Embed Size (px)
Citation preview

Letter to the Editor
Nephron 2000;86:346–347
Polycythemia vera Presenting withRapidly Progressive Glomerulonephritis andPyoderma gangrenosum
Oktay Oymaka F. Sema Oymakb Tahir Patirogluc Hülya Taskapana Ayhan Dogukana
Mustafa Çetind Cengiz Utasa
aNephrology Unit, bDepartment of Chest Diseases, cDepartment of Pathology, and dHematology Unit,Erciyes University Medical School, Kayseri, Turkey
Dr. Oktay OymakHemodiyaliz ÜnitesiErciyes Üniversitesi Tıp FakültesiTR–38039 Kayseri (Turkey)Fax +90 3524375807
ABCFax + 41 61 306 12 34E-Mail [email protected]
© 2000 S. Karger AG, Basel0028–2766/00/0863–0346$17.50/0
Accessible online at:www.karger.com/journals/nef
Dear Sir,Polycythemia rubra vera (PV) is a myelo-
proliferative disease characterized by poly-cythemia, leukocytosis, and thrombocytosis.Thromboembolic events are importantcauses of morbidity and mortality [1]. Var-ious paraneoplastic and immunologicallymediated diseases associated with PV suchas pyoderma gangrenosum, Sweet’s syn-drome, leukocytoclastic vasculitis, autoim-mune hemolytic anemia, and ulcerative coli-tis have been described [2–6]. Here, a pa-tient with PV who had pyoderma gangreno-sum and developed acute renal failure dueto rapidly progressive glomerulonephritis(RPGN) is presented.
A 66-year-old male patient was referredto the hospital because of renal dysfunctionwith an active urinary sediment. He has suf-fered from weakness, dizziness, and diffuseabdominal pain for the last 2 weeks. Onphysical examination, he had mild hyperten-sion (160/100 mm Hg), a reddish face, in-jected conjunctivae, and moderate hepato-splenomegaly. There were large (8 ! 10 cm)ulcerated skin lesions on both legs whichshowed central slough and perilesional ery-thema, suggesting pyoderma gangrenosum.Laboratory studies on admission were: he-moglobin 20.8 g/dl, hematocrit 70% whiteblood cell count 17.9 B 109/l, platelet count660 ! 109/l, blood urea nitrogen 128 mg/dl, serum creatinine 7.5 mg/dl, uric acid18.5 mg/dl, total protein 7.9 g/dl, and albu-min 3.6 g/dl. Complement component C3
and C4 levels were 58 and 44 mg/dl, re-spectively. Urinalysis revealed proteinuria(300 mg/dl), and many erythrocytes and 3–4granular casts per high-power area were seenon microscopic examination. Arterial bloodgases were: pH 7.25, PO2 92 mm Hg, PCO224 mm Hg, HCO–
3 14.7 mEq/l, and O2 satu-ration 96%. The serum erythropoietin levelwas low with 2 mU/ml (normal range 4–25).Abdominal ultrasonography showed hepato-splenomegaly and bilateral nephromegaly
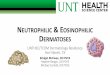
(both kidneys measured 15 ! 8 cm). Thesefindings were suggestive of PV, possibly as-sociated with acute renal failure. Renal biop-sy was performed immediately. All of 12 glo-meruli showed epithelial, endothelial, andmesangial cellular proliferation, mild basalmembrane thickening, focal necrosis areas,cellular crescents, and infiltration of inflam-matory cells, consistent with RPGN (fig. 1).Immunohistochemical studies revealed posi-tive staining for IgG, complement com-
Fig. 1. Light micrograph of the renal biosy specimen showing extra-capillary proliferation consistent with crescentic glomerulonephritis.HE. !80.
Dow
nloa
ded
by:
Uni
v. o
f Mic
higa
n, T
aubm
an M
ed.L
ib.
141.
213.
236.
110
- 9/
27/2
013
11:5
5:09
AM

Glomerulonephritis and Pyodermagangrenosum in Polycythemia vera
Nephron 2000;86:346–347 347
ponent C3, and fibrinogen. HBs-Ag, anti-HCV, cryoglobulin, anti-GBM, p-ANCA,c-ANCA, anti-dsDNA and antinuclear anti-body were negative. Daily phlebotomieswere performed to reduce the hematocritlevel to below 50%. Additionally, pulse cy-clophosphamide (750 mg i.v.) and predniso-lone (1 mg/kg p.o.) for the treatment ofRPGN and allopurinol for control of thehyperuricemia were started. The patient’s re-nal function recovered rapidly with the treat-ment. The pyoderma gangrenosum lesionsalso healed rapidly with atrophic scar forma-tion. One month later, the laboratory find-ings were: hematocrit 46%, white blood cellcount 11.7 ! 109/l, platelet count 327 !109/l, and serum creatinine 1.3 mg/dl. Twoweeks later the patient was hospitalizedagain with complaints of cough, dyspnea,and right-sided pleuritic pain. The clinicalfindings were suggestive of pulmonary em-bolism, and ventilation-perfusion scintigra-phy also showed a perfusion defect in theright lung. His laboratory findings on read-mission were: hematocrit 50%, white bloodcell count 26.1 B 109/l, platelet count 404 !109/l, and serum creatinine 1.5 mg/dl. Hewas anticoagulated initially with intrave-nous heparin infusion and thereafter withorally administered coumadin. His cytotoxictreatment was switched from pulse cyclo-phosphamide to oral azathioprine, and allo-purinol was discontinued. His complaintsresolved with the treatment, and he was dis-charged from the hospital with a regimenconsisting of prednisolone 20 mg, azathio-prine 150 mg, and coumadin 5 mg p.o.daily.
