Embed Size (px)
Citation preview

Policy At A Glance: April 2018 INSTITUTE FOR HEALTH POLICY AND LEADERSHIP
2/16/18 AB 3087 introduced as Health Facilities: Data Reporting
4/24/18 AB 3087 scheduled to be heard in the Assembly Health Committee
7/1/19 AB 3087 will go into effect if enacted
History
California Health Care Cost, Quality, and Equity Commission (AB 3087)
What is Assembly Bill 3087? Assemblymember Ash Kalra (D - San Jose) introduced Assembly Bill (AB) 3087, California Health Care Cost, Quality and Equity Commission (also known as “the Health Care Price Relief Act”). If enacted, AB 3087 would create an independent state agency called the California Health Care Cost, Quality and Equity Commission (“the Commission”). The Commission will have two major tasks1:
• Set payment rates for health plans, hospitals, physicians, physician groups, laboratories, imaging centers and other care providers including dentists
• Control in-state health care costs by setting a global cap on health care spending
The new payment rate will apply to all commercial health plans in California, including CalPERS (California Public Employee’s Retirement System), which manages the pension and health benefits for California’s public employees and their families. AB 3087 does not apply to federal or state financed health insurance programs such as Medicare, Medicaid, and the Federal Employees Health Benefit Program. This policy brief provides an initial assessment of AB 3087 as it stands today.
Bringing wholeness to individuals and communities, the Institute for Health Policy and Leadership (IHPL) strives to integrate health policy research and education with
leadership development. Our goal is to improve the health of our communities by building on our strong heritage of health promotion and disease prevention.
To learn more, visit us at www.IHPL.llu.edu
Assembly Bill 3087 proposes to establish an independent state commission that will regulate health care costs by setting prices for hospitals, physicians, physician groups, health plans, and others.
4/9/18 AB 3087 amended as California Health Care Cost, Quality and Equity Commission

2
INSTITUTE FOR HEALTH POLICY AND LEADERSHIP April 2018
1
Why was AB 3087 introduced?
The author cites four reasons for introducing AB 3087:1
• The United States spends more on private health care coverage than other Organization for Economic Cooperation and Development (OECD) countries
• Higher U.S. health care costs do not translate into better quality of health care services or longer life expectancy
• The main driver of high U.S. health care spending is high prices
• Hospital prices for the same procedure vary by a factor of three across all markets and by a factor of two within individual markets
The intent of AB 3087 is to “regulate the cost of health care by regulating health prices for health plans, hospitals, physicians, physician groups, and other health care cost drivers.”1
What will the Commission look like?
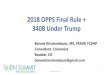
The Commission will be composed of nine members who will meet quarterly and publish reports annually. Of the nine members, one must be the Secretary of California Health and Human Services and another a CalPERS representative. The other seven members (see Figure 1) will have staggered six-year terms and will be appointed by the Governor, the Senate pro tempore and the Assembly Speaker.
2
Figure 1: Composition of the Commission
AB 3087 specifically prohibits health care providers, hospitals, clinics, and pharmaceutical manufacturers from serving in the Commission. These stakeholders may instead participate in a 15-member advisory committee convened by the Commission with appointments of at least one year.
How will the Commission set payment rates for providers?
Beginning on July 1, 2019, AB 3087 requires the Commission to set “base amounts” that health care entities are required to accept as full payment for health care services.
For health care providers, the base amount will be a percentage of Medicare rates, not lower than 100 percent of Medicare rates.

3
INSTITUTE FOR HEALTH POLICY AND LEADERSHIP April 2018
1
For health plans, the base amount will be a multiplier of Medicare Advantage’s capitated rate, which will be adjusted for age, risk mix, and other actuarial factors.
In determining the base amounts, the Commission will:
• Allow different payments rates for different health care providers and health plans
• Examine the provider’s financial status, changes in state or federal laws that can change costs, increase in labor costs, increase in capital investments, and changes in delivery of care
• Establish its own payment rate for pediatrics, obstetrics, gynecology, and other services not reimbursed or rarely reimbursed by Medicare or Medicare Advantage
• Consider underserved or rural areas separately and adjust the base amounts for services provided in these areas
The Commission will not include Medicare rating factors such as Medicare Disproportionate Share Hospitals (DSH) rates, graduate medical education, and readmission penalties into the base amount until the Commission determines whether to include or alter these factors.
2
Can health care entities appeal to adjust their base amounts?
AB 3087 requires the Commission to establish an appeals process by July 1, 2019. Readjustment to the base amounts will depend on the health entity’s financial condition, justifiable differences in costs, and unanticipated events that increase costs such as natural disasters or disease outbreaks among other factors. A provider has justifiable differences in costs when it offers a service unavailable from other providers in the region or provides care in rural or medically underserved areas.
How will the Commission set a global cap for health care?
Details are not available at this time. The Commission will use the gross state product to set a global cap for California’s total health care expenditures. If appropriate data does not exist, the commission will collect sufficient data to assess the cost of health care, as well as its impacts on quality, equity, and workforce adequacy.
Who supports AB 3087?
This bill is co-sponsored by Health Access California and the California Labor Federation. Some patient advocates and labor groups such as Service Employees International Union (SEIU) California also support AB 3087.

4
INSTITUTE FOR HEALTH POLICY AND LEADERSHIP April 2018
Union leaders support AB 3087 because growing health care costs “cut into the take-home pay their workers receive.”2
Who opposes AB 3087?
The California Hospital Association, the California Medical Association, the California Dental Association, and the California Society of Anesthesiologists oppose AB 3087. Although the California Association of Health Plans has not taken an official position, it opposes government price control regulations. The California Nurses Association supported last year’s single-payer legislation (SB 562). But they oppose AB 3087 for having too limited a scope, observing that AB 3087 is a “piecemeal approach.”6
The California Hospital Association estimates that hospitals will lose at least $18 billion in the first year in revenue if AB 3087 goes into effect and it will cost 175,000 health care worker jobs.3 The California Hospital Association also warns that AB 3087 will drive physicians out of California, exacerbating the problem of physician shortage.
Is AB 3087 similar to Maryland’s All-Payer Payment Model?
Some reports contend that AB 3087 follows the lead of Maryland’s “all payer” model.2,4,5 Maryland’s model is similar to AB 3087 in that a state commission directly sets the rates for procedures at all of its hospitals (it does not set rates for any other health entity). However, Maryland’s model is different in that the state sets hospital rates for all payers, including Medicare. References
1. https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201720180AB3087
2. http://www.latimes.com/politics/la-pol-ca-california-healthcare-price-control-bill-20180409-story.html
3. https://www.calhospital.org/sites/main/files/file-attachments/california_hospitals_overwhelmingly_oppose_ab_3087_4918.pdf
4. https://californiahealthline.org/news/california-aims-to-tackle-health-care-prices-in-novel-rate-setting-proposal/
5. https://decisionresourcesgroup.com/drg-blog/health-reform/california-bill-cap-hospital-prices/
6. http://www.capradio.org/articles/2018/04/09/should-california-regulate-cost-of-health-care-services-proposed-new-law-would-put-state-in-charge-of-pricing/
Did you know?
11209 Anderson Street Loma Linda, CA 92354
Phone: 909-558-7022 Fax: 909-558-5638
www.IHPL.llu.edu
Questions? Please contact Helen Jung, DrPH, MPH. Senior Health Policy Analyst at the Institute for Health Policy & Leadership ([email protected])
AB 3087 is now headed to the Assembly Health Committee where testimony in support or opposition to the bill will be heard. A majority vote is needed for AB 3087 to pass
out of the Assembly Health Committee and move to the Assembly Appropriations
Committee.