Embed Size (px)
DESCRIPTION
Polymorphisms in the promoter regions of the matrix metalloproteinases-7, -9 and the risk of endometriosis and adenomyosis
Citation preview

Molecular Human Reproduction Vol.12, No.1 pp. 35–39, 2006Advance Access publication February 2, 2006 doi:10.1093/molehr/gal002
© The Author 2006. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For
Permissions, please email: [email protected] 35
Polymorphisms in the promoter regions of the matrix metalloproteinases-7, -9 and the risk of endometriosis and adenomyosis in China
Kang Shan1, Zuo Lian-Fu2, Du Hui1, Guo Wei2, Wang Na2, Jin Xia1 and Li Yan2,3
1Department of Obstetrics and Gynaecology, Hebei Medical University, Fourth Hospital and 2Department of Molecular Biology, Hebei Cancer Institute, Shijiazhuang, China3To whom correspondence should be addressed: Hebei Cancer Institute, Hebei Medical University, Jiankanglu 12, Shijiazhuang 050011, China. E-mail: [email protected]
Matrix metalloproteinases (MMPs) may contribute to the development of endometriosis. The aim of this study was to assess theeffects of the polymorphisms in the promoters of MMP-7 (181A/G) and MMP-9 (1562C/T) on the risk of occurrence of endometri-osis and adenomyosis. We genotyped 219 patients (143 women with endometriosis, 76 women with adenomyosis) and 160 controlwomen in North China. There was a significant difference in frequency of the MMP-7 genotype between endometriosis andcontrols (P = 0.01) and also between adenomyosis and controls (P = 0.01). The frequency of the G allele in two groups of patients(7.3 and 7.9%) was significantly higher than in the controls (2.8%) (P = 0.01 and 0.01, respectively). Compared to the A/A geno-type, the genotype with the -181G allele showed a significantly increased susceptibility to both diseases, with adjusted odds ratio of2.62 [95% confidence interval (CI) = 1.17–5.87] for endometriosis and 3.14 (95% CI = 1.26–7.81) for adenomyosis. However, theoverall genotype and allelotype distribution of the MMP-9 in the two case groups were not different from that of controls. We con-clude that MMP-7–181A/G polymorphism has a potential to be a susceptibility factor for endometriosis and adenomyosis whileMMP-9–1562C/T polymorphism may not provide a useful marker to predict susceptibility to endometriosis and adenomyosis, atleast in women from North China.
Key words: adenomyosis/endometriosis/matrix metalloproteinase-7/matrix metalloproteinase-9/single nucleotide polymorphism
IntroductionEndometriosis is a common gynaecological disease, characterized his-tologically by the presence of endometrial glands and stroma outsidethe uterine cavity, which plays an importance role in female infertility.Adenomyosis has some similarities to endometriosis, being character-ized by the presence of ectopic endometrium within the myometrium.The two diseases are invasive but benign diseases that require remod-elling of the extracellular matrix (ECM) for ectopic implantation ofendometrium.
Matrix metalloproteinases (MMPs) are an important group of zincenzymes that are responsible for degradation of ECM componentssuch as collagen and proteoglycans in normal embryogenesis andremodelling and in many disease processes such as carcinoma inva-sion. The over-expression of MMPs has been demonstrated in a vari-ety of cancers and is correlated with invasion and tumour metastasis,for example in oral cancer (Jordan et al., 2004), colorectal cancer(Adachi et al., 1999), esophageal squamous cell cancinomas (Ohashiet al., 2000) and endometrial cancer (Aglund et al., 2004). Like carci-noma, endometriosis and adenomyosis have the unique characteristicsof invasion and metastasis, though pathologically, they are benign. Pre-vious studies have shown that many MMPs were more highly expressedin ectopic endometrium than in eutopic endometrium in women withendometriosis. Thus the over-expression of MMPs may contribute tothe development of endometriosis (Kokorine et al., 1997; Cox et al.,2001; Szamatowicz et al., 2002; Gilabert-Estelles et al., 2003).
