Embed Size (px)
Citation preview

NURSING CLINICAL PRACTICE MANUAL Page 1 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
This policy has been approved and adopted by the following Parkview Hospital/Entity:
[x*] Hospital / Entity
Origination Date
Last Revision
Date
Last Approval
Date
Approved by:Name & Title of
Authorizing Leaderx Parkview LaGrange 6/13 8/13 J. Disler ,VP Patient care
xParkview Huntington
6/13 6/13 Juli Johnson, VP of Patient Care
x Parkview Whitley 6/13 6/13 B. Johnson VP Patient care
xParkview Ortho
6/13 6/13 L. Ferrell, Director of Nursing
x Parkview Noble 6/13 11/13 C. Byrd, VP Patient Care
xParkview Hospital (Randallia)
6/13 6/13 J. Boerger, S VP Patient Care
xParkview Regional Medical Center
6/13 6/13 J. Boerger, S VP Patient Care
Parkview BehavioralS. Boyce, Director of Nursing
*An asterisk indicates an addendum is included for this facility
I. POLICY STATEMENT All blood and blood products administered to patients within the Parkview health system will be administered according to the procedure outlined in this document.
II. DEFINITIONS
Informed Consent: Informed Consent is the communication that occurs between a physician and a patient, or person responsible for the patient’s care, regarding the risks and benefits of a proposed treatment and possible alternative treatments.Consent for Blood Transfusion: Paper consent that represents evidence of the communication between the physician and patient regarding the risks, benefits, and alternatives to transfusion.
1

NURSING CLINICAL PRACTICE MANUAL Page 2 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Type and Screen (T&S): Pre-transfusion testing required for blood products containing red blood cells. Testing includes ABO and Rh type with antibody screen for atypical red cell antibodies. Two ABO types are required for all patients receiving red blood products. Order is valid for 72 hours.ABO/Rh: Minimum pre-transfusion blood testing for Fresh Frozen Plasma, cryoprecipitate and platelets. Licensed Professional: A licensed professional includes, but not limited to: Registered Nurse (RN), Licensed Practical Nurse (LPN), Paramedic, and Respiratory Therapist (RT), Medical Technologist.Transfusion Nurse: The registered nurse (RN) who is responsible for the transfusion.Transfusion Administration Record (TAR): paper form (Form #425-2) used to document transfusion used for circumstances when the electronic medical record (EMR) is not available.Pediatric Transfusion: patient age 5 months through 18 years. Infant Transfusion: patient less than 5 months of age, refer to NICU Blood Transfusion. Emergent Transfusion: Physician ordered blood or blood products for hemodynamically unstable patients with exsanguinating hemorrhage requiring rapid transfusion.Massive Transfusion Protocol (MTP): Blood Bank standard for efficient and effective procurement and delivery of blood products for hemodynamically unstable patients with exsanguinating hemorrhage requiring rapid transfusion.
III. PRE-TRANSFUSION REQUIREMENTS
A. Valid physician order for the transfusion is required.1. Blood Bank staff may accept a telephone order for an emergent or massive transfusion from the
Emergency Room (ER), Operating Room (OR), or an Intensive Care Unit.2. Reference Blood and Blood Product Administration Guide for Nursing:
“Enter Transfusion “Order Set” (1)”.
B. Pre-transfusion blood specimen is dependent upon the type of blood or blood product. 1. Blood (Packed RBC’s): requires a Type and screen (T&S). If blood products are to be administered, the
appropriate cross-match test will automatically be performed by the lab.2. Blood products (FFP, platelets, and cryoprecipitate): requires an ABO/Rh Type and are issued from
blood bank ‘type-compatible’.
2

NURSING CLINICAL PRACTICE MANUAL Page 3 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
C. Proper collection and labeling of the pre-transfusion blood sample is critical. 1. For nurse collected specimen, “Print Label” must be completed from the “Worklist”.
a. Reference Blood and Blood Product Administration Guide for Nursing: Nurse Collection and Labeling of Pre-transfusion Specimen (2).
2. Patient Identification/Specimen collection - Patient should be asked to state his full name and Date of Birth to match to the labels used. In addition, the collector should compare the patient’s full name and MRN on the armband and the labels used.
3. Order of Blood draw - Refer to Lab Test Directory. 4. Specimen labeling - Blood samples for pre-transfusion testing must include the patient’s full name, MRN,
date and time of collection, and the identity of the collector (employee ID number).
D. Informed Consent/Consent Form for Transfusion . The ordering/authorizing provider is responsible for obtaining informed consent.
1. Prior to the transfusion, the Blood Consent form should be signed by the patient (or person responsible for the patient’s care) and witnessed/signed by the nurse.
2. Place signed consent under Tab 17 inside the patient’s paper chart.Note: Physician signature on the consent form is not required at time of transfusion and may be obtained later.
E. Pre-transfusion Documentation:1. Reference Blood and Blood Product Administration Guide for Nursing:
Pre-transfusion Documentation (3 ) .
F. Transfusion Teaching includes, but not limited to providing the patient/family the “Transfusion Information Brochure” (Form 2496-1). Avoid explaining the signs of transfusion reactions too graphically as it may cause the patient to “feel” symptoms of a reaction before the transfusion. Reference: “Blood Component Information” (page 12) for specific information.
G. Patient Assessment:1. Assess patient for adverse reaction to previous transfusion.
3

