Embed Size (px)
Citation preview

Point-of-care Autoantibody Testing in a Rheumatology Setting
Konstantin N. Konstantinov, MD, PhD.Associate Professor – Medicine / Rheumatology
UNM School of Medicine, New Mexico, USA
Disclosure Statement
Nothing to declare
Evidence-based medicine (EBM) slide
Konstantinov KN et al. Rapid detection of anti-chromatin autoantibodies in human serum using a portable electrochemical biosensor. Biosensors and Bioelectronics, 2009, 24:1949-1954
Renger F et al. Immediate determination of ACPA and rheumatoid factor – a novel point of care test for detection of anti-MCV antibodies and rheumatoid factor using a lateral-flow immunoassay. Arthritis Research & Therapy, 2010, 12:R120
Schlichtiger A et al. Biosensor approaches for the detection of autoantibodies in human serum. Bioanalytical Reviews, March 2012, Springer online publication
American Academy of Microbiology. Bringing the Lab to the patient: developing point of care diagnostics for resource limited settings. June 2012, American Society for Microbiology online publication

Hieronymous Bosch (c 1450-1516), The Cure of Folly (Extraction of the Stone of Madness), 1475-1480, Dutch. Oil on board, 48 × 35 cm, Museo del Prado, Madrid
POCTherapy Diagnostics

The Point of Point of Care Testing
No accepted universal definition, often referred to as near patient, bedside, or extra laboratory testing
Critical elements are:» Rapid turn-around and communication of results to guide clinical
decisions
» Completion of testing and follow-up action in the same clinical encounter
Point of Care Tests: The Times They Are a-Changing
Near real-time monitoring of clinical samples Overcomes disadvantages of centralized, purpose-built laboratories Equipment miniaturization due to technological advances in
materials, microfluidics and computerization Mass fabrication of disposable components Acceptable replacement cost Operational use with minimal instruction
Possibility for instant, result-deduced therapeutic action

Is the ideal POC test only cheap or fast?
The ideal POC test should have different characteristics simultaneously:
A S S U R E D
AffordableSensitiveSpecificUser-friendlyRobust and RapidEquipment-freeDeliverable
Bringing the Lab to the Patient; Report from the American Academy of Microbiology, 2012; www.asm.org
