Embed Size (px)
Citation preview

Case Report
Polymicrogyria in Fetal Alcohol Syndrome
Konstanze Reinhardt,1* Alexander Mohr,2 Jutta Gartner,1 Hans-Ludwig Spohr,3 and Knut Brockmann1
1Department of Pediatrics and Pediatric Neurology, University of Gottingen, Gottingen, Germany2Department of Neuroradiology, University of Gottingen, Gottingen, Germany3Department of Pediatrics, Hospital of the German Red Cross, Berlin, Germany
Received 28 July 2009; Accepted 13 August 2009
BACKGROUND: Intrauterine exposure to alcohol may result in a distinct pattern of craniofacial abnormalitiesand central nervous system dysfunction, designated fetal alcohol syndrome (FAS). The spectrum of malfor-mations of the brain associated with maternal alcohol abuse during pregnancy is much broader than the rel-atively uniform clinical phenotype of FAS. Among these malformations the most striking abnormalitiesinvolve the impairment of neuronal cell migration. However, polymicrogyria (PMG) has so far been reportedonly once in a human autopsy study of a child with FAS. CASE: A 16-year-old girl with confirmed maternalalcohol consumption during pregnancy and full phenotype of FAS presented after two generalized epilepticseizures for neurologic assessment. Cranial magnetic resonance imaging revealed bilateral PMG in the supe-rior frontal gyrus with asymmetric distribution. History, clinical features, and genetic investigations pro-vided no evidence for any of the known genetic or acquired causes of PMG. Therefore, we propose that pre-natal alcohol exposure is the cause of PMG in this patient rather than a mere coincidence. CONCLUSION:
Our observation represents only the second patient of PMG in FAS and confirms the phenotypic variabilityof cerebral malformations associated with maternal alcohol abuse during pregnancy. In patients with clinicalfeatures of FAS and neurologic deficits or seizures neuroimaging is recommended. Furthermore, FAS shouldbe considered as a differential diagnosis for PMG. Birth Defects Research (Part A) 88:128–131, 2010. � 2009Wiley-Liss, Inc.
Key words: FAS; fetal alcohol spectrum disorders; fetal alcohol syndrome; partial fetal alcohol syndrome;polymicrogyria
INTRODUCTION
Intrauterine exposure to alcohol may result in a dis-tinct pattern of craniofacial abnormalities and centralnervous system dysfunction. The term fetal alcohol spec-trum disorders (FASD) has been coined to characterizethe wide range of conditions associated with teratogeniceffects of alcohol. Fetal alcohol syndrome (FAS), describ-ing the full phenotype, and partial fetal alcohol syn-drome (pFAS), with some but not all of the features, aregathered under the umbrella term FASD. FAS is one ofthe most frequent causes of developmental delay(Sampson et al., 1997; May and Gossage, 2001).
According to recent guidelines for referral and diagno-sis of FAS (Bertrand et al., 2004) diagnostic criteria ofFAS comprise facial dysmorphia (smooth philtrum, thinvermillion, small palpebral fissures), prenatal or postnatalgrowth at or below the 10th percentile, and structural,
neurologic, as well as functional central nervous system(CNS) abnormalities. The last named include, amongother features, head circumference at or below the 10thpercentile, clinically significant brain abnormalitiesobservable through imaging, and global cognitive or in-tellectual deficits or functional deficits in severaldomains.Ethanol exposure during brain development induces
microcephaly as the principal feature (Clarren et al.,1978) but can be associated with a wide spectrum ofother lesions. Neuropathologic abnormalities found in
*Correspondence to: Konstanze Reinhardt, Department of Pediatrics andPediatric Neurology, Georg August University, Robert Koch Str. 40, 37075Gottingen, Germany. E-mail: [email protected] online 17 September 2009 in Wiley InterScience (www.interscience.wiley.com).DOI: 10.1002/bdra.20629
Birth Defects Research (Part A): Clinical and Molecular Teratology 88:128�131 (2010)
� 2009 Wiley-Liss, Inc. Birth Defects Research (Part A) 88:128�131 (2010)

FAS include hydranencephaly, anencephaly, holoprosen-cephaly, cerebral dysgenesis, abnormal neural migration,hydrocephaly, enlarged, reduced, or absent ventricles,and severe CNS disorganization. Furthermore, abnormal-ities of basal ganglia, diencephalon, cerebellum, brain-stem, optic nerve, olfactory bulb, hippocampus, pituitary,and neuronal tube were also reported (Jones and Smith,1973, 1975; Clarren et al., 1978; Peiffer et al., 1979;Wisniewski et al., 1983; Coulter et al., 1993). Neuroimag-ing studies revealed brain abnormalities in vivo compris-ing overall size, shape, and symmetry of the brain, alongwith regional decreases in white and gray matter. Inaddition, abnormalities have been noted in specific struc-tures, such as cerebellum, corpus callosum, and basalganglia (Mattson et al., 1996; Swayze et al., 1997;Riikonen et al., 1999; McGee and Riley, 2006; Spadoniet al., 2007).