NURSING CLINICAL PRACTICE MANUAL Page 4 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
2. Assess patient for any pre-existing symptoms that are common to a transfusion reaction (e.g. back pain, headache, nausea, and cough).
3. Administer pre-transfusion medications as ordered.4. Assess appropriateness of the indwelling Vascular Access Device (VAD) and the VAD site.
“Blood or blood components may be transfused via a 14- to 24-gauge short peripheral catheter” or a Central Venous Access Device (CVAD) “as small as 1.9 French” (Journal of Infusion Nursing (2011), pg.S93).
5. Confirm VAD site is dedicated for only the blood or blood product.a. If patient requires additional intravenous drugs or fluids during a blood or blood product
transfusion, a separate vascular access site must be used or another site established (Journal of Infusion Nursing 2011; AABB 2010).
b. 0.9% sodium chloride (normal saline) is the only solution compatible with blood or blood components (Journal of Infusion Nursing 2011; AABB 2010).
6. Obtain vital signs (blood pressure/temperature/heart rate/respirations/O2 sat (if applicable) within 30 minutes of start of transfusion.
H. Gather supplies appropriate for the blood or blood product component administration .1. Electronic Infusion Administration (e.g. Inpatient areas).
a. Electronic Infusion Device (EID)b. EID primary pump tubing.c. Secondary infusion set with in-line filter.
2. Gravity administration (e.g. Critical Care areas, Operating Room):a. Y-Type blood tubing with standard in-line blood filter.b. 0.9% Normal Saline.
3. Supplementary equipment, if required:a. Blood and Fluid Pressure Infusersb. Blood and Fluid Warmers NOTE: Level 1 ® fluid infuser and warmer is “not for use in warming platelets, cryo-precipitates, or granulocyte suspensions” (Smiths Medical 2008).
4

NURSING CLINICAL PRACTICE MANUAL Page 5 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
I. Prime Tubing and Filter with .9% Normal Saline and ensure that the top of the filter is covered with saline.1. Attach primed tubing to venous access device (VAD) and set flow rate of .9% Normal Saline.
NOTE: Standard in-line filter (170- to 260-micron filter) and the IV tubing may be used for 4 hours or up to 4 units of RBC’s in 4 hours (Journal of Infusion Nursing 2011; AABB 2011).
O. “Release” blood or blood product unit for transfusion:1. EMR : For each unit transfused, a “Transfuse Order” form must be printed.
a. Reference Blood and Blood Product Administration Guide for Nursing: “Transfuse Order” Release and Form (4).
2. Non-EMR area or Downtime : Complete the paper “Blood Dispensing Form” .3. Emergent or Massive Transfusion: Call the Blood Bank. The patient’s full name and medical record
number is required to release blood for emergent or massive transfusion.NOTE: Call Blood Bank if a Transfusion Administration Record (TAR) is requested.
IV. BLOOD OR BLOOD PRODUCT ARRIVES ON UNIT
If the transfusion must be postponed, the blood or blood product must be returned to Blood Bank within 15 minutes.
If the start of the transfusion is delayed (e.g. new IV start needed, patient treatment), it is acceptable to hold onto the blood product until the transfusion can be initiated, as long as the transfusion is completed in 4 hours from the time of issue.
V. PATIENT AND DONOR-UNIT VERIFICATION“Accurate identification and verification of the donor’s blood and the intended recipient may be the single most important step in ensuring transfusion safety” (AABB, 2011, p. 525).
One RN & the second licensed professional must each independently perform a separate and independent verification of the blood or blood product (AABB, 2010).
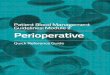
Patient and Donor-Unit Verification Process
5

NURSING CLINICAL PRACTICE MANUAL Page 6 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
1. At patient’s bedside, identify patient by means of two patient identifiers.2. Verify p atient’s name and the Medical Record Number (MRN) on the Compatibility Label matches the
patient’s name on the armband.3. Confirm that the Donor Unit Number, the Donor ABO/Rh, and the Expiration Date on the Face Label
(front of bag) matches the Donor unit number, the Donor ABO/Rh, and the Expiration Date on the Compatibility Label (back of bag).
4. Verify the Donor ABO/Rh type matches (or is compatible) with the Patient’s ABO/Rh type.5. Confirm that any patient-specific special requirements have been met (e.g. irradiation, CMV negative, splitting of units).Visual InspectionRed Packed Cells (RBC): Check for discoloration or leaking, clumping or clots.Non-Red Cell Products: Check for clots or leaking, foaming, or “egg-drop soup” appearance of platelets.Do Not Hang the blood or blood product if there is any question during the patient and donor unit verification or visual inspection of the unit. Contact the Blood Bank.
Reference Blood and Blood Product Administration Guide for Nursing: Second Licensed Professional: Documentation of Verification of the Patient and Donor Unit Identification (5).
ADDENDUM: Intraoperative Second Patient Identification Process
For the period of time when the patient is unable to participate in the patient identification process due to anesthesia, as well as restricted access to the patient’s ID band, the following patient identification process will utilized.
1. A duplicate patient ID band, confirmed with the patient’s ID band prior to the intraoperative phase will serve as the second patient identifier.
Face Label (front of bag) Compatibility Label (Back of bag)
6

