Embed Size (px)
Citation preview

•Poor adherence to medication results in $300 billion of unnecessary health care (Vlasnik et al. 2005)
•Medication discontinuation and subsequent failure of treatment results in 10% of hospitalizations (Harrold, 2008).
•It is estimated that ½ of all patients skip or discontinue long term medical therapy for chronic illnesses and 1 out of 5 patients do not pick up filled prescriptions (Reginster, 2006).
•Studies have determined specific factors that effect adherence such as the dosing regimen, side effects, cost, and pill burden. Greater case management that increases patient knowledge and the understanding of patient concerns has been effective in increasing medication adherence (Vlasnik et al. 2005).
•Although medications for rheumatic conditions are often directly related to greater mobility and pain relief, patients often discontinue long term therapy (Harrold, 2008)
•For patients with rheumatic conditions, the effect of drug class and safety perception on medication adherence is not known. Such knowledge could increase the rate of adherence and minimize the loss of billions of dollars while improving the quality of life of patients with chronic rheumatic diseases.
•Determine the medication adherence of 8 specific drug classes
•Determine If safety perception for prescribed drug class effects medication adherence
•Determine if there is a specific motivation to discontinue medication
The Effect of Drug Class and Safety Perception on the Medication Adherence of Rheumatology Patients
Kathryn C. Fischer, Department of Biological Sciences York College of PennsylvaniaMethods
•Immunosuppressant drugs were discontinued the most. Pain Relievers and Corticosteroids were discontinued the least. However, only 27 of 100 patients described discontinuing their medication.
•Patients who felt their prescribed medication was dangerous discontinued therapy 100% of the time. However, 75% of patients felt their medication was safe or moderately safe.
•Similar to past medication adherence studies, the greatest motivation for discontinuing long term medical therapy for patients at AACR is side effects (Vlasnik et al. 2005).
•It is now known that a significant amount of patients who discontinue prescribed medications at AACR feel the risks of side effects outweigh the benefits of continuing therapy. Factors influencing adherence such as safety perception and motivation to discontinue can be addressed in order to intervene in patients who have concerns about their long term therapy.
•Further research involving a greater quantity of patients would increase the significance of discontinuation, both within specific drug classes and due to patient safety perception.
LITERATURE CITEDHarrold, Leslie R., and Susan E. Andrade. "Medication Adherence of Patients with Selected Rheumatic Conditions: A Systematic Review of Literature." Seminars in Arthritis and Rheumatism (2008).
Klippel, John H., and Patience H. White, eds. Primer on the Rheumatic Diseases. New York: Springer, 2007.
Reginster, Jean-Yves. "Adherence and persistence: Impact on outcomes and health care resources." Bone 38 (2006): 18-21.
Vlasnik, Jon J., Sherry L. Aliotta, and Bonnie DeLor. "Medication Adherence Factors Influencing Compliance with Prescribed Medication Plans." The Case Manager 16 (2005): 47-51.
Whitley, Heather P., Joli D. Fermo, Kelly Ragucci, and Eleanor C. Chumney. "Assessment of patient knowledge of diabetic goals, self-reported medication adherence, and goal attainment." Pharmacy Practice 4 (2006): 183-90.
Results
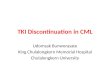
A survey was developed regarding patient disorder and medication,
safety perception, media observations, personal conversations, medication discontinuation,
and motivation to discontinue.
Surveys were distributed to 110 patients at Advanced Arthritis Care and Research
in Scottsdale, Arizona over 21 days prior to examination before the physician entered the room.
Completed surveys were delivered directly to the receptionist after appointment. New patients were excluded from the study
and 10 patients declined to participate.
Objective Percentage of Discontinuation
Within Drug Classes
0
10
20
30
Figure 2. Percentage of medication discontinuation for allpatients surveyed. Chi-Square statistical analysis provided a p
value of 0.120 which fails to reject the null hypothesis. This showsno significant relationship between drug class and
discontinuation.
Drug Class
Perc
en
tag
e o
f P
ati
en
ts
Figure 1. Copy of survey distributed to patients at Advanced Arthritis Care and Research in Scottsdale, Arizona.
Patient Saftey Perceptionfor Drug Class Perscribed
0
10
20
30
40
Figure 3. Analysis of patient safety perception for all patientssurveyed. Chi-Square statistical analysis provied the p value ofless than 0.0001 which supports rejection of the null hypothesis.
This supports a significant difference in perception of safety withinthe patient population.
Safety Perception
Perc
en
tag
e o
f P
ati
en
ts
Patient Motivation for Medication Discontinuation
0
10
20
30
40
50
Figure 5. Analysis of patient motivation and medicationdiscontinuation. A non-parametric Chi-Square test resulted in ap value of 0.004 which rejects the null hypothesis. This supportsa significant difference in motivation of skipping or discontinuing
medication.
Motivation
Perc
en
tag
e o
f P
ati
en
ts
Data was compiled and statistical analysis was performed using SPSS
Percentage of DiscontinuationWithin Saftey Perception Categories
0
20
40
60
80
100
Figure 4. Percentage of patients who discontinued medicationwithin each saftey perception category. Chi-square statistical
analysis provided a p value of 0.164 which fails to reject the nullhypothesis. This shows no significant difference in saftey
perception and discontinuation of drug prescribed.
Safety Perception
Perc
en
tag
e o
f P
ati
en
ts
ACKNOWLEDGEMENT • I would like to thank Dr. Warren C. Rizzo of Advanced Arthritis Care and Research
in Scottsdale, Arizona for my internship experience and guidance.• Also thanks to mentors Dr. Carolyn Mathur and Dr. Joshua Landau for their
guidance.• And a special thanks to Peter and Alison Fischer for their ever present inspiration
to better the lives of individuals with rheumatic diseases.
ConclusionIntroduction