Polymicrogyria (PMG) has so far been reported onlyonce in a human autopsy study of a child with FAS(Peiffer et al., 1979). Here we report bilateral PMGdetected by neuroimaging in a 16-year-old girl with FAS.
CASE REPORT
This 16-year-old girl presented after two generalizedepileptic seizures for neurologic assessment. Based onhistory and characteristic clinical features a fetal alcoholsyndrome had been diagnosed at age nine years. She wasborn in Russia to parents both addicted to alcohol, andchronic maternal alcohol abuse of the mother during thepregnancy with this girl was confirmed. Further detailsconcerning pregnancy, birth, and early developmentwere not available. Allegedly she and her youngerbrother grew up under severe psychosocial deprivation.
When the girl was five years old authorities took overguardianship for the siblings and ordered their accom-modation in a children’s home. At that time the girlcould hardly speak. Later both siblings were adoptedand moved to Germany. At the age of nine years FASwas diagnosed because of microcephaly, FAS characteris-tic facial anomalies including short palpebral fissures,thin vermilion border of the upper lip and smooth phil-trum, as well as postnatal growth retardation (height 3rdpercentile, weight 3rd–10th percentile, head circumfer-ence <3rd percentile). Psychological testing at 10 years ofage using the Hamburg Wechsler Intelligence Scale forChildren revealed an IQ of 84. Cardiac and abdominalultrasound showed no abnormalities. An EEG at the ageof 10 years was normal. The girl attended a specialschool and showed slow developmental progress.At 16 years of age, two generalized tonic clonic seiz-
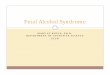
ures prompted further investigations. Body weight andheight were at the 3rd percentile, and head circumferencewas 0.5 cm below the 3rd percentile. Facial abnormalitiesincluded small palpebral fissures, smooth philtrum, andthin vermillion. Neurologic examination was otherwisenormal. A waking state EEG showed focal slowing andfocal sharp waves in the right temporal region; an EEGduring sleep was normal. MRI of the brain revealed anabnormally thick cortex with bilateral PMG in the supe-rior frontal gyrus with asymmetric distribution (Fig. 1).In addition, two small unspecific periventricular lesionswere detected.Karyotyping was normal. Mutation analysis of exons
2–14 including the sequences of flancing introns of theGPR56 gene (Piao et al., 2004) revealed no abnormalities.In addition, multilocus probe (MLP) analysis providedno evidence for a deletion or duplication of 22q11.
Figure 1. Cerebral magnetic resonance imaging (cMRI) of a girl with FAS at age 16 years. Original slices with 0.75 mm slice thickness(D, E) of a 3D MPRAGE T1 MRI-dataset and 2 mm coronal (A–C) and transversal (F) reconstructions, acquired on a 3 Tesla unit.Arrows indicate the cortical areas with polymicrogyria. Image D represents the original slice intersecting perpendicular to A throughthe pathologic region. Image E intersects images B and C at the level of the superior frontal sulcus. Note the different appearance of thedisorder depending on the level of intersection and on the orientation of the plane.