NURSING CLINICAL PRACTICE MANUAL Page 7 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Donor Unit NumberExpiration DateABO/Rh
Yellow Sticker: Date/Time issued from Blood Bank
Patient;s NamePatient’s MRNPatient’s ABO/Rh type---------------------------------------------------------Donor Unit NumberDonor ABO/Rh typeExpiration Date/Time
ABO Compatibility ChartRed Blood Cell Compatibility Plasma CompatibilityGroup O may receive Group O red blood cells Group O may receive Group O, A, B or AB
plasmaGroup A may receive Group A or O red blood cells
Group A may receive Group A or AB plasma
Group B may receive Group B or O red blood cells
Group B may receive Group B or AB plasma
Group AB may receive Group AB, A, B or O red blood cells
Group AB may receive Group AB plasma
7

NURSING CLINICAL PRACTICE MANUAL Page 8 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
VI. INITIATE TRANSFUSION
A. Reference Blood and Blood Product Administration Guide for Nursing: Scanning (6).
B. Reference Blood and Blood Product Administration Guide for Nursing: Intial Documentation in the MAR (7).
C. Reassess patency of vascular access.
D. Gently mix contents of blood or blood product immediately prior to administration.
E. Observe Universal Precautions. Gloves must be worn (face shield is optional) (AABB, 2011).
F. Connect the blood or blood product to the primed blood tubing utilizing aseptic technique. Note: Each blood product bag has two sterile, sealed ports. Do not use ports that are not sealed.Utilize care when connecting the blood or blood product not to “spike through” the other side of bag.
G. Prime the blood or blood product through the tubing close to VAD site. Note: To expedite initiation of transfusion, the infusion rate may be temporarily increased.
H. “Set the initial rate of transfusion to ensure that 20-50 milliliters (ml) of blood or blood product is infused during the first 15 minutes (Adult/Child).
I. The RN must stay with the patient for 15 minutes after the “Start Time” (time when the transfusion enters the patient’s vein) to monitor for signs or symptoms of a transfusion reaction.
J. Once the initial15 minutes of the transufsion is complete:1. Assess patient for signs/symptoms of transfusion reaction or fluid overload.
8

NURSING CLINICAL PRACTICE MANUAL Page 9 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
2. Obtain and document vital signs.3. Adjust the rate of transfusion according to MD order or per component specific recommendation.4. Reference Blood and Blood Product Administration Guide for Nursing:
Adjust the Rate (8).NOTE: All transfusions must be completely infused within 4 hours from the “Issue Time”.
VII. DURING TRANSFUSION
A. Monitor patient for signs and sypmptoms of reaction.
B. Monitor VAD site for signs or symptoms of complications.C. Vital Sign frequency requirements:
1. Adults: At the conclusion of transfusion and as needed.2. Pediatric: Hourly, at conclusion of transfusion, and as needed.
B. Patient Assessment requirements: Reference Blood and Blood Product Administration Guide for Nursing: Patient Assessment Documentation (9).1. Patient Assessment is required every 30-minutes during the transfusion and one-hour post-transfusion.
NOTE: The transfusion RN may designate the patient assessments to a licensed professional nurse (LPN).
VIII. END OF TRANSFUSION
A. Ensure all of blood or blood product has infused and allow 0.9% Normal Saline to clear the tubing.
B. Assess patient, obtain vital signs and document.
C. Discard blood product bag and IV tubing in an appropriate biohazard trash receptacle.
D. Reference Blood and Blood Product Administration Guide for Nursing:
9

NURSING CLINICAL PRACTICE MANUAL Page 10 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
End of Transfusion (10). IX. POST TRANSFUSION ASSESSMENT AND EDUCATION
A. ONE-HOUR POST-TRANSFUSION assessment and documentation is required for all patients. 1. If an ambulatory patient requests to leave prior to the “One-Hour Post Transfusion” assessment, document
that the “patient left prior to one-hour assessment completion”.
B. Transfusion Discharge Instructions are required for all patientsReference Blood and Blood Product Administration Guide for Nursing: Discharge Education (11).1. Non-EMR areas or during Downtime: Utlize Outpatient Blood Transfusion Discharge Instructions (Form
#3657).
X. TRANSFER OF PATIENT DURING TRANSFUSION
A. If the patient must be transported to another patient care area (e.g. Radiology or Endoscopy), the RN/LPN responsible for the patient must notify the license professional staff that will accept the patient and the responsibility for the transfusion in progress. Accepting staff will continue to monitor the patient, the VAD site, and documentation.
XI. USE OF TRANSFUSION ADMINISTRATION RECORD (TAR) (e.g. Critical Care, Perioperative, Interventional Radiology, Dialysis, Cath Lab)
A. EMR to TAR1. Blood or blood product initiated in the EMR and the patient is transferred to an area without electronic
transfusion documentation. Call the Blood Bank to request a TAR to complete documentation.2. EMR documentation requires that a rate of “O” be entered into the blood or blood product MAR.
B. TAR to TAR:
10