Biosensors: the canary in the coalmine
Science and Economics: the “canary in the coalmine” is healthy and kicking
Biosensors world market generate annual sales of $13 billion, the lion’s share still belongs to glucose home meters
» Cranfield University Study, 2009
Global demand for biosensors in medical diagnostics is forecast to reach $16.5 billion by 2017
» (Global Industry Analysts Report, 2012)
Spawn 6,000 research papers in 2011» Anthony PF Turner, Editor-in-Chief: Biosensors and Bioelectronics
_____________________________
Comparison: NIH budget for 2012 is $ 32 billion
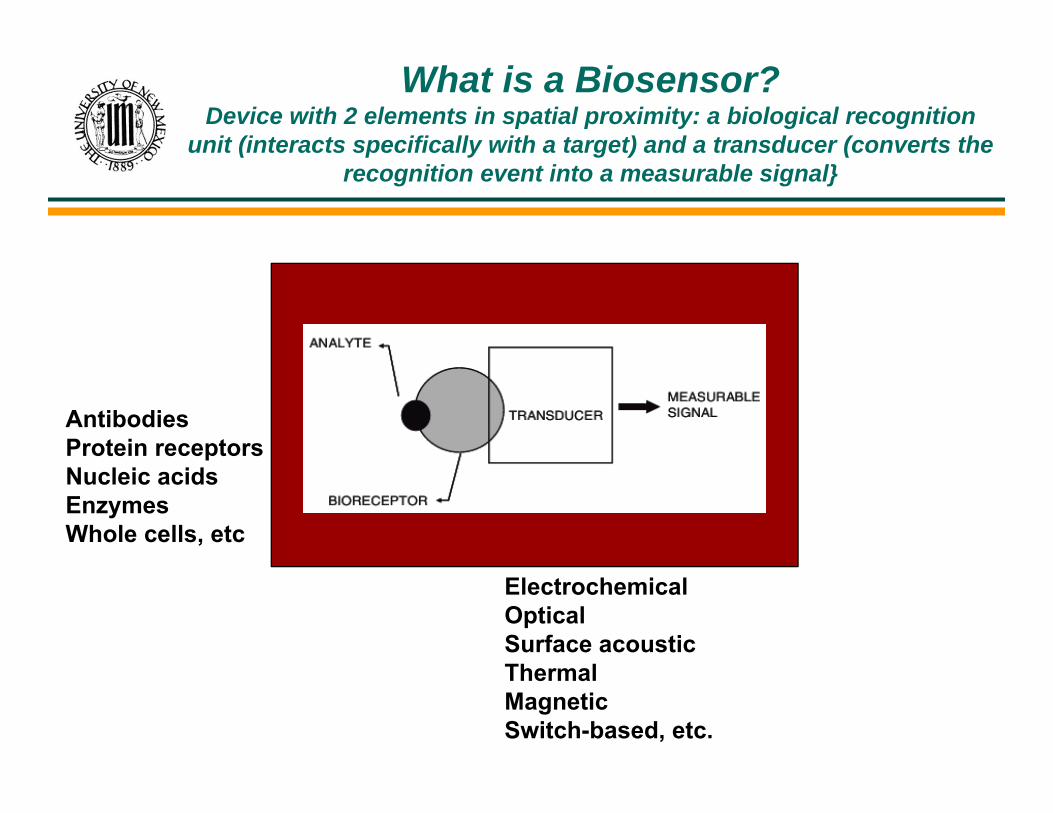
What is a Biosensor?Device with 2 elements in spatial proximity: a biological recognition
unit (interacts specifically with a target) and a transducer (converts the recognition event into a measurable signal}
ElectrochemicalOpticalSurface acousticThermalMagneticSwitch-based, etc.
AntibodiesProtein receptorsNucleic acidsEnzymesWhole cells, etc
Small and light weight
Use small sample sizes
Store results
Transmit them (wirelessly)
Be amenable to quality control checks
“The time taken to reach the correct diagnosis may critically impact on the patient’s chances of survival”
British Medical Journal, Gordon Caldwell
Accurate diagnostics affects health care decisions to a degree wellout of proportion to their cost.
Diagnostics account for 2% of the cost of health care, yet can affect60-70% of treatment decisions
Bufton A. 2002, Business Briefing: Medical Device Manufacturing & TechnologyMedicare laboratory payment policy. 2000, Institute of Medicine, National Academy Press
POC Testing in Rheumatology or Seeing the Forest for the Trees
Getting the big picture means asking a lot of little questions and S E T T I N G P R I O R I T I E S
Which diagnostic tests are most needed? What characteristics do they have to have to succeed? Is there a clear link to diagnosis, treatment or counseling plan? Does it offer convenience to patients and care providers? Can it improve health care in limited resource areas?

Why autoantibodies?
Predict incipient disease Facilitate diagnosis refinement Indicate disease severity or impending flares Prognostic marker for further organ involvement Monitor efficacy of therapy Monitor induction of autoimmunity by drugs
POC Autoantibody Testing: Is It Ready for Primetime?
