Embed Size (px)
Citation preview
Pocket Lexicon of Clinical Pharmacology
with biostatistical terminology
Edited by:Géza LaknerBéla GachályiJúlia Singer
1/25
Editors:
Lakner, Géza dr.Gachályi, Béla dr.Singer, Júlia dr.
Authors:
Pocket lexicon of clinical pharmacology
Gachályi, Béla dr.Lakner, Géza dr.
Vereczkey, László dr.
Biostatistical terminology
Boda, Krisztina dr.Hajtman, Béla dr.
Lang, ZsoltReiczigel, Jen dr.ő
Singer, Júlia dr.Vargha, Péter
Review:
Vas, Ádám dr.
Special thanks to:
Árvay, Krisztina dr. Mathiász, Dóra dr.Bors, Zsuzsa dr. Nagy, Lajos dr.
Borvendég, János dr. Paál, Tamás dr.Bölcsvölgyi, Tamás dr. Polecsák, Mária dr.Eggenhofer, Judit dr. Róna, Kálmán dr.
Elek, Sándor dr. Sági, ZsuzsannaKarányi, Zsolt Sipos, Adrien dr.
Kovács, Péter dr.
2/25
Contents
INTRODUCTION.......................................................................................................... .4
POCKET LEXICON..................................................................................................... .6
ACRONYMS AND SYMBOLS.................................................................................. .12
THEMATICAL INDEX................................................................................................ .14
LITERATURE............................................................................................................. .16Clinical pharmacology......................................................................................................................17Biostatistics.......................................................................................................................................23
3/25
Introduction
4/25
The Pocket Lexicon of Clinical Pharmacology collects over 800 terms and synonyms from the interdisciplinary field of clinical pharmacology and medical research-related aspects of biostatistics. 500+ entries represent a comprehensive coverage of general clinical pharmacology, human drug development, Evidence Based Medicine, pharmacokinetics and pharmacodynamics, pharmacoeconomy, pharmacoepidemiology, pharmacogenetics and chronopharmacology, as well as important organizations and institutional research formations.
The author team of the Hungarian Society for Clinical Biostatistics has selected 300+ notions in biostatistics and applied numeric analytical methods with detailed descriptions, providing a valuable intellectual asset for the Pocket Lexicon.
Structure of the book
The Pocket Lexicon contains entries in following format: term (acronym) [topic]
Body text is typesetted as plain text. Concepts discussed in current article are formatted in bold-face. Bold-italic highlighting is articulatory. Expressions shown in italic are cross-referenced at the end of current entry (cross-references).---> cross-references
Next, Acronyms and symbols section contains phrasings for mathematical-biostatistical, biochemical and pharmaceutical tokens, and exposes various common and less common abbreviations and acronyms.
The Thematical index provides a quick and easy way to execute thematized searches.
The volume ends with Literature references.
The Pocket Lexicon of Clinical Pharmacology targets various professionals - medical doctors, pharmacists, biologists, biostaticians - engaged in human drug development and clinical research, practizing physicians with special interests in this interdisciplinary science and medical students. In this textbook we sincerely present to the Reader the best of clinical pharmacology as an intersection of an applied pharmaceutical science, a clinical entity and human research methodology.
5/25
Pocket lexicon
6/25
absolute risk reduction (ARR) [EBM]
The absolute arithmetic difference in the event rates of a target variable (endpoint, outcome) between the experimental and the control group. ARR = |EER-CER| , where EER is the experimental event rate, CER is the control event rate.---> absolute risk, event rate, relative risk reduction
ADME [GEN]
The pharmacokinetic plot (graphical representation of drug concentration over time) is a summation of four processes running parallel in the body: Absorption, Distribution, Metabolism and Elimination. The acronym ADME reflects these processes which ultimatively determine the fate of drugs in an organism. An ADME-study is a human study aimed at the observation of pharmacokinetic properties of a drug candidate,---> absorption, distribution, metabolism, elimination
antagonism [PKPD]
~ is a type of drug interaction where the pharmacological effects of some or all concomittantly administered drugs diminish. The ~ may be reversible or irreversible. A different classification for ~s is:• Competitive: The two drugs in interaction connect at the same binding site of the same
receptor, e.g. acetylcholin vs. atropine. In this case the antagonist drug shows affinity to the given binding site but it does not express intrinsic activity (for comparison, see: agonist).
• Noncompetitive: The two drugs fix at different binding sites of the same receptor or at different receptors, e.g. papaverine in higher doses attaches to muscarinerg receptors.
• Indirect: The interacting drug fixes itself on the allosteric binding site.• Competitive-noncompetitive: The antagonist compound acts a competitive one in lower
doses and turns noncompetitive in higher concentrations, e.g. acetylcholine vs. papaverine.
• Functional: Two agonist pharmacons exert opposing effects on different receptors in the same organ / tissue, e.g. histaminergic and β2-adrenergic combined effect on bronchial
musculature.• Physiological: Two agonist pharmacons produce opposing effects on different receptors
of different organs / tissues, e.g. combined effect of the indirect vasopressor activity of heart glycosides and vasodilator activity of hydralazine.
• Chemical: One compound enters into chemical reaction with an another and deactivates the latter regardless of being bound to a receptor or not. Several antidotes, commonly used in oxyology and toxicology fall into this category, e.g. protamine, chelating agents, dimercaptol.
