Embed Size (px)
Citation preview

Population HealthResearch Institute
Population Health Research InstituteHamilton Health Sciences/McMaster
UniversityHamilton, Canada
Steroids In caRdiac Surgery (SIRS) Trial
SIRS was funded by grants from the Canadian Institutes of Health Research (CIHR)and the Canadian Network and Centre for Trials Internationally (CANNeCTIN)

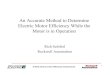
Trial Flow DiagramRandomized (n = 7,507)
Allocated to steroid* (n = 3,755)
Allocated to Placebo (n = 3,752)
Analyzed by intention-to-treat (n = 3,755)
Complete follow-up data (n = 3,754)
Analyzed by intention-to-treat (n = 3,752)
Complete follow-up data (n = 3,751)
Lost to follow-up (n = 1)Did not receive study drug (n =
105)
Lost to follow-up (n = 0)Did not receive study drug (n =
106)
*500 mg IV Methylprednisolone given intra-operatively

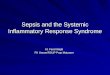
Co-Primary Outcomes (30 days)
30-Day Outcome Steroid Placebo RR (95% CI) p-value
First Co-Primary - Death 155 (4.1) 176 (4.7) 0.88 (0.71-1.09) 0.23Second Co-Primary - Composite death, MI, stroke, new renal failure, respiratory failure
913 (24.3) 875 (23.3) 1.04 (0.96-1.13) 0.31
Components of Composite
MI 508 (13.5) 419 (11.2) 1.21 (1.07-1.37) 0.001Stroke 72 (1.9) 80 (2.1) 0.90 (0.66-1.23) 0.51
New Renal Failure 107 (2.8) 114 (3.0) 0.94 (0.72-1.22) 0.62
Respiratory Failure 343 (9.1) 375 (10.0) 0.91 (0.79-1.05) 0.20

Conclusion
Methylprednisolone does not reduce death or major morbidity at 30 days for high-risk patients undergoing cardiac surgery with the use of cardiopulmonary bypass.
Methylprednisolone increases the risk of early post-operative myocardial infarction, defined by CK-MB biomarker release.

Implications
Methylprednisolone should not be administered prophylactically to high-risk patients undergoing cardiac surgery with the use of cardiopulmonary bypass.
Further work is necessary to understand the mechanism of steroid-driven myocardial infarction.