Embed Size (px)
Citation preview
PNEUMONIA
Prof T Rogers
THE IMPORTANCE OF PNEUMONIA
• A major killer in both developed and developing countries
• Accounts for more deaths than other infectious diseases
• Mortality rates vary but can be as high as 25%
• A major cause of death in children in developing countries
• Incidence here (?) 2-5/1000 population
PNEUMONIA
• Neither radiological or microbiological criteria are specific for predicting the cause of pneumonia
• A better approach is to first consider the clinical circumstances under which pneumonia acquired
• Add the clinical background of the particular patient…
Classification of pneumonia
• Community-acquired
• Hospital-acquired
• Aspiration and anaerobic
• Pneumonia in immunocompromised
• AIDS-related
• Geographically restricted
• Recurrent
COMMUNITY-ACQUIRED PNEUMONIA: INTRODUCTORY POINTS
• More common at the extremes of age
• Twice as common in winter months
• A General Practitioner is likely to see up to 10 cases per yr
• Represent <10% of all respiratory infection cases prescribed antibiotics
• Most will be managed in the community
TYPES OF COMMUNITY ACQUIRED PNEUMONIA
• In a previously healthy individual
• Here the infection may have been acquired by droplet spread from another
• Alternatively, in patients with underlying diseases endogenous colonizing bacteria may be the cause
• These are more likely to be resistant to first-line antibiotics
SYMPTOMS OF PATIENTS WITH COMMUNITY-ACQUIRED PNEUMONIA(%)
[Mc Farlane unpublished]
• Cough 92• Fever 86• Breathlessness 67• Pleural pain 62• Headache 55• New sputum production 54• Muscle aches 44• Nausea/vomiting 48
British Thoracic Society CAP severity assessment:
CURB 65 score
• Any of: confusion, urea> 7mmol/l, respiratory rate>30/min, blood pressure systolic <90mmHg diastolic<60mmHg, age>65 years
• Low (0-1), moderate (2), high (3+) severity• Will help determine where treated (home vs
hospital), and likely mortality.• ICU admission indicated by CURB score of 4-5
COMMUNITY ACQUIRED PNEUMONIA: WHAT’S CAUSING IT?
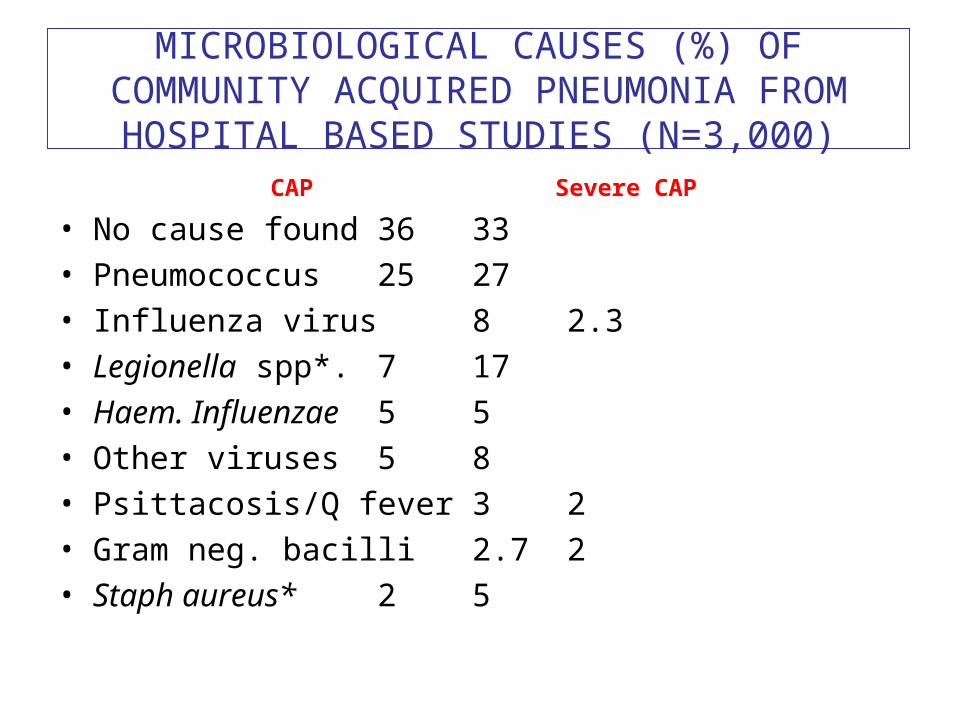
MICROBIOLOGICAL CAUSES (%) OF COMMUNITY ACQUIRED PNEUMONIA FROM
HOSPITAL BASED STUDIES (N=3,000)CAP
Severe CAP
• No cause found 36 33• Pneumococcus 25 27• Influenza virus 8 2.3• Legionella spp*. 7 17• Haem. Influenzae 5 5• Other viruses 5 8• Psittacosis/Q fever 3 2• Gram neg. bacilli 2.7 2• Staph aureus* 2 5

INVESTIGATIONS FOR DIAGNOSIS OF PNEUMONIA
• Non-invasive: blood count, urea, albumin,LFT’s, sputum gram, chest X-ray, CT scan
• Culture of sputum, blood, pleural fluid
• Serology: pneumococcal, Legionella antigen