Support for considerable value of direct monitoring of autoantibodies in the clinic comes from:
1. Diagnostic Process in acute-care settings2. Assessing active disease
3. Other advantages
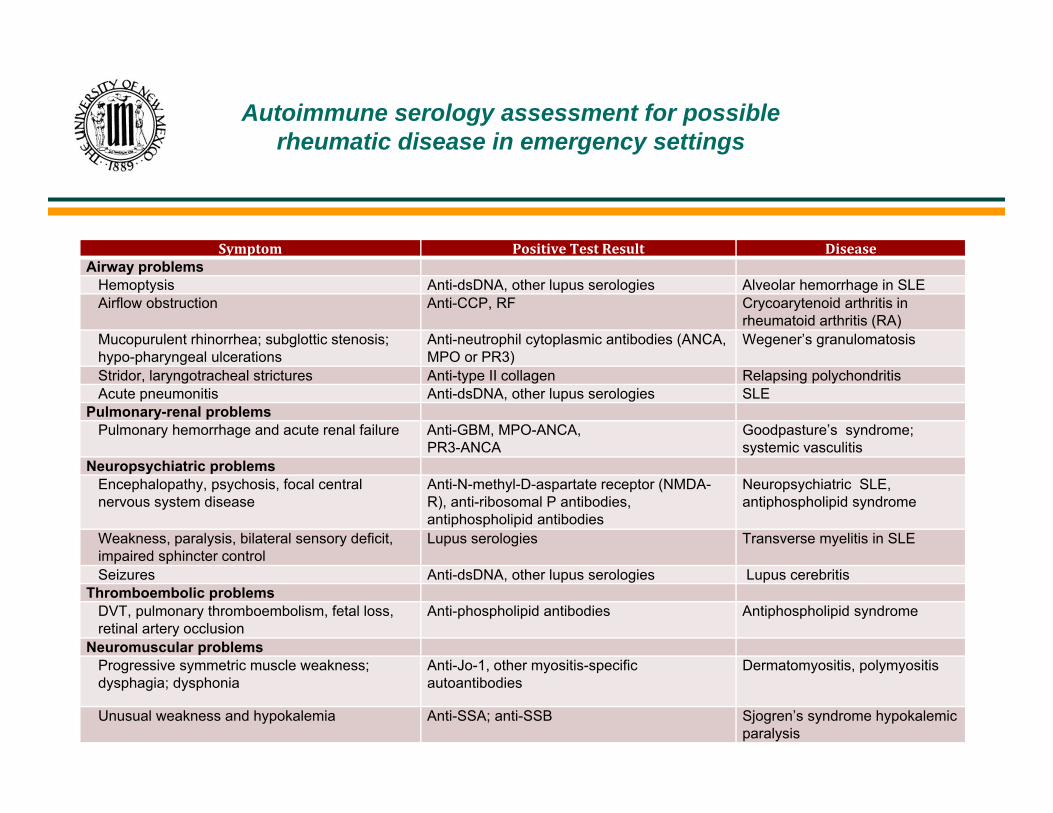
Autoimmune serology assessment for possible rheumatic disease in emergency settings
Symptom PositiveTestResult DiseaseAirway problems
Hemoptysis Anti-dsDNA, other lupus serologies Alveolar hemorrhage in SLEAirflow obstruction Anti-CCP, RF Crycoarytenoid arthritis in
rheumatoid arthritis (RA)Mucopurulent rhinorrhea; subglottic stenosis; hypo-pharyngeal ulcerations
Anti-neutrophil cytoplasmic antibodies (ANCA, MPO or PR3)
Wegener’s granulomatosis
Stridor, laryngotracheal strictures Anti-type II collagen Relapsing polychondritisAcute pneumonitis Anti-dsDNA, other lupus serologies SLE
Pulmonary-renal problemsPulmonary hemorrhage and acute renal failure Anti-GBM, MPO-ANCA,
PR3-ANCAGoodpasture’s syndrome;systemic vasculitis
Neuropsychiatric problemsEncephalopathy, psychosis, focal central nervous system disease
Anti-N-methyl-D-aspartate receptor (NMDA-R), anti-ribosomal P antibodies,antiphospholipid antibodies
Neuropsychiatric SLE, antiphospholipid syndrome
Weakness, paralysis, bilateral sensory deficit, impaired sphincter control
Lupus serologies Transverse myelitis in SLE
Seizures Anti-dsDNA, other lupus serologies Lupus cerebritisThromboembolic problems
DVT, pulmonary thromboembolism, fetal loss, retinal artery occlusion
Anti-phospholipid antibodies Antiphospholipid syndrome
