingestionon
glucose-stimulated insulin secretion, sen-sitivity and clearance in
overweight andobese, non-diabetic humans.
Diabetologia.2006;49:1371-1379.
. Trevisan M, Krogh V, Freudenheim J,Blake A, Muti P, Panico S,
Farinaro E,Mancini M, Menotti A, Ricci G. Consump-tion of olive
oil, butter, and vegetable oilsand coronary heart disease risk
factors.The Research Group ATS-RF2 of the Ital-ian National
Research Council. JAMA.1990;263:688-692.
. Canadian Diabetes Association ClinicalPractice Guidelines
Expert Committee.Clinical practice guidelines for the preven-tion
and management of diabetes in Can-ada. Can J Diabetes 2003;27(suppl
2):S1-S163. Available at:
http://www.diabetes.ca/cpg2003/downloads/cpgcomplete.pdf. Ac-cessed
July 10, 2007.
. Zock PL, Katan MB. Linoleic acid intakeand cancer risk: A
review and meta-analy-sis. Am J Clin Nutr. 1998;68:142-153.
. Shoda R, Matsueda K, Yamato S, UmedaN. Epidemiologic analysis
of Crohn diseasein Japan: Increased dietary intake of
n-6polyunsaturated fatty acids and animalprotein relates to the
increased incidence ofCrohn disease in Japan. Am J Clin
Nutr.1996;63:741-745.
. Sturdevant RA, Pearce ML, Dayton S. In-creased prevalence of
cholelithiasis in meningesting a serum-cholesterol-loweringdiet. N
Engl J Med. 1973;288:24-27.
. Pearce ML, Dayton S. Incidence of cancerin men on a diet high
in polyunsaturatedfat. Lancet. 1971;1:464-467.
. Tsai CJ, Leitzmann MF, Willett WC, Gio-vannucci EL. The effect
of long-term intakeof cis unsaturated fats on the risk for
gall-stone disease in men: A prospective cohortstudy. Ann Intern
Med. 2004;141:514-522.
. Lands WE. Primary prevention in cardio-vascular disease:
Moving out of the shad-ows of the truth about death. Nutr
MetabCardiovasc Dis. 2003;13:154-164.
. Calder PC, Grimble RF. Polyunsaturatedfatty acids,
inflammation and immunity.Eur J Clin Nutr
2002;56(suppl):S14-S19.
. Tsimikas S, Reaven PD. The role of dietaryfatty acids in
lipoprotein oxidation and ath-erosclerosis. Curr Opin Lipidol.
1998;9:301-307.
. Simopoulos AP. Evolutionary aspects ofdiet and essential fatty
acids. World RevNutr Diet. 2001;88:18-27.
. Simopoulos AP. Essential fatty acids inhealth and chronic
disease. Am J ClinNutr. 1999;70(suppl 3):560S-569S.
. Salem N Jr, Wegher B, Mena P, Uauy R.Arachidonic and
docosahexaenoic acids arebiosynthesized from their 18-carbon
pre-cursors in human infants. Proc Natl AcadSci U S A.
1996;93:49-54.
. Pawlosky RJ, Hibbeln JR, Lin Y, Goodson
S, Riggs P, Sebring N, Brown GL, Salem N
September 2007 Journal ofJr. Effects of beef- and fish-based
diets onthe kinetics of n-3 fatty acid metabolism inhuman subjects.
Am J Clin Nutr. 2003;77:565-572.
. Hussein N, Ah-Sing E, Wilkinson P, LeachC, Griffin BA,
Millward DJ. Long-chainconversion of [13C]linoleic acid and
alpha-linolenic acid in response to markedchanges in their dietary
intake in men. JLipid Res. 2005;46:269-280.
. Goyens PL, SpilkerME, Zock PL, KatanMB,Mensink RP.
Compartmental modeling toquantify alpha-linolenic acid conversion
afterlonger term intake of multiple tracer boluses.J Lipid Res.
2005;46:1474-1483.