NURSING CLINICAL PRACTICE MANUAL Page 11 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
1. If a blood or blood product is initiated on a TAR and the patient is transferred to another critical care area (e.g. PACU, Critical Care), the TAR should be completed by the receiving unit.
C. Operating Room:1. All blood or blood products initiated and/or completed in the Operating Room will utilize the paper TAR.
XII. TRANSFUSION REACTION
A. If the patient experiences a 2 degree Fahrenheit increase in temperature from pre-transfusion may indicate a transfusion reaction. Other symptoms include: new onset headache, cough, or pain; rapid onset respiratory distress; sustained, unexpected hypotension (drop of 30 mm Hg systolic or more); nausea/vomiting; chest tightness; chills; hives; or itching.NOTE: A transfusion reaction should not be initiated if patient is hypothermic and actively being warmed unless the patient experiences a 2 degree F or greater increase in temperature, AND that temperature is 99 degree F or above, or patient exhibits any other signs and symptoms of a transfusion reaction.
B. Immediate actions: (If patient is unstable, call a Rapid Response)1. Stop the transfusion. 2. Keep the vein open with normal saline to maintain venous access.3. Assess/monitor patient’s vital signs.
a. If the patient’s clinical condition is unstable, initiate a Rapid Response.4. Reverify Patient’s name, medical record number, verify ABO/Rh, unit number, expiration date/time on the
blood bag label with the order in the EMR.5. Contact Blood Bank STAT to report patient condition.6. Follow Blood Bank recommendations.
a. If Transfusion Reaction work-up indicated, Reference Blood and Blood Product Administration Guide for Nursing: Transfusion Reaction (16).
b. Hold the transfusion until notified by the Blood Bank with the preliminary interpretation of the Transfusion Reaction Panel.
11

NURSING CLINICAL PRACTICE MANUAL Page 12 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
c. The blood bank staff can report on the presence or absence of an acute hemolytic transfusion reaction only. They may make recommendations for further testing if the patient symptoms indicate a Transfusion-related Acute Lung Injury (TRALI) reaction.
7. Notify the physician of the Transfusion Reaction Panel and follow MD orders. 8. Document the following:
a. Assessment of patient and vital signs.b. Verification of repeated patient identification.c. Time transfusion stopped.d. Blood Bank notification.
9. If requested, send the following to Blood Bank:a. Blood bag with the tubing.b. Properly labeled urine specimen.
10.Closely monitor patient’s intake and output.
XIII. EMERGENT TRANSFUSION: See Blood Transfusions: Emergent Policy
A. If T & S has been performed, a TAR will be sent with blood or blood products to complete.
B. If no T & S has been performed, the Blood Bank will release “Uncrossmatched blood” along with a Transfer Sheet listing the units sent.
C. EMR Documentation:1. During emergent/urgent circumstances, document “Unit Given Uncrossedmatched” in the Blood
Administration flow.under Transfusion Documentation.2. Blood or blood product volumes are to be documented under Intake/Output >“Massive/Emergent
Transfusion.
12

NURSING CLINICAL PRACTICE MANUAL Page 13 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
XIV. MASSIVE TRANSFUSION: See Blood Transfusion-Massive: Adult Policy or Blood Transfusion-Massive: Pediatrics Policy
A. During a Massive Transfusion, it is crucial that the volume of each blood or blood product infused is recorded.
B. Document blood or blood product unit specific volumes in the EMR under Intake/Output> Massive/Emergent Transfusion.NOTE: If the patient is transferred to another area during the transfusion, each area (e.g. ICU, ER, PACU) will take part in documenting the Intake/Output >“Massive/Emergent Transfusion in the EMR.Exception: The Operating Room (OR) fluid totals will be on the anesthesia sheet.
Blood Component Information : (Press Control & Click on the blood or blood component you wish to review)Red_Blood Cells (PRBC, CMV Negative, Irradiated, Leuko Depleted, Washed)Random_Donor_PlateletsPheresed_PlateletsHuman_Leukocyte_Antigen (HLA) Matched Pheresed Platelets, Crossmatched PlateletsFresh_Frozen_Plasma (FFP) (FP24)
13

