Embed Size (px)
Citation preview
OonaPa
ru
FR
a
Journal of the American College of Cardiology Vol. 52, No. 14, 2008© 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00P
CLINICAL RESEARCH Interventional Cardiology
Point-of-Care Measurement of ClopidogrelResponsiveness Predicts Clinical Outcome inPatients Undergoing Percutaneous Coronary InterventionResults of the ARMYDA-PRO (Antiplatelettherapy for Reduction of MYocardial Damage duringAngioplasty-Platelet Reactivity Predicts Outcome) Study
Giuseppe Patti, MD, FACC, Annunziata Nusca, MD, Fabio Mangiacapra, MD, Laura Gatto, MD,Andrea D’Ambrosio, MD, Germano Di Sciascio, MD, FACC
Rome, Italy
Objectives The aim of this study was to evaluate the correlation of point-of-care measurement of platelet inhibition withclinical outcome in patients undergoing percutaneous coronary intervention (PCI).
Background Individual variability of clopidogrel response might influence results of PCI.
Methods A total of 160 patients receiving clopidogrel before PCI were prospectively enrolled. Platelet reactivity was mea-sured by the VerifyNow P2Y12 assay (Accumetrics Inc., San Diego, California). Primary end point was 30-dayoccurrence of major adverse cardiac events (MACE) according to quartile distribution of P2Y12 reaction units(PRU).
Results Primary end point occurred more frequently in patients with pre-procedural PRU levels in the fourth quartileversus those in the lowest quartile (20% vs. 3%; p � 0.034), and it was entirely due to periprocedural myo-cardial infarction (MI). Mean PRU absolute levels were higher in patients with periprocedural MI (258 � 53vs. 219 � 69 in patients without; p � 0.030). On multivariable analysis pre-PCI PRU levels in the fourthquartile were associated with 6-fold increased risk of 30-day MACE (odds ratio: 6.1; 95% confidence inter-val: 1.1 to 18.3, p � 0.033). By receiver-operating characteristic curve analysis, the optimal cut-off for theprimary end point was a pre-PCI PRU value �240 (area under the curve: 0.69; 95% confidence interval:0.56 to 0.81, p � 0.016).
Conclusions This study indicates that high pre-PCI platelet reactivity might predict 30-day events. Use of a rapid point-of-careassay for monitoring residual platelet reactivity after clopidogrel administration might help identify patients inwhom individualized antiplatelet strategies might be indicated with coronary intervention. (J Am Coll Cardiol2008;52:1128–33) © 2008 by the American College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2008.06.038
rrp(tsaiptgpd
ptimal platelet inhibition plays a key role in the preventionf early myocardial ischemic complications during percuta-eous coronary intervention (PCI) (1,2); accordingly, thessociation of aspirin and clopidogrel, a nonreversible2Y12 platelet receptor inhibitor, represents the establishedntiplatelet therapy in this setting.
Because of inter-individual variability in clopidogrelesponsiveness, platelet function monitoring assays areseful tools to identify patients with different drug
rom the Department of Cardiovascular Sciences, Campus Bio-Medico University ofome, Rome, Italy.
cManuscript received March 25, 2008; revised manuscript received June 5, 2008,
ccepted June 9, 2008.
esponses who might potentially be at increased risk ofecurrent cardiac events or bleeding. Adenosine diphos-hate (ADP)-induced light transmittance aggregometryLTA) is the standard test for evaluating platelet reac-ivity in patients receiving clopidogrel, but this is non-pecific and time-consuming (3); conversely, more rapidnd specific tests measuring clopidogrel response in thendividual patient might be widely applicable in clinicalractice, thereby providing risk stratification and a guideo antithrombotic therapy. Thus, the ARMYDA studyroup (1,4 –7) has designed the ARMYDA-PRO (Anti-latelet therapy for Reduction of MYocardial Damageuring Angioplasty-Platelet Reactivity Predicts Out-
ome) study to prospectively evaluate whether point-of-
co
M
SpdsowrmicCms
lbDspdrtvt(
iMmc2FC6asfEs(vpibuiv
aeT
aclbqaeTfSts3tdbay3fpwh
mttcpgioweosaiwliwcdsSAc
R
Ci
v
1129JACC Vol. 52, No. 14, 2008 Patti et al.September 30, 2008:1128–33 Clopidogrel Response and Outcome After PCI
are measurements of platelet inhibition predict clinicalutcome in patients undergoing PCI.
