Embed Size (px)
Citation preview

Portal hypertension
X. RogiersX. Rogiers
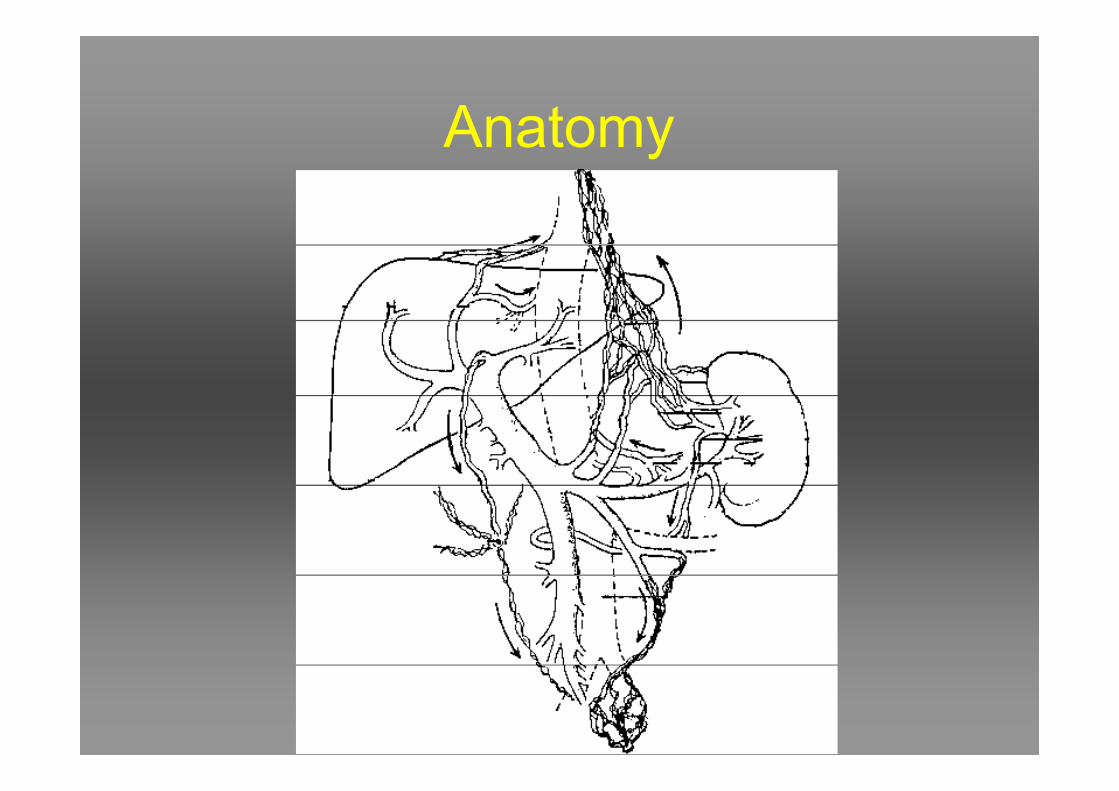
Anatomy

Physiology
• Flow : +- 1000 ml/min
– Variable according to filling status/cardiac
performance of patientperformance of patient
– Interaction portal vs arterial flow
• Pressure : 10-15 cm H2O (7-11 mm Hg)
– “portal hypertension” : > 10 mmHg
Etiology of portal hypertension
• Increased resistance to flow
– Prehepatic
– Hepatic
– Posthepatic– Posthepatic
• Increased portal blood flow
– Arterioportal fistula
– Increased splenic flow

Prehepatic PH
• Congenital atresia or stenosis
• Thrombosis of PV
• Thrombosis of splenic vein (“regional”
portal hypertension)portal hypertension)
• Extrinsic compression / invasion (eg
tumor)

Hepatic PH
• Liver cirrhosis
• Liver fibrosis
• Acute parenchymal disease (eg acute
hepatitis)hepatitis)
• Idiopathic portal hypertension
(hepatoportal sclerosis)
• Shistostomiasis

