Embed Size (px)
Citation preview
Policy Brief 4
Issued September 2014
Prevention
policyin other
areas

Policy Brief | Prevention Policy, Strategy and Practice 2
This policy brief describes different disciplinary approaches to prevention, and draws insights from successful prevention initiatives in other fields.
Key points
‒ Prevention policy, strategy and practice is approached differently in public health, criminology and other sociological fields, but they also share many commonalities.
‒ The public health approach has been significant in the field of prevention of violence against women and children, in particular for its conceptualisation of the multi faceted nature of violence.
‒ Learnings can be drawn from successful initiatives in other fields, such as promotion of road safety, chronic disease prevention, or mother-to-child transmission of HIV.
Prevention Policy, Strategy and Practice
Preventionpolicy, strategy
andpracticeWhat do we mean by prevention?
While the concept of prevention is defined differently across health, criminology and other sociological fields, all disciplines adopt a three-level approach to conceptualising prevention: primary, secondary and tertiary. Most sociological definitions of prevention draw on a public health approach to prevention, which has been adapted to a range of contexts, including violence prevention.
Policy Brief | The Public Health Approach to Prevention 3
The Public Health Approach to Prevention
The distinctions between primary, secondary and tertiary prevention are described in Policy Brief 1: Key terms, definitions and statistics. This public health approach assumes that violence can be eliminated, with the 2002 World Health Organisation’s (WHO) World Report on Violence and Health suggesting that violence ‘is not an intractable social problem or an inevitable part of the human condition’ but rather ‘the product of complex, yet modifiable social and environmental factors’. The seeds for the public health approach to prevention were sown at an international conference seeking a new, global public health movement held in Canada in 1986. This led to a broader focus for public health – from individual behaviours and risk factors, to population-level issues such as poverty and education.
In 2013, WHO further articulated the public health approach to prevention in Trade, foreign policy, diplomacy and health: Public Health. WHO described the approach as: ‘all organized measures (whether public or private) to prevent disease, promote health, and prolong life among the population as a whole, noting that this entails concern ‘with the total system and not only the eradication of a particular disease’.
The 2006 Australian National Public Health Partnership’s (NPHP) The Language of Prevention noted that the public health approach to prevention generates actions targeting the reduction, onset, causes, complications or recurrence of a social problem or disease. More specifically, the 2009 Trust for America’s Health study Prevention for a Healthier America: Investments in Disease Prevention Yield Significant Savings, Stronger Communities, defined primary prevention as the actions required to reduce or eliminate a problem from arising in the first place, as opposed to ‘treating or alleviating the consequences’.
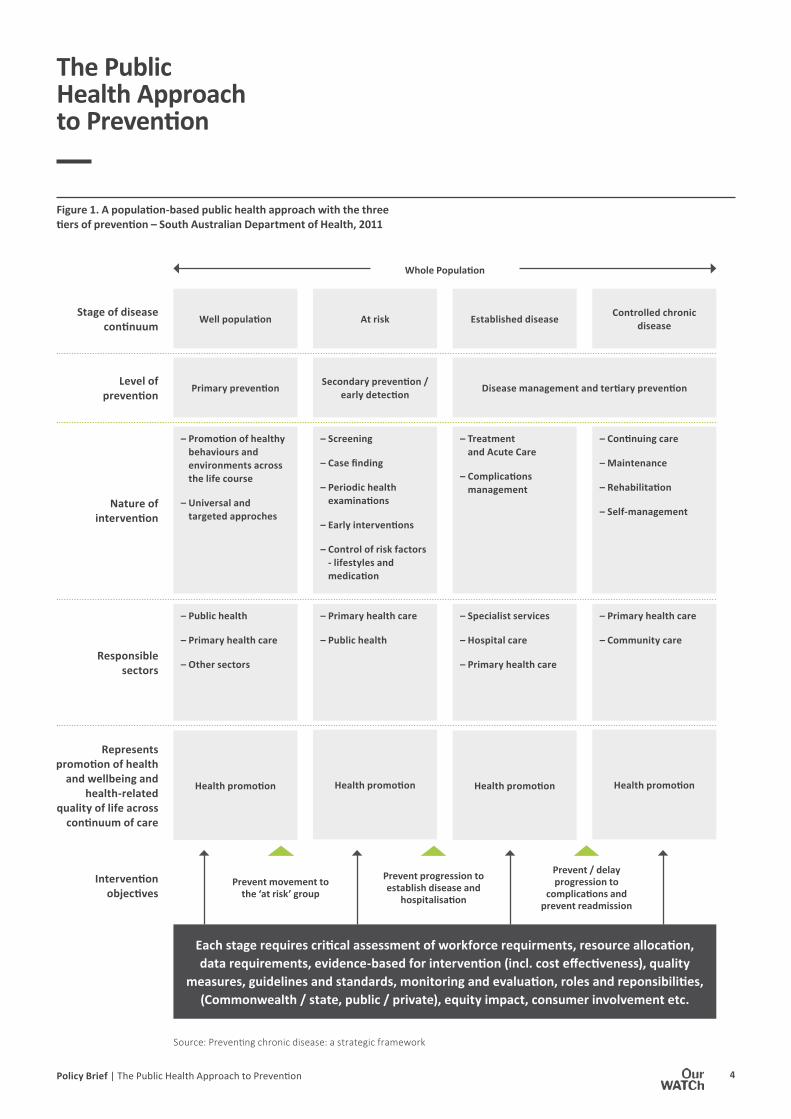
Figure 1 shows an Australian public health-based example of the prevention continuum from primary to tertiary intervention with differing target populations, at each stage and the different activities or interventions targeting each stage.
