Embed Size (px)
Citation preview

1
Population Health Management Arrangements: What’s Working and Why?
Joseph F. Damore, FACHE
Vice President, Population Health Management
Premier, Inc.
1
Today’s Agenda & Learning Objectives
• Introduction/Purpose
• Why Population Health Management Now?
– Gain a greater understanding of the changing health care environment in the U.S.
• The Current Population Health Environment
– Gain an understanding of the current population health management environment
• What’s working and Why
– New Care Models
– New Payment Models
• Summary
2

2
INTRODUCTION / PURPOSE
3
The Transformation to Population Health Management
FAD2010
TREND2012
REALITY2015
Population Health Management “The coordination of care delivery across a population to improve clinical and financial outcomes, through disease management, case management and demand management”
McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc.
Population Health “… the health outcomes of a group of individuals, including the distribution of such outcomes within the group.”
Wikipedia, the free encyclopedia
4

3
“WHEN WE ARE NO LONGER ABLE TO CHANGE A SITUATION – WE ARE CHALLENGED TO CHANGE OURSELVES.”
VIKTOR E. FRANKL“MAN’S SEARCH FOR MEANING”
5
WHY POPULATION HEALTH MANAGEMENT?WHY NOW?
6

4
Increasing Market Pressure
Federal State
Employee / Commercial• Current Medicare enrollment is
projected to increase from approximately 54M today, to 85M by 2035
• Dramatic projected growth of all major chronic diseases
• FFS payment cuts
7
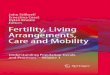
ACO Development Accelerating NationwideNumber of ACOs
50+
30 ‐ 49
20 ‐ 29
10 ‐ 19
5 ‐ 10
3 ‐ 4
0 ‐ 2
Percent of population covered by an ACO
>50%
10 ‐ 15%
6 ‐ 10%
4 ‐ 6%
2 ‐ 4%
0 ‐ 2%
• Nearly 700 public and private ACOs in every state and 7.8M Medicare lives in MSSPs
• Medicare-specific ACOs:– 32 CMMI “Pioneer” participants, program
began 1/1/2012; 9 dropped out with 7 converting to MSSP 1/1/2013; 4 dropped in 2014 with 2 converting to MSSP
– Medicare Shared Savings Program• 4/1/2012: 27 ACOs added
• 7/1/2012: 89 ACOs added
• 1/1/2013: 106 ACOs added
• 1/1/2014: 123 ACOs added
• 1/1/2015: 89 ACOs added
Composition of ACOsPhysician Group
Hospital
InsurerOther
8

5
THE CURRENT POPULATION HEALTHMANAGEMENT ENVIRONMENT
9
Market Developments• Growing movement to population health arrangements
• Multi-owner regional population health entities
• Growth/interest in provider sponsored health plans
• Medicare Shared Savings participation growth (over 400)
• CVS converts from retail Rx to population health
• MSSP Mergers/consolidation/growth
• State Medicaid models– ACO models (Oregon, Alabama, etc.)
– Episode of Care/Bundled Payment models (AR, TN, OH)
– DSRIP model (TX, CA, NJ, NY)
– Commercial Medicaid expansion (AK, IA, UT, PA)
• Commercial Payor developments– Shared Savings models (Aetna, Cigna, Humana, Anthem, UHC, and
multiple BC plans)
– Direct contracting shared savings models (Aetna)
10