---> agonist
bioavailability [PKPD]
The percentage of total amount of drug administered reaching the systemic circulation in unchanged form. The ~ of intravenous application is 100%, in case of other administration routes - due to absorption and first pass metabolism - it varies and can be remarkably lower than 100%.---> absorption, “first pass” metabolism
7/25
biorhythm [GEN]
~ is the cyclic-periodic biological activity of an organism aimed at the accomodation of the organism to changing environment, hence enhancing survival. Classification:
● by pacemaker of biological rhythm: ● exogenic (external)● endogenic (internal)
● by periodic time: ● ultradian (shorter than a day, e.g. part of day, ebb and flow)● circadian (cca. 24 hours)● infradian (longer than a day)● circaseptan (weekly)● circatrigintan (monthly)● circalunar (lunar month)● circaseasonal (seasonal)● circannual (yearly)
Special presentation of ultradian rhythms are tidal rhythms with phase shift, like phase advance and phase delay. Phase shift may be encountered when flying over multiple time zones on airplane (jet lag) or in case of shift work (night shift). It is thought to be easier to fly from east to west as the day extends (phase delay), rather than the opposite direction, when the day gets reduced (phase advance). A phase delay approach in shift work is also recommended: when changing shifts, it is more advisable to move to a later shift than to an earlier one. Moreover, the slow rotation of shifts is a more beneficial approach than a fast turnover.---> chronopharmacology
blind study [EBM]
Blinding is a study design technique where one or more parties of the clinical study are not informed about the allocation of treatments among trial subject groups (who receives active compound, who receives placebo).
● single blind study: the only uninformed party is the patient● double blind study: neither the subject nor the investigators are in the know of
treatment allocation ● triple blind study: in some special cases even the monitor / sponsor and those who
are responsible for data analysis are uninitiated.The aim of blinding is elimination of subjective factors during observation and analysis, therefore reducing bias. A blind design should be implemented with care, because active and control treatments are to be produced to remain visually indistinguishable and identical regarding their dosing scheme (number of tablets, frequency of administration) which postulates solid manufacturing and accurate organization. If the study drugs in a clinical trial with multiple active therapy arms could not be transformed to be visibly identical (color, shape, formulation), the preparations – depending on their size and formulation – may be hidden in capsules, although this manipulation may yield in gross variations of pharmacokinetic properties. Encapsulation may thus not be the first choice in early phase human studies where pharmacokinetic behavior is a prime question. In this setting the double dummy, or masked administration technique comes handy: a visually
8/25
indistinguishable placebo complement will be manufactured to each active treatment and – if the therapeutic regimes of the active compounds differ – the regimes will also be merged. A novel study design scheme is the Prospective Randomized Open Blinded Endpoint (PROBE) study. The identity of treatments is known to both the patients and researchers but a blinded endpoint committee evaluates the applicable study endpoints. PROBE is similar to a double blind study arrangement regarding its evaluation but it mimics more realistically common medical practice yet being even more cost-effective.
blockbuster drug [GEN]
~s are defined as drugs with 1 billion USD or more in sales revenue during their whole product life-cycle. Mega-blockbusters bring the $1 billion plus in revenue yet in their first year of marketing.
case-control study [EBM]
A study design where the treatment groups are identified by the presence or absence of a particular outcome and the exposure will be analysed retrospectively:
● case group (or cases): patients showing the predefined outcome, i.e. in whom the endpoint in question has occurred
● control group (or controls): in whom the predefined outcome has not occurred.---> observational study
clearance [PKPD]
The amount of plasma which is being “cleared” from a xenobiotic via a certain elimination route (e.g. hepatic, renal).
Total body clearance
CLD
AUCT =
− ∞0 , where D is the dose, AUC0-∞ is the area under the curve.
Renal clearance:
CLU
DCLR T= ⋅ , where U is the total amount of drug excreted in the urine.
Organ clearance (e.g. liver: CLH)CLorgan = Q · E , where Q is the blood flow of the organ, E is the extraction ratio.
Concerning the liver, as a principal party in drug elimination, the drugs can be divided in two groups according to their clearance:
9/25
● high clearance or perfusion-limited compounds (E > 0.8, e.g. propranolol, lidocain), where the elimination is limited by only the hepatic blood flow not the extraction ratio
● low clearance or extraction-limited drugs (E < 0.2, e.g. diazepam), where the drug metabolizing enzyme capacity is the rate limiting factor of the elimination.
---> extraction ratio, elimination, well-stirred model
clinical trial, clinical study (CT) [EBM]
A ~ is medical research conducted in human subjects aimed at the discovery, verification or refinement of the
● pharmacological, clinical- pharmacodynamic effects and/or● pharmacokinetic properties (ADME) and/or● safety profile of a candidate drug.
A ~ is an arrangement for obtaining sound arguments upon a drug’s harmlessness and clinical effectiveness. The terms clinical trial and clinical study are synonymous. In a narrower sense, however, under the term of clinical pharmacology (or preclinical) study pharmacokinetic-safety studies (like phase I or in some cases phase IIa studies) are understood, while phase IIb/III/IV studies are classifed as being ~s.---> ADME, controlled study, observational study, pharmacodynamics, phase I study, phase II study, phase III study, phase IV study, preclinical study, study drug
controlled study [EBM]
A study is controlled when the findings of a treatment group (or treatment groups) are compared to the results of a control group.In prospective studies the control group may be an
● active control group who receive a reference drug or a● placebo control group receiving blank - placebo - preparation.
In reports of retrospective studies the term historical control group may be encountered. In this setting the researcher analyzes past medical documentation, originating from routine medical care and the classification into treatment or control group results from historical data of past exposure.---> case-control study, confirmatory trial, observational study, placebo, randomized controlled clinical trial
essentially similar product [GEN]
A product is regarded as being essentially similar to the original if● the qualitative and quantitative composition of their active ingredients are the same● they are produced in the same drug formulation● the two products are biologically equivalent.