This public health approach assumes that violence can be eliminated, suggesting that violence ‘is not an intractable social problem or an inevitable part of the human condition’ but rather ‘the product of complex, yet modifiable social and environmental factors’.
Policy Brief | The Public Health Approach to Prevention 4
Each stage requires critical assessment of workforce requirments, resource allocation, data requirements, evidence-based for intervention (incl. cost effectiveness), quality
measures, guidelines and standards, monitoring and evaluation, roles and reponsibilities, (Commonwealth / state, public / private), equity impact, consumer involvement etc.
– Public health
– Primary health care
– Other sectors
Well population
– Promotion of healthy behaviours and environments across the life course
– Universal and targeted approches
Primary prevention
Health promotion
– Specialist services
– Hospital care
– Primary health care
Established disease
– Treatment and Acute Care
– Complications management
Disease management and tertiary prevention
Health promotion
– Primary health care
– Public health
At risk
– Screening
– Case finding
– Periodic health examinations
– Early interventions
– Control of risk factors - lifestyles and medication
Secondary prevention / early detection
Health promotion
– Primary health care
– Community care
Controlled chronic disease
– Continuing care
– Maintenance
– Rehabilitation
– Self-management
Health promotion
Prevent movement to the ‘at risk’ group
Source: Preventing chronic disease: a strategic framework
Stage of disease continuum
Level of prevention
Nature of intervention
Responsible sectors
Intervention objectives
Represents promotion of health
and wellbeing and health-related
quality of life across continuum of care
Prevent progression to establish disease and
hospitalisation
Whole Population
Prevent / delay progression to
complications and prevent readmission
Figure 1. A population-based public health approach with the three tiers of prevention – South Australian Department of Health, 2011
The Public Health Approach to Prevention
Policy Brief | The Public Health Approach to Prevention 5
Public health approaches to prevention have been adapted to prevention of violence generally, and to prevention of violence against women and their children specifically. The latter is discussed in Policy Brief 3: The international evidence base.
Prevention of violence generally through a public health model was established in the 2002 WHO World Report on Violence and Health. It noted that the public health approach does not replace criminal justice and human rights responses to violence; rather, it complements their activities and offers them additional tools and sources of collaboration.
The Report argued that violence prevention initiatives should be founded upon scientific, evidenced-based approaches that involve identifying contributing or risk factors for violence perpetration or victimisation, and developing reinforcing strategies to address these factors in a systemic and sustained way. This could include legislative reform, social marketing campaigns and educational programs. Evaluation is critical to the public health approach, which also aims to improve understandings, test hypotheses and build further evidence over time. It has already provided practical frameworks for preventing violence, and evidence-based advocacy to government, philanthropic and other stakeholders.