6
Market Response• Growth in Consumer Driven Health Plans and commercial shared
saving agreements continuing (2nd wave)
• Emerging application of accountable care principles to Medicaid programs (e.g., Maryland, Alabama, Arkansas, Illinois, NY, Oregon, NC, etc.)
• Significant growth in the number of MSSP applicants for 1/01/15 start date (89 new participants)
• Declining hospital inpatient admissions due to care management programs (e.g., 6% decrease in the Chicago market over the past 48 months)
• Growth in Patient Centered Medical Homes (30,000+ primary care physicians participating to date)
• Implementation of state health insurance exchanges (over 7.5 Million)
• 10 Million newly insured (Uninsured rate dropped from 17.5% to 12.4%)
11
Early Results Indicate the Effectiveness of ACOs
• Medicare costs per capita grew 0.8% in 2012 (while Pioneers grew at 0.3%)
• Physician Group Practice (PGP) Demonstration Project reduces cost of Dual Eligibles by $532 per year
• All 32 initial Pioneer ACOs achieved quality improvements
• 2/3 of Pioneer ACOs achieved cost savings in 2012
• Group Health and Geisinger report findings that team-based medical homes reduced per capita spending 7-8%
• Montefiore achieved $14M in shared savings in 2011, due in large part to a 10% decline in hospital admissions
• Mosaic Life, Hackensack, Banner Health, and WellStar generate significant shared savings in MSSP by reducing cost per capita
• Oregon’s new Medicaid program reports early success (1% decline in per capital costs in first year)
12

7
WHAT’S WORKING AND WHY:BUILDING NEW CARE MODELS
13
Four Stages in the Journey to Population Health Management
1. Preparatory1. Preparatory 2. Transformational2. Transformational 3. Implementation3. Implementation 3. Expansion3. Expansion
• Education• Assessment• Gap analysis• Operational
plan
• Primary care• Patient Centered
Medical Home• Clinical
integration• Care
management• Network
development• Health
informatics
• Defined population
• Payor partner• Post-acute
• Employee health plan
• Commercial arrangement
• Medicare• Medicaid• Employer
contracting• Uninsured
14

8
Integrating New Care Models and New Payment Models
Care Redesign
• Patient-Centered Medical Home• Clinical Integration• Care Management• Post-Acute Care• Electronic Health Record• Data analytics
Care redesign must not outpace changes in payment
Care redesign must not outpace changes in payment
New Payment Arrangements
• Care Transformation Costs• Care Management Payment• Shared Savings• Episodes of Care Payment• Global Payment
Population Health
Transformation
Population Health
Transformation
15
Care Transformation: Creating Alignment/Integration
• Primary Care Network Development
• Physician Led Clinical Integration
• Patient Centered Medical Home
• Care Network Development/Alignment
• Care Management Program– High Risk Population
– Chronic Disease Management
– Care Transitions/Post-acute care
– Episodes of Care
• Health Information Tools– EMR
– HIE / Interface Engine
– Claims Analytics / Predictive Modeling
– Care Management (Evidence-Based)
• Patient Engagement / Satisfaction
• Triple Aim-based Metrics
• Leadership / Cultural Transformation
16

9
Patient Centered Medical Home Model
Patient Centered
Medical Home(PCMH)
Comprehensive Care
Enhanced Access to Delivery System
CoordinatedCare
Team-BasedApproach
DiseaseRegistry
PatientEngagement
PCMH Expected Attributes:• NCQA / other certification• Adoption of standard IT
system• Use of care
coordinators/managers• Focus on team-based
approach to care
Health System Support:• Provide access/support of
IT adoption within PCP office
• Educate and provide training to PCP’s regarding PCMH adoption
• Assist with care redesign• Jointly hire and train care
coordinators/managers • Collaborate across
practices to develop performance based metrics focused on quality, safety, care coordination and costs
17
PCMH – Success Stories• Hill Air Force Base of Utah improved blood sugar control for 77% of their
diabetic population, reduced cost increases by approximately 10%, and improved patient satisfaction to 95%
• CareFirst Blue Cross Blue Shield of Maryland yielded an estimated 15% PMPM savings in the first year and $98 million in savings over two years
• Group Health of Washington reported overall cost savings of $17 PMPM including 29% fewer ER visits and 11% reduction in hospitalizations for ambulatory sensitive conditions
• Oklahoma Medicaid reported $29 PMPM savings
• HealthPartners in Minnesota reported 39% reduction in ER visits, 24% fewer hospitalizations, 40% reduction in readmission rates and 20% reduction in inpatient costs
• United Healthcare (UHC) reported an average 6.2% reduction in cost per capita in four states
• Michigan Blues (BCBS) reported $155M in savings over the first three years of the program. They also estimate, 3.5% higher quality measures, 5.1% higher preventive care measures, $26.35 lower PMPM cost.
18