There are several regulating mechanisms that may influence theactivities of MMPs such as regulation of transcription, activation oflatent MMPs, inhibition of MMP function by tissue inhibitors ofmetalloproteinases (TIMPs) and regulation by ovarian steroid hor-mones and so on. Of these mechanisms, the most important may betranscriptional regulation; since most MMPs genes are expressedonly when physiologically active or pathological tissue remodellingtakes place. There is growing evidence to indicate that naturalsequence variations in promoters of the MMPs genes may result indifferent expression of MMPs in different individuals (Ye, 2000).These polymorphisms have been associated with susceptibility tosome diseases including acute myocardial infarction (Nojiri et al.,2003), rheumatoid arthritis (Mattey et al., 2004), multiple sclerosis(Fiotti et al., 2004) and cancers (Yu et al., 2002; Zhang et al., 2004;Fang et al., 2005).
We hypothesize that increased expression of MMPs gene polymor-phisms might promote the susceptibility to endometriosis and adeno-myosis. We have previously studied the association between promoterpolymorphisms in MMP-1 and MMP-3 genes and patient susceptibil-ity to endometriosis (Kang et al., 2005) and found that the MMP-1promoter single nucleotide polymorphism (SNP) and the MMP 2G/6Ahaplotype may modify susceptibility to endometriosis. In the presentstudy, we investigated the role of MMP-7 (181A/G) and MMP-9(1562C/T) in the development of endometriosis and adenomyosis totest the above hypothesis.

K.Shan et al.
36
Materials and methods
Study participantsBlood was obtained from the following three groups and DNA was extractedfor genotyping: (i) healthy female blood donors aged 25–50 years (n = 160)and (ii) the endometriosis cases were inpatients for endometriosis in the FourthHospital, Hebei Medical University between 2001 and 2004 (n = 143). Thepatients were all clinically, endoscopically and histologically confirmed. Noneof the endometriosis patients had taken any hormonal treatment. All patientswere in endometriosis stages III and IV. Patients were staged according to therevised American Fertility Society (AFS, 1985) classification. (iii) The adeno-myosis cases were inpatients for adenomyosis in the same hospital between2002 and 2004 (n = 76). None of these patients had taken any hormonal treat-ment. General information of all patients was recorded in detail in the medicalrecords. The endometriosis patients who also had adenomyosis were excludedfrom the study.
The control group consisted of women of reproductive age without anymalignant disease confirmed by surgical exploration at voluntary abortion,cesarean section or pathologically confirmed after hysterectomy performed fordysfunctional uterine bleeding. The general information of the healthy controlswas extracted from their medical records. The study was approved by the Eth-ics Committee of Hebei Obstetrics and Gynecology Institute and informedconsent was obtained from all recruited subjects.
DNA extractionVenous blood (5 ml) was drawn from each subject into Vacutainer tubes con-taining EDTA and stored at 4°C. Genomic DNA was extracted within oneweek after sampling using proteinase K (Merck, Darmstadt, Germany) diges-tion followed by a salting out procedure according to the method of Milleret al. (1988).
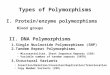
MMP-7 SNP genotypingThe MMP-7–181A/G genotypes were determined by PCR–restriction fragmentlength polymorphism (PCR–RFLP) assay. The primers for amplifying theMMP-7 fragment were 5′-TGGTACCATAATGTCCTGAATG-3′ (forward)and 5′-TCGTTATTGGCAGGAAGCACACAATGAATT-3′ (backward) (Jormsjoet al., 2001). The PCR was performed in a 20 μl volume containing 100 ng ofDNA template, 2.0 μl of 10× PCR buffer, 1.5 mM of MgCl2, 1 U of Taq-DNA-polymerase (BioDev-Tech, Beijing, China), 200 μM of dNTPs and 200 nM ofeach primer. The PCR cycling conditions were 5 min at 94°C followed by 35cycles of 30 s at 94°C, 30 s at 65°C and 30 s at 72°C and with a final step at72°C for 5 min to allow for the complete extension of all PCR fragments. An8 μl aliquot of PCR product was subjected to digestion at 37°C overnight in a10 μl reaction containing 10 U of EcoR I (TakaRa Biotechnology Co. Ltd, Dalian,China) and 1× reaction buffer. After digestion, the products were separated ona 4% agarose gel stained with ethidium bromide. As a result, the -181G alleleswere represented by DNA bands with size at 120 bp and 30 bp, the -181A alle-les were represented by a DNA band with size at 150 bp, whereas the heterozy-gotes displayed a combination of both alleles (150, 120 and 30 bp) (Figure 1).