---> bioequivalence, equivalence, generic product
“first pass” metabolism [PKPD]
Drugs entered into the body not directly via blood stream (e.g. by oral route or injected intramuscularly) undergo metabolism in the intestinal mucosa and/or liver prior to reaching the systemic circulation. When applying the same doses per os and intravenously the AUC
10/25
(area under the plasma drug concentration-time curve) for oral administration will be lower than that of the i.v. administration, hence lower the bioavailability.The ~ is a decisive factor upon oral administration, though its effects on various pharmacokinetic parameters should not be neglected in case of intraperitoneal route, either. Rectal administration seems to be an inherently favorable option, because the vena rectalis inferior - playing a prime part in absorption - inosculates into the vena cava inferior, bypassing the vena hepatica system (N.B. Vena rectalis superior and media are branching yet into vena hepatica!). The sublingual administration also minimizes ~ due to branching of vena lingualis into vena azygos / vena cava superior reservoir system.---> bioavailability, area under the plasma drug concentration-time curve, drug metabolism
orphan drug [GEN]
~s are pharmacological entities developed for curing rarely occurring diseases (frequency: USA: < 200 000 patients in total population; EU: < 5 patients / 10 000 inhabitants) like Huntington-chorea, myoclonus, amyotrophic lateralsclerosis, Tourette-syndrome and some muscular dystrophies. Current drug development is based on a statistical approach – the “one drug fits all” principle, because development costs for a small target patient population may not be justified, even in case of market exclusivity. ~ production is rewarded by ensuring benefits for ~ companies through a legislative way (Orphan Drug Act).
pharmacovigilance [GCP]
~ is the continuous tracking of drug treatment safety – monitoring, evaluation and actions taken in the know of safety-related data. ~ in its original context covers activities for recognition, assessment and prevention of adverse drug reactions but in a broader sense, beyond the safety of pharmaceuticals, it includes safety management of herbal extracts (phytovigilance), therapeutic agents of alternative medicine (homeovigilance), blood products (haemovigilance), vaccines (vaccinovigilance), and medical devices (materiovigilance). The ~ also weighs the safety profile of inactive components of therapeutic products (i.e. excipients) and their contribution to safety profile of the whole product. Moreover, ~ oversees the environmental effects of therapeutic products, their possible role in the pollution and also takes drug residuals (e.g. antibiotics, steroides) found in food products of animal origin under scrutiny. Methods for safety monitoring include:
● pre-approval surveillance: system of obligatory expedited adverse event reporting in conjunction with clinical trials, according to ICH-GCP, with special attention to Suspected Unexpected Serious Adverse Reactions (SUSAR)
● postmarketing / post-approval surveillance● passive: voluntary information sources, like spontaneous adverse events
reporting, causality assessment of case-series, literature review, database searches● intensified adverse event reporting: as an extension to spontaneous adverse
events reporting, the marketing authorisation holder may initiate a “campagin” for a shorter time frame (e.g. 6 months), immediately following introduction of a drug product
● active: updates of safety profile with Periodic Safety Update Reports (PSUR) issued by marketing authorisation holder
● research in pharmacoepidemiology
11/25
● drug utilization study (DUS): applied interdisciplinary research technique of pharmacoepidemiology and pharmacoeconimcs, conducted in special populations or patient groups (e.g. children, elderly people, patients suffering from parenchymal diseases; stratification by e.g. gender, age, concomittant medication) to reveal clinical, social and economic aspects and interrelations of drug therapy.
The corrective actions of ~ include alert letters (for manufacturers, clinicians or communication to the public) or modifications to the Summary of Product Characteristics or – as an ultimate measure – withdrawal of marketing authorisation.--> adverse drug reaction, adverse event reporting, marketing authorisation holder, Periodic Safety Update Report, pharmacoeconomics, pharmacoepidemiology, postmarketing surveillance, spontaneous adverse event reporting, Suspected Unexpected Serious Adverse Reaction
phase I study [EBM]
~s are principally pharmacological (preclinical) tolerability or safety studies. The principal aim of these studies is the determination of human tolerability - side effect profile, pharmacokinetics and in some cases pharmacodynamic effects of the study drug. ~ are required in the following cases:
● first human administration of a novel chemical entity,● change in formulation of a previously authorised product,● exploration of pharmacokinetics in subjects with altered metabolism (e.g. in patients
with liver or kidney disease).The trial subjects in a ~ are primarily healthy male volunteers. In some special clinical settings - like human research of antiretroviral products or cytostatics - due to the unjustified, extreme high risk associated with the administration of such potentially toxic compounds to healthy subjects, the participants of oncology and HIV trials are patients suffering from the target disease.---> exploratory trial, study drug, trial subject
Proof Of Concept (Proof Of Principle) study (POC) [EBM]
● In vitro essays or animal models during the preclinial phase of drug development which determine the pharmacological effect of a compound.
● During the human clinical trials, ~s confirm the pharmacological activity and/or clinical efficacy of the drug explored by preclinical data or former (early phase) human studies. The ~s, based on exploratory studies provide evidences of the highest grade in the hierarchy of clinical evidences.