ethods
tudy population and design. The ARMYDA-PRO is arospective study including 160 patients receiving clopi-ogrel before PCI. Patients with a variety of coronaryyndromes, including non–ST-segment elevation acute cor-nary syndromes (ACS) were enrolled. Exclusion criteriaere: primary PCI; platelet count �70 � 109/l; high bleeding
isk; and severe chronic renal failure (serum creatinine �2g/dl). All patients received 600 mg clopidogrel load approx-
mately 6 h before intervention (n � 120) or were receivinghronic clopidogrel therapy (75 mg/day for �5 days, n � 40).lopidogrel was continued for 1 month after PCI and for 12onths in patients with ACS or receiving drug-eluting
tents. All patients received aspirin.Platelet reactivity was evaluated in the catheterization
aboratory before PCI and at 8 and 24 h after interventiony the VerifyNow P2Y12 assay (Accumetrics Inc., Saniego, California), which is a rapid cartridge-based assay
pecifically measuring direct effects of clopidogrel on thelatelet P2Y12 receptor. Technical details were alreadyescribed elsewhere (8). Results are expressed as P2Y12eaction units (PRU)—the lower the PRU value, the greaterhe degree of P2Y12 receptor inhibition by clopidogrel andice versa. Twenty randomly selected patients were analyzedo assess intra-assay variability, which was 2.1 � 1.3%coefficient of variation: 6%).
Blood samples were also drawn before and at 8 and 24 hn all patients for creatine kinase-myocardial band (CK-
B; mass) and troponin-I (Tn-I; mass) levels; furthereasurements were obtained if symptoms suggested myo-
ardial ischemia. Measurements were performed by AccessImmunochemiluminometric assay (Beckman Coulter,
ullerton, California); normal limits were �4 ng/ml forK-MB and �0.08 ng/ml for Tn-I. One-month and-month clinical follow-up were obtained by office visit inll patients. Each patient gave informed consent to thetudy. The study was not supported by external sources ofunding.nd points. Primary end point of the ARMYDA-PRO
tudy was 30-day incidence of major adverse cardiac eventsMACE): cardiac death, myocardial infarction (MI), targetessel revascularization, in relation to quartile distribution oflatelet reactivity measured by PRU assay. Myocardialnfarction was defined as post-procedural increase of cardiaciomarkers (Tn or CK-MB) �3 � 99th percentile of thepper reference limit (9). Target vessel revascularizationncluded by-pass surgery or repeat PCI of the targetessel(s).
Secondary end points were: 1) evaluation of mean PRUbsolute values in patients with or without post-PCIlevation of markers of myocardial damage (CK-MB,
n-I); 2) distribution in PRU quartiles of patients with rny post-procedural increase ofardiac markers above normalimits; 3) correlation of vascular/leeding complications to PRUuartiles; and 4) clinical outcomet 6-month follow-up. Bleedingvents were defined according tohrombolysis In Myocardial In-
arction criteria (10).tatistics. On the basis of pa-
ients’ enrollment criteria, we as-umed 8% overall incidence of0-day MACE (1,11). Weested the hypothesis that inci-ence of 30-day MACE differedy PRU quartiles. We assumeds effect size for the power anal-sis a 7-fold increased risk of0-day MACE in patients of theourth quartile (12); thus, a studyopulation of at least 153 patientsould be needed to verify thisypothesis with alpha of 0.05 (2-tailed) and beta of 0.08.Continuous variables were compared by t test for nor-ally distributed values; otherwise the Mann-Whitney U
est was used. Proportions were compared by Fisher exactest when the expected frequency was �5; otherwise thehi-square test was applied. Event-free survival analysis waserformed by Kaplan-Meier method with log-rank testroup comparison. Odds ratios (ORs) and 95% confidencentervals (CIs) investigating the independent predictive rolef PRU quartiles on the occurrence of the primary end pointere assessed by logistic regression. The following param-
ters were first evaluated in a univariate model: comparisonf PRU quartiles (fourth vs. first quartile, third vs. first,econd vs. first); each of the variables indicated in Table 1;nd procedural variables, such as stent length, direct stent-ng, inflations duration. Only variables with p value �0.15ere then entered into the final model of multivariable
ogistic regression analysis. Ability of the assay to discrim-nate between patients with and without MACE at 30 daysas evaluated by receiver-operating characteristic (ROC)
urve analysis. The optimal cut-off value was calculated byetermining the PRU value providing the greatest sum ofensitivity and specificity. Results are expressed as mean �D. A p value �0.05 (2-tailed) was considered significant.nalysis was performed with SPSS 12.0 (SPSS Inc., Chi-
ago, Illinois) software.
esults
linical and procedural characteristics according to pre-ntervention PRU quartiles are indicated in Table 1.