10
Population-Based Care Management Framework
Case Management
Disease Management
Prevention
Well & Low Risk Members
(Prevention)
Low Risk Members (Prevention and
Disease Management)
Moderate Risk Members (Disease
Management)
High Risk, Chronic, Multiple Disease
States (Episodic Case Management-
Inpatient Clinical Guidelines)
Complex Catastrophic Care(Inpatient - LTC)
End of Life
Increasing Health Risk
Decreasing Health Risk
1 2 3 4 5
Source: Paul H. Keckley, Executive Director, Deloitte Center for Health Solutions, Washington DCPhD, 2007 National Predictive Modeling Summit: The Landscape for Predictive Models
19
Care Management: Target PopulationsComplex Individual Case
Management (40% of cost)
Complex Disease Management –Embedded/Primary Care
Disease Management –Virtual/Telephonic
Wellness/Prevention
2-3% of Population
5-7% of Population
20-25% of Population
100% of Population
20

11
Care Management – Success Stories• Swedish Covenant Hospital of Chicago lowered readmissions of chronically ill
patients from 27% to 16%. The aggressive care management effort included 1,800 follow-up phone calls, 175 home visits, and 88% of patients scheduling an appointment with their physician within 14 days of discharge.
• Princeton Healthcare System decreased hospitalizations amongst their high risk patients by approximately 30% by increasing immediate post-discharge follow-up to 100%, standardizing patient follow-up appointments to be within 7-14 of discharge, and using IT systems to proactively address concerns.
• UCSF Medical Center achieved a 46% decrease (over two years) in 30-day all-cause heart failure readmissions by enhancing patient education, arranging follow-up care, and improving transitions of care amongst their care team.
• Visiting Nurse Service of NY reduced hospitalizations by 54%, readmissions by 24%, and ED visits by 27% for frail elderly patients by improving transitional care.
• Cincinnati Children’s hospital lengthened time between hospital encounters to 100 days for asthma patients by helping families over-come barriers to effective self-care.
Sources: Commonwealth Fund; HealthIT.gov; Swedish Covenant Hospital
21
– LTACH-$42,500
– Inpatient Rehab Facility-$17,500
– Skilled Nursing Facility-$11,500
– Home Health-$5200
Managing the cost of Post-Acute Care: Case Example of Episode of Care/Payment for Post-Acute
22

12
Summary of ACO expenditures
Home health alone could generate over 3x the savings as inpatient expenses
NOTE: Client example; costs not severity adjusted
Expense for ACO Assigned Beneficiaries
All MSSP ACOs
Impact of 5% Cost
Reduction
Impact of Reaching
MSSP Average
Total $11,494 $9,824 $7,308,138 $21,236,584
ERSD $69,541 $65,029 $740,612 $961,103
Inpatient $3,550 $3,200 $2,257,328 $4,458,411
Skilled Nursing $1,088 $891 $692,058 $2,609,422
Home Health $1,664 $527 $1,012,427 $14,462,779
23
WHAT’S WORKING AND WHY:BUILDING NEW PAYMENT ARRANGEMENTS
24

13
Population Health Market Segments
Employee Health Plan
Self-funded Employers
Private Health Plans
Medicaid Program
Medicare Program
Uninsured
Retail Health Insurance
25
Projected spending
Actual spendingShared savingsConfidence interval
ACO Launched
Source: Lewis, Julie. “What Could be Next for Health Reform? The Debate In Washington” Presentation. The Dartmouth Institute for Health Policy & Clinical Practice. 2009-07-02.
The Medicare Shared Savings Model
26