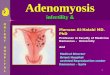
MMP-9 SNP genotypingThe MMP-9–1562C/T genotypes were determined by PCR–RFLP assay. Theprimers used for amplifying the MMP-9 SNP were 5′-GCCTGGCACATAG-TAGGCCC-3′ (forward) and 5′-CTTCCTAGCCAGCCGGCATC-3′ (reverse)(Zhang et al., 1999). The PCR reactions were performed in a 25 μl volumecontaining 100 ng of DNA template, 2.5 μl of 10× PCR buffer, 1.5 mM ofMgCl2, 1 U of Taq-DNA-polymerase (BioDev-Tech), 200 μM of dNTPs and200 nM of forward and reverse primer. The PCR cycling conditions were5 min at 94°C followed by 35 cycles of 30 s at 94°C, 30 s at 57°C and 30 s at72°C, with a final step at 72°C for 5 min to allow for the complete extension ofall PCR fragments. An 8 μl aliquot of PCR product was digested overnight at37°C in a 10 μl reaction containing 10 U of SphI enzyme (TakaRa BiotechnologyCo. Ltd). After overnight digestion, the products were subjected to electro-phoresis on a 2% agarose gel stained with ethidium bromide. The MMP-9–1562 T allele is digested by SphI, yielding fragments of 247 and 188 bp whilethe -1562 C allele is not cleaved by SphI and keeps the original PCR product(435 bp), the heterozygotes displayed a combination of both alleles (435, 247and 188 bp) (Figure 2).
For a negative control, distilled water was used instead of DNA in the reac-tion system for each panel of PCR. The PCR reactions of 10% of the sampleswere run in duplicate for quality control.
Statistical analysisStatistical analysis was performed using the SPSS10.0 software package(SPSS Company, Chicago, IL, USA). Hardy–Weinberg analysis was per-formed to compare the observed and expected genotype frequencies using thechi-square test. Comparison of the MMP-7 and MMP-9 genotype distributionin the study groups was performed by means of two-sided contingency tablesusing chi-square test. The odds ratio (OR) and 95% confidence interval (CI)were calculated using an unconditional logistic regression model. A probabil-ity level of 5% was considered significant.
ResultsAssociation of MMP-7 SNP with susceptibility to endometriosis and adenomyosisThe distribution of the MMP-7 genotypes in controls did not signifi-cantly deviate from that expected for a Hardy–Weinberg equilibrium(c2 = 0.00, P = 1.00). The frequency of the G allele among endometri-osis and adenomyosis patients (7.3 and 7.9%) was significantly higherthan in the healthy controls (2.8%) (c2 = 6.59 and 6.26, P = 0.01 and0.01, respectively). The frequencies of the A/A and A/G + G/G geno-types in endometriosis and adenomyosis patients were significantlydifferent from those in control (c2 = 6.10 and 6.57, P = 0.01 and 0.01,Table I). Compared with the A/A genotype, the A/G + G/G genotypesignificantly modified the risk of developing endometriosis and aden-omyosis. The odds ratios were 2.62 (95% CI = 1.17–5.87) and 3.14(95% CI = 1.26–7.81) (Table II).
Figure 1. MMP-7 genotyping by PCR–RFLP analysis followed by separationon 4% agarose gel as described in text. Lane 1, 100 bp ladder; lanes 2 and 3, A/A;lanes 4 and 5= A/G; lane 6, G/G.
Figure 2. MMP-9 genotyping by PCR–RFLP analysis followed by separationon 2% agarose gel as described in text. Lane 1, 100 bp ladder; lanes 2 and 6,C/ ; lanes 3 and 5, C/C; lanes 4 and 7, T/T.

