Embed Size (px)
Citation preview

POLYCYSTIC OVARIAN SYNDROME (PCOS)
“A GENERAL CONCEPT”
Prof. (Dr.) Dilip Panakkada, Professor & HoD, Deptt. of Hom. Pharmacy
&
Dr Varinder Kaur Roy, PGT (13th Batch), Dept of Homoeopathic Pharmacy,
National Institute of Homoeopathy, Kolkata..
ABSTRACT:-
Polycystic ovary syndrome (PCOS) is of clinical and public health importance as it is a very
common syndrome, affecting up to one in five women of reproductive age group. It is the
commonest endocrine disorder of women of reproductive age, manifested with a variety of
clinical signs & symptoms. Polycystic ovarian syndrome (PCOS) was originally discovered
in 1935 by Stein and Leventhal as a syndrome. It is also called "diabetes of bearded woman.”
It has significant and diverse clinical implications including reproductive
(infertility, hyperandrogenism, hirsutism), metabolic (insulin resistance, impaired glucose
tolerance, type 2 diabetes mellitus, adverse cardiovascular risk profiles) and psychological
features (increased anxiety, depression and worsened quality of life). PCOS has unique
interactions with the ever increasing obesity prevalence worldwide as obesity-induced insulin
resistance significantly exacerbates all the features of PCOS. Management should focus on
support, education, addressing psychological factors and strongly emphasising healthy
lifestyle with targeted medical therapy as required. Comprehensive evidence-based guidelines
are needed to aid early diagnosis, appropriate investigation, regular screening and treatment
of this common condition.
Today our knowledge about PCOS appears to have broader health implications
and to have profoundly altered our view of the gravity of this condition.
KEY WORDS:-
Polycystic ovarian syndrome, Stein and Leventhal syndrome, patho-physiology,
investigation and diagnosis, general management, homoeopathic treatment.
INTRODUCTION:-
Polycystic ovarian syndrome is one of the most common Endocrine disorders that affect
women and also a leading cause of infertility. Women with PCOD are in hyper androgenic

state and may be present with obesity, amenorrhoea, oligomenorrhoea, infertility, or
androgenic features. Those with PCOS are also at risk for both diabetes and diabetic
complications and cardiovascular disease, with a risk of a myocardial infarction 7 times than
the normal.
Nomenclature: Polycystic ovary syndrome (PCOS) is also known as polycystic ovarian
disease, functional ovarian hyperandroganism, ovarian hyperthecosis and sclerocystic ovary
syndrome.
Polycystic ovarian syndrome (PCOS) was originally discovered in 1935 by
Stein and Leventhal as a syndrome. Polycystic ovary syndrome (PCOS) is a health problem
that can affect a woman's:-
Menstrual cycle
Ability to have children
Hormones
Heart
Blood vessels
Definition: Polycystic ovary disease has been described in -some book as polycystic
syndrome which is recognised as a disease with presence of multiple small cysts in enlarged
ovaries, clinically associated with signs of androgen excess, i.e. hirsutism, alopecia, acne,
dandruff, problem in conceiving, obesity and menstrual cycle disturbances like
oligomenorrhoea and amenorrhoea. Some case may be identified as simple enlarged ovaries
with multiple small cysts without any clinical signs of the syndrome . When only the
radiological diagnostic criteria is met, it is called Polycystic Ovaries.
APPEARANCE: - with PCOS, women typically have –
High levels of androgens. (These are sometimes called male hormones, though
females also make them)
Missed or irregular periods (monthly bleeding).
Many small cysts (fluid-filled sacs) in their ovaries.
INCIDENCE:-
In a community-based study in the United Kingdom (UK), it was found that polycystic ovaries (PCO)
were particularly common among women of South Asian origin (52%)Ref#9. So every second women
in South Asia is likely to have PCOD, even young girls were more vulnerable to polycystic
ovarian syndrome than Europeans because as unhealthy diet and lack of exercise.
PATHOLOGY:-
Typically, the ovaries are enlarged two to five times the normal size. Stroma is increased. The
capsule is thickened and pearly white in colour. On bisection, multiple follicular cysts
measuring about 8- 10mm in diameter are crowded around the cortex.