14
• Medicare Shared Savings Program– Held spending $652M below targets
– Earned shared savings over $300M• One ACO in Track 2 overspent target by
$10M and owed shared losses of $4M
– Saved Medicare Trust Funds ≈$345 M
– Improved on 30 of 33 quality measures
– Surpassed other Medicare FFS providers' performance on 17 of the 22 GPRO Web Interface measures
• Pioneer shared savings:– $96M (saved Medicare Trust Fund
≈$41M)
– Showed improvements in 28 of 33 quality measures and experienced average improvements of 14.8% across all quality measures
Medicare ACO program
Performance year results
24%
24%
52%
MSSP PY1 Financial Results
Earned sharedSavings
Generatedsavings but didnot pass MSR
Did notgeneratesavings
48%
13%
26%
13%
Pioneer PY2 Financial Results
Earned sharedsavings
Generated sharedlosses
Did not surpassMSR
Deferedreconciliation
27
Washington
Oregon
California
Nevada
Idaho
Montana
Wyoming
ColoradoUtah
New Mexico
Arizona
Texas
Oklahoma
Kansas
Nebraska
South Dakota
North Dakota Minnesota
Wisconsin
Illinois
Iowa
Missouri
Arkansas
Louisiana
Alabama
Tennessee
Michigan
Pennsylvania
New York
Vermont
Georgia
Florida
Mississippi
Kentucky
South Carolina
North Carolina
MarylandOhio
Delaware
Indiana West Virginia
New JerseyConnecticut
Massachusetts
Maine
Rhode Island
Virginia
New Hampshire
Alaska
Hawaii
As of 8/04/2014
ACOs: 14
Bundled Payment: 3
DSRIP: 8
Only Colorado and Oregon have statewide Medicaid ACO models
28

15
Medicaid ACO Market & ResultsColorado’s Accountable Care Collaborative• Generated gross savings of $44M, returning $6M to
the state after expenses• Has 350K members (roughly ½ of the state’s Medicaid
population),
Utah’s Medicaid ACOs• On track to save the state $2.5B over the
next seven years • Representation of 85% of the state’s
Medicaid population
Oregon’s ACO model • Covers 93% of the state’s Medicaid population• Decreased ED visits by 13% & hospital admissions for
chronic conditions by 18% - 36%• Increase primary care spending by 18%• Expected to save the state $3.0B over the next 5 years
Source: Electronic Health Reporter, June 10, 2014
29
• Rapid movement toward consumer driven health plans and new payment arrangements
• Components of new payment models to IDNs/CINs– Transformational funding– Care management – Episodes of Care– Shared Savings
• Early adopters include the following– Regional Blue Cross plans (MN, MA, IL, HA, etc.)– Commercial Health Plans (Aetna, Cigna, Humana, etc.)
• Partnering with MSSP ACOs– Universal American (34/28 MSSPs)– Walgreens (3)– CVS/Caremark (Part D shared savings model)– Suppliers (Rx)
• Building delivery systems– Highmark purchases seven hospitals/physician practices– Cigna – Primary Care Network (PCMH) – Phoenix– United Healthcare-Monarch physicians group (2,300 physicians) and Optum– Aetna purchases Active Health– DaVita acquires Healthcare Partners and other physician groups
Major Commercial Health Plan Trends
30

16
Chasing Quality Improvements / Inefficiencies across the continuum
• Bundled payment is a reimbursement model that covers multiple health care services within a specific episode of care for an agreed upon amount (e.g., a target price).
• Goal - to improve patient outcomes while reducing the average cost of episodes.
• Results - Bundled payment has shown the potential for the greatest reduction in health care spending according to a study in the New England Journal of Medicine (NEJM).
Bundled Payment / Episodes of Care Overview
Hussey P., et al. New England Journal of Medicine 2009;361:2109-2111
Estimated Cumulative Percentage Changes in National Health Care Expenditures, 2010 through 2019, Given
Implementation of Possible Approaches to Spending Reform.
31
Direct Contracting
11% of employers are engaging in some form of direct contracting with employers, while another 28% expect to do
so within the next 3-5 years (Aon Hewitt, 2014 p. 33)
32