Posthepatic PH
• Budd-Chiari Syndrome
• Contrictive pericarditis• Contrictive pericarditis
• Tricuspid valve insufficiency


Pathophysiology
• Venous hypertension
– Oedema of bowel wall (eg hypertensive gastritis)
– Ascites
– Splenomegaly => hypersplenism
– (Venous infarction)
• Collateral circulation
– Oesophageal / gastric varices, …
• =>bleeding
– Spontaneous portosystemic shunts
• =>encephalopathy (?)
Surgical treatment of portal
hypertension
• Palliative :
– (TIPSS)
– Surgical portosystemic shunts– Surgical portosystemic shunts
– “Blocking procedures”
– Splenectomy
• Curative :
– Mesenterico-Rex shunt
– Liver transplantation

TIPSS TIPSS
TIPSSTIPSS
•• IndicationsIndications
––Endoscopically not controllable bleedingEndoscopically not controllable bleeding
––Ascites refractory to therapyAscites refractory to therapy
––(Beginning portal vein thrombosis)(Beginning portal vein thrombosis)––(Beginning portal vein thrombosis)(Beginning portal vein thrombosis)
––Bridge to liver transplantationBridge to liver transplantation
•• ContraindicatiesContraindicaties
––Liver failureLiver failure
––EncephalopathyEncephalopathy

TIPSSTIPSS
Recurrent bleedingRecurrent bleeding SurvivalSurvival
Rösch et al., 2001Rösch et al., 2001

Surgical portosystemic shunts
• End-to-side portocaval shunt
• Side-to-side portocaval shunt
• Mesocaval H shunt• Mesocaval H shunt
• Central(proximal) splenorenal shunt
• Distal splenorenal shunt (Warren shunt)


Portocavaler Shunt End-zu-SeitPortocavaler Shunt End-zu-Seit

EndEnd--toto--side / Sideside / Side--toto--sideside
portocaval shuntportocaval shunt

EndEnd--toto--side / sideside / side--toto--side side
Portocaval ShuntPortocaval Shunt
•• Mortality 18 %Mortality 18 %
––depending on liver function !!depending on liver function !!––depending on liver function !!depending on liver function !!
•• Recurrent bleeding 2Recurrent bleeding 2--5 % 5 %
•• Encephalopathy 15Encephalopathy 15--30 %30 %
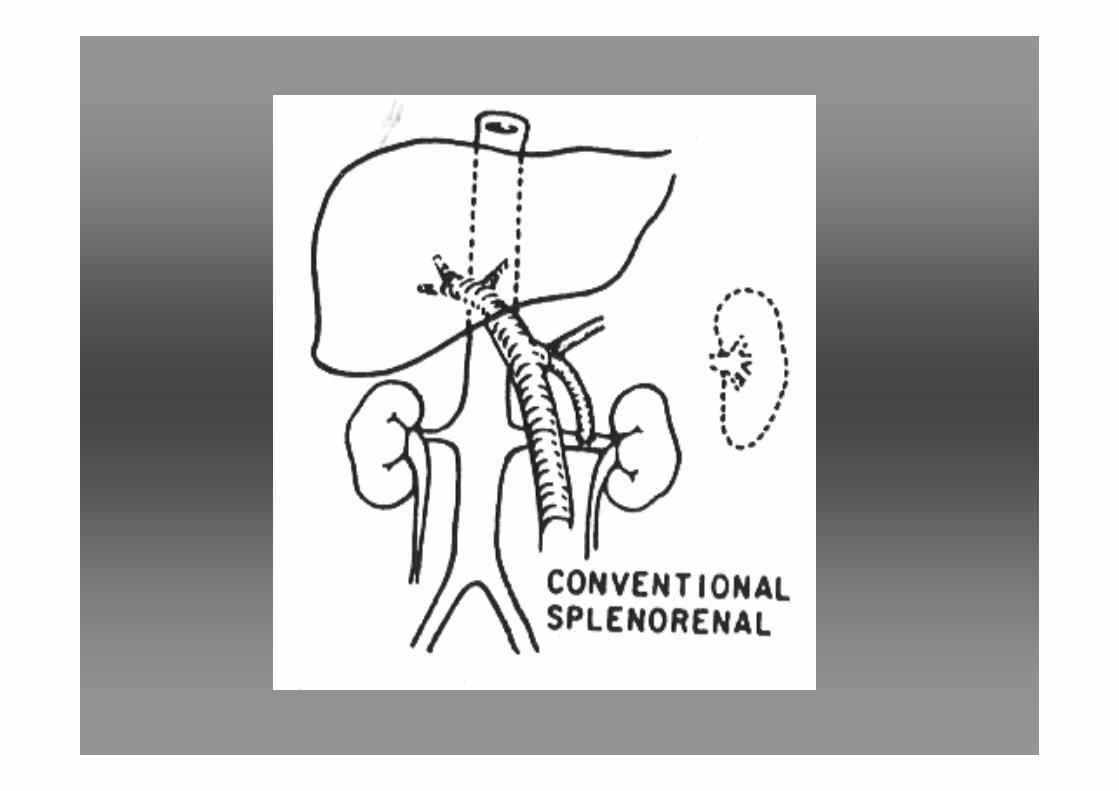