129PMG IN FAS
Birth Defects Research (Part A) 88:128�131 (2010)

DISCUSSION
The 16-year-old girl reported here fulfills the diagnosticcriteria of FAS including confirmed prenatal alcohol ex-posure, characteristic facial abnormalities, deficits ofbody and head growth, and global cognitive deficits. Theoutstanding feature of this patient is represented by bilat-eral PMG in the superior frontal gyrus revealed by cra-nial MRI.
A wide range of cerebral malformations is associatedwith FAS, as demonstrated in both histologic and neuro-radiological studies (Jones and Smith, 1973, 1975; Clarrenet al., 1978; Peiffer et al., 1979; Wisniewski et al., 1983;Coulter et al., 1993; Mattson et al., 1996; Swayze et al.,1997; Riikonen et al., 1999; McGee and Riley, 2006;Spadoni et al., 2007). It has been emphasized that thespectrum of malformations of the brain is much broaderthan the relatively uniform clinical phenotype. However,PMG in FAS has been described only in a single patientwho was included in a neuropathology study of threechildren and three fetuses with alcohol embryo- and fet-opathy (Peiffer et al., 1979). That nine-month-old girl haddied from pneumonia due to aspiration. Autopsyrevealed hydrocephalus internus, agenesis of the corpuscallosum, porencephaly of the left parietal region, malfor-mation of the cerebellum, and PMG in the orbital, tempo-ral, and parieto-occipital surfaces (Peiffer et al., 1979). Toour knowledge, PMG in FAS detected by in vivo neuroi-maging has not been reported before.
There is experimental evidence that alcohol interfereswith many molecular, neurochemical, and cellular eventsoccurring during normal development of the brain(Guerri, 2002). Cell acquisition, cell migration, and cellularmaturation result in the formation of functional neuronalnetworks in the developing nervous system (Lewis, 1985).It has been shown that all of these three mechanisms aresusceptible to disturbance by alcohol exposure. In the firstmonth of human gestation maternal ethanol drinking isassociated with a great incidence of craniofacial and neu-ronal tube anomalies. In addition, increased neural crestcell death was noted (Ernhart et al., 1987). In the secondtrimester alcohol exposure reduces the number of neuronsand glia cells in the neocortex and induces changes in ra-dial glia as well as neuronal proliferation, generation, andmigration (Miller, 1995). During the third trimester of ges-tation alcohol interferes with synaptogenesis as well asglial development and increases natural cell death and cellnecrosis (Guerri and Renau-Piqueras, 1997; Ikonomidouet al., 2000). Among these malformations the most strikingabnormalities appear to involve the impairment of neuro-nal cell migration (Miller, 1986, 1993). Animal experi-ments indicate that PMG is part of the spectrum of migra-tion disorders in FAS. In 1984 the first nonhuman primatemodel for the fetal alcohol syndrome was developed. Thebrains of two infant monkeys showed neuropathologicalchanges indicative of disturbed cell migration. The loweralcohol dose was associated with leptomeningeal neuro-glial heterotopia, while the brain of the infant monkeyexposed to high-dose alcohol was 30% smaller than nor-mal and grossly dysplastic. The frontal lobe demonstratedtrue PMG, which merged into pachygyria in the parietallobe and then agyria in the occipital lobe (Clarren andBowden, 1984).