NURSING CLINICAL PRACTICE MANUAL Page 14 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Cryoprecipitate/Cryosuperatant Reduced PlasmaRh (Immune Globulin) (RhIG) Tradename RhophylacAlbumin (5% or 25%)HextendDextran, Dextran 40, L.M.D. 10%Plasma_Protein_Fraction PPFImmune_Serum_GlobulinsAntihemophilic_Factor RecombinateHumate – P Antihemophilic_Factor /Von_Willeband Factor Complex (Human)Coagulation_Factor_IX Benefix (Recombinant)Recombinant_Coagulation_Factor_VIIa Novo Seven
14

NURSING CLINICAL PRACTICE MANUAL Page 15 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Blood/Blood Components: Packed Red Blood Cells (PRBC)/Leukodepleted Red Blood Cells (RBC)/Washed Red Blood Cells (RBC)/Irradiated PRBC/Cytomegalovirus (CMV) Negative PRBCAll red cell units at Parkview Health are leukodepleted which minimize the occurrence of febrile non-hemolytic transfusion reactions.
Where obtained: LabCommon Indications:PRBC/Leukodepleted RBC/Washed RBC
Irradiated PRBC
CMV Negative
Hypotension and Tachycardia not corrected by volume replacementSymptomatic Anemia; certain hemoglobinpathies, exchangetransfusions. Washed RBC are used for patients with IgA deficienciesand recurrent severe allergic reactions.Radiation destroys the leukocytes to prevent GVHD. Bone marrow/stem cell transplants, leukemias, Hodgkin’s Disease, neonates, directed units for transfusion to a blood relative, donor units selected for HLA compatibility, patients with congenital cellular immunodeficiencyFor CMV negative patients who are immunosuppressed, prior to and after bone marrow/stem cell transplants, and for ALL infants
Common Adverse Reactions: see TAR
Hives, headache, fever, chills, dyspnea, chest pain, shock febrile reaction, circulatory overload, red cell alloimmunization
Tubing/Filter: Primary pump set, blood secondary set (Y type blood set in ER and OR)Rate: Infuse at slow rate during first 15 minutes observation, if no adverse
reaction noted increase rate to infuse within 1½ - 2 ½ hours, not to exceed 4 hoursPeds: Rate per physician order
Assessment andMonitoring: Follow TAR
RN must initiate and stay with the patient for the first 15 minutesAfter the first 15 minutes, RN may delegate to a licensed professional who can monitor the patient.Adult: Vital Signs within 30 minutes prior to transfusion, 15 minutes after
15

NURSING CLINICAL PRACTICE MANUAL Page 16 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
initiation of transfusion and immediate post transfusion.Adult Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.Child/Infant: Vital signs within 30 prior to transfusion, 15 minutes after initiation of transfusion, then hourly and post transfusion.Child Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.
PEDIATRIC indications for transfusion:
All pediatric ages: Signs and symptoms of shock/blood lossPatients greater than 4 months of ageSignificant pre-op anemia in emergency situation (HCT < 30%) or when other corrective therapy is not availableIntraoperative blood loss of >15% of total blood volumeHCT < 24% (in perioperative period with symptoms, chronic congenital or acquired symptomatic anemia)Acute blood loss with hypovolemiaHCT < 40% with severe pulmonary diseaseSickle cell disease (simple or exchange transfusion)Patients less than 4 months of ageHCT < 21% with low recticulocyte count (< 100,000) and symptoms of anemiaHCT < 30%, HCT < 35% depending on hood O2 CPAP/IMV, O2 flow, presence of apnea, tachycardia, bradycardiaExchange transfusion in neonates
16

NURSING CLINICAL PRACTICE MANUAL Page 17 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Random Donor PlateletsWhere obtained: LabCommon Indications: Active bleeding, spontaneous hemorrhage, prevent hemorrhage in prespecified
low platelet counts, CMV (-) platelets used in immune suppressed patients especially after bone marrow transplant.
Common Adverse Reactions: Hives, headache, fever, chills, dyspnea, chest pain, shock, febrile reaction, circulatory overload NOTE: This product has a higher potential for bacterial contamination than refrigerated blood products. TRAILI is a specific concern with plasma products
Tubing/ Filter: Gravity: Blood Y Administration SetRate: As fast as patient can tolerate (less than 4 hours)Assessment and Monitoring: RN must initiate and stay with the patient for the first 15 minutes
After the first 15 minutes, RN may delegate to a licensed professional who can monitor the patient.Adult: Vital Signs within 30 minutes prior to transfusion, 15 minutes after initiation of transfusion and immediate post transfusion.Adult Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.Child/Infant: Vital signs within 30 prior to transfusion, 15 minutes after initiation of transfusion, then hourly and post transfusion.Child Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.
17

