Embed Size (px)
Citation preview

Poison Control Centres Monica Durigon
Field Epidemiologist Public Health Agency of Canada
Joanne Stares
Public Health Officer Public Health Agency of Canada
Placement site: BC Centre for Disease Control
Environmental Health Services
Environmental Health Surveillance Workshop Ottawa, Ontario
Feb 26, 2013
1

Poison Control Centres Receive calls from the general public and health care
professionals
Manage and respond to poisoning-related inquiries and exposures
Offer interactive service enabling rapid contact, assessment and early intervention
Staffed by health care professionals specially trained in the area of toxicology pharmacists nurses physicians
2

Established use Offer: direct patient care provision of information public and health care
provider education Receive: reports of suspected or
known exposures
3

Classic surveillance cycle
Data collection
Integration
Analysis and Interpretation Dissemination
Action
4

Data collection Basic demographic information
Geographic information caller site exposure site
Substances pharmaceutical and non-pharmaceutical
Exposure calls reason: intentional/unintentional/adverse/unknown routes: dermal/inhalation/ocular/ingestion/parenteral/bite/sting management site: health-care facility/on site
5

Data collection Treatment
Outcomes no effect/minor effect/moderate effect/major effect/death/no follow-up
Information-only calls
6

7

Classic surveillance cycle
Data collection
Integration
Analysis and Interpretation Dissemination
Action
8

Integration – United States National Poison Data System (NPDS)
developed by the American Association of Poison Control Centres (AAPCC)
data repository for all US poison control centres 2009: 61 participating centres services the entire US population anomalies or deviations from established baseline data generate an
automated e-mail alert
Centres can also carry out their own activities independent of the NPDS
9

Integration – Europe France:
10 poison control centres and 3 toxicovigilance centres toxicovigilance network coordinated by the French Institute for Public
Health Surveillance
some poisonings (carbon monoxide and lead) are registered and followed-up at a national level
Germany: 9 poison control centres strong legislation and links to industry
poisonings are reported to a surveillance unit at the Federal Institute for Risk Assessment (Berlin)
10

Classic surveillance cycle
Data collection
Integration
Analysis and Interpretation Dissemination
Action
11

Analysis and interpretation Detect and monitor the emergence of trends and/or novel real-
time incidents in: drug and substance abuse food-borne illness mass poisoning food/medication contamination adverse drug reactions injuries from commercial and consumer products paediatric poisoning
12

Classic surveillance cycle
Data collection
Integration
Analysis and Interpretation Dissemination
Action
13

Dissemination Provide key information to:
regulatory agencies consumer product and safety commissions drug and law enforcement agencies food and drug administration or their counterparts chemical and industry partners public health
14

Classic surveillance cycle
Data collection
Integration
Analysis and Interpretation Dissemination
Action
15

Information for action Implement prevention and control measures
Identify areas for research
Recall consumer products
Influence policy and program planning
16

17
Name Location
Provinces Served
Services Offered
Approximate annual call
volume
Primary data collection tool
Drug and Poison Information Centre
(DPIC) Vancouver, BC
Est. 1975
British Columbia & Yukon
Poison: 24/7 Drug: 9-16
Mon-Fri
36,000 All services
Electronic (since October 2011)
Poison and Drug Information Service
(PADIS) Calgary, AB Est. 1986
Alberta, Saskatchewan & Northwest Territories
Poison: 24/7 Drug: 8-16:15
Mon-Fri Herbal and Medication
Line: 24/7
40,000 All services Paper -based
Ontario Poison Centre Toronto, ON
Est. 1979 Ontario & Manitoba* Poison: 24/7 58,000 Electronic
(since 1997)
Centre Antipoison du Quebec
Quebec City, QC Est. 1986
Quebec Poison: 24/7 45,000 Paper-based
IWK Regional Poison Centre
Halifax, NS Est. 1993
Nova Scotia & Prince Edward Island Poison: 24/7 10,000 Electronic
(since 2006)
*as of July 1, 2012 New Brunswick = 24 hr nurse hotline Newfoundland and Labrador = associated with Janeway Children’s Health and Rehabilitation Centre in St. John’s
Poison Control Centres – Canada, 2013

British Columbia Drug and Poison Information Centre
24/7
Staffed by nurses/pharmacists and supported by medical toxicologists
Located within BCCDC
Oct 2011 – electronic client database
Vancouver
18

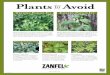
Detection of emerging health events – Fukushima
19
0
2
4
6
8
10
12
Mar
ch 1
1,20
11
Mar
ch 1
2,20
11
Mar
ch 1
3,20
11
Mar
ch 1
4,20
11
Mar
ch 1
5,20
11
Mar
ch 1
6,20
11
Mar
ch 1
7,20
11
Mar
ch 1
8,20
11
Mar
ch 1
9,20
11
Mar
ch 2
0,20
11
Mar
ch 2
1,20
11
Mar
ch 2
2,20
11
Mar
ch 2
3,20
11
Mar
ch 2
4,20
11
Mar
ch 2
5,20
11
Mar
ch 2
6,20
11
Mar
ch 2
7,20
11
Mar
ch 2
8,20
11
Mar
ch 2
9,20
11
Mar
ch 3
0,20
11
Mar
ch 3
1,20
11
Calls
Fukushima related calls to both the BC drug line and drug and poison
information line March 11-31, 2011
Drug and Poison Line Drug Line

Monitor trends and identify emerging health events: CO British Columbia
no current measures to monitor or report CO poisonings
Objective evaluate the utility of DPIC electronic client call records for the
surveillance of unintentional, non-fire related CO poisonings in BC
Specifically Data extraction algorithm enabling accurate detection of CO cases System to routinely monitor for CO aberrations
20

Potential to inform policy – Cosmetic pesticides Between 2003 and 2012, 41 municipalities in BC adopted bylaws prohibiting or restricting the use of cosmetic pesticides
20 banned 21 restricted 119 had no bylaws
Can compare historical DPIC data from 2003-2004 with data collected in 2012
Compare occurrence of exposure calls between municipalities where use is prohibited, restricted, or that have no bylaw
Compare occurrence of exposure calls before and after adoption of cosmetic pesticide bylaw
Examine demographic characteristics of individuals exposed
21

Data limitations Self reporting
External validity
Lack of coordination with public health and its partners
Data linkages not easily done
Data coding practices
In Canada, in particular, some centres use paper records
22

Future considerations Joint surveillance network
Highlight the value of the information found in poison control centre databases
Closer links with public health and its partners
Integrate with other data sources
Ensure consistency across centres regarding data coding practices and standards
23

24