Procedural success was obtained in 99% of patients. Noessel or side branch (�2 mm) closure occurred. No patient
Abbreviationsand Acronyms
ACS � acute coronarysyndromes
ADP � adenosinediphosphate
CK-MB � creatine kinase-myocardial band
LTA � light transmittanceaggregometry
MACE � major adversecardiac events
MI � myocardial infarction
PCI � percutaneouscoronary intervention
PRU � platelet (P2Y12)reaction units
ROC � receiver-operatingcharacteristic
Tn � troponin
equired emergency coronary artery
by-pass graft.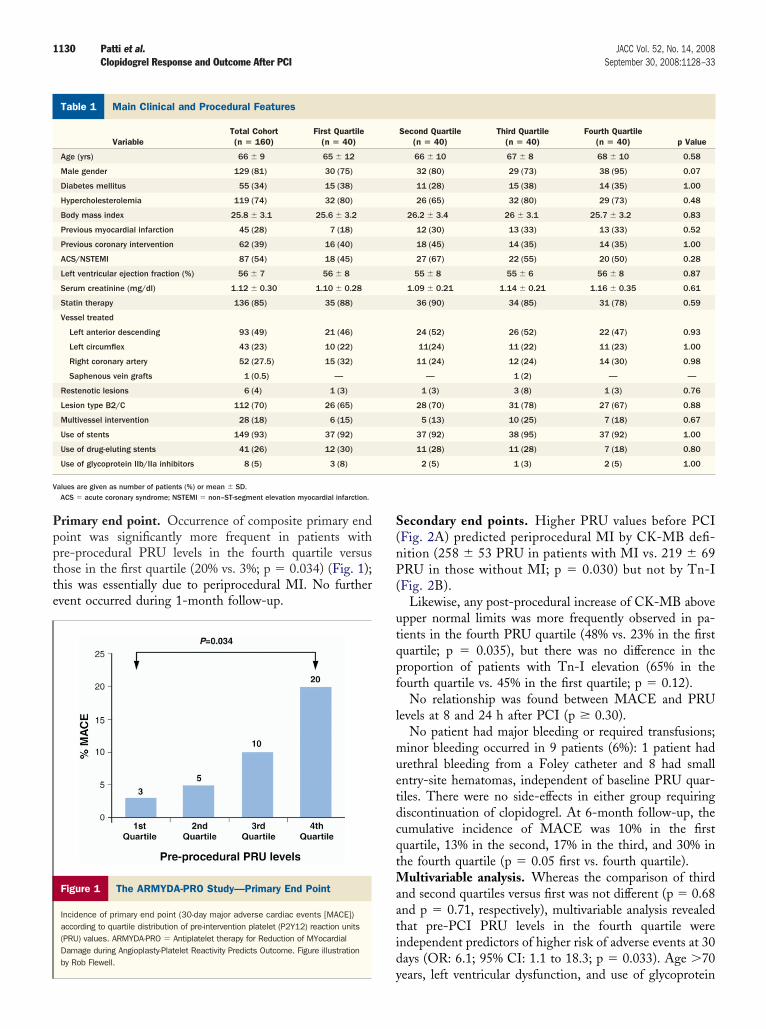
Ppptte
S(nP(
utqpf
l
muetdcqtMaatid
M
V
1130 Patti et al. JACC Vol. 52, No. 14, 2008Clopidogrel Response and Outcome After PCI September 30, 2008:1128–33
rimary end point. Occurrence of composite primary endoint was significantly more frequent in patients withre-procedural PRU levels in the fourth quartile versushose in the first quartile (20% vs. 3%; p � 0.034) (Fig. 1);his was essentially due to periprocedural MI. No furthervent occurred during 1-month follow-up.