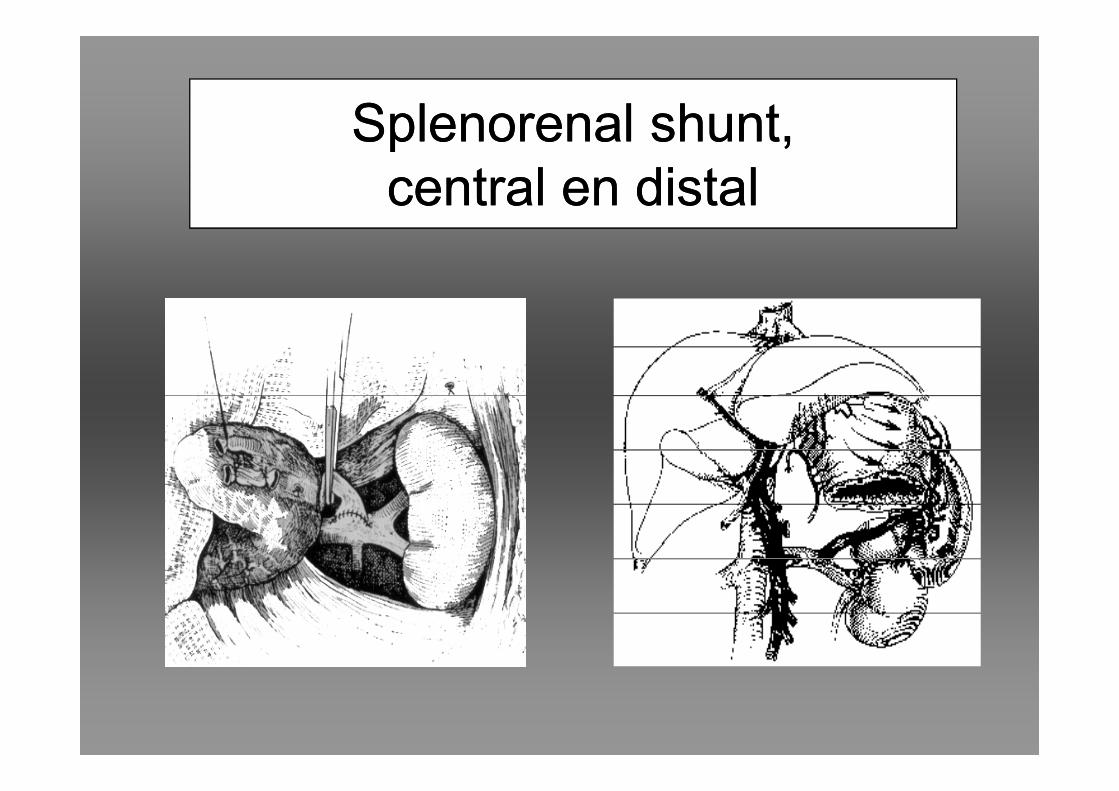
Splenorenal shunt,Splenorenal shunt,
central en distalcentral en distal