Polymorphisms in the promoter regions
37
Association of MMP-9 SNP with susceptibility to endometriosis and adenomyosisThe distribution of the MMP-9 genotypes in controls was consistentwith the Hardy–Weinberg equilibrium (c2 = 1.08, P = 0.58). The fre-quencies of the C allele among endometriosis, adenomyosis patientsand healthy controls were 88.8, 89.5 and 91.9%, respectively. The fre-quencies of the T allele among endometriosis patients, adenomyosispatients and healthy controls were 11.2, 10.5 and 8.1%, respectively.No significant difference in the MMP-9 allele distribution was shownbetween the endometriosis, adenomyosis patients and controls (c2 = 1.64and 0.73, P = 0.20 and 0.39, Table I). There was no significant differ-ence in genotype (C/C and C/T + T/T) distribution between endometri-osis, adenomyosis patients and healthy women (c2 = 1.46 and 0.81,P = 0.23 and 0.37). Compared with the C/C genotype, the C/T + T/Tgenotype did not significantly modify the risk of developing endome-triosis. The adjusted odds ratio was 1.55 (95% CI = 0.89–2.72)and 1.37 (95% CI = 0.69–2.75) (Table II).
DiscussionThis study shows that the MMP-7–181A/G genotype may be a poten-tially indicative factor for susceptibility to endometriosis and adenom-yosis, that is, genotypes with the G allele significantly increase the riskof development of endometriosis and adenomyosis. However, theMMP-9–1562C/T polymorphism may not be associated with the
occurrence of endometriosis and adenomyosis. To the best of ourknowledge, this is the first study to look for an association betweenpolymorphisms of MMP-7 and MMP-9 and the risk of development ofendometriosis and adenomyosis.
MMP-7 (also known as matrilysin or PUMP-1) is one of the small-est members of the MMP family described to date. Unlike otherMMPs, which are expressed in stromal cell, MMP-7 is an epithelial-specific MMP (Wilson and Matrisian, 1996). The over-expression ofMMP-7 has been documented in several cancer types as correlatingwith the potential for invasive cancer (Kioi et al., 2003; Leeman et al.,2003; Ajisaka et al., 2004). In the uterus, MMP-7 mRNA has not beendetected in normal, secretory-phase endometrium, but strong expres-sion has been observed in eutopic or ectopic endometrium removedduring the secretory phase from a patient with endometriosis (Bruneret al., 2002).
An A to G substitution at position -181 (-181A/G) is reported toinfluence the binding of nuclear proteins in the promoter region ofMMP-7, and the G allele was associated with higher basal transcrip-tional activity (Birkedal-Hansen et al., 1993). A study of colorectalcarcinoma patients suggested that the presence of the G allele in theMMP-7 gene promoter sequence may be a facilitating factor for can-cer growth, lymph node invasion and metastasis (Ghilardi et al.,2003). Our findings are consistent with this, suggesting that the Gallele of MMP-7 may enhance risk of endometriosis and adenomyosis.However, the G allele frequencies of controls in our study was lowerthan in the Italian population (2.8 versus 40.1%) (Ghilardi et al.,2003). In a previous study we found the same result that G allele ofMMP-7 may be associated with esophageal squamous cell carcinoma,gastric cardiac adenocarcinoma and non-small cell lung carcinoma(NSCLC) (Zhang et al., 2005).