. Agency of Healthcare Research and Qual-ity. Effects of omega-3
fatty acids on car-diovascular risk factors and intermediatemarkers
of cardiovascular disease. 2004.Available at:
http://www.ahrq.gov/clinic/epcsums/o3cardrisksum.htm. Accessed
Oc-tober 15, 2005.
. Djousse L, Pankow JS, Eckfeldt JH, Fol-som AR, Hopkins PN,
Province MA, HongY, Ellison RC. Relation between dietarylinolenic
acid and coronary artery diseasein the National Heart, Lung, and
BloodInstitute Family Heart Study. Am J ClinNutr.
2001;74:612-619.
. Hu FB, Stampfer MJ, Manson JE, RimmEB, Wolk A, Colditz GA,
Hennekens CH,Willett WC. Dietary intake of alpha-lino-lenic acid
and fatal ischemic heart diseaseamong women. Am J Clin Nutr.
1999;69:890-897.
. Dolecek TA. Epidemiological evidence ofrelationships between
dietary poly-unsat-urated fatty acids and mortality in theMultiple
Risk Factor Intervention Trial.Proc Soc Exp Biol Med.
1992;200:177-182.
. Albert CM, Oh K, Whang W, Manson JE,Chae CU, Stampfer MJ,
Willett WC, HuFB. Dietary alpha-linolenic acid intake andrisk of
sudden cardiac death and coronaryheart disease. Circulation.
2005;112:3232-3238.
. de Lorgeril M, Salen P, Martin JL, Mon-jaud I, Delaye J,
Mamelle N. Mediterra-nean diet, traditional risk factors and
therate of cardiovascular complications aftermyocardial infarction:
Final report of theLyon Diet Heart Study. Circulation.
1999;99:779-785.
. Mozaffarian D, Ascherio A, Hu FB,Stampfer MJ, Willett WC,
Siscovick DS,Rimm EB. Interplay between differentpolyunsaturated
fatty acids and risk of cor-onary heart disease in men.
Circulation.2005;111:157-164.
. Brouwer IA, Katan MB, Zock PL. Dietaryalpha-linolenic acid is
associated with re-duced risk of fatal coronary heart disease,but
increased prostate cancer risk: A meta-analysis. J Nutr.
2004;134:919-922.
. Koralek DO, Peters U, Andriole G, RedingD, Kirsh V, Subar A,
Schatzking A, HayesR, Leitzmann MF. A prospective study ofdietary
alpha-linolenic acid and the risk ofprostate cancer (United
States). CancerCauses Control. 2006;17:783-791.
. de Lorgeril M, Salen P. -linolenic acid,coronary heart
disease, and prostate can-cer. J Nutr. 2004;134:3385.
. Christensen JH, Riahi S, Schmidt EB, Mol-gaard H, Kirstein
Pedersen A, Heath F,Cosedis Nielsen J, Toft E. n-3 Fatty acidsand
ventricular arrhythmias in patients
with ischaemic heart disease and implant-
the AMERICAN DIETETIC ASSOCIATION 1609
-
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
ADA REPORTS
161able cardioverter defibrillators.
Europace.2005;7:338-344.
. Schrepf R, Limmert T, Claus Weber P,Theisen K, Sellmayer A.
Immediate effectsof n-3 fatty acid infusion on the induction
ofsustained ventricular tachycardia. Lancet.2004;363:1441-1442.
. Brouwer IA, Heeringa J, Geleijnse JM,Zock PL, Witteman JC.
Intake of very long-chain n-3 fatty acids from fish and inci-dence
of atrial fibrillation. The RotterdamStudy. Am Heart J.
2006;151:857-862.
. Mozaffarian D, Lemaitre RN, Kuller LH,Burke GL, Tracy RP,
Siscovick DS; Cardio-vascular Health Study. Cardiac benefits offish
consumption may depend on the typeof fish meal consumed: The
CardiovascularHealth Study. Circulation. 2003;107:1372-1377.