ain Clinical and Procedural Features
Table 1 Main Clinical and Procedural Features
VariableTotal Cohort(n � 160)
First Quartile(n � 40)
Age (yrs) 66 � 9 65 � 12
Male gender 129 (81) 30 (75)
Diabetes mellitus 55 (34) 15 (38)
Hypercholesterolemia 119 (74) 32 (80)
Body mass index 25.8 � 3.1 25.6 � 3.2
Previous myocardial infarction 45 (28) 7 (18)
Previous coronary intervention 62 (39) 16 (40)
ACS/NSTEMI 87 (54) 18 (45)
Left ventricular ejection fraction (%) 56 � 7 56 � 8
Serum creatinine (mg/dl) 1.12 � 0.30 1.10 � 0.28
Statin therapy 136 (85) 35 (88)
Vessel treated
Left anterior descending 93 (49) 21 (46)
Left circumflex 43 (23) 10 (22)
Right coronary artery 52 (27.5) 15 (32)
Saphenous vein grafts 1 (0.5) —
Restenotic lesions 6 (4) 1 (3)
Lesion type B2/C 112 (70) 26 (65)
Multivessel intervention 28 (18) 6 (15)
Use of stents 149 (93) 37 (92)
Use of drug-eluting stents 41 (26) 12 (30)
Use of glycoprotein IIb/IIa inhibitors 8 (5) 3 (8)
alues are given as number of patients (%) or mean � SD.ACS � acute coronary syndrome; NSTEMI � non–ST-segment elevation myocardial infarction.
Figure 1 The ARMYDA-PRO Study—Primary End Point
Incidence of primary end point (30-day major adverse cardiac events [MACE])according to quartile distribution of pre-intervention platelet (P2Y12) reaction units(PRU) values. ARMYDA-PRO � Antiplatelet therapy for Reduction of MYocardialDamage during Angioplasty-Platelet Reactivity Predicts Outcome. Figure illustrationby Rob Flewell.
y
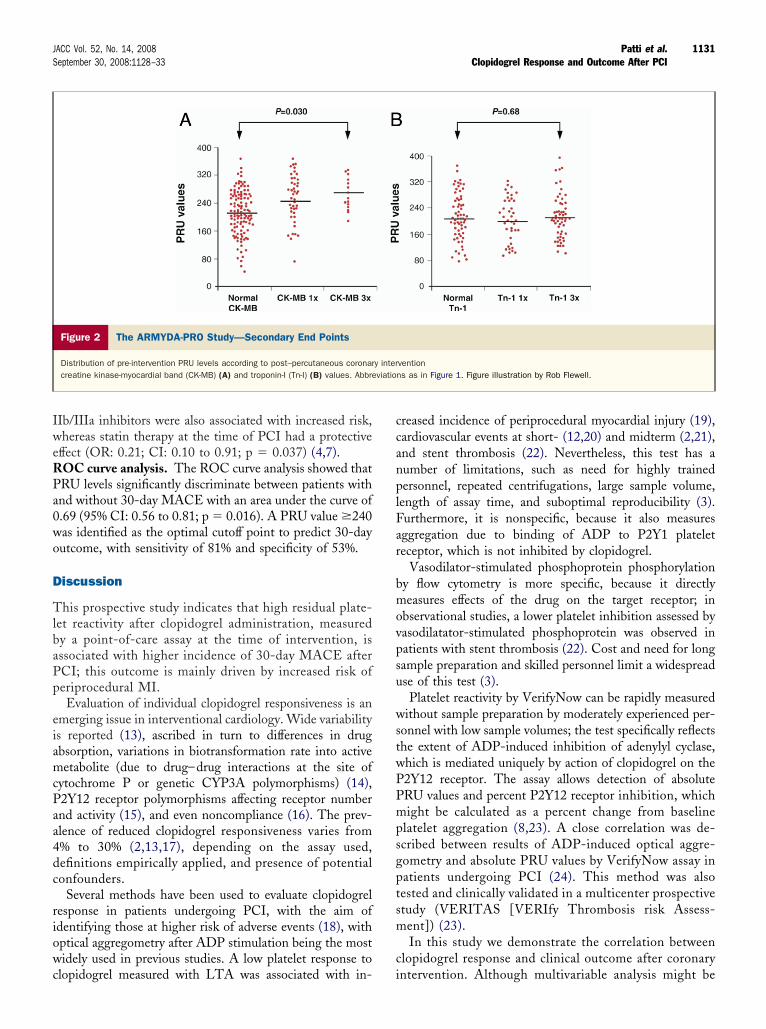
econdary end points. Higher PRU values before PCIFig. 2A) predicted periprocedural MI by CK-MB defi-ition (258 � 53 PRU in patients with MI vs. 219 � 69RU in those without MI; p � 0.030) but not by Tn-I
Fig. 2B).Likewise, any post-procedural increase of CK-MB above
pper normal limits was more frequently observed in pa-ients in the fourth PRU quartile (48% vs. 23% in the firstuartile; p � 0.035), but there was no difference in theroportion of patients with Tn-I elevation (65% in theourth quartile vs. 45% in the first quartile; p � 0.12).