The increased promoter activity of the -181G allele may induce ele-vation of the MMP-7 mRNA and in turn increase protein expression(Jormsjo et al., 2001). MMP-7 can not only degrade elastin, prote-oglycans, fibronectin and type IV collagen (Quantin et al., 1989), butalso cleaves non-matrix substrates from the cell surface, includingE-cadherin (Noe et al., 2001), pro-tumour necrosis factor a (TNF-α)(Haro et al., 2000) and Fas ligand (Powell et al., 1999). E-cadherin isan important cell adhesion protein that forms a key part of the adher-ent junctions between epithelial cells (Gumbiner, 1996). The reduc-tion of E-cadherin in ectopic endometrium results in decreasedadhesion between the epithelial cell and stromal cell and between theendometrial epithelial cells. Consequently, it is easier for shed epithe-lial cells from the endometrium to relocate and form ectopic lesions(Scotti et al., 2000; Poncelet et al., 2002). Additionally, FasL has animportant role in apoptosis. The over-expression of MMP-7 could res-ult in the shedding of FasL from the cell surface and the generation ofsoluble FasL with less potent activity in terms of triggering apoptosisby cross-linking with Fas through the recently described TNFRSF6/
Table I. Distribution of genotypes and alleles of a single nucleotide polymorphism in MMP-7 and MMP-9 genes
Groups Control[n = 160 (%)]
Endometriosis [n = 143 (%)]
P value Adenomyosis [n = 76 (%)]
P value
MMP-7 genotype
A/A 151 (94.4) 123 (86.0) 0.01 64 (84.2) 0.01A/G 9 (5.6) 19 (13.3) 12 (15.8)G/G 0 (0) 1 (0.7) 0 (0)
MMP-7allelotype
A 311 (97.2) 265 (92.7) 0.01 140 (92.1) 0.01G 9 (2.8) 21 (7.3) 12 (7.9)
MMP-9 genotype
C/C 134 (83.8) 112 (78.3) 0.23 60 (79.0) 0.37C/T 26 (16.2) 30 (21) 15 (19.7)T/T 0 (0) 1 (0.7) 1 (1.3)
MMP-9 allelotype
C 294 (91.9) 254 (88.8) 0.20 136 (89.5) 0.39T 26 (8.1) 32 (11.2) 16 (10.5)
Table II. Association of two single nucleotide polymorphisms with the risk of development of endometriosis and adenomyosis
*Odds ratio of the A/G + G/G genotype against the A/A genotype in endometriosis.†Odds ratio of the A/G + G/G genotype against the A/A genotype in adenomyosis.‡Odds ratio of the C/T + T/T genotype against the C/C genotype in endometriosis.§Odds ratio of the C/T + T/T genotype against the C/C genotype in adenomyosis.
Gene Genotype Controls (n) Endometriosis Adenomyosis
n aOR (95% CI) n aOR(95% CI)
MMP-7 A/A 151 123 64A/G + G/G 9 20 2.62 (1.17–5.87)* 12 3.14 (1.26–7.81)†
MMP-9 C/C 134 112 60C/T + T/T 26 31 1.55 (0.89–2.72)‡ 16 1.37 (0.69–2.75)§

K.Shan et al.
38
TNFSF6 [Fas/Fas ligand (FasL)] pathway (Schneider et al., 1998;Powell et al., 1999; Poulaki et al., 2001). A less effective FasL path-way would more readily enable cancer cells to evade apoptosis andthus promote tumour survival (Igney and Krammer, 2002). Webelieve that a similar mechanism may explain the survival of endome-trial cells in the peritoneal cavity of women with endometriosis.
MMP-9, also known as gelatinase B or 92-kDa type IV collagenase,has a broad substrate specificity, being particularly active againstgelatins and type IV collagen (Birkedal-Hansen et al., 1993). It alsopossesses proteolytic activity against proteoglycan core protein andelastin. The MMP-9 in ectopic endometrium was significantly higherthan in eutopic endometrium (Chung et al., 2001; Yu et al., 2003).This increased expression may be one of the reasons for the invasiveproperties of the endometrium, resulting in the development ofendometriosis (Chung et al., 2001).
A transition of C to T at the 1562 base pair position upstream of thetranscription initiation site (C-1562T) of MMP-9 has been reported.In vitro studies have demonstrated that the -1562T MMP-9 alleles areassociated with increased promoter activity. Transient transfectionexperiments showed that the -1562T MMP-9 allele had a two-foldhigher promoter activity than the -1562C allele (Zhang et al., 1999).Matsumura (Matsumura et al., 2005) reported that the T allele of theMMP-9 polymorphism is linked with the invasive phenotype of gas-tric cancer, but, Grieu and others (2004) thought that the MMP-9–1562T allele was associated with a better prognosis than C homozy-gotes in breast cancer. Our study suggests that the MMP-9C-1562Tpolymorphism is not associated with susceptibility for endometriosisand adenomyosis. This is consistent with our study into NSCLC(Wang et al., 2005). This discrepancy may be explained first by thedifferent role the MMP-9 polymorphism plays in different diseases.Second, although it has been shown that the MMP-9–1562T allele hasa higher promoter activity than the C allele, which may be because ofthe preferential binding of a putative transcription repressor protein tothe C allelic promoter (Pollanen et al., 2001), the significant differ-ence in promoter activity between the -1562C and -1562T alleles hasnot been observed in primary amnion epithelial cell cultures (Ferrandet al., 2002). Therefore, the significance of the MMP-9 C-1562T poly-morphism in disease development and progression should be furtherinvestigated in the different genotypes and phenotypes. Finally, fur-ther studies on other functional polymorphisms in the MMP-9 genemay help to explore the role of MMP-9 in development of disease.