. Hu FB, Bronner L, Willett WC, StampferMJ, Rexrode KM, Albert
CM, Hunter D,Manson JE. Fish and omega-3 fatty acidintake and risk
of coronary heart disease inwomen. JAMA. 2002;287:1815-1821.
. Siscovick DS, Raghunathan T, King I,Weinmann S, Bovbjerg VE,
Kushi L, CobbLA, Copass MK, Psaty BM, Lemaitre R,Retzlaff B, Knopp
RH. Dietary intake oflong-chain n-3 polyunsaturated fatty acidsand
the risk of primary cardiac arrest.Am J Clin Nutr
2000;71(suppl):208S-212S.
. Albert CM, Hennekens CH, ODonnell CJ,Ajani UA, Carey VJ,
Willett WC, RuskinJN, Manson JE. Fish consumption and riskof sudden
cardiac death. JAMA. 1998;279:23-28.
. Dolecek TA, Granditis G. Dietary polyunsat-urated fatty acids
and mortality in the Mul-tiple Risk Factor Intervention Trial
(MR-FIT). World Rev Nutr Diet. 1991;66:205-216.
. He K, Song Y, Daviglus ML, Liu K, VanHorn L, Dyer AR,
Greenland P. Accumu-lated evidence on fish consumption and
cor-onary heart disease mortality: A meta-analysis of cohort
studies. Circulation.2004;109:2705-2711.
. He K, Song Y, Daviglus ML, Liu K, VanHorn L, Dyer AR,
Goldbourt U, GreenlandP. Fish consumption and incidence ofstroke: A
meta-analysis of cohort studies.Stroke. 2004;35:1538-1542.
. Wang C, Harris WS, Chung M, Lichten-stein AH, Balk EM,
Kupelnick B, JordanHS, Lau J. n-3 fatty acids from fish or fish-oil
supplements, but not -linolenic acid,benefit cardiovascular disease
outcomes inprimary- and secondary-prevention stud-ies: A systematic
review. Am J Clin Nutr.2006;84:5-17.
. de Deckere EA. Possible beneficial effect offish and fish n-3
polyunsaturated fatty ac-ids in breast and colorectal cancer. Eur
JCancer Prev. 1999;8:213-221.
. Nkondjock A, Shatenstein B, MaisonneuveP, Ghadirian P.
Specific fatty acids andhuman colorectal cancer: An overview.Cancer
Detect Prev. 2003;27:55-66.
. Calviello G, Di Nicuolo F, Gragnoli S, Pic-cioni E, Serini S,
Maggiano N, Tringali G,Navarra P, Ranelletti FO, Palozza P.
n-3PUFAs reduce VEGF expression in humancolon cancer cells
modulating the COX-2/PGE2 induced ERK-1 and -2 and HIF-1al-pha
induction pathway. Carcinogenesis.2004;25:2303-2310.
. MacLean CH, Newberry SJ, Mojica WA,Khanna P, Issa AM, Suttorp
MJ, Lim YW,
Traina SB, Hilton L, Garland R, Morton 151
0 September 2007 Volume 107 Number 9SC. Effects of omega-3 fatty
acids on cancerrisk: A systematic review. JAMA.
2006;295:403-415.
. SanGiovanni JP, Chew EY. The role ofomega-3 long-chain
polyunsaturated fattyacids in health and disease of the retina.Prog
Retin Eye Res. 2005;24:87-138.
. Peet M, Stokes C. Omega-3 fatty acids inthe treatment of
psychiatric disorders.Drugs. 2005;65:1051-1059.
. Hibbeln JR, Nieminen LR, Blasbalg TL,Riggs JA, Lands WE.
Healthy intakes ofn-3 and n-6 fatty acids: Estimations consid-ering
worldwide diversity. Am J Clin Nutr.2006;83(suppl):1483S-1493S.
. Schaefer EJ, Bongard V, Beiser AS,Lamon-Fava S, Robins SJ, Au
R, TuckerKL, Kyle DJ, Wilson PW, Wolf PA. Plasmaphosphatidylcholine
docosahexaenoic acidcontent and risk of dementia and Alzhei-mer
disease: The Framingham HeartStudy. Arch Neurol.