No relationship was found between MACE and PRUevels at 8 and 24 h after PCI (p � 0.30).
No patient had major bleeding or required transfusions;inor bleeding occurred in 9 patients (6%): 1 patient had
rethral bleeding from a Foley catheter and 8 had smallntry-site hematomas, independent of baseline PRU quar-iles. There were no side-effects in either group requiringiscontinuation of clopidogrel. At 6-month follow-up, theumulative incidence of MACE was 10% in the firstuartile, 13% in the second, 17% in the third, and 30% inhe fourth quartile (p � 0.05 first vs. fourth quartile).
ultivariable analysis. Whereas the comparison of thirdnd second quartiles versus first was not different (p � 0.68nd p � 0.71, respectively), multivariable analysis revealedhat pre-PCI PRU levels in the fourth quartile werendependent predictors of higher risk of adverse events at 30ays (OR: 6.1; 95% CI: 1.1 to 18.3; p � 0.033). Age �70
Second Quartile(n � 40)
Third Quartile(n � 40)
Fourth Quartile(n � 40) p Value
66 � 10 67 � 8 68 � 10 0.58
32 (80) 29 (73) 38 (95) 0.07
11 (28) 15 (38) 14 (35) 1.00
26 (65) 32 (80) 29 (73) 0.48
26.2 � 3.4 26 � 3.1 25.7 � 3.2 0.83
12 (30) 13 (33) 13 (33) 0.52
18 (45) 14 (35) 14 (35) 1.00
27 (67) 22 (55) 20 (50) 0.28
55 � 8 55 � 6 56 � 8 0.87
1.09 � 0.21 1.14 � 0.21 1.16 � 0.35 0.61
36 (90) 34 (85) 31 (78) 0.59
24 (52) 26 (52) 22 (47) 0.93
11(24) 11 (22) 11 (23) 1.00
11 (24) 12 (24) 14 (30) 0.98
— 1 (2) — —
1 (3) 3 (8) 1 (3) 0.76
28 (70) 31 (78) 27 (67) 0.88
5 (13) 10 (25) 7 (18) 0.67
37 (92) 38 (95) 37 (92) 1.00
11 (28) 11 (28) 7 (18) 0.80
2 (5) 1 (3) 2 (5) 1.00
ears, left ventricular dysfunction, and use of glycoprotein
IweRPa0wo
D
TlbaPp
eiamcPaa4dc
riowc
ccanplFar
bmovpsu
wstwPPmpsgptsm
c
1131JACC Vol. 52, No. 14, 2008 Patti et al.September 30, 2008:1128–33 Clopidogrel Response and Outcome After PCI
Ib/IIIa inhibitors were also associated with increased risk,hereas statin therapy at the time of PCI had a protective
ffect (OR: 0.21; CI: 0.10 to 0.91; p � 0.037) (4,7).OC curve analysis. The ROC curve analysis showed thatRU levels significantly discriminate between patients withnd without 30-day MACE with an area under the curve of.69 (95% CI: 0.56 to 0.81; p � 0.016). A PRU value �240as identified as the optimal cutoff point to predict 30-dayutcome, with sensitivity of 81% and specificity of 53%.
iscussion
his prospective study indicates that high residual plate-et reactivity after clopidogrel administration, measuredy a point-of-care assay at the time of intervention, isssociated with higher incidence of 30-day MACE afterCI; this outcome is mainly driven by increased risk oferiprocedural MI.Evaluation of individual clopidogrel responsiveness is an
merging issue in interventional cardiology. Wide variabilitys reported (13), ascribed in turn to differences in drugbsorption, variations in biotransformation rate into activeetabolite (due to drug–drug interactions at the site of
ytochrome P or genetic CYP3A polymorphisms) (14),2Y12 receptor polymorphisms affecting receptor numbernd activity (15), and even noncompliance (16). The prev-lence of reduced clopidogrel responsiveness varies from% to 30% (2,13,17), depending on the assay used,efinitions empirically applied, and presence of potentialonfounders.