So far, the aetiology of endometriosis and adenomyosis isunknown. Although adenomyosis and endometriosis differ withrespect to diagnosis and treatment, these two diseases seem to share acommon developmental mechanism with respect to MMP.
AcknowledgementsWe Dr Charles Hocart, Australian National University, for critical reading ofthe manuscript.
ReferencesAdachi Y, Yamamoto H, Itoh F, Hinoda Y, Okada Y and Imai K (1999) Con-
tribution of matrilysin (MMP-7) to the metastatic pathway of human color-ectal cancer. Gut 45,252–258.
AFS (1985) Revised American Fertility Society classification of endometriosis.Fertil Steril 43,351–352.
Aglund K, Rauvala M, Puistola U, Angstrom T, Turpeenniemi-Hujanen T,Zackrisson B and Stendahl U (2004) Gelatinases A and B (MMP-2 andMMP-9) in endometrial cancer-MMP-9 correlates to the grade and the stage.Gynecol Oncol 94,699–704.
Ajisaka H, Yonemura Y and Miwa K (2004) Correlation of lymph node metas-tases and expression of matrix metalloproteinase-7 in patients with gastriccancer. Hepatogastroenterology 51,900–905.
Birkedal-Hansen H, Moore WG, Bodden MK, Windsor LJ, Birkedal-Hansen B,DeCarlo A and Engler JA (1993) Matrix metalloproteinases: a review. CritRev Oral Biol Med 4,197–250.
Bruner-Tran KL, Eisenberg E, Yeaman GR, Anderson TA, McBean J andOsteen KG (2002) Steroid and cytokine regulation of matrix metalloprotein-ase expression in endometriosis and the establishment of experimentalendometriosis in nude mice. J Clin Endocrinol Metab 87,4782–4791.
Chung HW, Wen Y, Chun SH, Nezhat C, Woo BH and Polan ML (2001)Matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-3mRNA expression in ectopic and eutopic endometrium in women withendometriosis: a rationale for endometriotic invasiveness. Fertil Steril75,152–159.
Cox KE, Piva M and Sharpe-Timms KL (2001) Differential regulation ofmatrix metalloproteinase-3 gene expression in endometriotic lesions com-pared with endometrium. Biol Reprod 65,1297–1303.
Fang S, Jin X, Wang R, Li Y, Guo W, Wang N, Wang Y, Wen D, Wei L andZhang J (2005) Polymorphisms in the MMP1 and MMP3 promoter and non-small cell lung carcinoma in North China. Carcinogenesis 26,481–486.
Ferrand PE, Parry S, Sammel M, Macones GA, Kuivaniemi H, Romero R andStrauss JF 3rd (2002) A polymorphism in the matrix metalloproteinase-9promoter is associated with increased risk of preterm premature rupture ofmembranes in African Americans. Mol Hum Reprod 8,494–501.
Fiotti N, Zivadinov R, Altamura N, Nasuelli D, Bratina A, Tommasi MA,Bosco A, Locatelli L, Grop A, Cazzato G et al. (2004) MMP-9 microsatel-lite polymorphism and multiple sclerosis. J Neuroimmunol 152,147–153.
Ghilardi G, Biondi ML, Erario M, Guagnellini E and Scorza R (2003) Colorec-tal carcinoma susceptibility and metastases are associated with matrix met-alloproteinase-7 promoter polymorphisms. Clin Chem 49,1940–1942.
Gilabert-Estelles J, Estelles A, Gilabert J, Castello R, Espana F, Falco C,Romeu A, Chirivella M, Zorio E and Aznar J (2003) Expression of severalcomponents of the plasminogen activator and matrix metalloproteinase sys-tems in endometriosis. Hum Reprod 18,1516–1622.