Histologically, there is thickening of tunica albuginea. The cysts are
follicles at varying stages of maturation and atresia. There is theca cell hypertrophy (stromal
hyperthecosis). Patient may present with features of diabetes mellitus (insulin resistance).
CAUSES:-
The cause of PCOS is unknown. But most experts think that several factors including
genetics could play a role. Women with PCOS are more likely to have a mother or sister with
PCOS.
Themain underlying problem in PCOS is a hormonal imbalance. In women with PCOS, the
ovaries make more androgens than normal. Androgens are male hormones that females also
make. High levels of Androgens hormones affect the development and release of eggs during
ovulation.
Researchers also think insulin may be linked to PCOS. Insulin is a hormone that controls the
change of sugar, starches, and other food into energy for the body to use or store. Many
women with PCOS have too much insulin in their bodies because they have problems using
itof lack of utilization. Excess insulin appears to increase production of androgen. High
androgen levels can lead to:
Acne
Excessive hair growth
Weight gain
Problems with ovulation
CLINICAL FEATURES:-
The patient complains of increasing obesity, menstrual abnormalities in the form of
oligomenorrhoea, amenorrhoea, or DUB and infertility. There may be hirsutism.
Virilism is rare.
Acanthosis nigricans is characterised by specific skin changes due to insulin
resistance. The skin becomes thickened and pigmented. Commonly affected sites are
nape of neck, inner thighs, and axilla.
HAIR-AN syndrome in patients with PCOD is characterised by hyperandrogenism,
insulin resistance and acanthosis nigricans.
Internal examination reveals bilateral enlarged cystic ovaries.
PATHO-PHYSIOLOGY:-
PCOS have trouble with menstrual cycle and fertility the ovaries, where women eggs are
produced, have tiny fluid filled sacs called follicles or cysts. As the egg grows, the follicles
build up fluid. When the egg matures, the follicles breaks open, the egg is released, and the
egg travels through the fallopian tube to the uterus (womb) for fertilization. This is called
ovulation. In women with PCOS, the ovary doesn’t make all of the hormones it needs for an
egg to fully mature. The follicles may start to grow and build up fluid but ovulation does not
occur. Instead, some follicles may remain as cysts. For these reasons, ovulation does not
occur and the hormone progesterone is not made. Without progesterone, a women’s
menstrual cycle is irregular or absent, along with that the ovaries make male hormones
(Androgens), which also prevent ovulation.
PCOS CHANGES AT MENOPAUSE:-
PCOS affects many systems in the body. So, many symptoms may persist even though
ovarian function and hormone levels change as a woman nears menopause. For instance,
excessive hair growth continues, and male-pattern baldness or thinning hair gets worse after
menopause. Also, the risks of complications (health problems) from PCOS, such as heart
attack, stroke, and diabetes, increase as a woman gets older.
AFFECT OF PCOS DURING PREGNANCY:-
Women with PCOS appear to have higher rates of –
Miscarriage
Gestational diabetes
Pregnancy-induced high blood pressure (preeclampsia)
Premature delivery
Babies born to women with PCOS have a higher risk of spending time in a neonatal intensive
care unit (NICU) or of dying before, during, or shortly after birth. Most of the time, these
problems occur in multiple-birth babies (twins, triplets).
OTHER HEALTH PROBLEMS:-
Women with PCOS have greater chances of developing several serious health conditions,
including life-threatening diseases. Recent studies found that –
More than 50 percent of women with PCOS will have diabetes or pre-diabetes
(impaired glucose tolerance) before the age of 40.
The risk of heart attack is 4 to 7 times higher in women with PCOS than women of
the same age without PCOS.
Women with PCOS are at greater risk of having high blood pressure.
Women with PCOS have high levels of LDL (bad) cholesterol and low levels of HDL
(good) cholesterol.
Women with PCOS can develop sleep apnoea. This is when breathing stops for short
periods of time during sleep.
Women with PCOS may also develop anxiety and depression.
Women with PCOS are also at risk for endometrial cancer.

(Irregular menstrual periods and the lack of ovulation cause women to produce the hormone
estrogens, but not the hormone progesterone. Progesterone causes the endometrium (lining of
the womb) to shed each month during menstruation. Without progesterone, the endometrium
becomes thick, which can cause heavy or irregular bleeding. Over time, this can lead to
endometrial hyperplasia
INVESTIGATIONS AND DIAGNOSIS:-
PCOS is a diagnosis of exclusion, and biochemical and/or radiologic studies must be done to
ascertain the diagnosis.