PMG is characterized by an excessive number of smalland prominent convolutions spaced out by shallow and
enlarged sulci, giving the cortical surface a lumpyappearance (Guerrini and Carrozzo, 2001). The pathoge-nesis of PMG is poorly understood. Brain pathologydemonstrates abnormal development or loss of neurons.Two histologic types are recognized. In unlayered PMG,the molecular layer is continuous and does not followthe profile of the convolutions, and the underlying neu-rons have radial distribution but no laminar organization(Ferrer, 1984). In four-layered PMG, there is a layer ofintracortical laminar necrosis with the consequent impair-ment of late migration and postmigratory disruption ofcortical organization (Richman et al., 1974). These twosubtypes do not necessarily have a distinct origin,because both may coexist in contiguous cortical areas(Harding and Copp, 1997). PMG can be confined to a sin-gle gyrus, involve a portion of one hemisphere andappear bilateral and asymmetrical, bilateral and symmet-rical, or diffuse. PMG may occur as an isolated lesion, inassociation with other brain malformations such as heter-otopias or white matter lesions, or as part of several mul-tiple congenital anomaly and mental retardation syn-dromes (Guerrini and Parrini, 2009).Genetic causes of PMG (Jansen and Andermann, 2005;
Guerrini et al., 2008; Guerrini and Parrini, 2009) includechromosomal aberrations (Campeau et al., 2008), peroxi-somal disorders (Liu et al., 1976), GPR56 mutations (Piaoet al., 2004), microdeletion of 22q11 (Sztriha et al., 2004;Robin et al., 2006), mutations in the carnitine palmitoyl-transferase II gene (Meir et al., 2009), MECP2 mutationswith severe neonatal encephalopathy (Geerdink et al.,2002), PAX6 gene mutation with the absence of the pinealgland (Mitchell et al., 2003), mutation in MTTL1 genewith dysmorphic features and raised lactic acid (Kenget al., 2003), muscular dystrophies with defective dystro-glycan glycosylation (Clement et al., 2008), SRPX2 muta-tions with Rolandic epilepsy, mental retardation, andspeech dyspraxia (Roll et al., 2006), as well as TBR2mutations with agenesis of the corpus callosum andmicrocephaly (Baala et al., 2007).Acquired causes of PMG comprise intrauterine cytome-
galy virus infection (Marques Dias et al., 1984; Haywardet al., 1991; Barkovich and Lindan, 1994), vasculardisruption during the period of neuronal migration(Norman, 1980; Barth and van der Harten, 1985;Barkovich et al., 1995; Iannetti et al., 1998; Curry et al.,2005), and maternal drug ingestion (Barkovich et al.,1995).The clinical and neuroradiologic features of the patient
reported here as well as systematic laboratory investiga-tions provided no evidence for any of known inborn oracquired causes for PMG. Therefore, we propose a closerelationship between prenatal alcohol exposure and PMG.Our observation represents only the second patient of
PMG in FAS and confirms the phenotypic variability ofcerebral malformations associated with maternal alcoholabuse during pregnancy. In patients with severe neuro-logic impairment or seizures neuroimaging is recom-mended. Furthermore, FAS should be considered as adifferential diagnosis for PMG.
ACKNOWLEDGMENTSWe thank Dr. Ute Hehr, Human Genetics, University
of Regensburg, for performing mutation analysis of theGPR56 gene and the MLP analysis of 22q11.
130 REINHARDT ET AL.
Birth Defects Research (Part A) 88:128�131 (2010)

REFERENCES
Baala L, Briault S, Etchevers HC, et al. 2007. Homozygous silencing of T-box transcription factor EOMES leads to microcephaly with polymi-crogyria and corpus callosum agenesis. Nat Genet 39:454–456.
Barkovich AJ, Lindan CE. 1994. Congenital cytomegalovirus infection ofthe brain: imaging analysis and embryologic considerations. AJNRAm J Neuroradiol 15:703–715.
Barkovich AJ, Rowley H, Bollen A. 1995. Correlation of prenatal eventswith the development of polymicrogyria. AJNR Am J Neuroradiol16:822–827.
Barth PG, van der Harten JJ. 1985. Parabiotic twin syndrome with topicalisocortical disruption and gastroschisis. Acta Neuropathol 67:345–349.
Bertrand J, Floyd RL, Weber MK, et al. 2004. Fetal alcohol syndrome:guidelines for referral and diagnosis. Atlanta: Center for DiseaseControl and Prevention.
Campeau PM, Ah Mew N, Cartier L, et al. 2008. Prenatal diagnosis ofmonosomy 1p36: a focus on brain abnormalities and a review of theliterature. Am J Med Genet A 146A:3062–3069.
Clarren SK, Alvord EC, Jr, Sumi SM, et al. 1978. Brain malformationsrelated to prenatal exposure to ethanol. J Pediatr 92:64–67.
Clarren SK, Bowden DM. 1984. Measures of alcohol damage in utero inthe pigtailed macaque (Macaca nemestrina). Ciba Found Symp105:157–172.
Clement E, Mercuri E, Godfrey C, et al. 2008. Brain involvement in mus-cular dystrophies with defective dystroglycan glycosylation. AnnNeurol 64:573–582.