2006;63:1545-1550.
. van Gelder BM, Tijhuis M, Kalmijn S,Kromhout D. Fish
consumption, n-3 fattyacids, and subsequent 5-y cognitive declinein
elderly men: The Zutphen Elderly Study.Am J Clin Nutr.
2007;85:1142-1147.
. Beydoun MA, Kaufman JS, Satia JA, Ro-samond W, Folsom AR.
Plasma n-3 fattyacids and the risk of cognitive decline inolder
adults: The Atherosclerosis Risk inCommunities Study. Am J Clin
Nutr. 2007;85:1103-1111.
. Innis SM, Palaty J, Vaghri Z, Lockitch G.Increased levels of
mercury associated withhigh fish intakes among children from
Van-couver, Canada. J Pediatr 2006;148:759-763.
. Innis SM. Polyunsaturated fatty acids inhuman milk: An
essential role in infantdevelopment. Adv Exp Med Biol.
2004;554:27-43.
. Innis SM. Essential fatty acids in growthand development. Prog
Lipid Res. 1991;30:39-103.
. Farquharson J, Cockburn F, Patrick WA,Jamieson EC, Logan RW.
Effect of diet onthe fatty acid composition of the
majorphospholipids of infant cerebral cortex.Arch Dis Child.
1995;72:198-203.
. Makrides M, Neumann MA, Byard RW,Simmer K, Gibson RA. Fatty
acid composi-tion of brain, retina, and erythrocytes inbreast- and
formula-fed infants. Am J ClinNutr. 1994;60:189-194.
. Elias SL, Innis SM. Newborn infantplasma trans, conjugated
linoleic, n-6 andn-3 fatty acids are related to maternalplasma
fatty acids, length of gestation andbirth weight and length. Am J
Clin Nutr.2001;73:807-814.
. Koletzko B, Braun M. Arachidonic acid andearly human growth,
is there a relation?Ann Nutr Metab. 1991;35:128-131.
. Innis SM. Trans fatty acid intakes duringpregnancy and early
childhood. AthersoclerSuppl. 2006;7:17-20.
. Chen ZY, Pelletier G, Hollywood R, Rat-nayake WM. Trans fatty
acid isomers inCanadian human milk. Lipids. 1995;30:15-21.
. Innis SM, King J. Trans fatty acids in hu-man milk are
inversely associated withconcentrations of essential all-cis n-6
andn-3 fatty acids and determine trans, butnot n-6 and n-3, fatty
acids in plasma lipidsof breast-fed infants. Am J Clin Nutr.
1999;70:383-390.. Mosley EE, Wright AL, McGuire MK,McGuire MA.
Trans fatty acids in milkproduced by women in the United States.Am
J Clin Nutr. 2005;82:1292-1297.
. Friesen R, Innis SM. Trans fatty acids inhuman milk in Canada
declined with theintroduction of trans fat food labeling. JNutr.
2006;136:2558-2561.
. Carnielli VP, Wattimena DJ, Luijendijk IH,Boerlage A,
Degenhart HJ, Sauer PJ. Thevery low birth weight premature infant
iscapable of synthesizing arachidonic and do-cosahexaenoic acids
from linoleic and linole-nic acids. Pediatr Res.
1996;40:169-174.
. Uauy R, Mena P, Wegher B, Nieto S, SalemN Jr. Long chain
polyunsaturated fattyacid formation in neonates, effect of
gesta-tional age and intrauterine growth. PediatrRes.
2000;47:127-135.
. Williams CM, Burdge GC. Long-chain n-3PUFA: Plant v marine
sources. Proc NutrSoc. 2006;65:42-50.
. Ponder DL, Innis SM, Benson JD, SiegmanJS. Ponder DL, Innis
SM, Benson JD, Sieg-man JS. Docosahexaenoic acid status ofterm
infants fed breast milk or infant for-mula containing soy oil or
corn oil. PediatrRes. 1992;32:683-688.