The Report reinforced the ‘socio-ecological model’ for understanding the multi-faceted nature of violence (described in further detail in Policy Briefs 2 and 3). It emphasised that creating safe and healthy communities around the globe requires commitment on the part of multiple sectors at the international, national and community levels to:
‒ document the problem
‒ build the knowledge base
‒ promote the design and testing of prevention programs
‒ promote the dissemination of lessons learned.
The Report postulated that a scientific, evidence-based public heath approach to prevention of violence can lead to significant reductions in incidence and prevalence. Violence can be reduced and prevented in much the same way as has occurred with road traffic accidents, chronic disease or HIV/AIDS – and these examples are described below.
The Public Health Approach to Prevention
Policy Brief | The Criminological Approach to Prevention 6
The criminological approach to prevention of violence contrasts to the public health approach in that most analyses assume that a base level of violent crime will always exist in society and cannot be eradicated. It does, however, assume that crime can be significantly reduced, with the Australian Institute of Criminology (AIC) 2003 study Approaches to Understanding Crime Prevention describing crime prevention as ‘any action that causes a reduction in the level of criminal activity and the resulting harm, or in the number of criminal offenders and their victims’.
The Australian and New Zealand Crime Prevention Senior Officers’ Group defined primary prevention in the 2011 National Crime Prevention Framework as the strategies and measures that seek to reduce the risk of crimes occurring, and their potential harmful effects on individuals and society, including fear of crime, by intervening to influence their multiple causes.
The criminological approach to primary prevention therefore shares a common aim with the public health approach: to stop future occurrences of violence before they happen. The broad goal of primary crime prevention activities is to reduce opportunities for crime and/or strengthen community or social structures. This goal can be achieved in two different ways:
‒ Situational crime prevention measures – designed to minimise the environmental factors that enable the commission of crime, such as street lighting or alarm systems, but not seeking to address the underlying causes of crime.
‒ Social crime prevention measures – directly targeting offenders and potential offenders. The AIC study describes the factors that influence an individual’s likelihood of committing a crime as, for example, mental health concerns and conditions or past histories of trauma that impact a person’s capacity for empathy.
The Criminological Approach to Prevention
The criminological approach to primary prevention shares a common aim with the public health approach: to stop future occurrences of violence before they happen.
Policy Brief | Examples of Successful Primary Prevention from other Fields 7
In 2003, six American universities collaborated in a review of studies across four areas – juvenile delinquency and violence, substance abuse, risky sexual behaviour, and school failure – to identify characteristics consistently associated with effective prevention programs. In What Works in Prevention: Principles of Effective Prevention Programs, the authors concluded that programs evaluated as successful across all fields consistently:
‒ demonstrated comprehensiveness
‒ included varied teaching methods
‒ provided for sufficient frequency and duration
‒ were driven by evidence-based theories
‒ provided opportunities for positive relationships
‒ matched to the target group, so appropriately timed and culturally relevant
‒ included outcome evaluations
‒ involved well trained staff.
Chronic disease – the 5 A’s
Primary prevention has been distilled into a step-by-step formulation for prevention of chronic disease that has achieved major reductions in illness prevalence (such as the occurrence of smoking-related diseases). This approach is called the ‘5 As’ and is described in The Role of Australian Primary Health Care in Preventing Chronic Disease, a study for the Australian National Health Preventative Agency. It has been widely adopted internationally in addressing the behavioural risk factors that lead to disease development in the first place:
1. Ask Systematic identification
2. Assess Multiple risk, readiness to change, understanding of the issue
3. Advise/ Tailored information, motivational interviewing, goal setting
4. Assist Referral to intensive interventions
5. Arrange Follow up, maintenance
Examples of Successful Primary Prevention from other Fields
Agree
Best practice of primary prevention from other fields have been reviewed to see how they achieved positive outcomes through their findings and evidence based methods.