NURSING CLINICAL PRACTICE MANUAL Page 18 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Pheresed Platelets Where obtained: LabCommon Indications: Active bleeding, spontaneous hemorrhage, prevent hemorrhage,
prophylactically in ITP patients prior to splenectomy, prophylactically prior to invasive procedure where significant bleeding is anticipated. CMV (-) platelets used in immune suppressed patients especially after bone marrow transplant.Pheresed platelets one donor per treatment1 unit pheresed platelets = approximately 6 random donor platelets
Common Adverse Reactions: Hives, headache, fever, chills, dyspnea, chest pain, shock febrile reaction, circulatory overload
Tubing/Filter: Gravity: Blood Y Administration SetRate: As fast as patient can tolerate (less than 4 hours)Assessment and Monitoring: RN must initiate and stay with the patient for the first 15 minutes
After the first 15 minutes, RN may delegate to a licensed professional who can monitor the patient.Adult: Vital Signs within 30 minutes prior to transfusion, 15 minutes after initiation of transfusion and immediate post transfusion.Adult Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.Child/Infant: Vital signs within 30 prior to transfusion, 15 minutes after initiation of transfusion, then hourly and post transfusion.Child Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.
18

NURSING CLINICAL PRACTICE MANUAL Page 19 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Human Leukocyte Antigen (HLA) Matched Pheresed Platelets, Crossmatched PlateletsWhere obtained: LabCommon Indications: Active bleeding, spontaneous hemorrhage, prevent hemorrhage,
prophylactically in ITP patients prior to splenectomy, prophylactically prior to invasive procedure where significant bleeding is anticipated. CMV (-) platelets used in immune suppressed patients especially after bone marrow transplant. HLA matched Pheresed Platelets = one donor typed specifically to one recipient
Common Adverse Reactions: Hives, headache, fever, chills, dyspnea, chest pain, shock febrile reaction, circulatory overload
Tubing/Filter: Gravity: Blood Y Administration SetRate: As fast as patient can tolerate (less than 4 hours)Assessment and Monitoring: RN must initiate and stay with the patient for the first 15 minutes
After the first 15 minutes, RN may delegate to a licensed professional who can monitor the patient.Adult: Vital Signs within 30 minutes prior to transfusion, 15 minutes after initiation of transfusion and immediate post transfusion.Adult Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.Child/Infant: Vital signs within 30 prior to transfusion, 15 minutes after initiation of transfusion, then hourly and post transfusion.Child Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.
19

NURSING CLINICAL PRACTICE MANUAL Page 20 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Fresh Frozen Plasma (FFP) or Plasma Frozen within 24 hours (FP24) may be substituted. Both products become Thawed Plasma after thawing.
Where obtained: Lab – Notify lab of time needed. Thaw time 20-45 minutesdepending upon the facility equipment. In general, PRMC should have immediate to 20 minute plasma availability, while the other sites have 25-45 minute plasma availability.
Common Indications: Microvascular bleeding, prior to invasive procedure, patients at high risk for bleeding (elevated INR), correction of coagulation factor deficiency when specific concentrate are unavailable,TTPPlasma Exchange
Pediatric: Coagulation factor deficiency, with bleeding prior to invasive surgery, when specific factor replacement is not possibleVitamin K deficiency resulting in a coagulopathy with bleeding or prior to invasive proceduresReplacement therapy in congenital antithrombin III deficiency when specific factor is not possibleElevated PT, PTT for correction of microvascular bleedingFP 24 not recommended for neonates, use FFP only
Common Adverse Reactions: Most common reaction is urticarial. TRAILI is a specific concern with plams products. Circulatory overload
Tubing/ Filter: Gravity: Blood Y Administration SetRate: As fast as patient can tolerate (less than 4 hours)Assessment and Monitoring: RN must initiate and stay with the patient for the first 15 minutes
After the first 15 minutes, RN may delegate to a licensed professional who can monitor the patient.Adult: Vital Signs within 30 minutes prior to transfusion, 15 minutes after initiation of transfusion and immediate post transfusion.Adult Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.Child/Infant: Vital signs within 30 prior to transfusion, 15 minutes after initiation
20

NURSING CLINICAL PRACTICE MANUAL Page 21 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
of transfusion, then hourly and post transfusion.Child Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.
21

NURSING CLINICAL PRACTICE MANUAL Page 22 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Cryoprecipitate/Sryosupernatent-reduced plasmaWhere obtained: Lab
Cryopreciptate: Thaw/pooling time 10-15 minutesSryosupernatant-reduced plasma
Common Indications:Cryopreciptate
Syrosupernatant-reduced plasma
Fibrinogen < 100mg/dl, Factor XII deficiency, Prophylaxis in non-bleeding, perioperative or peripartum patient with congenital fibrinogen deficiencies or Von Willebrands disease when appropriate factor concentrates are not available, active bleeding in patient with von Willebrands Disease when appropriate factor concentrates are not availableTTP Plasma Exchange
Pediatric Von Willebrands disease with bleeding or preoperatively when other replacement factor unavailable, hypofibrinogenemia or dysfibrinogenemia with bleeding or preoperatively, replacement therapy for factor XIII deficiency, mild hemophilia A when factor VIII concentrates unavailable
Common Adverse Reactions: Most common is uticariaTubing/Filter: Gravity: Blood Y Administration SetRate: 1-2 ml/min or 60-120 ml/HR (Less than 4 hours)
Start with NS and flush tubing with NS when infusion completeAssessment and Monitoring: RN must initiate and stay with the patient for the first 15 minutes
After the first 15 minutes, RN may delegate to a licensed professional who can monitor the patient.Adult: Vital Signs within 30 minutes prior to transfusion, 15 minutes after initiation of transfusion and immediate post transfusion.Adult Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.Child/Infant: Vital signs within 30 prior to transfusion, 15 minutes after initiation of transfusion, then hourly and post transfusion.
22