Lab Studies:-
Androgen excess can be tested by checking for testosterone levels. (An elevated free
testosterone level is a sensitive indicator of androgen excess).
Levels of sex hormone-binding globulin (SHBG) are usually low in patients with
PCOS.
Other androgens, such as dehydroepiandrosterone-sulfate (DHEA-S), may be normal
or slightly above the normal range in patients with PCOS.
Pelvic Examination:-
If one has an ovarian cyst, the doctor may find that the ovaries feel larger than normal, and
there is more than usual discomfort during the bimanual exam than normally do. In this case,
the doctor may recommend additional laboratory tests to help make a diagnosis.
Imaging Studies:- Ultrasonography (USG) :-
Ovarian ultrasonography, preferably by trans-vaginal scan, can be performed to assess
ovarian morphology. Ultrasound is one of the most frequently used methods of diagnosing
ovarian cysts.
The most accurate pictures can be obtained by doing a trans-vaginal ultrasound (TVS). The
accuracy of the trans-vaginal ultrasound, some doctors skips the abdominal ultrasound and
goes directly to this method. The other advantage is that patent need not have a full bladder.
Imaging criteria:
12 or more peripheral simple cysts
Usually Characteristic 'string-of-pearls' appearance.
Ovaries are typically enlarged to >10cc, although in 30% of patients the ovaries have a normal volume.

Blood Tests:-
These may include:
Testosterone
DHEA sulfate
Luteinizing hormone (LH)
Follicle-stimulating hormone (FSH)
17-hydroxy progesterone
Prolactin
Thyroid-stimulating hormone (TSH), which triggers the release of thyroid hormone
from the thyroid gland.
Additional blood testing may include:
Fasting glucose
Cholesterol
Triglyceride levels
Blood tests are very useful for making the diagnosis. Typically, blood levels of hormones
reveal a high LH (Luteinising hormone) level; and a normal FSH (Follicle stimulating
hormone) level; and elevated levels of androgens.
COMPLICATIONS:-
Type 2 diabetes
High blood pressure
Increased triglycerides
Decreased high-density lipoprotein (HDL) cholesterol
Cardiovascular disease
Metabolic syndrome
Because PCOS disrupts the reproductive cycle and exposes the uterus to a constant supply of
oestrogen, women with PCOS are at risk of:
Abnormal uterine bleeding
Cancer of the uterine lining (endometrial cancer)
During pregnancy, one may be at increased risk of gestational diabetes and pregnancy-
induced high blood pressure.
GENERAL MANAGEMENT:-
Exercise
Exercise helps lower the blood sugar levels.
An increase in daily physical activity and participation in a regular exercise regimen
are essential for treating or preventing insulin resistance and for helping weight-control
efforts.
Weight loss in patients with PCOS who are obese is associated with a reduction of
hirsutism and a return of ovulatory cycles in 30% of women.
A change in the lifestyle here is a must to follow healthy dietary patterns and to be
within proper Body Mass Index levels. Most of the obese patients can minimize their PCOD
related problems just by losing weight.
Diet
Women who have impaired glucose tolerance should start a comprehensive program of diet
and exercise to reduce their risk of developing diabetes mellitus.
Low Carbohydrate diet
Advise women with polycystic ovary syndrome to follow a low-carbohydrate diet.
A diet high in protein offers more benefit to women with PCOS than does a diet high in
carbohydrates. However, a diet that calls for increased protein to compensate for decreased
carbohydrates may spike the intake of saturated fats, elevating the blood cholesterol levels
and increasing the risk of cardiovascular disease.
Carbohydrates provide energy, so strict restriction is not advisable.
Instead of carbohydrate choose complex carbohydrates, which are high in fiber. The more
fiber in a food, the more slowly it’s digested and the more slowly the blood sugar levels rise.
High-fiber carbohydrates include whole-grain breads and cereals, whole-wheat,
barley, brown rice and beans.
Consider quitting in case of smokers. Women who smoke have higher androgen
levels that may contribute to PCOS symptoms. Smoking also increases the risk for heart
disease.
A doctor may also prescribe medicines, such as:
Birth control pills. They can help the periods be regular and can reduce symptoms
such as excess facial hair and acne. These medicines are not used one is trying to get
pregnant.