• Invasive: induced sputum, bronchoscopy, open lung biopsy
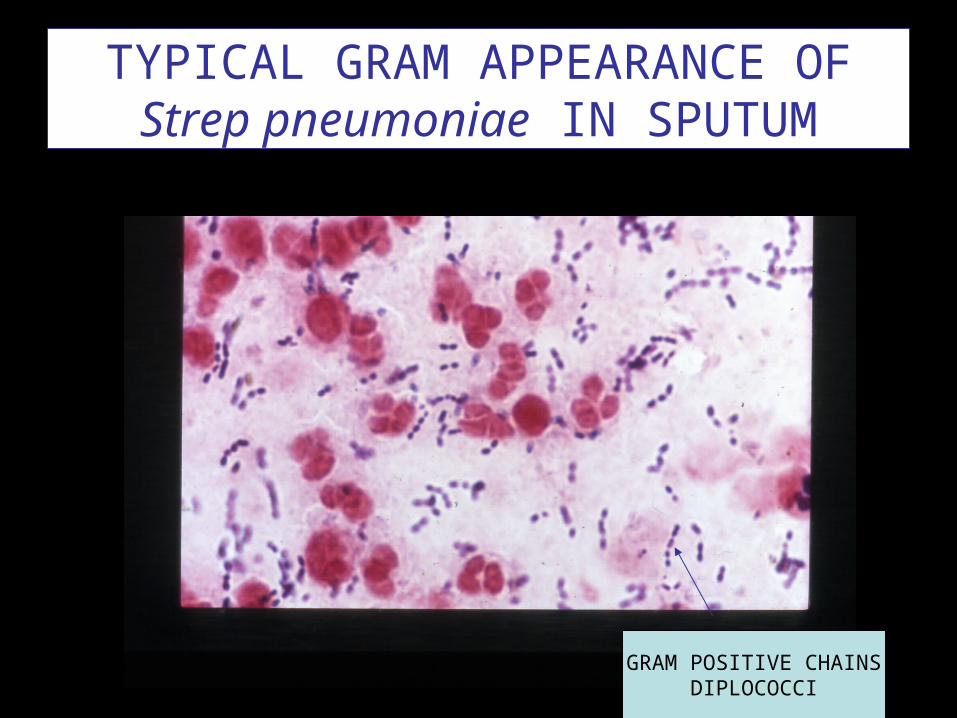
TYPICAL GRAM APPEARANCE OF Strep pneumoniae IN SPUTUM
GRAM POSITIVE CHAINSDIPLOCOCCI
Streptococcus pneumoniae (pneumococcus)
• A gram positive coccus that grows in short chains
• Alpha haemolytic on blood agar
• Identified by its susceptibility to optochin
• Polysaccharide capsule confers pathogenicity-at least 80 serotypes
• There are multivalent vaccines for prevention of pneumococcal disease
SOME COMPLICATIONS OF PNEUMOCOCCAL SEPSIS
• Bacteraemia (10%+)
• Empyema (1%)
• Meningitis (<0.5%)
• Mortality rates of 10-25%
• Splenectomy or asplenia a major risk factor
Pneumococcal vaccine is recommended for:
• Age >65 years
• Underlying chronic lung disease
• Asplenia
• Alcoholism
• Diabetes mellitus
• Chronic renal failure
• HIV infection
VIRUSES THAT CAUSE COMMUNTIY ACQUIRED PNEUMONIA

INFLUENZA
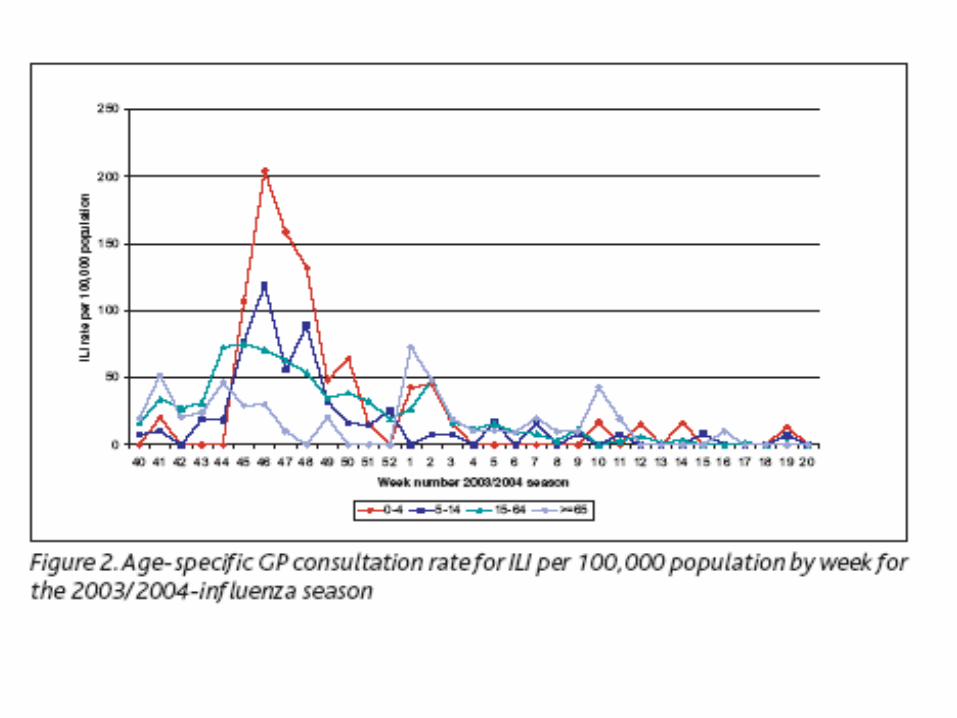
© March Issue of Epi-Insight, Vol 6, Issue 3, Health Protection Surveillance Centre, Ireland

Pandemic influenza H1N1
• An acute respiratory illness• Sudden onset of: fever (>38oC), headache,
cough, sore throat, muscle aches, pneumonia
• Transmitted by respiratory droplets from coughing, sneezing, and from “infected” surfaces.