NURSING CLINICAL PRACTICE MANUAL Page 23 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Child Assessments: 0-15 minutes, then every 30 minutes, and 1 hour post transfusion.
23

NURSING CLINICAL PRACTICE MANUAL Page 24 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Rh (Immune Globulin) (RhIG) (Tradename) RhophylacWhere obtained: LabCommon Indications: Rh negative Mom at 28 weeks gestation
Rh negative Mom post partum with Rh positive babyFetal demise assume Rh positive babyRh negative pregnant woman after a traumaTransfusion of Rh incompatible blood or blood products
Common Adverse Reactions: Slight redness, swelling, soreness at sight of injection, slight feverTubing, Filter & Needle: Rh – IM injection or IVAssessment and Monitoring: Routine assessment & monitoring
Volume Expanders: Albumin (5% or 25%)Where obtained: PharmacyCommon Indications: Hypovolemia, hypoalbuminemia, Acute nephrosis / or hemodialysis patients,
burns, hemolytic disease of newbornsCommon Adverse Reactions: Precipitation of CHF, dyspnea, pulmonary edema, fever, nausea, vomitingTubing, Filter & Needle: Comes with own tubing and filter but may use IV standard vented tubingRate: Albumin administration roles vary depending upon indication, present blood
volume, patient response and concentration of solution. Administration rates for infants and children may need to be slower. Check with physician who orders.For 5% solution rate = 2-4 ml/min (may go up to 5-10 ml/min)For 25% solution rate = 1 ml/min (may go up to 2-3 ml/min)
Assessment and Monitoring: Routine Assessment & Monitoring
24

NURSING CLINICAL PRACTICE MANUAL Page 25 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
HextendWhere obtained: PharmacyCommon Indications: Adjunct in the early management of shock or impending shock due to: burns,
hemorrhage, surgery, sepsis, trauma, when fluid replacement and plasma volume expansion are needed.*Special care should be exercised in patients with impaired/renal clearance, since Hextend eliminated by kidneys.
Common Adverse Reactions: Circulatory overload, CHF, vomiting, elevated temp, anaphylactic reactions (shortness of breath, urticaria hives), hypotension, coagulopathics, including DIC, transient prolong bleeding time, headache, peripheral edema
Tubing, Filter & Needle: Standard pump tubingRate: Up to 20 ml/kg per hour (per physician order), total dose not more than
20ml/kg/dayAssessment and Monitoring: Monitor VS every 15 minutes x 4 then every 1 hour x 2; monitor urine output
every hourIf patient experiences anaphylaxis, stop infusion immediately and call physician
Dextran, Dextran 40, L.M.D. 10%Where obtained: PharmacyCommon Indications: Emergency management of hypovolemic shock when more appropriate
products or solutions unavailableTherapy should not exceed 5 days
Common Adverse Reactions: Fever, anaphylactic reactions (shortness of breath, wheezing, urticaria hives, hypotension), nausea, vomiting, bleeding
Tubing, Filter & Needle: Standard pump tubingRate: Per physician order
Dextran 40 – the total daily dose = 20ml/kg – 1st 10ml/kg may be infused rapid bolus with remaining dose slower per physician order
25

NURSING CLINICAL PRACTICE MANUAL Page 26 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Assessment and Monitoring: Monitor VS every 15 minutes x 4 and every hour x 2. Monitor urine output every hour.
Plasma Protein Fraction PPFWhere obtained: Pharmacy
* Note: Cannot be sent through tube stationsCommon Indications: Expansion of plasma volume and to maintain cardiac output in situations
associated with deficiencies in circulatory volume, including: shock, hemorrhage, burns, temporary replacement therapy in edema associated with low plasma proteins such as nephritic syndrome and end stage liver disease.
Common Adverse Reactions: There are no ABO blood group antibodies present; therefore compatibility is not a factor.Hypotension has been associated with rapid infusion of PPF.
Tubing, Filter & Needle: Comes with own tubing and filter, but may use standard IV tubing if ventedDo Not Shake
Rate: Adult: 1-10 ml/min or 60-600 ml/HRNormal blood volume: 1 ml/min (60ml/hr)Shock: 5-10 ml/min (300-600 ml/hr)Hypoproteinemia: Single 500 ml over 1 hour, larger doses – maximum 100 ml/hr
Assessment and Monitoring: Routine assessment and monitoring
26