Neuromuscular problemsProgressive symmetric muscle weakness; dysphagia; dysphonia
Anti-Jo-1, other myositis-specific autoantibodies
Dermatomyositis, polymyositis
Unusual weakness and hypokalemia Anti-SSA; anti-SSB Sjogren’s syndrome hypokalemic paralysis
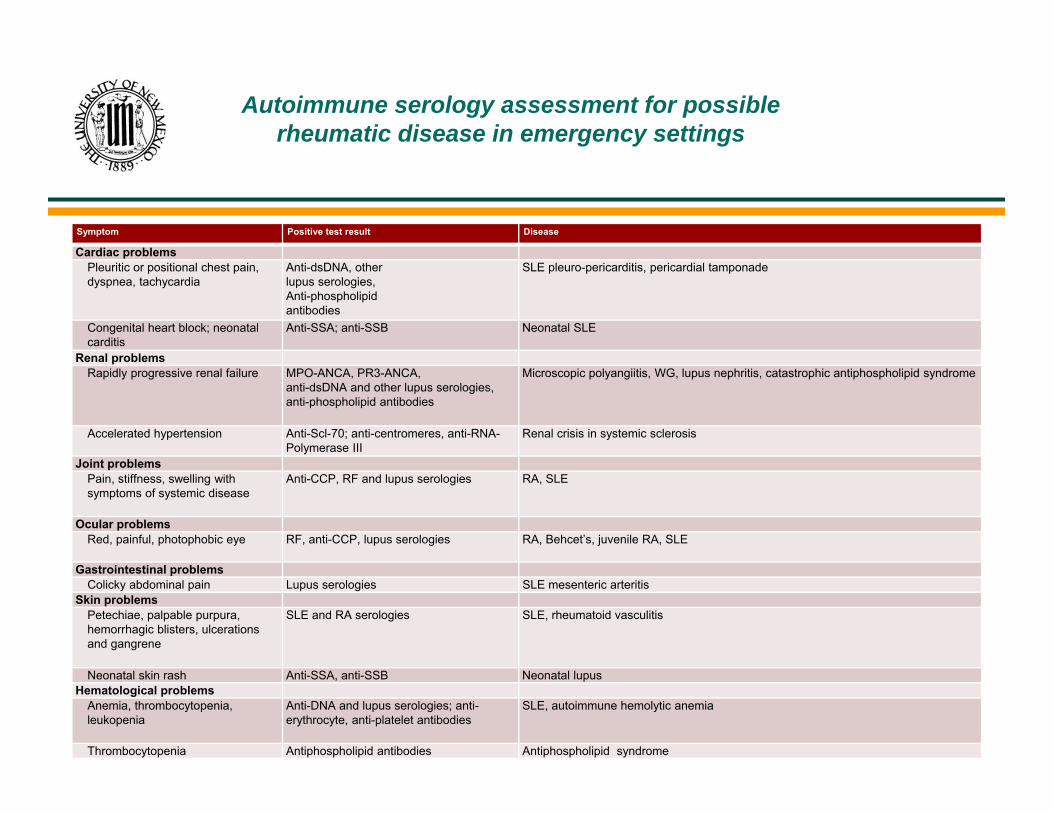
Autoimmune serology assessment for possible rheumatic disease in emergency settings
Symptom Positive test result Disease
Cardiac problemsPleuritic or positional chest pain, dyspnea, tachycardia
Anti-dsDNA, otherlupus serologies,Anti-phospholipidantibodies
SLE pleuro-pericarditis, pericardial tamponade
Congenital heart block; neonatal carditis
Anti-SSA; anti-SSB Neonatal SLE
Renal problemsRapidly progressive renal failure MPO-ANCA, PR3-ANCA,
anti-dsDNA and other lupus serologies, anti-phospholipid antibodies
Microscopic polyangiitis, WG, lupus nephritis, catastrophic antiphospholipid syndrome
Accelerated hypertension Anti-Scl-70; anti-centromeres, anti-RNA-Polymerase III
Renal crisis in systemic sclerosis
Joint problemsPain, stiffness, swelling with symptoms of systemic disease
Anti-CCP, RF and lupus serologies RA, SLE
Ocular problemsRed, painful, photophobic eye RF, anti-CCP, lupus serologies RA, Behcet’s, juvenile RA, SLE
Gastrointestinal problemsColicky abdominal pain Lupus serologies SLE mesenteric arteritis
Skin problemsPetechiae, palpable purpura, hemorrhagic blisters, ulcerations and gangrene
SLE and RA serologies SLE, rheumatoid vasculitis