17
• Commercial insurers are experimenting with Bundled Payments• Payors can benefit from a discounted fee arrangement and the chance to
partner with a provider willing to work to improve care delivery to the payor’s beneficiaries
• Commercial bundled payment agreements have the potential to increase volume
Direct Contracting & Commercial Bundles
• Jackson Laboratory joined the Maine Health Management Coalition 6 years ago and reported in October of 2014, maintaining flat healthcare cost since 2007, reducing hospitalization by 43% and halving claims above $50,000
• Aon Hewitt reports in its “2014 Health Care Survey” that 11% of employers are engaging in some sort of direct health contracting program and that they expect this to increase to 28% in the next 3-5 years
33

Population Health Management Arrangements: What’s Working and Why?
Bibliography
Munro, Dan. Forbes. 2012 – The Year in Healthcare Charts. http://www.forbes.com/sites/danmunro/2012/12/30/2012-the-year-in-healthcare-charts/? goback=.gde_700187_member_199832527. December 20, 2012.
Center for Medicare & Medicaid Services Trustees Report 2014. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ReportsTrustFunds/index.html?redirect=/ReportsTrustFunds/. 2014
Kaiser Family Foundation. State Facts and Issue Brief/ “Medicare Advantage Spotlight: Enrollment Market Update”. May 1, 2014
David Feinberg, MD, MBA, president of the UCLA Health System and CEO for the UCLA Hospital System
Przybyciel, Nick. “Aggressive Intervention Helps Chicago Hospital Drastically Lower Number of Patients Readmitted After Treatment”. April 24, 2014
Rupp, Scott. “Some Early Results and Optimism for Medicaid ACOs”. http://electronichealthreporter.com/some-early-results-and-optimism-for-medicaid-acos/. June 10, 2014.
HealthIT.gov. “Dr. Fisch Improves Care Coordination for a High-Risk Population”. April 24, 2014.
Lewis, Julie. “What Could be Next for Health Reform? The Debate In Washington” Presentation. The Dartmouth Institute for Health Policy & Clinical Practice. 2009-07-02.
Frankl, Viktor E. Man’s Search For Meaning.1946
The Commonwealth Fund. Measuring Progress Toward Accountable Care. http://www.commonwealthfund.org/publications/fund-reports/2012/dec/measuring-accountable-care. December, 2012
Health Affairs. ACO Results: What We Know So Far. http://healthaffairs.org/blog/2014/05/30/aco-results-what-we-know-so-far/. May 30, 2014
Health Affairs. First National Survey Of ACOs Finds That Physicians Are Playing Strong Leadership And Ownership Roles. http://content.healthaffairs.org/content/33/6/964.full.pdf+html. 2014
CMS.gov. Center for Medicare & Medicaid Services • “Press Release: Pioneer Accountable Care Organizations succeed in improving care, lowering costs”.
July 16, 2013 • “Program News and Announcements”. December 22, 2014 • CMS, Office of the Actuary. Healthcare Spending and the Medicare Program MEDPAC. June, 2013