Several methods have been used to evaluate clopidogrelesponse in patients undergoing PCI, with the aim ofdentifying those at higher risk of adverse events (18), withptical aggregometry after ADP stimulation being the mostidely used in previous studies. A low platelet response to
Figure 2 The ARMYDA-PRO Study—Secondary End Points
Distribution of pre-intervention PRU levels according to post–percutaneous coronarcreatine kinase-myocardial band (CK-MB) (A) and troponin-I (Tn-I) (B) values. Abbre
lopidogrel measured with LTA was associated with in- i
reased incidence of periprocedural myocardial injury (19),ardiovascular events at short- (12,20) and midterm (2,21),nd stent thrombosis (22). Nevertheless, this test has aumber of limitations, such as need for highly trainedersonnel, repeated centrifugations, large sample volume,
ength of assay time, and suboptimal reproducibility (3).urthermore, it is nonspecific, because it also measuresggregation due to binding of ADP to P2Y1 plateleteceptor, which is not inhibited by clopidogrel.
Vasodilator-stimulated phosphoprotein phosphorylationy flow cytometry is more specific, because it directlyeasures effects of the drug on the target receptor; in
bservational studies, a lower platelet inhibition assessed byasodilatator-stimulated phosphoprotein was observed inatients with stent thrombosis (22). Cost and need for longample preparation and skilled personnel limit a widespreadse of this test (3).Platelet reactivity by VerifyNow can be rapidly measured
ithout sample preparation by moderately experienced per-onnel with low sample volumes; the test specifically reflectshe extent of ADP-induced inhibition of adenylyl cyclase,hich is mediated uniquely by action of clopidogrel on the2Y12 receptor. The assay allows detection of absoluteRU values and percent P2Y12 receptor inhibition, whichight be calculated as a percent change from baseline
latelet aggregation (8,23). A close correlation was de-cribed between results of ADP-induced optical aggre-ometry and absolute PRU values by VerifyNow assay inatients undergoing PCI (24). This method was alsoested and clinically validated in a multicenter prospectivetudy (VERITAS [VERIfy Thrombosis risk Assess-ent]) (23).In this study we demonstrate the correlation between
lopidogrel response and clinical outcome after coronary
ventionns as in Figure 1. Figure illustration by Rob Flewell.
y interviatio
ntervention. Although multivariable analysis might be

ocfpoa3tpi(PtIPbIepbvsva
sadwa
nccw
htrrbete(otmn
RcUE
R
1
1
1
1
1
1
1
1
1
1
1132 Patti et al. JACC Vol. 52, No. 14, 2008Clopidogrel Response and Outcome After PCI September 30, 2008:1128–33
verfitted, given the number of end point events in-luded, the predictive value for adverse events of theourth quartile of platelet reactivity was independent ofossible confounding factors, with a 6-fold increased riskf periprocedural MI versus the first quartile. An ROCnalysis indicated that this assay can predict outcome at0 days, with optimal cutoff point to discriminate pa-ients at higher risk of events of �240 PRU, and aositive predictive value of 81%. The threshold identifiedn our study coincides with that observed by Price et al.25) in an observational study in which a cutoff �235RU correlated with 6-month events, including stent
hrombosis, in patients receiving sirolimus-eluting stents.n ARMYDA-PRO, the negative predictive value ofRU in the first quartile was 98%, with minimal proba-ility of early adverse events with PRU levels �178.nterestingly, higher PRU values correlated with CK-MBlevation but not with Tn-I elevation, suggesting thatlatelet-unrelated events (i.e., distal embolization) mighte also responsible for Tn raise after PCI (12). No cut-offalue for events was described in a recent study (26) ontable patients treated with drug-eluting stents afterariable loading doses of clopidogrel (300 or 600 mg) thatlso used VerifyNow.