Coulter CL, Leech RW, Schaefer GB, et al. 1993. Midline cerebral dysgene-sis, dysfunction of the hypothalamic-pituitary axis, and fetal alcoholeffects. Arch Neurol 50:771–775.
Curry CJ, Lammer EJ, Nelson V, Shaw GM. 2005. Schizencephaly: hetero-geneous etiologies in a population of 4 million California births. AmJ Med Genet A 137:181–189.
Ernhart CB, Sokol RJ, Martier S, et al. 1987. Alcohol teratogenicity in thehuman: a detailed assessment of specificity, critical period, andthreshold. Am J Obstet Gynecol 156:33–39.
Ferrer I. 1984. A Golgi analysis of unlayered polymicrogyria. Acta Neuro-pathol 65:69–76.
Geerdink N, Rotteveel JJ, Lammens M, et al. 2002. MECP2 mutation in aboy with severe neonatal encephalopathy: clinical, neuropathologicaland molecular findings. Neuropediatrics 33:33–36.
Guerri C. 2002. Mechanisms involved in central nervous system dysfunc-tions induced by prenatal ethanol exposure. Neurotox Res 4:327–335.
Guerri C, Renau-Piqueras J. 1997. Alcohol, astroglia, and brain develop-ment. Mol Neurobiol 15:65–81.
Guerrini R, Carrozzo R. 2001. Epileptogenic brain malformations: clinicalpresentation, malformative patterns and indications for genetic test-ing. Seizure 10:532–543, quiz544–547.
Guerrini R, Dobyns WB, Barkovich AJ. 2008. Abnormal development ofthe human cerebral cortex: genetics, functional consequences andtreatment options. Trends Neurosci 31:154–162.
Guerrini R, Parrini E. 2009. Neuronal migration disorders. Neurobiol Disdoi: 10.1016/j.nbd. 2009.02.008.
Harding B, Copp A. 1997. Malformations of the nervous system. In:Graham J, Lantos ,PL, editors. Greenfield’s neuropathology. London:Edward Arnold. pp.521–538.
Hayward JC, Titelbaum DS, Clancy RR, Zimmerman RA. 1991. Lissence-phaly-pachygyria associated with congenital cytomegalovirus infec-tion. J Child Neurol 6:109–114.
Iannetti P, Nigro G, Spalice A, et al. 1998. Cytomegalovirus infection andschizencephaly: case reports. Ann Neurol 43:123–127.
Ikonomidou C, Bittigau P, Ishimaru MJ, et al. 2000. Ethanol-induced apo-ptotic neurodegeneration and fetal alcohol syndrome. Science287:1056–1060.
Jansen A, Andermann E. 2005. Genetics of the polymicrogyria syndromes.J Med Genet 42:369–378.
Jones KL, Smith DW. 1973. Recognition of the fetal alcohol syndrome inearly infancy. Lancet 2:999–1001.
Jones KL, Smith DW. 1975. The fetal alcohol syndrome. Teratology 12:1–10.
Keng WT, Pilz DT, Minns B, Fitzpatrick DR. 2003. A3243G mitochondrialmutation associated with polymicrogyria. Dev Med Child Neurol45:704–708.
Lewis PD. 1985. Neuropathological effects of alcohol on the developingnervous system. Alcohol Alcohol 20:195–200.
Liu HM, Bangaru BS, Kidd J, Boggs J. 1976. Neuropathological considera-tions in cerebro-hepato-renal syndrome (Zellweger’s syndrome). ActaNeuropathol 34:115–123.
Marques Dias MJ, Harmant-van Rijckevorsel G, Landrieu P, Lyon G.1984. Prenatal cytomegalovirus disease and cerebral microgyria: evi-dence for perfusion failure, not disturbance of histogenesis, as themajor cause of fetal cytomegalovirus encephalopathy. Neuropediat-rics 15:18–24.
Mattson SN, Riley EP, Sowell ER, et al. 1996. A decrease in the size of thebasal ganglia in children with fetal alcohol syndrome. Alcohol ClinExp Res 20:1088–1093.