Mesocaval shuntMesocaval shunt


Side-to-side splenorenal

Meso-Rex-Shunt

•Decompression
•Maintenance of
physiologic passage
Meso-Rex-Shunt
physiologic passage
•Avoidance of
encephalopathy

“blocking” procedures
• Oesophageal transsection and
reanastomosis
• Sigiura procedure and variants
– Oesophageal transsection– Oesophageal transsection
– Devascularisation of upper two thirds of
stomach
– (splenectomy)

Oesophageal varices
prophylaxis (no previous bleeding)
• Risk factors :– Severe cirrhosis : Child-Pugh C
– PV diameter > 13 mm (ultrasound)
– hypothrombinemia
– Large varices– Large varices
– Red spots
• Treatment:– (Expectant)
– Propranolol (monitor HVPG)
– (endoscopy - band ligation)
De Franchis et al J of Gastroenterology 2006De Franchis et al J of Gastroenterology 2006
Curr Opin gastroenterol 2006; 22(3) : 254Curr Opin gastroenterol 2006; 22(3) : 254--262262
Groszman et al N Eng J Med 2005; 353Groszman et al N Eng J Med 2005; 353
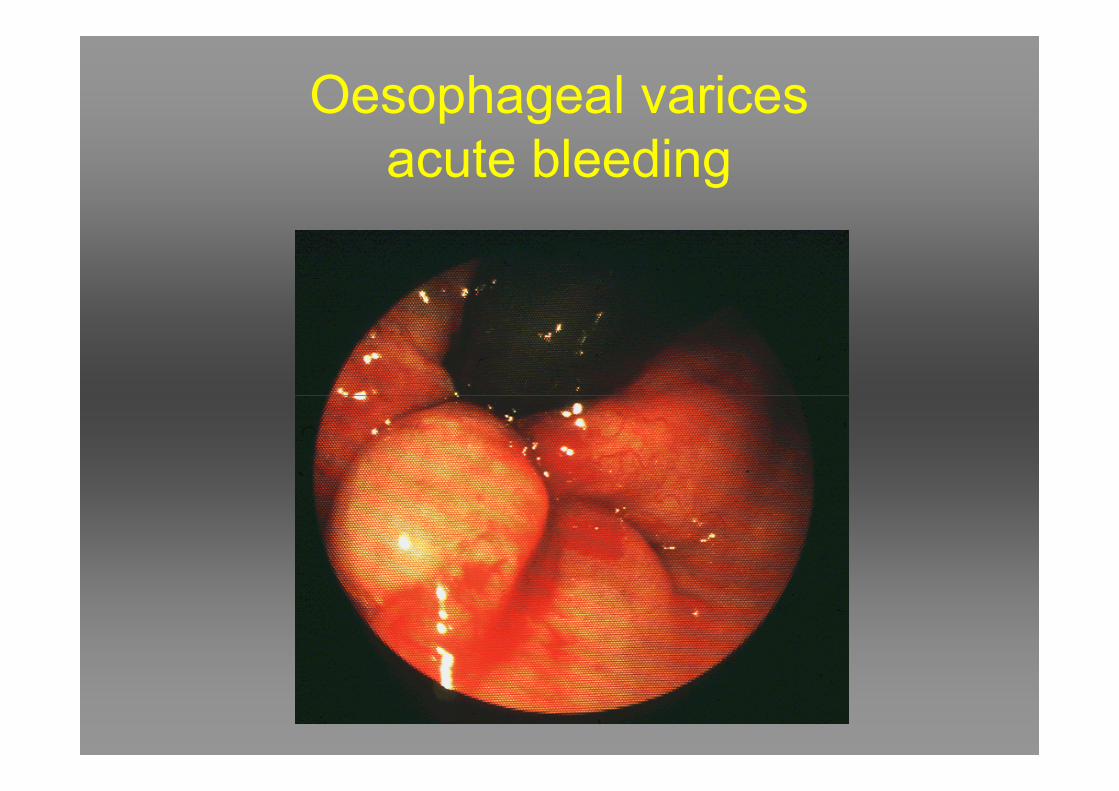
Oesophageal varices
acute bleeding