---> confirmatory trial, Evidence Based Medicine, exploratory study
12/25
Acronyms and symbols
13/25
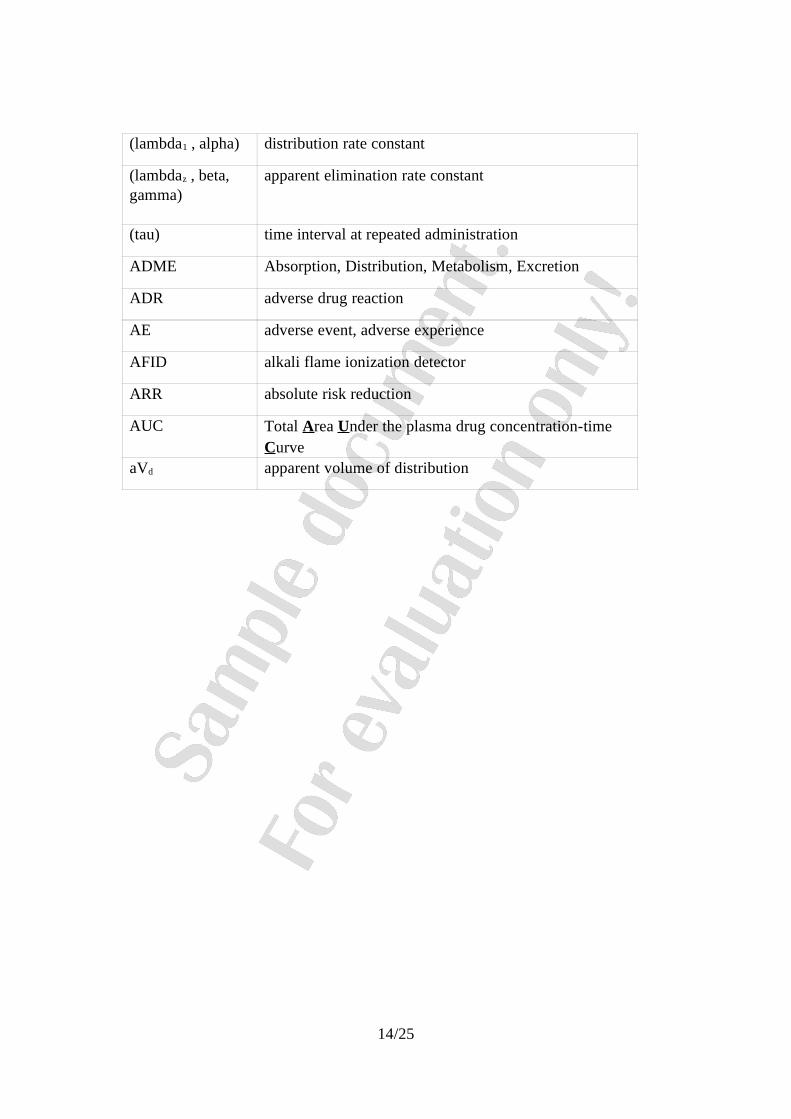
(lambda1 , alpha) distribution rate constant
(lambdaz , beta, gamma)
apparent elimination rate constant
(tau) time interval at repeated administration
ADME Absorption, Distribution, Metabolism, Excretion
ADR adverse drug reaction
AE adverse event, adverse experience
AFID alkali flame ionization detector
ARR absolute risk reduction
AUC Total Area Under the plasma drug concentration-time Curve
aVd apparent volume of distribution
14/25
Thematical index
[EBM] Evidence Based Medicine
[GCP] Good Clinical Practice
[GEN] General clinical pharmacology
[ORG] Organisations, institutions
[PE] Pharmacoeconomy
[PG] Pharmacogenomics
[PKPD] Pharmacokinetics-pharmacodynamics
[STAT] Biostatistics
15/25
[...]
16/25
Literature
17/25
Clinical pharmacology
[1] A gyógyszervizsgálatok helyes klinikai gyakorlata irányelvek bevezetése. Good Clinical Practice. Országos Gyógyszerészeti Intézet, 1992.
[2] A szabályos gyógyszergyártás irányelvei: GMP. Az Országos Gyógyszerészeti Intézet kiadványa. Budapest 1995.
[3] Biron P: La pharmacovigilance de “A” á “Z”; Édition électronique et évolutive, révisée en mars 1999; Département de pharmacologie Faculté de médecine Université de Montréal Montréal, Québec, Canada
[4] Bohaychuk W, Ball G, Lawrence G, Sotirov K: Definicies in Informed Consent Procedures. Applied Clinical Trials, Vol. 7. No. 9 1998 pp. 32-41.
[5] Bohaychuk W, Ball G, Lawrence G, Sotirov K: Ethics Committee and IRB Audit Results. Applied Clinical Trials; Vol.7, No.11. (1998) 46-55.
[6] Borchardt J K: Playing the economics game with outsourcing. Modern Drug Discovery, 2000, 3(2) 28-29, 31-32, 34.
[7] Born P H, Simon C J: Patients and Profits: The Relationship Between HMO Financial Performance and Quality of Care; Health Aff 20(2):167-174, 2001
[8] Borowitz S M: Drug-Nutrient Interactions. Pediatric Pharmacotherapy 1(5), 1995.
[9] Borvendég J és mtsai: Generikus gyógyszerek és törzskönyvezésük. A gyógyszerészeti tudomány aktuális kérdései 11, 5-69, 1994.
[10] Buck M L: The Cytochrome P450 Enzyme System and Its Effect on Drug Metabolism (or Why all the fuss about Seldane®?). Pediatric Pharmacotherapy 3(5), 1997.
[11] Bullock P L: Viewpoint - Pharmacogenetics and Its Impact on Drug Development. Drug Benefit Trends 11(1):53-54, 1999.
[12] Burton S L: An Ethicist's Evaluation of Drug Coverage. Drug Benefit Trends 12(2):58-59, 2000.