• 1,613 cases confirmed with 4 deaths in Ireland up to 3rd October
Underlying diseases with an increased risk of severe influenza
• Chronic lung, liver, CNS, conditions, • Immunosuppression• Diabetes mellitus• Asthma• Age <5 years or >65 years• Severely obese (BMI 40 or more)• Pregnancy• haemoglobinopathies
Preventing the spread of pandemic (swine) influenza
• Wash hands with soap and water
• Avoid unnecessary contact with cases
• Avoid touching eyes, nose , mouth
• Cover mouth and nose with tissue
• Patients admitted to hospital who have a confirmed diagnosis will be nursed in a negative pressure room
• HCW’s wear protective clothing
Treatment and prevention of pandemic influenza H1N1
• Oseltamivir treatment of severe cases
• Can also be considered as antiviral prophylaxis in selected high risk patients
• Should be used prudently because of risk of drug resistance
• Vaccine about to be issued, will include provision for health care workers
AVIAN
FLU

OTHER VIRAL CAUSES
• Respiratory syncytial virus (RSV)
• Parainfluenza viruses
• Enteroviruses
• (Cytomegalovirus)

© July 2003 issue of Virus Alert, bulletin of the National Virus Reference
Laboratory
SARS

Severe Acute Respiratory Syndrome (SARS)
o Identified in Guangdong Province, China, in November 2002
o Rapidly spread to Hong Kong, South East Asia, North America..The World
o By the end of outbreak in June 2003 more than 8,000 cases had occurred with >800 deaths
o Person to person transmission demonstrated
CAUSES OF ‘ATYPICAL’ PNEUMONIA
• Mycoplasma pneumoniae
• Chlamydia pneumoniae
• Legionella pneumophila
• Coxiella burnetii
Mycoplasma pneumoniae
• Has no cell wall, therefore doesn’t respond to beta lactams
• Causes atypical pneumonia in adolescents and young adults