May PA, Gossage JP. 2001. Estimating the prevalence of fetal alcohol syn-drome: a summary. Alcohol Res Health 25:159–167.
McGee CL, Riley EP. 2006. Brain imaging and fetal alcohol spectrum dis-orders. Ann Ist Super Sanita 42:46–52.
Meir K, Fellig Y, Meiner V, et al. 2009. Severe infantile carnitine palmi-toyltransferase Ii (Cpt Ii) deficiency in 19-week fetal sibs. Pediatr DevPathol 2009 Mar 31:1. [Epub ahead of print].
Miller MW. 1986. Effects of alcohol on the generation and migration ofcerebral cortical neurons. Science 233:1308–1311.
Miller MW. 1993. Migration of cortical neurons is altered by gestationalexposure to ethanol. Alcohol Clin Exp Res 17:304–314.
Miller MW. 1995. Effect of pre- or postnatal exposure to ethanol on thetotal number of neurons in the principal sensory nucleus of the tri-geminal nerve: cell proliferation and neuronal death. Alcohol ClinExp Res 19:1359–1363.
Mitchell TN, Free SL, Williamson KA, et al. 2003. Polymicrogyria andabsence of pineal gland due to PAX6 mutation. Ann Neurol 53:658–663.
Norman MG. 1980. Bilateral encephaloclastic lesions in a 26 week gesta-tion fetus: effect on neuroblast migration. Can J Neurol Sci 7:191–194.
Peiffer J, Majewski F, Fischbach H, et al. 1979. Alcohol embryo- and fet-opathy: neuropathology of 3 children and 3 fetuses. J Neurol Sci41:125–137.
Piao X, Hill RS, Bodell A, et al. 2004. G protein-coupled receptor-depend-ent development of human frontal cortex. Science 303:2033–2036.
Richman DP, Stewart RM, Caviness VS Jr. 1974. Cerebral microgyria in a27-week fetus: an architectonic and topographic analysis. J Neuropa-thol Exp Neurol 33:374–384.
Riikonen R, Salonen I, Partanen K, Verho S. 1999. Brain perfusion SPECTand MRI in foetal alcohol syndrome. Dev Med Child Neurol 41:652–659.
Robin NH, Taylor CJ, McDonald-McGinn DM, et al. 2006. Polymicrogyriaand deletion 22q11.2 syndrome: window to the etiology of a commoncortical malformation. Am J Med Genet A 140:2416–2425.
Roll P, Rudolf G, Pereira S, et al. 2006. SRPX2 mutations in disorders oflanguage cortex and cognition. Hum Mol Genet 15:1195–1207.
Sampson PD, Streissguth AP, Bookstein FL, et al. 1997. Incidence of fetalalcohol syndrome and prevalence of alcohol-related neurodevelop-mental disorder. Teratology 56:317–326.
Spadoni AD, McGee CL, Fryer SL, Riley EP. 2007. Neuroimaging andfetal alcohol spectrum disorders. Neurosci Biobehav Rev 31:239–245.
Swayze VW 2nd, Johnson VP, Hanson JW. 1997. Magnetic resonanceimaging of brain anomalies in fetal alcohol syndrome. Pediatrics99:232–240.
Sztriha L, Guerrini R, Harding B, et al. 2004. Clinical, MRI, and pathologi-cal features of polymicrogyria in chromosome 22q11 deletion syn-drome. Am J Med Genet A 127A:313–317.
Wisniewski K, Dambska M, Sher JH, Qazi Q. 1983. A clinical neuropatho-logical study of the fetal alcohol syndrome. Neuropediatrics 14:197–201.
131PMG IN FAS
Birth Defects Research (Part A) 88:128�131 (2010)



![The oculocerebrorenal syndrome of Lowe: an update...hypoplasia, pachygyria, polymicrogyria, aberrant neuronal migration,subependymalcysts,andcystslocatedinthewhite matter [13]. Kidney](https://img.pdfslide.us/doc/110x75/5f0b30697e708231d42f4994/the-oculocerebrorenal-syndrome-of-lowe-an-update-hypoplasia-pachygyria-polymicrogyria.jpg)