Oesophageal varices
acute bleeding• Stabilise, protect airway, correct coagulation, prevent encephalopathy, blood volume replacement
• IV infection prophylaxis (17% pos. bloodcultures!)
•• Emergency endoscopyEmergency endoscopy (sclerotherapy, band ligation)
• (Sengstaken type tube only in exceptions)
• Vasopressin/terlipressin
• Octreotide (somatostatin,..)Wright, RikkersJ gastrointest Surg2005; 9(7):992Wright, RikkersJ gastrointest Surg2005; 9(7):992--10051005
Zaman et al Gastroenterol Clin North Am 2005;34(4):623Zaman et al Gastroenterol Clin North Am 2005;34(4):623--4242
Shah et al Am J Gastroenterol 2004; 99(7): 1289Shah et al Am J Gastroenterol 2004; 99(7): 1289--9090

Obliteration Obliteration Band-ligationBand-ligation

•Strictuur 11,8 %
•Bloeding uit necrosen 12,7%
•Strictuur 11,8 %
•Bloeding uit necrosen 12,7%
Complicaties van sclerotherapieComplicaties van sclerotherapie
•Aspiratiepneumonie 6,8 %
•Perforatie 4,3 %
•Aspiratiepneumonie 6,8 %
•Perforatie 4,3 %
Infante-Rivard et al., 1989Infante-Rivard et al., 1989

Oesophageal varices
acute bleedingEndoscopy 80-90 % successfull
Rebleeding 12-40 %
Usually controllable with re-endoscopy
• Emergency TIPSS (Transjugular
intrahepatic portosystemic stent shunt)intrahepatic portosystemic stent shunt)
• Emergency surgical portosystemic shunt
– H-mesocaval shunt
• (Oesophageal transsection)

Oesophageal varices
therapy (previous bleeding = sign of alarm!)
• 70 % chance of rebleeding
• Treatment:
– endoscopy - band ligation/sclerotherapy
– Propranolol– Propranolol
– Surgery
• Transplantation!!!
• Portosystemic shunt
– Selective (distal splenorenal (Warren))
– Mesocaval

ASCITES
Differential diagnosis
• Portal hypertension
• Pancreatic ascites (amylase)
• Malignant ascites (cytology, LDH)• Malignant ascites (cytology, LDH)
• (Primary) bacterial peritonitis (culture,
leucocytes)
ASCITES
Treatment
• Diuretics (spironolactone, lasix)
• Large volume peritoneal taps (cave
albumine : Barcelona protocol!)
• TIPSS• TIPSS
• Portosystemic shunt (side-to-side
portocaval, mesocaval H)
• Peritoneovenous shunt (LeVeen, Denver)
• Liver transplantation

Budd-Chiari Syndrome
• Obstruction of hepatic venous outflow
• Symptoms
• Treatment :
– TIPSS– TIPSS
– (side-to-side portocaval shunt, mesocaval shunt)
– (mesoatrialshunt)
– ((peritoneovenous shunt))
– liver transplantation
– Anticoagulation?

Extrahepatic portal hypertension

AV Fistel Arteria-Vena lienalisAV Fistel Arteria-Vena lienalis

![Portal hypertension: Imaging of portosystemic collateral ...€¦ · portal hypertension[3-5]. Clinically significant portal hypertension is defined as an increase in HVPG to ≥](https://img.pdfslide.us/doc/110x75/5f03e1347e708231d40b3854/portal-hypertension-imaging-of-portosystemic-collateral-portal-hypertension3-5.jpg)