[13] Cahill N E, McDermott W E: Cost-Effectiveness Analyses: Legal and Ethical Issues. Drug Benefit Trends 10(2):31-36, 1998
[14] Chalumeau M, Tréluyer J M, Salanave B, Assathiany R, Chéron G, Crocheton N, Rougeron C, Mares M, Bréart G, Pons G: Off label and unlicensed drug use among French office based paediatricians; Arch Dis Child 2000;83:502-505
[15] Combinatorial Chemistry: Novel Strategies, Chemistry, Purification and Chemoinformatics. Drug & Market Development Publications, Oct 1999.
[16] Conroy S, McIntyre J, Choonara I: Unlicensed and off label drug use in neonates; Arch Dis Child Fetal Neonatal Ed 1999;80:F142-F145
[17] Crown W H: Productivity Measurement in Pharmaceutical Studies. Drug Benefit Trends 12(2):5-8 BH, 2000.
18/25
[18] Cutler D M, McClellan M: Is Technological Change In Medicine Worth It? Health Aff 20(5):11-29, 2001.
[19] Detailed guidance on the European database of Suspected Unexpected Serious Adverse Reactions (Eudravigilance - Clinical Trial Module) April 2004; European Commission, Enterprise Directorate-General, Brussels, ENTR/CT 4, Revision 1
[20] Directive 2001/20/EC of the European Parlament and of the Council of 4 April 2001. Az Európai Közösségek Parlamentje és Tanácsa 2001. április 4.-i irányelve a Tagállamok törvényeinek, jogszabályainak és hatósági intézkedéseinek közelítésér l a helyes klinikaiő gyakorlat bevezetésér l az embergyógyászat alkalmazású gyógyszerkészítményekkelő végzett klinikai vizsgálatok során.
[21] Dorian P: Drug-Drug and Drug-Device Interactions. 20th Annual Scientific Sessions of the North American Society of Pacing and Electrophysiology, Day 2 - May 13, 1999.
[22] Dorosz: Guide Pratique des Médicaments. Maloine, 2003.
[23] Drabant S, Klebovich I, Gachályi B, Renczes G, Farsang Cs: Ételinterakciós farmakokinetikai vizsgálatok helye és jelent sége a gyógyszerfejlesztésben: Teofillinő retard, nifedipin retard és buspiron tabletták ételinterakciós vizsgálata. Acta Pharm. Hung. 68: 294-306, 1998.
[24] EFGCP Ethics Working Party: Guidelines and recommendations for European Ethics Committees. EFGCP, Brussels, 1995.
[25] Elek S: A gyógyszer interakciókról. Medicus Anonymus, 2: 2-5, 2002.
[26] Elek S: Az id skori gyógyszer mellékhatásokról. Gyógyszereink, 51:9-14, 2001ő
[27] European Forum for Good Clinical Practice Audit Working Party. Protocol Compliance. (www.efgcp.org)
[28] European Forum for Good Clinical Practice Audit Working Party. The handling of Case Report Form (CRF) at an investigational site. (www.efgcp.org)
[29] European Guidelines for Auditing Independent Ethics Committees. Applied Clinical Trials, 11,6 (2002) 96-101 & 111.
[30] FDA Guidance pages (http://www.fda.gov/cder/guidance)
[31] Fernandez A: Benchmarking Outsourced Trials. Applied Clinical Trials, Vol.7.No.6. (1998) 46-52.
[32] Flexner C: Pharmacokinetics for Physicians - A Primer. Medscape HIV/AIDS eJournal 5(3), 1999.
[33] Fürst Zs (szerk.) : Gyógyszertan. Medicina, 1998.
[34] Gachályi B (szerk.): Bevezetés a klinikai farmakológiába. Springer Hungarica, 1992.
[35] Gachályi B, Róna K: Farmakogenetika, In: Klinikai genetika (Szerk.: Papp Z.), Golden Book, (1995), 640.
[36] Gachályi B, Lakner G, Borvendég J (szerk.) : Klinikai farmakológia a gyakorlatban. Springer Tudományos Kiadó, 2003.
19/25
[37] Gachályi B, Renczes G, Szabó I: A gyógyszerválasztás és a gyógyszerdozírozás speciális szempontjai. In: Humán farmakológia 1270-1283, Medicina, Budapest, 1997.
[38] Gachályi B, Renczes G: Táplálék és gyógyszer-kölcsönhatások. In: Táplálkozás-diéta 179-182. Medicina, Budapest, 1996.
[39] Gachályi B, Róna K, Vas Á: Phenocopy in pharmacogenetics. An issue for controversy? Int. J. Clin. Pharm. Ther.Tox. 28: 490, 1990.
[40] Gachályi B, Vas Á, Róna K, Küpfler A, Káldor A.: Polymorphism of cytochrome P-450 mediated oxidative metabolism.Population studies in Hungary. In: Cytochrome P-450. Biochemistry and Biophysics (Vienna July 3-8. 1988) pp:572-575; Taylor and Francis London- New York-Philadelphia 1989. ed.: Schuster I.
[41] Genomics Glossaries & Taxonomies; Cambridge Healthtech Institute (http://www.genomicglossaries.com)
[42] Getz K: Strategic Sourcing; Applied Clinical Trials ,Vol. 7. No. 6. (1998) 40-42.
[43] Gottlieb H: Medication Nonadherence: Finding Solutions to a Costly Medical Problem. Drug Benefit Trends 12(6):57-62, 2000.
[44] Guidance for Industry E11 Clinical Investigation of Medicinal Products in the Pediatric Population ICH; December 2000.
[45] Guidance for Industry, Bioanalytical Method Validation, FDA, CDER, CVM (2001).