. Innis SM. Essential fatty acid transfer andfetal development.
Placenta. 2005;26:S70-S75.
. Helland IB, Saugstad OD, Smith L, SaaremK, Soluoll R, Ganes T,
Drevon CA. Similareffects on infants of n-3 and n-6 fatty
acidssupplementation to pregnant and lactatingwomen. Pediatrics.
2001;108:E82-E92.
. Innis SM, Gilley J, Werker J. Are human-milk long-chain
polyunsaturated fatty ac-ids related to visual and neural
develop-ment in breast-fed infants? J Pediatr.
2001;139:532-538.
. Innis SM. Perinatal biochemistry andphysiology of long chain
polyunsaturatedfatty acids. J Pediatr. 2003;143:S1-S8.
. Ceruku SR, Montegomery-Downs HE, Far-kas SL, Thoman EB,
Lammi-Keefe CJ.Higher maternal plasma docosahexaenoicacid during
pregnancy is associated withmore mature neonatal sleep-state
pattern-ing. Am J Clin Nutr. 2002;76:608-613.
. Jorgensen MH, Hernell O, Hughes E,Michaelsen KF. Is there a
relation betweendocosahexaenoic acid concentration inmothers milk
and visual acuity develop-ment in term infants. J Pediatr
Gastroen-terl Nutr. 2001;32:293-296.
. Hibbeln JR, Davis JM, Steer C, Emmett P,Rogers I, Williams C,
Golding J. Maternalseafood consumption in pregnancy
andneurodevelopmental outcomes in childhood(ALSPAC study): An
observational cohortstudy. Lancet. 2007;369:578-585.
. Innis SM. Dietary (n-3) fatty acids andbrain development. J
Nutr. 2007;137:855-859.
. Ghys A, Bakker E, Hornstra G, van denHount M. Red blood cell
and plasma phos-pholipid arachidonic and docosahexaenoicacid at
birth and cognitive development at4 years of age. Early Human Dev.
2002;69:83-90.
. Helland IB, Smith L, Saarem K, SaugstadOD, Drevon CA. Maternal
supplementa-tion with very-long-chain n-3 fatty acidsduring
pregnancy and lactation augmentschildrens IQ at 4 years of age.
Pediatrics.2003;111:e39-e44.
. Cohen JT, Bellinger DC, ConnorWE, Shay-
witz BA. A quantitative analysis of prena-
-
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
A Delegates Leadership Team on April1 December 31, 2011. ADA
authorizesre t/support paper, in its entirety, pro-v quests to use
portions of the positionm ers at 800/877-1600, ext 4835, orp
D, RD (Penn State University, Uni-v DN (University of British
Columbia,V
, PhD, RD (Ohio University, Athens,O th Israel Deaconess Medical
Center,B ractice Dietetic Practice Group (De-b n management
specialist, self-em-p unn, MA, RD (Keene State College,K (The
Center for Genetics, Nutritiona
Bruce E. McDonald, PhD, FCIFST(U , Canada); Catherine J. Field,
PhD,R AB, Canada); Frances Johnson, RD(P , British Columbia,
Canada); RhonaH Waterloo, Waterloo, ON, Canada).
orkgroup: Sonja Connor, MS, RD(c ; Norman Salem Jr, PhD
(contenta
ADA REPORTStal intake of n-3 polyunsaturated fattyacids and
cognitive development. Am JPrev Med. 2005;29:366-374.
. Lauritzen L, Jorgensen MH, Mikkelsen TB,Skovgaard M, Straarup
EM, Olsen SF, HoyCE,Michaelsen KF.Maternal fish oil
supple-mentation in lactation: Effect on visual acu-ity and n-3
fatty acid content of infant eryth-rocytes. Lipids.
2004;39:195-206.
. Lauritzen L, Jorgensen MH, Olsen SF,Straarup EM, Michaelsen
KF. Maternalfish oil supplementation in lactation: Effecton
developmental outcome in breast-fed in-fants. Reprod Nutr Dev.