NURSING CLINICAL PRACTICE MANUAL Page 27 of 29
Policy / Procedure Title:Blood & Blood Component Administration ( Adult and Pediatrics )
Policy Category / Subtopic: Patient Care
Immune Serum GlobulinsWhere obtained: PharmacyCommon Indications: ITP – Idiopathic Thrombocytopenia Purpura
Platelet counts begin to rise in 1-2 days with peak at 7-14 days, effect may last about 30 daysSuppression of Rh isolmmunization in pregnancyPrimary immunodeficiency diseaseKawasaki Syndrome
Common Adverse Reactions: Fatigue, muscle aches, chills, anaphylactic shock, wheezing, hypotension, fever, fainting, headache, chest tightness, back/hip pain, hives, nausea, vomitingIn ITP: destruction of red blood cells resulting in decreased Hgb
Tubing, Filter & Needle: Standard IV tubing and filterMay use IV pump at 0.6ml/kg/hr and can gradually increase to 2.4 mg/kg/hr If no reaction
Rate: Start slow at recommendations for administration rate vary according to rand of IV immune globulin being used. For example, Gammagard: 0.5 ml/kg/hr up to 4 ml/kg/hr. Gammagard Liquid: 0.5 ml/kg/hr up to 5 ml/kg/hr. Privigen: 0.3 ml/kg/hr up to 4.8ml/kg/hr. Carimune: 30 ml/hr up to 150 ml/hr.Neonates/Peds rate per physician order .01 ml/kg per minute.
Assessment and Monitoring: BP, P&R every 15 minutes x 4 and every 1 hour until infused.If there is a reaction, stop infusion immediately and call the physician
27

Antihemophilic Factor RecombinateWhere obtained: PharmacyCommon Indications: Hemophilia A related bleeding with factor VIII
deficiency (prevention & control of bleeding)Common Adverse Reactions:
Flushing, nausea, fever, chills, fatigue, nose bleed, hives
Tubing, Filter & Needle: Standard IV tubingFilter needle to remove from vial
Rate: IVP (no faster than 10ml/min)Assessment and Monitoring:
Heart rate, blood pressure, AHF levels, bleeding, development of VIII inhibitors
Humate- P Antihemophilic Factor / Von Willeband Factor Complex (Human)
Where obtained: PharmacyCommon Indications: Treatment & prevention of bleeding in hemophilia A
Treatment of spontaneous & trauma bleeding in severe Von Willeband disease
Common Adverse Reactions:
Fever, chills, phlebitis, vasodilation
Tubing, Filter & Needle: Standard IV tubingRate: IVP (no faster than 4 ml/min)Assessment and Monitoring:
Heart rate, blood pressure, Hct, signs & symptoms of hemolysis, bleeding, AHF levels
Coagulation Factor IX Benefix (Recombinant)Where obtained: PharmacyCommon Indications: Control & prevention of bleeding associated with
hemophilia BCommon Adverse Reactions:
Nausea, altered taste, burning, sensation in jaw, headache, fever, chills, fatigue
Tubing, Filter & Needle: Standard IV tubingFilter needle to remove from vial
Rate: IVP over several minutesAssessment and Monitoring:
Factor IX levels, aPT
Recombinant Coagulation Factor VIIa Novo SevenWhere obtained: PharmacyCommon Indications: Hemophilia A or B related bleeding in patients with
inhibitors to Factor VIII or IXCommon Adverse Reactions:
Hypertension, hemorrhage, low plasma fibrinogen, fever
Tubing, Filter & Needle: Standard IV tubingRate: IVP over 2-5 minutesAssessment and Monitoring:
Signs & symptoms of activation of coagulation system or thrombosis, aPT, PT, factor VII, clotting activity

REFERENCES:
AABB (2012). Standards for blood banks and transfusion services. (28th ed.).
Bethesda, MD: AABB.
AABB (2009). Circular of information. (2009 rev.). Retrieved from website
http://www.aabb.org/resources/bct/Documents/coi0809r.pdf
Infusion nursing standards of practice [Supplemental material]. (2011,
January/February). Journal of Infusion Nursing, 34(1S), S93-S94.
Parkview Health. (2011, January). Consent for treatment: Informed consent for surgery
invasive procedures and administration of blood or blood products (Policy).
Retrieved from Team.Parkview website: http://team.parkview.com
Roback, J.D. (Ed). (2011). AABB Technical Manual (17th ed.). Bethesda, MA:
AABB.
Smiths Medical. (2008). Blood & fluid warming systems (Level 1®). In Operator’s
manual. Retrieved from
http://www.smiths-medical.com/catalog/fluid-warming/fast-flow/hardware/level-1-
h-1200.html
Origination Date: 6/13 Original Source: Nursing Professional Practice Committee
Revision Source:Review/Revision Date: Authorized By:6/13 PHH – Linda Prus, Director of Patient Services
PLH – Jordi Disler, VP Patient CarePNH – Cathy Byrd, VP Patient Care
6/13 POH –Laura Ferrell, DON6/13 PWH – Bridget Johnson, VP Patient Care6/13 PRMC/PVH - Judy Boerger, Sr. VP, CNO
PBH – Sally Boyce, Director of Nursing