HOMOEOPATHIC TREATMENT:-
Treatment goals are based on symptoms similarity (Totality of Symptoms), whether or not
women want to become pregnant, and chances of getting heart disease and diabetes. For
selection of remedy, definitely a detailed case taking is necessary. Apart from this the
repertory is very useful especially where clear cut indication is not present. The cases where
there are clear signs and symptoms there is no need of repertorization as the presenting signs
and symptoms will clearly indicate the remedy. And the cases without distinct signs and
symptoms are of real challenge. In this type of patients, the repertory is of real help. So
according to presenting complaints under PCOD, few rubrics are given from different books
which is not exhaustive.
KENT’S REPERTORY:-
Generalities, Obesity
1st Grade: Ferr., Graph., Caps., Calc.
2nd
Grade: Am-m., ant-c., aur., calc-ar., cupr., kali-bi., kali-c., lac-d., lyc., puls., sulp.
3rd
Grade: Agar., ambr., asaf., bry., canth., chin., cocc., con., guai., iod., lach.,mag-c., nux-
m., op., plb., sep., thuj., verat., etc.
Female, Menses, absent, amenorrhoea:
1st grade: Aur., Carb-s., Con., Tub., Ferr-i., Ferr., Graph., Kali-c., Lyc., Puls., Senec.,
Sep., Sil., Sulph.,Dulc.
2nd
grade: acon., am-c., apis., ars., bell., bry., calc., cocc., dros., ferr-ar., ferr-p., hell., ign.,
iod., kali-ar., kali-p., lach., nat-m., nux-m., phos., staph., valer., zinc, etc.
3rd
grade: aesc., agar., am-m., benz-ac., carb-v., cina., colch., dig., gels., nat-c., nat-p.,
podo., stram., verat., etc.
Female, Menses, short duration:
1st grade: Am-c., Lach., Puls., Sulph.
2nd
grade: alum., asaf., berb., carb-s., cocc., con., dulc., graph., nat-m., nux-v., phos., sep.,
thuj., etc.
3rd
grade: ars-i., ars., bov., clem., colch., iod., kali-c., lyc., mag-c., nat-s., sabad., sil., zinc.,
etc.

Menses, suppressed:
1st grade: Bell., Con., Cycl., Dulc., Ferr-i., Graph., Kali., Lach., Lyc., Puls., Senec., Sil.,
Sulph.
2nd
grade: Abrot., acon., am-c., ant-c., apis., aur-m., brom., bry., calc., cocc., colch., ferr-p.,
ferr., gels., hell., hyos., kali-ar., kali-n., nat-m., nux-m., rhust., sep., stram., verat., zinc., etc.
3rd
grade: aeth., alum., ars-i., berb., bufo., carb-v., coloc., dros., guai., hep., iod., kali-i., kali-
p., mag-c., merc., nux-v., op., podo., sang., sec., stann., thuj., verat-v., etc.
Female, STERILITY:
1st grade: Aur., Bor., Nat-c., Nat-m., Sep.
2nd
grade: Alet., am-c., calc., coff., con., ferr-p., ferr., grsph., hyos., iod., kali-bi., lach.,
merc., phos., plat., sil., zinc., etc.
3rd
grade: agn., apis., canth., carb-s., caust., dulc., helon., nat-p., nux-m., phyt., ruta., sulph.,
etc.
Female, Tumours, Ovaries:
1st grade: Apis., Lach., Lyc.
2nd
grade: Ars., bar-m., calc., coloc.,iod., plat., podo.
3rd
grade: apoc., ars-i., fl-ac., graph., hep., staph., stram., syph., thuj., zinc.
Female, Tumours, Ovaries, right:
1st grade: Lyc.
2nd
grade: Apis., podo.
3rd
grade: fl-ac.
Female, Tumours, Ovaries, left:
1st grade: Lach.
2nd
grade: Podo.
Female,Tumours, Ovaries,cysts:
2nd
grade: Apis., bov., bufo., coloc., iod., kali-br., lach., plat., rhus-t.
3rd
grade: canth., carb-an., merc., murx., prun., rhod., thuj.