Neonatal skin rash Anti-SSA, anti-SSB Neonatal lupusHematological problems
Anemia, thrombocytopenia,leukopenia
Anti-DNA and lupus serologies; anti-erythrocyte, anti-platelet antibodies
SLE, autoimmune hemolytic anemia
Thrombocytopenia Antiphospholipid antibodies Antiphospholipid syndrome
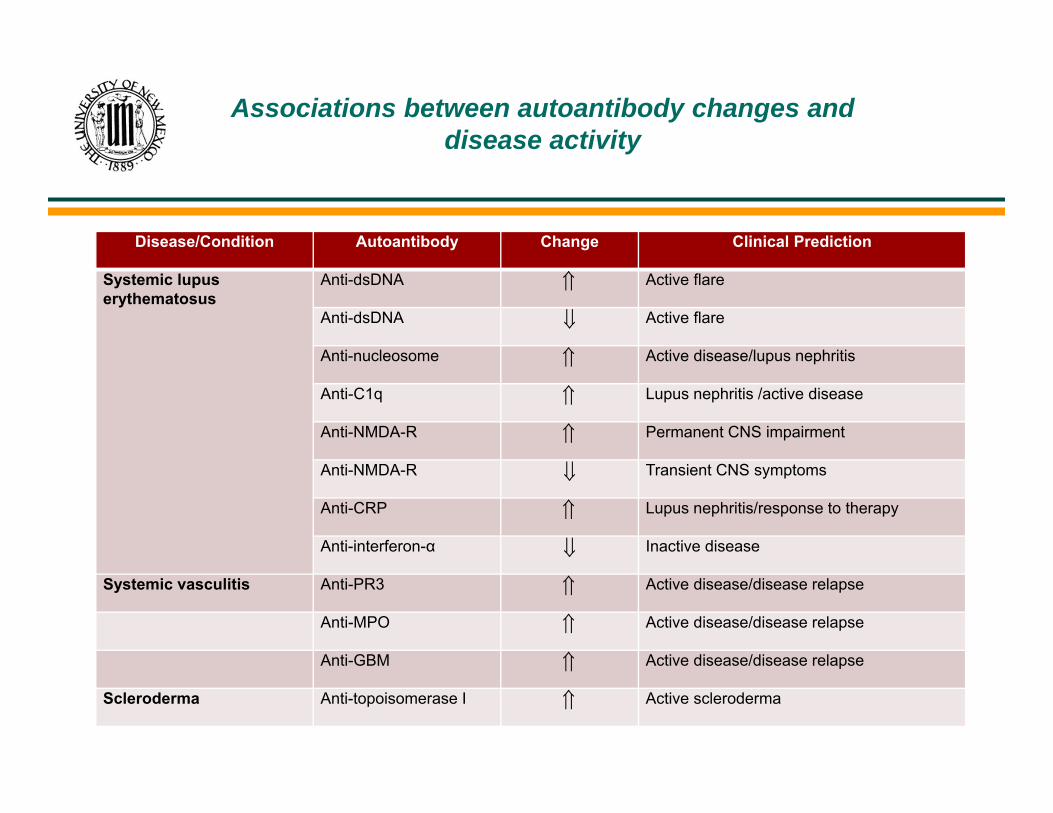
Associations between autoantibody changes and disease activity
Disease/Condition Autoantibody Change Clinical Prediction
Systemic lupus erythematosus
Anti-dsDNA Active flare
Anti-dsDNA Active flare
Anti-nucleosome Active disease/lupus nephritis
Anti-C1q Lupus nephritis /active disease
Anti-NMDA-R Permanent CNS impairment
Anti-NMDA-R Transient CNS symptoms
Anti-CRP Lupus nephritis/response to therapy
Anti-interferon-α Inactive disease
Systemic vasculitis Anti-PR3 Active disease/disease relapse
Anti-MPO Active disease/disease relapse
Anti-GBM Active disease/disease relapse
Scleroderma Anti-topoisomerase I Active scleroderma

Associations between autoantibody changes and disease activity
Disease/Condition Autoantibody Change Clinical Prediction
Rheumatoid arthritis Anti-drug (Adalimumab) Treatment failure
Antiphospholipid syndrome/SLE
Anti-phospholipid Procoagulant state, thrombosis
Necrotizing myopathy Anti-signal recognition particle
Decreased muscle strength, increased creatine kinase activity
Thrombotic thrombocyto-penic purpura
Anti-ADAMTS13 antibodies Disease relapse
Pregnancy in SLE Anti-Ro(SSA)/ anti-Ro52 Congenital heart block
Anti-La(SSB) Neonatal lupus