[46] Guideline for good clinical practice (CPMP/ICH/135/95). ICH Secretariat, CPMP Geneva/London 1999.
[47] Guidelines for Good Epidemiology Practices for Drug, Device, and Vaccine Research in the United States. Revised: March 27, 1996. International Society for Pharmacoepidemiology, 1996.
[48] Guidelines on practice of ETHICS COMMITTEES in Medical Research involving HUMAN SUBJECTS (third edition). The Royal College of Physician of London Aug 1996.
[49] Henry C M , Washington C E: Genetic markers such as single-nucleotide polymorphisms may lead to personalized medicines for a wide variety of diseases. August 13, 2001; Volume 79, Number 33; CENEAR 79 33 pp. 37-42.
[50] Hollon T: The making of the pharmacogenomic prescription. GeneLetter 1(12), January 2001.
[51] ICH Harmonised Tripartite Guideline - Clinical Investigation Of Medicinal Products In The Pediatric Population - Topic E11, 2000
[52] ICH Harmonised Tripartite Guideline for Good Clinical Practice. Bookwood Medical Publications, Second Edition 1997.
[53] ICH Topic E8 - NfG. on general considerations for clinical trials (CPMP/ICH/291/95)
[54] International Ethical Guidelines for Biomedical Research Involving Human Subjects CIOMS Geneva 1993.
[55] Is Pharmacoeconomic Analysis Relevant in Formulary Decision-making? Drug Ther Perspect 12(9):14-16, 1998.
20/25
[56] IUPAC Compendium of Chemical Terminology, 2nd Edition (1997)
[57] Jackson K, Young D, Pant S: Drug-excipient interactions and their affect on absorption. PSTT Vol. 3, No. 10 October 2000 pp. 336-345.
[58] Jávor T: Klinikai Farmakológia. Medicina 1980.
[59] Káldor A, Gachályi B, Vas Á: Egészséges-e az "egészséges" önkéntes? Gyógyszereink 39: 26, 1989.
[60] Katz HI: Dermatologist’s Guide to Adverse Therapeutic Interactions. Lippincott-Raven 1997.
[61] Klepser D G: Pitfalls Associated With Commonly Used Methods for Pharmacoeconomic Analyses. Pharmacotherapy 22(2s):35-38, 2002.
[62] Koren G, Pastuszak A: Drugs in Pregnancy. The New England Journal of Medicine, 1998;338: 1128-1137.
[63] Lakner G : Az internet lehet ségei a kórház irányításban I-II. Kórház, 1997/11, pp. 44-46,ő 1997/12, pp. 46-47.
[64] Lakner G, Balkányi L, Surján Gy, Kovács J: Quality of Healthcare related Software Applications - setting up an accreditation system in Hungary; Medical Informatics Europe ‘97. Amsterdam: IOS Press, 1997. pp. 791-795
[65] Lightfoot G D, Getz K A, Harwood F, Hovde M, Rausher S M, Reilly P, Vogel J R: Faster Time to Market. Applied Clinical Trials, Vol. 7. No. 4. (1998) 56-68.
[66] Limon L: Drug Interactions: Decreasing the Risk. APhA 2000 - American Pharmaceutical Association Annual Meeting.
[67] Lippens F J P: Clinical Trials in Central and Eastern Europe. 12-13 October 1999 Budapest, Hungary, abstract book.
[68] Loo J, Riegelman S: New method for calculating the intrinsic absorption rate of drugs. J. Pharm. Sci. 57. 918-928 (1968).
[69] Magyarországi Gyógyszergyártók Országos Szövetsége: Klinikai vizsgálatok Good Clinical Practice (GCP) - ICH irányelvek szerinti tervezése, végzése, ellen rzése éső értékelése.
[70] MAGYOTT Farmakovigilancia Munkacsoport: Kézifüzet a gyógyszer-mellékhatások helyes kezeléséhez egészségügyi szakemberek részére; Magyar Gyógyszertörzskönyvez kő Társasága, 2003. május
[71] MAGYOTT Farmakovigilancia Munkacsoport: Útmutató a gyógyszer-mellékhatások helyes kezeléséhez, 2.kiadás; Magyar Gyógyszertörzskönyvez k Társasága, 2002.ő szeptember
[72] Mancinelli L, Cronin M, Sadee W: Pharmacogenomics: The Promise of Personalized Medicine. AAPS Pharmsci 2000; 2 (1).
[73] McClay N: ‘Better medicines for children’ - Which is the right way forward for Europe? Journal of Generic Medicines.Vol. 1. No 4. 305-312. July 2004
[74] McDonough R P: Improving Outcomes by Identifying and Resolving Problems in Drug Therapy. Drug Benefit Trends 9(2):18,23-25,29-30, 1997.
21/25
[75] McIntyre J, Conroy S, Avery A, Corns H, Choonara I: Unlicensed and off label prescribing of drugs in general practice; Arch Dis Child 2000;83:498-501
[76] Molecular mechanisms of diversity in response to drugs and chemicals in man. Research Group Prof. Urs A. Meyer. http://www.biozentrum.unibas.ch/meyer
[77] Moll F, Bender H: Biopharmazeutische Untersuchungsverfahren. Wissenschaftliche Verlagsgesellschaft mbH, Stuttgart, 1994
[78] Mutschler E: Arzneimittelwirkungen. Wissenschaftliche Verlagsgesellschaft mbH, Stuttgart, 1991.