We used quartile distribution, because clopidogrel re-ponsiveness is multifactorial and it should be considered ascontinuum; accordingly, a progressively increasing inci-
ence of events was observed across PRU quartiles (Fig. 1),ith a similar pattern of correlation between PRU values
nd peak levels of myocardial markers (Fig. 2).Unlike the Price et al. study (25), ARMYDA-PRO was
ot powered to evaluate relationship between degree oflopidogrel inhibition and occurrence of bleeding compli-ations or late thrombotic events; larger prospective studiesith longer follow-up are needed to address this issue.Clopidogrel responsiveness variability, within the en-
anced thrombotic milieu of PCI, requires careful evalua-ion. The ARMYDA-PRO study supports the use of aapid point-of-care assay for monitoring residual plateleteactivity after clopidogrel administration: VerifyNow cane a useful and easily applicable method that might helpstablish a clinically driven threshold of platelet reactivityhat would identify patients at higher risk of periproceduralvents; in those, individualized antithrombotic strategiesi.e., restricted use of drug-eluting stents, more extensive usef glycoprotein IIb/IIIa inhibitors, higher clopidogrel main-enance dose, or use of newer P2Y12 receptor antagonists)ight be indicated to improve clinical outcome after coro-
ary intervention.
eprint requests and correspondence: Prof. Germano Di Scias-io, Department of Cardiovascular Sciences, Campus Bio-Mediconiversity, Via Alvaro del Portillo, 200, 00128 Rome, Italy.
-mail: [email protected].EFERENCES
1. Patti G, Colonna G, Pasceri V, Lassandro Pepe L, Montinaro A, DiSciascio G. Randomized trial of high loading dose of clopidogrel forreduction of periprocedural myocardial infarction in patients undergo-ing coronary intervention: results from the ARMYDA-2 study.Circulation 2005;111:2099–106.
2. Gurbel PA, Bliden KP, Guyer K, et al. Platelet reactivity in patientsand recurrent events post-stenting: results of the PREPARE POST-STENTING Study. J Am Coll Cardiol 2005;46:1820–6.
3. Michelson AD. Platelet function testing in cardiovascular diseases.Circulation 2004;110:489–93.
4. Pasceri V, Patti G, Nusca A, Pristipino C, Richichi G, Di Sciascio G.Randomized trial of atorvastatin for reduction of myocardial damageduring coronary intervention: results from the ARMYDA study.Circulation 2004;110:674–8.
5. Patti G, Chello M, Candura D, et al. Randomized trial of atorvastatinfor reduction of postoperative atrial fibrillation in patients undergoingcardiac surgery: results of the ARMYDA-3 study. Circulation 2006;114:1455–61.
6. Patti G, Chello M, Pasceri V, et al. Protection from proceduralmyocardial injury by atorvastatin is associated with lower levels ofadhesion molecules after percutaneous coronary intervention: resultsfrom the ARMYDA-CAMs substudy. J Am Coll Cardiol 2006;48:1560–6.
7. Patti G, Pasceri V, Colonna G, et al. Atorvastatin pretreatmentimproves outcomes in patients with acute coronary syndromes under-going early percutaneous coronary intervention: results of theARMYDA-ACS randomized trial. J Am Coll Cardiol 2007;49:1272–8.
8. Malinin A, Pokov A, Swaim L, Kotob M, Serebruany V. Validation ofa VerifyNow-P2Y12 cartridge for monitoring platelet inhibition withclopidogrel. Methods Find Exp Clin Pharmacol 2006;28:315–22.
9. Thygesen K, Alpert JS, White HD, on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of MyocardialInfarction. Universal definition of myocardial infarction. J Am CollCardiol 2007;50:2173–95.
0. Rao AK, Pratt C, Berke A, et al. Thrombolysis in MyocardialInfarction (TIMI) Trial-phase I: hemorrhagic manifestations andchanges in plasma fibrinogen and the fibrinolytic system in patientstreated with recombinant tissue plasminogen activator and streptoki-nase. J Am Coll Cardiol 1988;11:1–11.