2005;45:535-547.
. Jensen CL, Voigt RG, Prager TC, Zou YL,Fraley JK, Rozelle JC,
Turcich MR,Llorente AM, Anderson RE, Heird WC. Ef-fect of maternal
docosahexaenoic acid in-take on visual function and
neurodevelop-ment in breast-fed infants. Am J Clin
Nutr.2005;82:125-132.
. Dunstan JA, Mori TA, Barden A, Beilin LJ,Holt PG, Calder PC,
Taylor AL, PrescottSL. Effects of n-3 polyunsaturated fattyacid
supplementation in pregnancy on ma-ternal and fetal erythrocyte
fatty acid com-position. Eur J Clin Nutr. 2004;58:429-437.
. Carlson SE, Werkman SH, Peeples JM,Cooke RJ, Tolley EA.
Arachidonic acid sta-tus correlates with first year growth in
pre-term infants. Proc Natl Acad Sci U S A.1993;90:1073-1077.
. Carlson SE, Cooke RJ, Werkman SH,Tolley EA. First year growth
of preterminfants fed standard compared to marine-oil n-3
supplemented formula. Lipids.1996;27:901-907.
. Carlson SE,Werkman, SH, Tolley EA. Effectof long-chain n-3
fatty acid supplementationon visual acuity and growth of preterm
in-fants with and without bronchopulmonarydysplasia. Am J Clin
Nutr. 1996;63:687-697.
. Ryan AS, Montalto MB, Groh-Wargo S, Mi-mouni F,
Sentipal-Walerius J, Doyle J,Siegman JS, Thomas AJ. Effect of
DHA-containing formula on growth of preterminfants to 59 weeks
postmenstrual age.Am J Human Biol. 1999;11:457-467.
. Olsen SF, Sorensen JD, Secher NJ, Hede-gaard M, Henriksen TB,
Hansen H, GrantA. Randomized controlled trial of effect offish oil
supplementation on pregnancy du-ration. Lancet.
1992;339:1003-1007.
. Olsen SF, Secher NJ. Low consumption ofseafood in early
pregnancy as a risk forpreterm delivery; prospective cohort
study.BMJ. 2002;324:447-456.
. Bulstra-Ramakers MT, Huisjes HJ, VisserGH. The effects of 3g
eicosapentaenoic aciddaily on recurrence of intrauterine
growthretardation and pregnancy induced hyper-tension. Br J Obstet
Gynaecol. 1995;102:123-126.
. Malcolm CA, McCulloch DL, MontgomeryC, Shepherd A, Weaver LT.
Maternal doco-sahexaenoic acid supplementation duringpregnancy and
visual evoked potential de-velopment in term infants: A double
blind,prospective, randomised trial. Arch DisChild Fetal Neonatal
Ed. 2003;88:F383-F390.
. Olsen SF, Secher NJ, Taber A, Weber T,Walker JJ, Gluud C.
Randomized clinicaltrials of fish oil supplementation in highrisk
pregnancy. BJOG. 2000;107:382-395.
. Onwude JL, Lilford RJ, Hjartardottir H,Staines A, Tuffnell D.
A randomised double
blind placebo controlled trial of fish oil inhigh risk
pregnancy. Br J Obstet Gynaecol.1995;102:95-100.
. Birch EE, Castaneda YS, Wheaton DH,Birch DG, Uauy RD, Hoffman
DR. Visualmaturation of term infants fed long-chainpolyunsaturated
fatty acid-supplementedor control formula for 12 mo. Am J ClinNutr.
2005;81:871-879.
. Hoffman DR, Birch EE, Castenda YS,Fawcett SL, Wheaton DH,
Birch DG, UauyDR. Visual function in breast-fed term in-fants
weaned to formula with or withoutlong-chain polyunsaturates at 4 to
6months: A randomized clinical trial. J Pe-diatr.
2003;142:669-677.
. Heird WC, Lapillonne A. The role o