• Dry hacking cough, low grade fever, headache feature
• Isolation by culture of the organism is difficult therefore diagnosis is confirmed by a high CFT or rising titre of specific antibodies
• Cold agglutinins also typical• Macrolides or tetracyclines most active
Chlamydia pneumoniae
• An obligate intracellular bacterium
• Causes mild pneumonia but may cause protracted symptoms
• Sore throat, hoarseness, URT symptoms feature
• Serological diagnosis rather than culture
• Tetracyclines, macrolides, quinolones active
Legionnaires’ disease
• A severe pneumonia due to Legionella pneumophila
• Can be community or hospital acquired
• Organism is acquired from environmental sources eg, humidified air conditioning, showers
• Usually attacks debilitated individuals
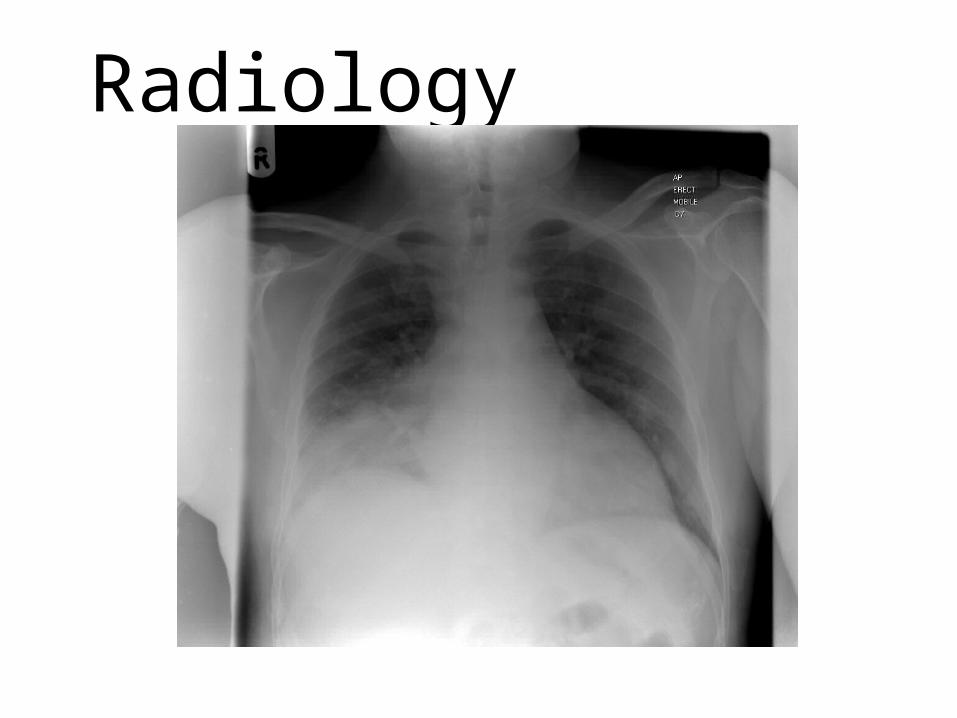
Radiology
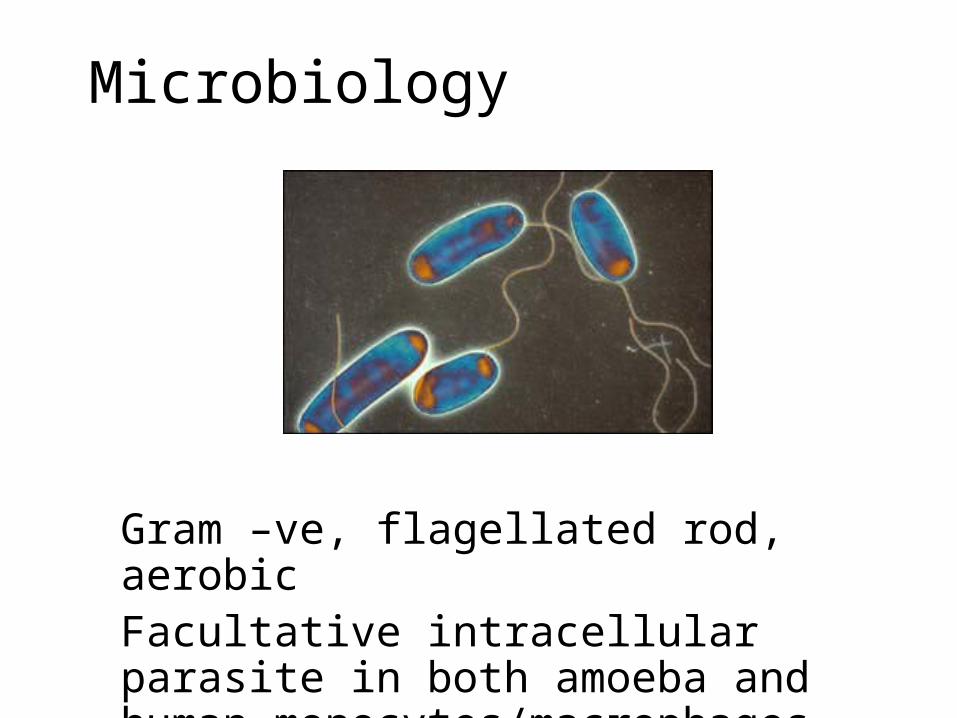
Microbiology
Gram –ve, flagellated rod, aerobicFacultative intracellular parasite in both amoeba and human monocytes/macrophages
RISK FACTORS
• Male sex
• Advanced age
• Cigarette smokers
• Alcoholism
• Chronic lung disease
• Immmunosuppression, malignancy
Legionnaires’ disease
• Hyponatremia, confusion, nausea, vomiting, abnormal LFT’s a feature
• Diagnosis often confirmed by urinary antigen test (specific for serogroup 1)
• Can be cultured on special media• Must be notified to Public Health as it can
cause outbreaks• Most active antibiotics are: macrolides,
quinolones, rifampicin
Antibiotic Treatment of Community Acquired Pneumonia
• The priority is to cover pneumococcus
• Penicillin, amoxycillin, cephalosporins, new quinolones and macrolides have all been used as monotherapy
• Choice will be influenced by local resistance rates for pneumococcus
Examples of antibiotics for CAI