Polycythemia, leukocytosis, thrombocy-tosis, normal arterial blood oxygen tension,absence of any hypoxic pulmonary or car-diac disease, a very low level of erythropoie-tin, and the presence of splenomegaly sup-
ported the diagnosis of PV. Renal diseaseduring the course of the PV is very rare.Plomley et al. [7] reported on 6 patients withPV and proteinuria, 3 of them showed histo-logically defined mesangioproliferative glo-merulonephritis. Later, a case of focal seg-mental glomerulosclerosis and a case of He-noch-Schönlein purpura have been reportedin patients with PV [8, 9]. Recently, Kasunoet al. [10] described 2 cases of crescentic IgAnephropathy in association with PV, show-ing simultaneous amelioration of both dis-eases during treatment. To the best of ourknowledge, this is the first case presentingwith acute renal failure due to RPGN inassociation with PV. Light microscopic find-ings, immunohistochemical staining pattern,and depressed serum complement compo-nent C3 levels were consistent with immunecomplex mediated RPGN.
Simultaneous appearance of RPGN andpyoderma gangrenosum lesions and their re-sponse to treatment suggest that similar im-munolgic or pathologic mechanisms mayhave played a role in their development.
Arterial and venous thromboembolicevents are well-known complications in pa-tients with PV. Pearson and Wetherley-Mein[11] have described a strong correlation be-tween hematocrit level and thrombotic com-plications. However, the patient developedpulmonary embolism despite the achieve-ment of normal hematocrit values, suggest-ing that normalization of the hematocrit lev-els may not be sufficient for the preventionof thromboembolic complications.
In conclusion, RPGN should be consid-ered in the differential diagnosis of patientswith PV presenting with acute renal failure,and early renal biopsy and institution ofimmunosuppressive treatment may be life-saving.
References
1 Schwarcz TH, Hogan LA, Endean ED, Roti-man IT, Kazmers A, Hyde GL: Thromboem-bolic complications of polycythemia: Polycy-themia vera versus smokers’ polycythemia. JVasc Surg 1993;17:518–523.
2 Ho KK, Otridge BW, Vandenberg E, PowellFC: Pyoderma gangrenosum, polycythemiarubra vera, and the development of leukemia. JAm Acad Dermatol 1992;27:804–808.
3 Cox NH, Leggat H: Sweet’s syndrome associat-ed with polycythemia rubra vera. J Am AcadDermatol 1990;23:1171–1172.
4 Wahba-Yahav AV: Chronic leukocytoclasticvascultitis associated with polycythemia vera:Effective control with pentoxifylline. J AmAcad Dermatol 1992;26:1006–1007.
5 Lenz HJ, Waller HD: Autoimmune hemolyticanemia in a patient with polycythemia vera:First description. Acta Haematol 1991;85:111.
6 Ching CK, Allan RN: Polycythemia rubra veraand ulcerative colitis. Am J Gastroenterol1990;85:1203–1204.
7 Plomley RF, Sullivan JR, Whitworth JA, Kin-caid-Smith PS, Fairley KF, Brown RW: Poly-cythemia vera and glomerulonephritis. AustNZ J Med 1983;13:125–129.
8 Sharma RK, Kohli HS, Arora P, Gupta A,Murari M, Pandey R, Kher V, Das BK: Focalsegmental glomerulosclerosis in a patient withpolycythemia rubra vera. Nephron 1995;69:361.
9 Kanauchi M, Dohi K, Shiiki H, Fujii Y, Ishika-wa H: Henoch-Schönleich purpura nephritisassociated with polycythemia vera. Intern Med1994;33:36–40.
10 Kasuno K, Ono T, Kamata T, Kawamura T,Suyama K, Oyama A, Matsushima H, Kuwa-hara T, Muso E, Sasayama S: IgA nephropathyassociated with polycythaemia vera: Acceler-ated course. Nephrol Dial Transplant 1997;12:212–215.
11 Pearson TC, Wetherley-Mein G: Vascular oc-clusive episodes and venous haematocrit in pri-mary proliferative polycythaemia. Lancet1978;ii:1219–1222.
Dow
nloa
ded
by:
Uni
v. o
f Mic
higa
n, T
aubm
an M
ed.L
ib.
141.
213.
236.
110
- 9/
27/2
013
11:5
5:09
AM