Autoantibody serum screening
Anti-DFS70 ANA-positive healthy individuals
Possible advantages for POC testing of autoantibodies
1. Isotype determination vs Biosensor analysis of β2-glycoprotein I-reactive autoantibodies: evidence for isotype-specific binding and differentiation of pathogenic from infection-induced antibodies. Metzger et al, Clinical Chemistry, 2007, 56:3
2.Affinity of interactionBiomolecular interaction monitoring ofautoantibodies by scanning surface plasmon resonance microarray imaging. Lokate et al, J Am Chem Soc, 2007, 129:14013
3. Epitope “profiling” during active diseaseDiversity of PR3-ANCA epitope specificity in Wegener’s granulomatosis. Analysis using the biosensor technology. Rarok et al, J Clin Immunol, 2003, 23:460

POC modus operandi(Devices with potential to test
autoantibodies at the point-of-care)
Autoantibody Detection Technology/Assay Platform Assay duration
Anti-dsDNA Electrochemical reduction of redox-tagged probe/Ab Inhibition in single-step cell
Decreased resonance frequency/Piezoelectric quartz crystal microbalance
Refractive index change/Surface plasmon resonance sensor chip
~45 min
<60 min
~5 min
Anti-CCP Formation of visual line by colored nanoparticles/lateral-flow chromatography
Refractive index change/Surface plasmon resonance sensor chip
10 min~5 min
Anti-chromatin Peroxidase-mediated electrochemical amplification/ flow-through cell
20 min
Anti-IgG (RF)Anti-MCV
Formation of visual line by colored nanoparticles/lateral-flow chromatography
15 min
