Embed Size (px)
Citation preview
Polio End-game: What are the implications on polio vaccination
policy?
Dr Raju Shah

2010*
* data as on 30 October 2010
Last detected case January 2011
What more for – a polio free India!
No WPV from any source since January 2011
India is no longer an endemic country!

cVDPV cases, India 2009-2011•cVDPV cases detected in 2009-10
•100% due to type 2
DistrictType 2
2009 2010 2011
Badaun 3 0 0
Bulandshahar 2 0 0
Ghaziabad 0 1 0
Meerut 2 0 0
Moradabad 2 0 0
Pilibhit 4 0 0
Shahjahanpur 2 1 0
Total 15 2 0

State Type 1 Type 2
Assam 1Bihar 3Karnataka 1Madhya Pradesh 1Rajasthan 1Uttar Pradesh 4West Bengal 1
Total 1 11
iVDPV & aVDPV cases, India 2009 to 2012*
*: data as on 10 March 2012
iVDPV aVDPV
State Type 1 Type 2 Type 3
Chhattisgarh 1Punjab 1Tamil Nadu 1Uttar Pradesh 1Odisha 1
Total 1 3 1
ambiguous VDPV (aVDPV): origin uncertain e.g. single isolate from single AFP case, non-immunodeficient person
5
What is the polio 'endgame'?

6
'After interruption of wild poliovirus, continued use of OPV would compromise the goal of a polio-free world.
Expert Consultation on Vaccine-derivedPolioviruses (VDPVs), Sept 2003, Geneva

7
The endgame: addressing risks due to the oral polio vaccine (OPV) after eradication
• Cases of Vaccine-Associated Paralytic Poliomyelitis (VAPP): very rare severe adverse event; occurs in OPV recipients or a close contact.
• Outbreaks of circulating vaccine-derived poliovirus (cVDPV): very rare event; occurs when vaccine virus regains ability to paralyze and circulate.

8
Evolution of the 'Post-Eradication' Timeline
0 2 4 6 8 10 12
Years
Wild virus eradication
Global Cert Comm (1995) Certification
Expert Advisory Meeting (1998)
Certification & containment
Wild virus eradication
Last WPV case OPV cessation
ACPE (2004)VDPV elimination?Wild virus
eradicationCertification & containment
VDPV elimination & validation
Wild virus eradication
World Health Assembly (2008)
Post-OPV surveillance
Certification & containment
The 'Polio Endgame' refers to management of the
'post-eradication' risks due to OPV.

9
Why is the world now rethinkingthe Polio Endgame?

10
cVDPVs (Global): Problem in Eradication
Circulating Vaccine-Derived Poliovirus Oubreaks (cVDPVs) 2000-2010
Since 2009, 97% of cVDPV cases are due
to type 2
(& 40% of VAPP)
Type 2 (450 cases)
Type 1 (79 cases)
Type 3 (9 cases)

11
Risks of Polio After 'Eradication'with Continued OPV Use
VAPP 2-4/m birth cohort 250-500 stable
iVDPV 39 identified ~1 decreases
(since 1962)
cVDPV 0-3* per year ~20 increases
Frequency Annual Evolution
Risk to date burden over time
*based on current understanding

12
Recent developments allow a major 'rethink' of the endgame
• New bivalent vaccine (bOPV) outperforms trivalent OPV.
• New diagnostics show type 2 OPV is the main problem.
• New, very low cost 'IPV options' can allow all countries to continue type 2 immunization if they want/need to.

Best Solution
• Switch to IPV from OPV
Problem is COST!!!
Any developing country can afford?
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2010. All rights reserved
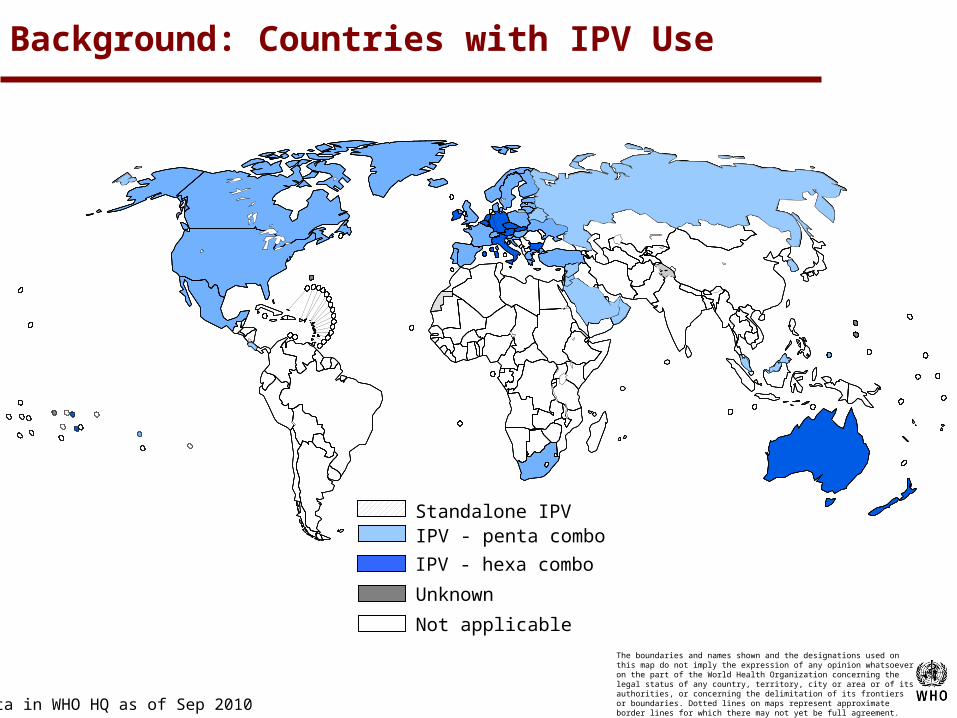
Standalone IPV
IPV - hexa combo
Data in WHO HQ as of Sep 2010
IPV - penta combo
Unknown
Not applicable
Background: Countries with IPV Use