The Commonwealth Fund. “Reducing Heart Failure Readmissions: The Story of UCSF Medical Center” http://www.commonwealthfund.org/publications/newsletters/the-commonwealth-fund-connection/2012/nov/november-19-2012/recent-releases/reducing-heart-failure-readmissions. November 19, 2012 United Health Group: Advancing Primary Care Delivery. http://www.unitedhealthgroup.com/~/media/UHG/PDF/2014/UNH-Primary-Care-Report-Advancing-Primary-Care-Delivery.ashx. September, 2014
The Commonwealth Fund. Accountable Care Strategies: Lessons from the Premier Health Care Alliance’s Accountable Care Collaborative. http://www.commonwealthfund.org/publications/fund-reports/2012/aug/accountable-care-strategies. August, 2012
Annals of Family Medicine. Strategies for Achieving Whole-Practice Engagement and Buy-In to the Patient Centered Medical Home. http://www.annfammed.org/content/12/1/37.full.pdf+html. January, 2014
Annals of Family Medicine. Medical Home Transformation in Pediatric Primary Care – What Drives Change? http://www.annfammed.org/content/11/Suppl_1/S90.full.pdf+html. 2013
Brookings. Year One Results from Medicare Shared Savings Program: What it Means Going Forward. http://www.brookings.edu/blogs/up-front/posts/2014/02/07-results-medicare-shared-savings-program-kocot-mostashari. February 7, 2014
AJMC.com Managed Markets Network. ACO Contracting With Private and Public Payers: A Baseline Comparative Analysis. http://www.ajmc.com/publications/issue/2014/2014-vol20-n12/aco-contracting-with-private-and-public-payers-a-baseline-comparative-analysis. December 12, 2014
Commonwealth Fund. Montefiore Medical Center: Integrated Care Delivery for Vulnerable Populations. http://www.commonwealthfund.org/publications/case-studies/2010/oct/montefiore-medical-center. October, 19, 2010
Paquette, Danielle. The Washington Post. The way we pay for health care is broken. A CEO describes how. http://www.washingtonpost.com/news/storyline/wp/2014/11/20/a-ceo-describes-how-our-health-care-payment-system-is-broken/. November 20, 2014
Gamble, Molly. ACO Manifesto: 50 Things to Know About Accountable Care Organizations. http://www.beckershospitalreview.com/accountable-care-organizations/aco-manifesto-50-things-to-know-about-accountable-care-organizations.html. September 3, 2013
The New England Journal of Medicine. Changes in Patients' Experiences in Medicare Accountable Care Organizations. http://www.nejm.org/doi/full/10.1056/NEJMsa1406552. October 30, 2014
The New England Journal of Medicine. Transforming Specialty Practice – The Patient Centered Medical Neighborhood. http://www.nejm.org/doi/full/10.1056/NEJMp1315416. April 10, 2014
The New England Journal of Medicine. Post-acute Care Reform – Beyond the ACA. http://www.nejm.org/doi/full/10.1056/NEJMp1315350. February 20, 2014

Brino, Anthony. Healthcare Payer News. State Medicaid ACO program sees double year-over-year savings. http://www.healthcarepayernews.com/content/state-medicaid-aco-program-sees-double-year-over-year-savings. November 6, 2013
Blue Cross Blue Shield of Michigan. Blue Cross Blue Shield of Michigan saves an estimated $155 million over three years from Patient-Centered Medical Home program. http://www.bcbsm.com/blue-cross-blue-shield-of-michigan-news/news-releases/2013/july-2013/bcbsm-saves-155-million-pcmh.html. July 8, 2013
Hancock, Jay. Kaiser Health News. New Insurer-Hospital ACO Touts Early Success. http://kaiserhealthnews.org/news/new-insurer-hospital-aco-touts-early-success/. March 8, 2012
Molpus, Jim. Health Leaders Media. Norton, Humana Commercial ACO Notches Cost Savings. http://www.healthleadersmedia.com/page-1/LED-269502/Norton-Humana-Commercial-ACO-Notches-Cost-Savings. August 8, 2011
The Commonwealth Fund. Creating Connections: An Early Look at the Integration of Behavioral Health and Primary Care in Accountable Care Organizations. http://www.commonwealthfund.org/publications/fund-reports/2014/dec/creating-connections. August 28, 2014
The Commonwealth Fund. Few ACOs Pursue Innovative Models That Integrate Care for Mental Illness and Substance Abuse with Primary Care. http://www.commonwealthfund.org/publications/in-the-literature/2014/oct/acos-pursue-integrated-model. October 7, 2014.
The Commonwealth Fund. Gaining Ground: Care Management Programs to Reduce Hospital Admissions and Readmissions Among Chronically Ill and Vulnerable Patients. http://www.commonwealthfund.org/publications/case-studies/2013/jan/care-transitions-synthesis. January 23, 2013.
Adamopoulos, Helen. Becker’s Hospital CFO. 3 Key Observations of Medicare Advantage Cuts in 2015. http://www.beckershospitalreview.com/finance/3-key-observations-on-medicare-advantage-cuts-in-2015.html. March 13, 2014.
Jacobson, Gretchen. Kaiser Family Foundation. Medicare Advantage 2015 Data Spotlight: Overview of Plan Changes. http://kff.org/medicare/issue-brief/medicare-advantage-2015-data-spotlight-overview-of-plan-changes/. December 10, 2014