Anti-Ro/SSA,Anti-Ro52,Anti-La/SSB
Luminescence by luciferase-tagged probe/ bead immobilized Ab in two-step cells
25 min
Anti-β2-glyco-protein I Refractive index change/Surface plasmon resonance sensor chip
~5 min
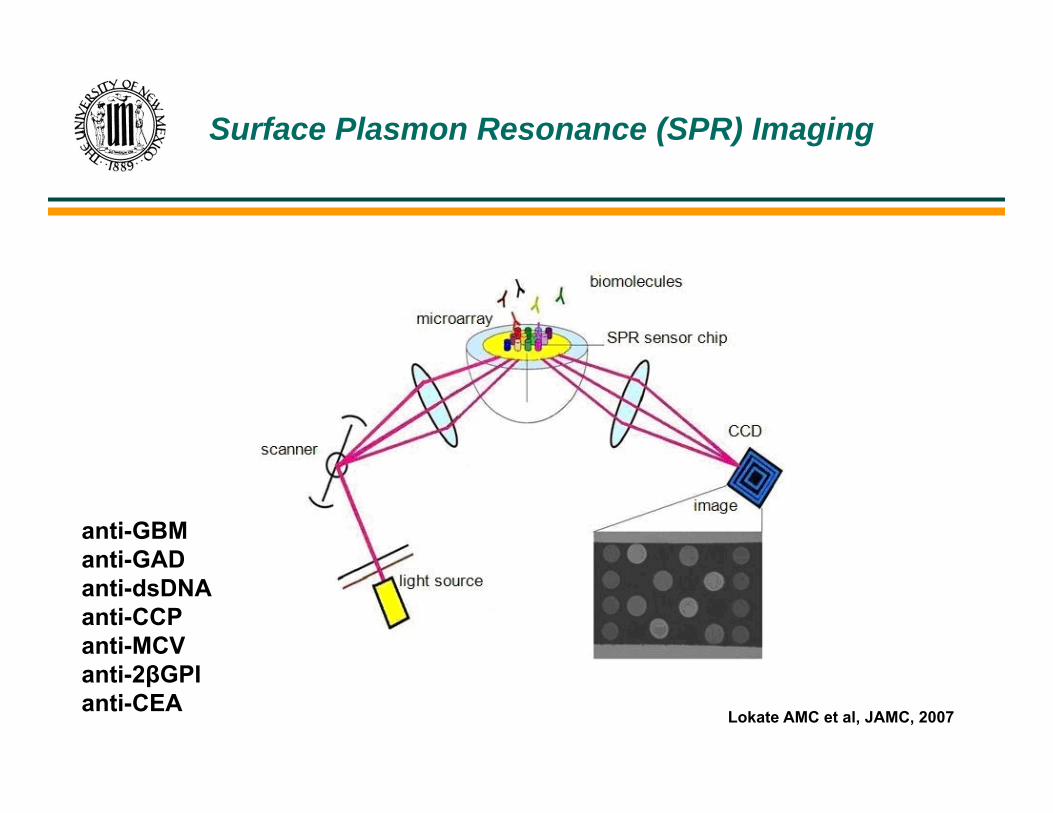
Surface Plasmon Resonance (SPR) Imaging
Lokate AMC et al, JAMC, 2007
anti-GBManti-GADanti-dsDNAanti-CCPanti-MCVanti-2βGPIanti-CEA
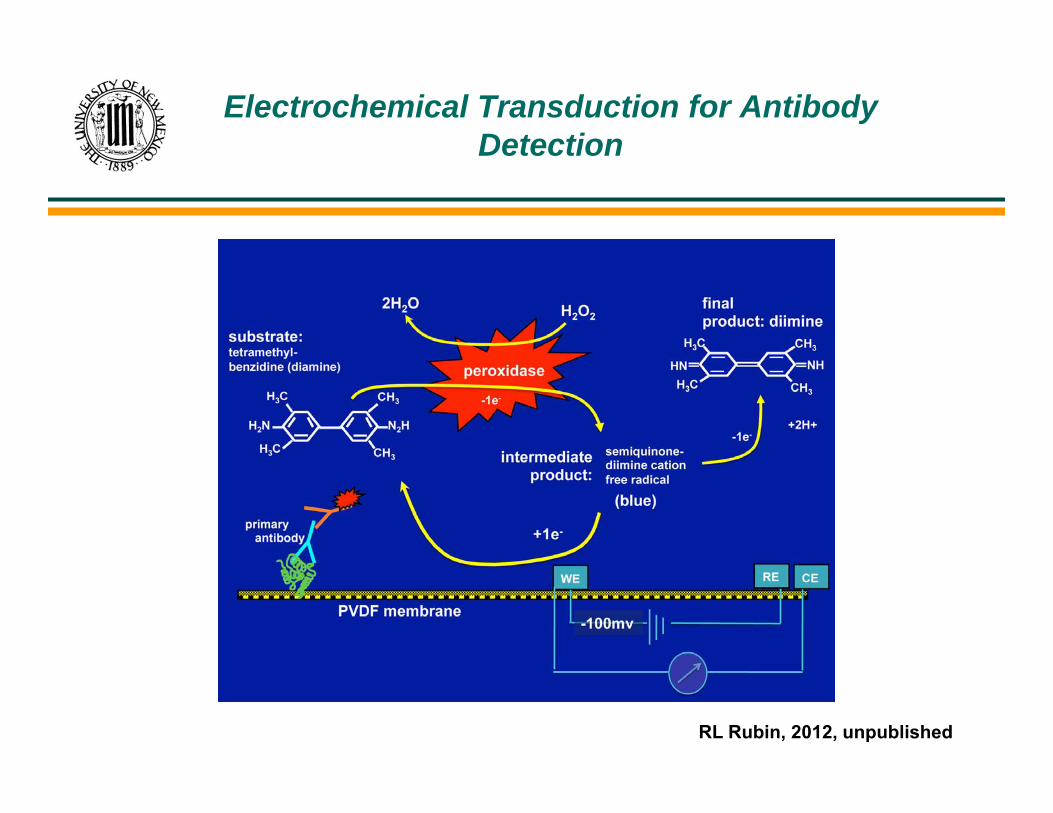
Electrochemical Transduction for Antibody Detection
RL Rubin, 2012, unpublished

Flow through device for measuring antibodies in 8 samples
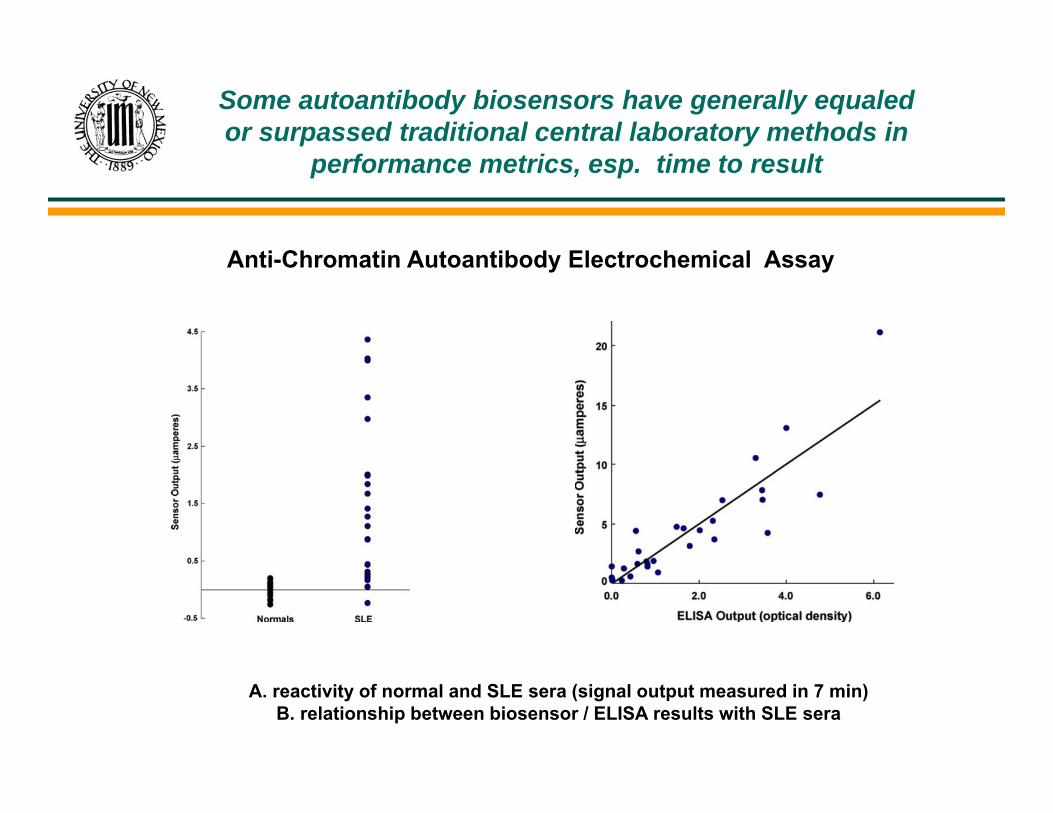
Some autoantibody biosensors have generally equaled or surpassed traditional central laboratory methods in
performance metrics, esp. time to result
A. reactivity of normal and SLE sera (signal output measured in 7 min)B. relationship between biosensor / ELISA results with SLE sera
Anti-Chromatin Autoantibody Electrochemical Assay
Vive la Difference, but…
Surface plasmon resonance-based sensors are the most rapid, but will require adaptation to inexpensive miniaturized devices
Lateral flow based methods will probably be restricted to non-quantitative readouts
Devices requiring specialized antigen tags may have limited practical potential
Electrochemical amplification methods using readily available autoantigens are especially promising.
A Pioneer’s perils
T e c h n i c a l r e q u i r e m e n t s Non-specific binding: any autoantibody specificity is usually a