[79] Müller-Bohn T, Ulrich V: Pharmakoökonomie - Einführung in die ökonomische Analyse der Arzneimittelanwendung. Wissenschaftliche Verlagsgesellschaft mbH, Stuttgart, 2000
[80] Nebert D W, Russell D W: Clinical importance of the cytochromes P450; The Lancet (360) 2002: 1155-1162
[81] Nunn A J: Making medicines that children can take; Arch Dis Child 2003;88:369-371
[82] Nuremberg Code (adopted by the US Tribunal on 19 July 1947). In: Fluss S: International Guidelines on Bioethics. Supplement to the EFGCP News, 2000.
[83] Odedina F T, Sullivan J, Nash R, Clemmons C D: Use of Pharmacoeconomic Data in Making Hospital Formulary Decisions. Am J Health-Syst Pharm 59(15):1441-1444, 2002.
[84] One Size Does Not Fit All: The Promise Of Pharmacogenomics. National Center for Biotechnology Information, Revised November 27, 2001
[85] Operational Guidelines fo Ethics Committees That Review Biomedical Research. WHO Geneva 2000.
[86] Paál T: A helyes laboratóriumi gyakorlat (Good Laboratory Practice, GCP) irányelvei és a megfelelést biztosító intézményrendszer. In Kozák K. (szerk.): Veszélyes anyagok és készítmények. Közgazdasági és jogi Könyvkiadó, Budapest 1998. 75-108.
[87] Paál T: An updated situation of the current compliance within Hungary and other Eastern and Central European countries. In Dent N J (ed.): Good Research Practices. Butterworth-Heinemann, Oxford 1997. 388-420.
[88] Paál T: Anti-generikus program? Gyógyszereink 191-195, 1999.
[89] Paál T: Gyógyszer-törzskönyvezés. In Vizi E.Sz: Humán farmakológia. Medicina, Budapest 1997. 92-111.
[90] Paál T: Hungary. In Brunier, P.D, Nahler, G: International Clinical Trials. Interpharm Press, Denver 1999. 413-443.
[91] Pang K S, Rowland M.: Hepatic clearance of drugs. I. Theoretical considerations of a „well-stirred” model and a „parallel tube” model: Influence of hepatic blood flow, plasma and blood cell binding, and the hepatocellular enzymatic activity on hepatic drug clearance. J.Pharmacokin. Biopharm. 5. 625-653 (1977).
[92] Pharmacovigilance Planning (PVP) E2E - Draft Consensus Guideline; November 2003, ICH Steering Committee
[93] Pizzolanti J M: Nutraceuticals - Food and Drugs. American Society of Consultant Pharmacists Annual Meeting, 1999.
22/25
[94] Post-Approval Safety Data Management: Definitions And Standards For Expedited Reporting E2D; November 2003, ICH Steering Committee
[95] PriceWaterhouseCoopers: Pharma 2005 - An Industrial Revolution in R&D, 1998, pp.13.
[96] Regulation (EC) Of The European Parliament And Of The Council Of The European Union on medicinal products for paediatric use; March 2004, Draft For Public Consultation
[97] Renczes G, Gachályi, B: Élelmiszer-gyógyszerinterakciók. Táplálkozás-Anyagcsere-Diéta 1 (5-6): 2-6, 1996.
[98] Renczes, G, Gachályi B: Életmin ség vizsgálatok a klinikai gyakorlatban. Orvosképzés 71ő (4):195-201, 1996.
[99] Rioux P P, Basilion J P: What's New in Pharmacogenomics? Medscape Pharmacotherapy 2(2), 2000.
[100] Rodvold K A, Meyer J: Drug-Food Interactions with Grapefruit Juice. Infect Med 13(10):868,871-873,912, 1996.
[101] Schaub W: Strategies that work in CRO Relationship; Applied Clinical Trials, Vol. 7. No. 10 (1998) 28-36.
[102] Schumacher J, Klaiberg A, Brähler E: Diagnostik von Lebensqualität und Wohlbefinden - Eine Einführung. In: Schumacher J, Klaiberg A, Brähler E (Hrsg.) - Diagnostische Verfahren zu Lebensqualität und Wohlbefinden. Göttingen: Hogrefe, 2003
[103] Shreve J L, Van Den Bos J, Pedlow K: The Use of Pharmacoeconomic Research by MCOs: An Actuary's View. Drug Benefit Trends 12(2):45-54, 2000
[104] Sietsema W K: Best Practices for Site Start-up and Subject Enrollment. Applied Clinical Trials, Vol.8.No.9.1999 pp. 58-66.
[105] Smith D A, van de Waterbeemd H: Pharmacokinetics and metabolism in early drug discovery. Current Opinion in Chemical Biology 1999, 3:373-378.
[106] SMOs: the Race to Consolidate. CenterWatch, Vol. 4, Issue 3 (1997) 7-19.
[107] Spear B B: Viewpoint - Pharmacogenomics: Today, Tomorrow, and Beyond. Drug Benefit Trends 11(2):53-54, 1999.
[108] Spilker A: The Drug Development and Approval Process; Pharmaceutical Research and Manufacturers of America: www.phrma.org, 2001.
[109] Spilker B: Guide to Clinical Trials, Lippincott-Raven, 1996.
[110] Spilker B: Guide to planning managing multiple clinical studies. Raven Press, New York, 1987.
[111] Spilker B: Guideline to Clinical Studies and Developing Protocols. Raven Press, NY. 1985.
[112] Stephens M D B: The pre-marketing establishment of side-effect profile of a new drugs. In: Detection of New Adverse Drug Reactions (ed. Stephens M D B, Talbot J C C and Routledge P A), Macmillan Reference Ltd, 1998, pp. 197-252.
[113] Swartz M E, Krull I S: Analytical method development and validation, Marcel Dekker, Inc. (1997).