1. Kastrati A, Mehilli J, Neumann FJ, et al. Abciximab in patients withacute coronary syndromes undergoing percutaneous coronary interven-tion after clopidogrel pretreatment: the ISAR-REACT 2 randomizedtrial. JAMA 2006;295:1531–8.
2. Hochholzer W, Trenk D, Bestehorn HP, et al. Impact of the degreeof peri-interventional platelet inhibition after loading with clopidogrelon early clinical outcome of elective coronary stent placement. J AmColl Cardiol 2006;48:1742–50.
3. Gurbel PA, Bliden KP, Hiatt BL, O’Connor CM. Clopidogrel forcoronary stenting: response variability, drug resistance, and the effect ofpretreatment platelet reactivity. Circulation 2003;107:2908–13.
4. Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, et al. Contribution ofgene sequence variations of the hepatic cytochrome P450 3A4 enzymeto variability in individual responsiveness to clopidogrel. ArteriosclerThromb Vasc Biol 2006;26:1895–900.
5. Fontana P, Dupont A, Gandrille S, et al. Adenosine diphosphate-induced platelet aggregation is associated with P2Y12 gene sequencevariations in healthy subjects. Circulation 2003;108:989–95.
6. Serebruany VL. The “clopidogrel resistance” trap. Am J Cardiol2007;100:1044–6.
7. Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, Bhatt DL,Topol EJ. Variability in platelet responsiveness to clopidogrel among544 individuals. J Am Coll Cardiol 2005;45:246–51.
8. Snoep JD, Hovens MM, Eikenboom JC, van der Bom JG, JukemaJW, Huisman MV. Clopidogrel nonresponsiveness in patients under-going percutaneous coronary intervention with stenting: a systematicreview and meta-analysis. Am Heart J 2007;154:221–31.
9. Gurbel PA, Bliden KP, Zaman KA, Yoho JA, Hayes KM, Tantry US.
Clopidogrel loading with eptifibatide to arrest the reactivity of plate-
2
2
2
2
2
2
2
K
1133JACC Vol. 52, No. 14, 2008 Patti et al.September 30, 2008:1128–33 Clopidogrel Response and Outcome After PCI
lets: results of the CLEAR PLATELETS study. Circulation2005;111:1153–9.
0. Cuisset T, Frere C, Quilici J, et al. Benefit of a 600-mg loading doseof clopidogrel on platelet reactivity and clinical outcomes in patientswith non–ST-segment elevation acute coronary syndrome undergoingcoronary stenting. J Am Coll Cardiol 2006;48:1339–45.
1. Bliden KP, DiChiara J, Tantry US, Bassi AK, Chaganti SK, GurbelPA. Increased risk in patients with high platelet aggregation receivingchronic clopidogrel therapy undergoing percutaneous coronary inter-vention: is the current antiplatelet therapy adequate? J Am CollCardiol 2007;49:657–66.
2. Gurbel PA, Bliden KP, Samara W, et al. Clopidogrel effect on plateletreactivity in patients with stent thrombosis: results of the CRESTstudy. J Am Coll Cardiol 2005;46:1827–32.
3. Malinin A, Pokov A, Spergling M, et al. Monitoring platelet inhibi-tion after clopidogrel with the VerifyNow-P2Y12 rapid analyzer: theVERIfy Thrombosis risk ASsessment (VERITAS) study. Thromb
Res 2007;119:277–84. a4. Van Werkum JW, Van der Stelt CA, Seesing TH, Hackeng CM,Ten Berg JM. A head-to-head comparison between the VerifyNowP2Y12 assay and light transmittance aggregometry for monitoringthe individual platelet response to clopidogrel in patients undergo-ing elective percutaneous coronary intervention. J Thromb Hae-most 2006;4:2516 – 8.
5. Price MJ, Endemann S, Gollapudi RR, et al. Prognostic significanceof post-clopidogrel platelet reactivity assessed by a point-of-care assayon thrombotic events after drug-eluting stent implantation. EurHeart J 2008;29:992–1000.
6. Buch AN, Singh S, Roy P, et al. Measuring aspirin resistance,clopidogrel responsiveness, and postprocedural markers of myonecrosisin patients undergoing percutaneous coronary intervention. Am JCardiol 2007;99:1518–22.
ey Words: clopidogrel y percutaneous coronary intervention y platelet
ggregometry.




