Grieu F, Li WQ and Iacopetta B (2004) Genetic polymorphisms in the MMP-2and MMP-9 genes and breast cancer phenotype. Breast Cancer Res Treat88,197–204.
Gumbiner BM (1996) Cell adhesion: the molecular basis of tissue architectureand morphogenesis. Cell 84,345–357.
Haro H, Crawford HC, Fingleton B, Shinomiya K, Spengler DM and MatrisianLM (2000) Matrix metalloproteinase-7-dependent release of tumor necrosisfactor-alpha in a model of herniated disc resorption. J Clin Invest 105,143–150.
Igney FH and Krammer PH (2002) Death and anti-death: tumour resistance toapoptosis. Nat Rev Cancer 2,277–288.
Jordan RC, Macabeo-Ong M, Shiboski CH, Dekker N, Ginzinger DG, WongDT and Schmidt BL (2004) Overexpression of matrix metalloproteinase-1and -9 mRNA is associated with progression of oral dysplasia to cancer.Clin Cancer Res 10,6460–6465.
Jormsjo S, Whatling C, Walter DH, Zeiher AM, Hamsten A and Eriksson P(2001) Allele-specific regulation of matrix metalloproteinase-7 promoteractivity is associated with coronary artery luminal dimensions among hyper-cholesterolemic patients. Arterioscler Thromb Vasc Biol 21,1834–1839.
Kang S, Wang Y, Zhang JH, Guo W and Na W and Li Y (2005) The functionof SNP in the MMP1 and MMP3 promoter is associated with susceptibilityto endometriosis in china. Mol Hum Reprod 11,423–427.
Kioi M, Yamamoto K, Higashi S, Koshikawa N, Fujita K and Miyazaki K(2003) Matrilysin (MMP-7) induces homotypic adhesion of human coloncancer cells and enhances their metastatic potential in nude mouse model.Oncogene 22,8662–8670.
Kokorine I, Nisolle M, Donnez J, Eeckhout Y, Courtoy PJ and Marbaix E (1997)Expression of interstitial collagenase (matrix metalloproteinase-1) is related tothe activity of human endometriotic lesions. Fertil Steril 68,246–251.
Leeman MF, Curran S and Murray GI (2003) New insights into the roles ofmatrix metalloproteinases in colorectal cancer development and progres-sion. J Pathol 201,528–534.
Matsumura S, Oue N, Nakayama H, Kitadai Y, Yoshida K, Yamaguchi Y,Imai K, Nakachi K, Matsusaki K, Chayama K et al. (2005) A single nucle-otide polymorphism in the MMP-9 promoter affects tumor progressionand invasive phenotype of gastric cancer. J Cancer Res Clin Oncol131,19–25.
Mattey DL, Nixon NB, Dawes PT, Ollier WE and Hajeer AH (2004) Associa-tion of matrix metalloproteinase 3 promoter genotype with disease outcomein rheumatoid arthritis. Genes Immun 5,147–149.
Miller SA, Dybes DD and Polesky HF (1988) A simple salting out procedurefor extracting DNA from human nucleated cells. Nucleic Acids Res16,1215.

Polymorphisms in the promoter regions
39
Noe V, Fingleton B, Jacobs K, Crawford HC, Vermeulen S, Steelant W,Bruyneel E, Matrisian LM and Mareel M (2001) Release of an invasion pro-moter E-cadherin fragment by matrilysin and stromelysin-1. J Cell Sci114,111–118.
Nojiri T, Morita H, Imai Y, Maemura K, Ohno M, Ogasawara K, Aizawa T,Saito A, Hayashi D, Hirata Y et al. (2003) Genetic variations of matrixmetalloproteinase-1 and -3 promoter regions and their associationswith susceptibility to myocardial infarction in Japanese. Int J Cardiol92,181–186.
Ohashi K, Nemoto T, Nakamura K and Nemori R (2000) Increased expres-sion of matrix metalloproteinase 7 and 9 and membrane type 1-matrixmetalloproteinase in esophageal squamous cell carcinomas. Cancer88,2201–2209.