BOERICKE’S REPERTORY
Female sexual system, OVARIES- CYSTS, DROPSY:
1st grade: Apoc., Arn., Ars., Aur. m. n., Bell., Bov., Bry., Cinch., Con., Ferr. Iod., Ggaph.,
Kali-br., Lach., lil-t., Med., Rhod., Sab., Tereb., Zinc.
2nd
grade: Apis., oophor., aur. iod., col., iod., lyc.
Female sexual system, OVARIES, CYSTS, DROPSY, Induration:
1st grade: Aur., Aur. m. n., Carbo an., Graph., Lach., Pall., Plat., Ustil.
2nd
grade: con., iod.
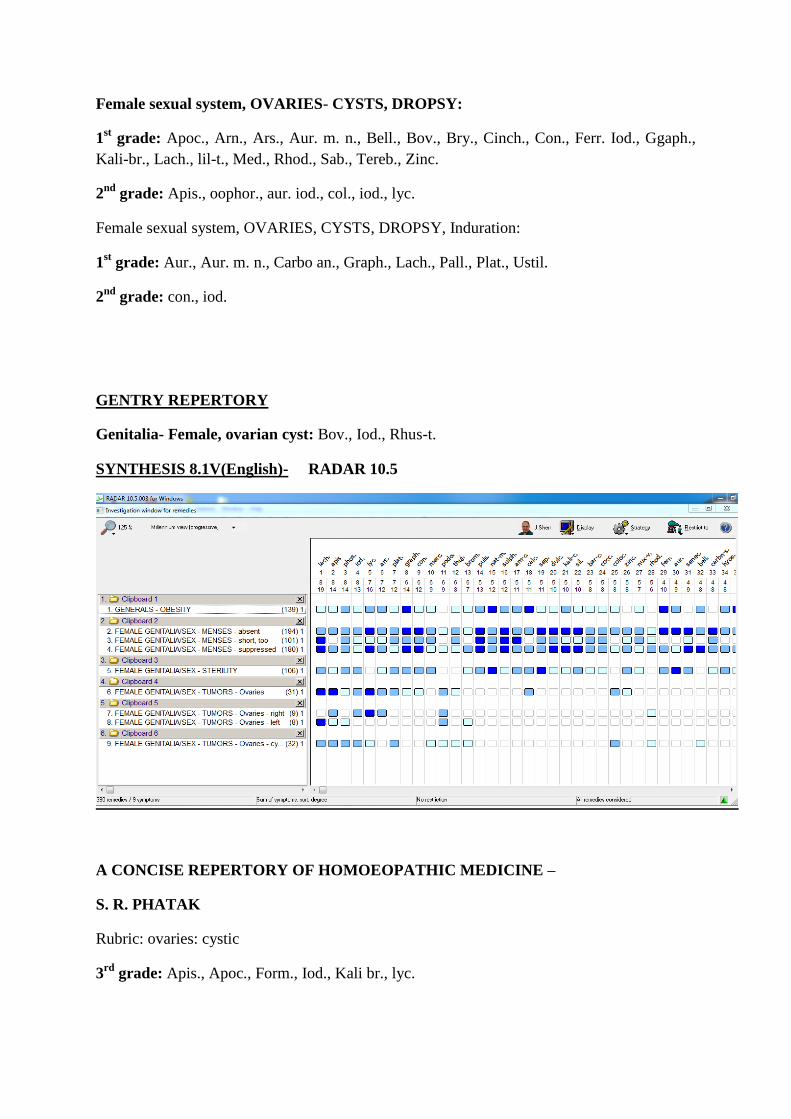
GENTRY REPERTORY
Genitalia- Female, ovarian cyst: Bov., Iod., Rhus-t.
SYNTHESIS 8.1V(English)- RADAR 10.5
A CONCISE REPERTORY OF HOMOEOPATHIC MEDICINE –
S. R. PHATAK
Rubric: ovaries: cystic
3rd
grade: Apis., Apoc., Form., Iod., Kali br., lyc.

BIBLIOGRAPHY
1. Boericke W, Pocket Manual of Homoeopathic Materia Medica and repertory. Reprint
ed. 2000. B. Jain publishers Pvt. Ltd.;
2. Dutta DC. Text book of gynaecology including contraceptions. Fourth reprint ed.
Calcutta. New Central Book Agency Pvt Ltd.; 2007.