“IPV would serve as a kind of
Insurance policy.” Roland Sutter
WHO, Research and production coordinatorGPE

How does universal or selective use of IPV helps?
Humoral immunity: a number of trials have addressed this question
• One dose of IPV after multiple doses of OPV effectively closes the remaining immunity gaps (~90% of seronegative cases will seroconvert)
• In seropositive individuals, a dramatic boosting of antibody titers is seen (~70-90%)
• After boosting, the antibody persist and then decline to a new baseline that is higher that before the IPV booster dose

Thinking of Affordable IPV Strategy: Approaches:
• Enables IPV production in developing countries with less or non-infectious strain
• Use adjuvant to reduce antigen contents per dose
• Develop intradermal (ID) device or micro-needle patch to stretch doses
• Use fewer doses per schedule
Reduce number of doses
Reduce amount of dose
Reduce antigen content
Reduce production cost

18
Affordable IPV options in the short-term:
Full-dose
$3
$0.6
Current price(low volume)
< $0.3
IPV price($ per dose)
** assumes full dose price of < US$1.5/dose at high volume
1/5th of 1 dose of IPV could be very affordable (<$0.5/dose)
1/5th fractional dose
Expected price(high volume**)
1/5th of 1 dose of IPV can induce a response in >90% of children
0
10
20
30
40
50
60
70
80
90
100
P1 P2 P3
Response* after 1 dose(%, intradermal IPV, Cuba)
* includes seroconversion & priming

IPV introduction
• Benefit – impact on RI ?• Timing/Age/Doses/Route – follow global SAGE
recs or our own ?• Frequency: 2 doses to all or in known cVDPV
risk areas?

Schedule of IPV administration
How to harvest optimal immunity gains of IPV: (seroconversion and antibody titers)
• IPV performance is negatively affected by levels of maternally-derived antibody
• So the timing of IPV administration should be delayed to minimize the interference effect
• The DTP3 visit (14 weeks in the EPI schedule) may offer the best compromise in terms of timing
IPV should be introduced in routine programs at least 6 months before an anticipated switch from tOPV to bOPV

21
What are the major elements of the 'New Polio Endgame'?

22
New Polio Endgame: Guiding Principles
• Phased removal of Sabin/OPV viruses, beginning with highest-risk (type 2).
• Elimination of type 2 in parallel by switching from tOPV to bOPV for routine EPI & campaigns.
• Introduction of 1 IPV dose to boost immunity 6 months prior to a tOPV-bOPV switch & provide type 2 'priming'.

23
New 'Endgame' strategy: parallel risk management
0 2 4 6 8 10 12
Years
Last wild polio case trivalent OPV cessation
VDPV elimination & validation
Wild virus eradication
Sequential risk management
Post-OPV surveillance
Certification & containment
VDPV2 elimination & validation
Post-OPV surveillance
Wild virus eradication
Parallel risk management
Certification & containment
OPV2 cessation& IPV introduction
bivalent OPV 1&3 (bOPV) cessation

24
Some Implications for IPV• IPV could be scaled up much earlier than anticipated
(i.e. tOPV-bOPV switch could be prior to April 2014).
• standalone IPV would be used for the 'tOPV-bOPV switch' with hexavalent having a 'post-OPV' role (e.g.
from 2017-18).
• a fractional (1/5th dose) intradermal IPV option may be essential for acceptability, cost, supply, manufacturer risk.
• the probability of expanded, longterm IPV use would increase substantially.

25
Advantages of the New Approach
• Accelerate type 1 & 3 eradication (with bOPV)
• Address >90% of VDPV risk while surveillance & response capacity is optimized
• Substantially shorten the post-eradication phase
• Boost routine immunization coverage (i.e. IPV at DPT3) and bridge immunity gaps

26
Potential Disadvantages of the New Approach
• Distraction to wild poliovirus eradication efforts in few countries. (to stop ongoing cVDPV2s; to coordinate tOPV-bOPV switch).
• Complications of adding a new vaccine (IPV) to shedule. (however, GPEI has introduced many new vaccines already).
• Risk of failure to stop new cVDPV2s as this is totally new stretegy. (but, with this approach could even 'restart' tOPV temporarily if needed).
• Risk of outbreaks of cVDPV 3 & 1. ( introduce IPV two doses)

Key target dates for a tOPV-bOPV switch timeline –
SAGE Polio Working Group (March 26, 2012)
• By end-2012: cessation of the ongoing cVDPV2 in Nigeria
• By September 2013 (latest): introduction of one supplementary IPV dose at an immunization contact (at or above age 14 weeks) in all OPV-using countries
• By April 2014: replacement of tOPV with bOPV for routine & supplementary immunization globally (possibly linked to a Global Immunization Week)
IPV in all OPV-using countries could begin latest by 7 September 2013, to enable a global tOPV-bOPV switch by April
2014, possibly linked to the 'global immunization week'.

Thanks








![POLIO VACCINATION IN NIGERIA: THE ‘GOOD’, THE ‘BAD’ … · transmission of wild polio virus types 1, 3 and cVDPV2.[2] This paper reports the ògood the îbad and the îugly](https://img.pdfslide.us/doc/110x75/5cd384bc88c993f5338d8b07/polio-vaccination-in-nigeria-the-good-the-bad-transmission-of.jpg)




