Policy Brief | Examples of Successful Primary Prevention from other Fields 8
Road safety
In 2004, WHO called for a public health prevention approach to reduce road traffic accidents in Europe. The evidence for adopting a primary prevention approach suggested that identifying risk factors and countermeasures at each stage from pre-crash to post-crash provided the optimal way to achieve a reduction.
WHO used the Haddon Matrix (a model applied to injury prevention and response strategies (see Figure 2 below) to show that risk factors identified at the pre-crash phase correspond with those factors that would be identified using a primary prevention approach. Further analysis of the most significant risk factor at this phase identified the ‘environmental’ aspect of speed. The WHO report Preventing Road Traffic Injury: A Public Health Perspective for Europe (2005) noted that intervention activity focused on this single element alone reaped some of the highest reductions in incidence and prevalence of road traffic accidents in Europe.
Figure 2. The Haddon Matrix from report on road traffic injury in Europe for WHO (2005)
FactorsPhase Human Vehicles and equipment Environment
Pre-crash Crash prevention
Information Attitudes Impairment Police enforcement
Roadworthiness Lighting Braking Handling Speed management
Road design and road lay out Speed limits Pedestrian facilities
Crash Injury prevention during the crash
Use of restraints Impairment
Occupant restraints Other safety devices Crash-protective design
Crash-protective roadside objects
Post-crash Life sustaining
First aid skill Access to medics
Ease of access Fire risk
Rescue facilities Congestion
Examples of Successful Primary Prevention from other Fields

Policy Brief | Examples of Successful Primary Prevention from other Fields 9
Mother-to-child transmission of HIV
The 2002 report Prevention of HIV in Infants and Young Children: Review of WHO activities was based on the evidence that avoiding infection in women prevents HIV transmission to infants and young children. It recommended that in high-risk contexts, HIV prevention programs be directed at a broad range of women at risk and their partners, with a particular effort required to reach young people.
WHO and UNICEF implemented prevention programs targeting education and preventative initiatives to women and different groups across communities. These programs achieved a significant reduction in the incidence and prevalence of the illness among those populations. In Thailand, between 1997 and 2001, paediatric cases of AIDS declined from over three per cent to less than 0.5 per cent.
The United Nations Population Fund 2008 Annual Report identified a major obstacle in achieving primary prevention of this illness as the inadequate engagement of male partners for practicing safer sex. They noted the concurrent need to work at preventing violence against women, and gain the support of male partners, demonstrating the importance of multi-faceted prevention.
Initiatives tailored to specific communities
Tailored approaches may be required for primary prevention policies, programs and services for demographic groups experiencing intersecting forms of disadvantage and discrimination, or who are harder to reach with initiatives aimed at the whole population, such as:
‒ culturally and linguistically diverse (CALD) communities
‒ Aboriginal and Torres Strait Islander (ATSI) communities
‒ people with a disability
‒ lesbian, gay, bisexual, transgender, intergender and queer (LGBTIQ) communities.
Some of the reasons for tailoring initiatives to particular groups include lack of access to appropriate programs or services, environmental factors, or isolation from mainstream settings. Risk factors can be higher, and control of these factors can be lower in communities affected by broader discrimination and disadvantage than in the population as a whole. This was demonstrated, for example, in the 2012 American Heart Association study Behavioural Strategies for Cardiovascular Risk Reduction in Diverse and Under-Served Racial/Ethnic Groups.
Techniques to implement effective primary prevention in specific communities are highly dependent upon the context, and aspects prohibiting control of risk factors. There is no single set of principles, however a stronger evidence base would help build effective primary prevention approaches for these communities.
For example, strategies to develop and implement health promotional initiatives in Aboriginal and Torres Strait Islander communities have incorporated community development principles. The 2002 Sydney Consensus Statement on Principles for Better Practice in Aboriginal Health Promotion describes these principles as:
‒ acknowledging Aboriginal cultural influences and the historical, social and cultural context of communities
‒ practice being based on available evidence and designed to build capacity in the community, government, service systems, organisations and the workforce
‒ equitable resource allocation (including flexible purchaser-provider arrangements), cultural security and respect in the workplace
‒ ongoing community involvement and consultation.