3. Kent JT. Reportery of Homoeopathic Materia Medica. Sixth American reprint ed.
New Delhi: B Jain Publishers Pvt Ltd; 2004.
4. Phatak SR. A Concise Reportery of Homoeopathic medicines. Fourth ed. New Delhi:
B Jain Publishers Pvt Ltd; 2005.
5. Schroyens F.; Repertorium Homoeopathicum Syntheticum 8.1; B. Jain Publishers (P)
Ltd. New Delhi; 2005.
6. women.webmd.com/tc/polycystic-ovary-syndrome-pcos-topic-overview.
7. wikipedia.org/wiki/polycystic-ovary-syndrome.
8. Internet searches.
9. Rodin DA, Bano G, Bland JM, Taylor K, Nussey SS: Polycystic ovaries and
associated metabolic abnormalities in Indian subcontinent Asian women.
Clin Endocrinol 1998, 49:91-99
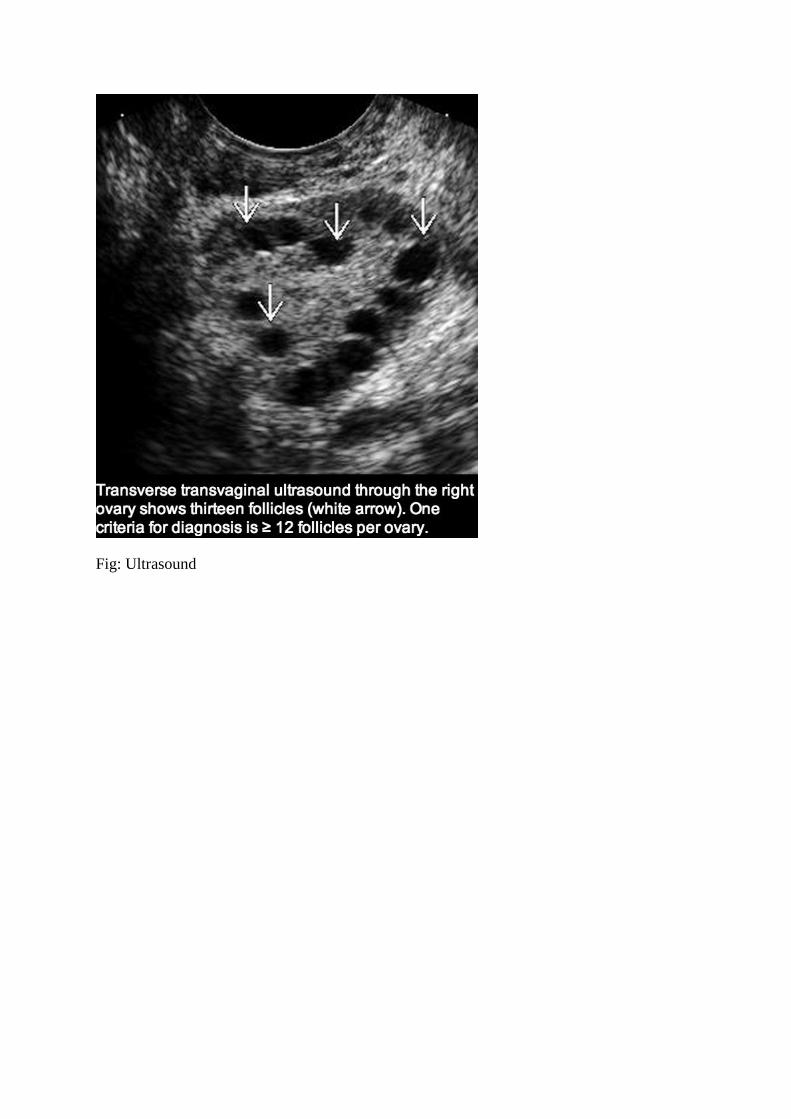
Fig: Ultrasound

Fig: MRI















![The regulation of ovarian follicular growth by anti ...fa.jmor.jp/pdf/35/1/035010013.pdf · ovarian syndrome (PCOS) patients and in the diagnosis of ovarian failure [23–25]. As](https://img.pdfslide.us/doc/110x75/5e6803a2bdc24c51c937f140/the-regulation-of-ovarian-follicular-growth-by-anti-fajmorjppdf351-ovarian.jpg)