Pollanen PJ, Karhunen PJ, Mikkelsson J, Laippala P, Perola M, Penttila A,Mattila KM, Koivula T and Lehtimaki T (2001) Coronary artery complicatedlesion area is related to functional polymorphism of matrix metalloproteinase9 gene: an autopsy study. Arterioscler Thromb Vasc Biol 21,1446–1450.
Poncelet C, Leblanc M, Walker-Combrouze F, Soriano D, Feldmann G,Madelenat P, Scoazec JY and Darai E (2002) Expression of cadherins andCD44 isoforms in human endometrium and peritoneal endometriosis. ActaObstet Gynecol Scand 81,195–203.
Poulaki V, Mitsiades CS and Mitsiades N (2001) The role of Fas and FasL asmediators of anticancer chemotherapy. Drug Resist Updat 4,233–242.
Powell WC, Fingleton B, Wilson CL, Boothby M and Matrisian LM (1999)The metalloproteinase matrilysin proteolytically generates active solubleFas ligand and potentiates epithelial cell apoptosis. Curr Biol 9,1441–1447.
Quantin B, Murphy G and Breathnach R (1989) Pump-1 cDNA codes for aprotein with characteristics similar to those of classical collagenase familymembers. Biochemistry 28,5327–5334.
Schneider P, Holler N, Bodmer JL, Hahne M, Frei K, Fontana A and TschoppJ (1998) Conversion of membrane-bound Fas (CD95) ligand to its solubleform is associated with down-regulation of its proapoptotic activity and lossof liver toxicity. J Exp Med 187, 1205–1213.
Scotti S, Regidor PA, Schindler AE and Winterhager E (2000) Reduced prolif-eration and cell adhesion in endometriosis. Mol Hum Reprod 6,610–617.
Szamatowicz J, Lauda ski P and Tomaszewska I (2002) Matrix metalloprotein-ase-9 and tissue inhibitor of matrix metalloproteinase-1: a possible role inthe pathogenesis of endometriosis. Hum Reprod 17,284–288.
Wang Y, Fang SM, Wei LH, Wang R, Jin X, Wen DG, Li Y, Guo W, Wang Nand Zhang JH (2005) Association of the C-1562T polymorphism in the pro-moter of matrix metalloproteinase-9 gene with non-small cell lung carci-noma. Lung Cancer 49,155–161.
Wilson CL and Matrisian LM (1996) Matrilysin: an epithelial matrix metallo-proteinase with potentially novel functions. Int J Biochem Cell Biol28,123–136.
Ye S (2000) Polymorphism in matrix metalloproteinase gene promoters: impli-cation in regulation of gene expression and susceptibility of various dis-eases. Matrix Biol 19,623–629.
Yu C, Pan K, Xing D, Liang G, Tan W, Zhang L and Lin D (2002) Correlationbetween a single nucleotide polymorphism in the matrix metalloproteinase-2 promoter and risk of lung cancer. Cancer Res 62,6430–6433.
Yu YY, Guo XH, Qian JH, Du Zhang JH and XJ (2003) The expression ofmatrix metalloproteinase 9 and tissue inhibitor of metalloproteinase 3 inendometriosis. Prog Obstet Gynecol 12,25–27.
Zhang B, Ye S, Herrmann SM, Eriksson P, de Maat M, Evans A, Arveiler D,Luc G, Cambien F, Hamsten A et al. (1999) Functional polymorphism in theregulatory region of gelatinase B gene in relation to severity of coronaryatherosclerosis. Circulation 99,1788–1794.
Zhang JH, Jin X, Fang S, Li Y, Wang R, Guo W, Wang N, Wang Y, Wen D,Wei L et al. (2004) The functional SNP in the matrix metalloproteinase-3promoter modifies susceptibility and lymphatic metastases in esophagealsquamous cell carcinoma but not in gastric cardiac adenocarcinoma. Car-cinogenesis 25,2519–2524.
Zhang J, Jin X, Fang S, Wang R, Li Y, Wang N, Guo W, Wang Y, Wen D, Wei Let al. (2005) The functional polymorphism in the matrix metalloproteinase-7promoter increases susceptibility to esophageal squamous cell carcinoma,gastric cardiac adenocarcinoma and non-small cell lung carcinoma. Carcino-genesis 26,1748–1753.
Submitted on November 2, 2005; accepted on December 12, 2005