Examples of Successful Primary Prevention from other Fields
Policy Brief | References 10
Australian and New Zealand Crime Prevention Senior Officers’ Group (2011), National Crime Prevention Framework, prepared by the Australian Institute of Criminology, Canberra.
Australian Institute of Criminology (2003), ‘Approaches to Understanding Crime Prevention’ in AICrime Reduction Matters, 20 May 2003, Canberra.
Bellefontaine, T (2011), ‘Evaluating Place-Based Approaches: A Window of Opportunity?’ in Policy Insight, Policy Horizons Canada (Government of Canada).
Centre for Disease Control (2009), The Social-Ecological Model: A Framework for Prevention, available at: http://www.cdc.gov/violenceprevention/overview/social-ecologicalmodel.html
Collins, L and Dupe, A (2011), Preventing HIV and Unintended Pregnancies: Strategic Framework 2011-2015, UN Population Fund, World Health Organisation and UNICEF, Geneva.
Harris, M and Lloyd, J (2012), The Role of Australian Primary Health Care in Preventing Chronic Disease, Centre for Primary Health Care and Equity, University of NSW for the Australian National Health Preventative Agency, Canberra.
Kumpfer, KL and Baxley, GB (1997), Drug abuse prevention: What works, National Institute on Drug Abuse, Rockville.
Multicultural Centre for Women’s Health (2011), On Her Way: Primary prevention of violence against immigrant and refugee women in Australia, prepared by Carolyn Poljski, Melbourne.
National Public Health Partnership (2006), The Language of Prevention, Melbourne.
Nation, M, Crusto, C, Wandersman, A, Kumpfer, KL, Seybolt, D, Morrissey-Kane, E and Davino, K (2003), ‘What Works in Prevention: Principles of Effective Prevention Programs,’ in American Psychologist, June/July 2003, pp.449-456.
National Aboriginal Community Controlled Health Organisation (ed), ‘Health Promotion and Prevention,’ available at: http://www.naccho.org.au/aboriginal-health/health-promotion-and-prevention/#fnl-4
References
Racioppi, F, Eriksson, L, Tingval, C and Villaveces, A (2005) Preventing Road Traffic Injury: A Public Health Perspective for Europe, World Health Organisation, Geneva.
South Australia Department of Health (2011), Primary Prevention Plan 2011-2016, Government of South Australia, Adelaide.
Stuart-Shor, E, Berra, K, Kamau, M and Kumanyika, S (2012), ‘Behavioral Strategies for Cardiovascular Risk Reduction in Diverse and Underserved Racial/Ethnic Groups’ in Recent Advances in Preventive Cardiology and Lifestyle Medicine, 2012; 125, pp.171-184.
Trust for America’s Health (2009), ‘Prevention for a Healthier America: Investments in Disease Prevention Yield Significant Savings, Stronger Communities,’ in Preventing Epidemics, Protecting People, February 2009.
US National Library (2009), National Institutes of Health, Medical Subject Headings: http://www.nlm.nih.gov/mesh/
World Health Organisation (2002), World Report on Violence and Health: http://www.who.int/violence_injury_prevention/violence/world_report/en/
World Health Organisation (2002), Prevention of HIV in Infants and Young Children: Review of the WHO’s activities: http://www.who.int/hiv/pub/mtct/en/hiv_2002_08_en.pdf
World Health Organisation (2013), Trade, foreign policy, diplomacy and health: Public health: http://www.who.int/trade/glossary/story076/en/#.Uk95Y064LFk.gmail

Policy Brief | About Our Watch 11
About Our Watch
Our Watch has four members: the Commonwealth, Victorian, Northern Territory and South Australian Governments. Remaining states and territories have been invited to join as members.
Since its incorporation, Our Watch has commissioned a series of policy briefs to assist in the development of the strategic program. The briefs are not designed to be comprehensive or definitive, but rather to provide a ‘point in time’ summary of issues and evidence in particular areas. They will be published progressively over the next 6 months, and available at ourwatch.org.au.
Our Watch is an independent, not-for-profit organisation, working to raise awareness and engage the community in action to prevent violence against women and their children.