tiny fraction of total serum immunoglobulin Built-in capacity for data portability, security, and reporting Shelf-life: long-term stability of biological receptor and
transducer in the test environment
R e g u l a t o r y r e q u i r e m e n t s Successful deployment requires long-term commitment Health care managers must invest in POCT programs, rather
than merely purchase rapid tests Regulators and will have to address financial matters and
reimbursement issues
Hold that thought
Autoantibody tests are widely employed by rheumatologists to aiddiagnosis and monitor disease activity and treatment efficacy.
The need for centralized clinical laboratories for measuringautoantibodies impedes ability of physicians to promptly act on thisserological information (ACR position statement on value of de-centralized laboratory testing)
Point-of-care testing for autoantibodies is an emerging technology thatholds promise to enhance the usefulness of these biomarkers forphysicians, resulting in better patient management by providing real-timeautoantibody data while patients remain in the clinic.
William French, 1818–1898, engraver,Die Kranke Frau, Clements C. Fry Collection of Prints and
Drawings, Cushing/Whitney Medical Library, Yale University.
The POC Autoantibody Testingthat Came In From the Cold
Collaborators
Albuquerque, NM, USA
Antonios Tzamaloukas, MD Renal Section, VA Med CenterDavid Wall Voss ScientificKonstantin Konstantinov, MD, PhD. UNM School of MedicineRobert Rubin, PhD UNM, Dept. Mol. Genet & Microbiology