23/25
[114] Tenner A, DeToro I: Teljes kör min ségmenedzsment, M szaki Könyvkiadó, 2001, pp.ű ő ű 26-34.
[115] Text on Validation of Analytical Procedures, Tripartite ICH Text, ICH. Tech Coordination, London, 1994.
[116] The European Agency for the Evaluation of Medicine products: CPMP/EWP/QWP/1401/98 (July 2001).
[117] The Impact of Implementation of ICH Guidelines in Non-ICH Countries; Report of a WHO Meeting Geneva, 13-15 September 2001; Regulatory Support Series, No. 9
[118] The Importance Of Pharmacovigilance - Safety Monitoring Of Medicinal Products, WHO 2002
[119] The U.S. Pharmacopeia Drug Utilization Review Advisory Panel: Drug Utilization Review: Mechanisms to Improve Its Effectiveness and Broaden Its Scope. J Am Pharm Assoc 40(4):538-545, 2000.
[120] Thor S, Fietze I:Einfluss der Tageszeit auf die Wirksamkeit von Medikamenten, 16.04.2001; BSMO - BertelsmannSpringer Medizin Online GmbH.
[121] Trillini B: Grapefruit: the last decade acquisitions. Fitoterapia 71 (2000) 29-37.
[122] Tucker G T: What number of patients is necessary to establish drug safety.In: Clinical Measurement in Drug Evaluation (ed. W. Nimmo and G. Tucker), Wiley 1995, pp. 231-244.
[123] Vas Á, Gachályi B, Káldor A: Bevezetés a kronofarmakológiába. Orvostud. Akt. Probl. 61: 75-84, 1989.
[124] Vas Á, Gachályi B, Róna K, Káldor A: Az oxidatív gyógyszermetabolizmus polimorfizmusa. Orvosképzés 64: 55-62, 1989.
[125] Vas, Á.; Róna, K, Szabó I, Gachályi B: A farmakogenetikai kutatások klinikai jelent sége.ő Lege Artis Medicinae, 2: 320-325, 1992.
[126] Veenstra D L, Higashi M K, Phillips K A: Assessing the Cost-Effectiveness of Pharmacogenomics. AAPS Pharmsci 2000; 2 (3).
[127] Vitillo J A: Adverse Drug Reaction Surveillance: Practical Methods for Developing a Successful Monitoring Program, Medscape Pharmacists, 2000.
[128] Vizi E Sz: Humán farmakológia. Medicina Könyvkiadó. Budapest, 1997.
[129] Vogel J R: Maximizing the Benefits of SMOs. Applied Clinical Trials, Vol. 8. No. 11. (1999) 56-62.
[130] Wagner J, Nelson E: Per cent absorbed time plots derived from blood level and/or urinary excretion data. J. Pharm. Sci. 52. 610-611 (1963).
[131] Weiland A J: The Challenges of Genetic Advances. Healthplan 41(6):24-30, 2000
[132] Weiss S R: Prescription Medication Use in Pregnancy. Medscape Pharmacotherapy 2(2), 2000.
[133] Williams J I: The Unanswered Challenges in Measuring Quality of Life. Canadian Journal of Nursing Research 30(4): 295-298, 1999.
24/25
[134] Wilson AE: De-Mystifying Pharmacoeconomics. Drug Benefit Trends 11(5):56-67, 1999.
[135] Woodward R S: Becoming a Good and Valued CRO Client. Applied Clinical Trials, Vol. 7. No. 6. (1998) 76-82.
[136] Woodward R S: Choosing a Contract Research Organization; Applied Clinical Trials, Vol 6, No. 6 (1997) 66-72.
[137] World Medical Association Declaration of Helsinki (as amended last by the 52nd World Medical Association General Assembly, Edinburgh, 2000)
Biostatistics
[138] Ádány R, Hajdu P. Epidemiológiai szótár. Medicina Könyvkiadó, Budapest, 2003.
[139] Altman, DG : Practical statistics for medical research, Chapman Hall, London, 1991.
[140] Armitage P: Statistical Methods in Medical Research. pp. 184-188. Blackwell, 1971.
[141] Bolton S: Pharmaceutical Statistics. pp. 187-202. 2nd ed. Marcel Dekker, Inc., 1990.
[142] Day S.: Dictionary for Clinical Trials, Wiley, Chichester, 2001.
[143] Fleiss, J. L. The Design and Analysis of Clinical Experiments. Wiley, New York, 1986.
[144] Hajtman B: Bevezetés a matematikai statisztikába pszichológusok számára. Akadémiai Kiadó, Budapest, 1968.
[145] ICH E3. Structure and Content of Clinical Study Reports, July 1996
[146] ICH E4. Dose-Response Information to Support Drug Registration, November 1994.
[147] ICH E6. Good Clinical Practice: Consolidated Guideline, May 1996.
[148] ICH E8. General Considerations for Clinical Trials, December 1997.
[149] ICH E9. Statistical Principles for Clinical Trials - September 1998.
[150] Jánossy, A, Muraközi, T, Aradszky, G (szerk.): Biometriai Értelmez Szótár.ő Mez gazdasági Kiadó, Budapest, 1966.ő
[151] Pereira-Maxwell F: A-Z of Medical Statistics. Arnold, London, 1998.
[152] Snedecor, GW and Cochran, WG: Statistical Methods. The Iowa State University Press, Iowa, 1979. Sixth Edition, Tenth printing
[153] Vargha A: Matematikai statisztika pszichológiai, nyelvészeti és biológiai alkalmazásokkal. Pólya Kiadó, Budapest, 2000.
25/25