• Benzylpenicillin
• Penicillin V
• Ampicillin, amoxycillin, Augmentin
• Cefuroxime, cefotaxime, ceftriaxone
• Moxifloxacin (a quinolone)
• Erythromycin, clarythromycin, azithromycin
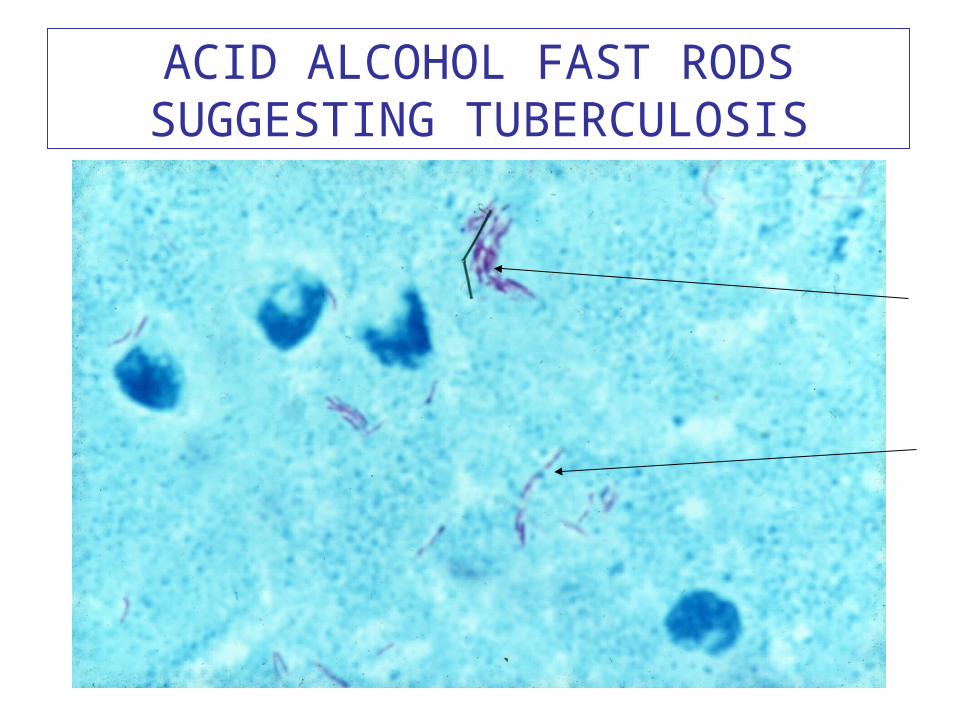
ACID ALCOHOL FAST RODS SUGGESTING TUBERCULOSIS
KLEBSIELLA PNEUMONIA (RARE)
COMMUNITY ACQUIRED PNEUMONIA IN INFANTS AND CHILDREN
• Group B streptococcus and E coli cause pneumonia in neonates
• RSV an important pathogen in infants
• Bordetella pertussis (cause of whooping cough) important in young children
• As is Haemophilus influenzae type b

SOME FEATURES OF NOSOCOMIAL PNEUMONIA
• Often ventilator associated, therefore seen in ITU most commonly
• Due to both endogenous organisms and others acquired by cross infection
• MRSA, gram negatives predominate
• High associated mortality because of co-morbidity and antibiotic resistance
HOSPITAL ACQUIRED PNEUMONIA: Pseudomonas aeruginosa

TREATMENT OF HOSPITAL ACQUIRED PNEUMONIA
• Will depend on the local epidemiology of the unit/hospital
• Often require good cover for MRSA and gram negative enterobacteria
• Therefore vancomycin and carbapenem or Tazocin may be used
PNEUMONIA IN THE IMMUNOCOMPROMISED HOST
• Cause depends on the underlying immunodeficiency
• More likely to present as a diffuse interstitial pneumonia
• Treatment often empirical as establishing the cause is often difficult

MAJOR CAUSES OF PNEUMONIA IN IMMUNOCOMPROMISED
• Pneumocystis jiroveci (carinii)
• Cytomegalovirus
• Other respiratory viruses
• Tuberculosis
• Fungi

Pneumocystis jiroveci(Lung biopsy)
Cyst stage
NOCARDIOSIS(Cause: Nocardia asteroides, acid fast rod)
Geographically restricted pneumonias
• Typhoid
• Melioidosis
• Brucellosis
• Endemic mycoses: histoplasmosis
• Helminthic: paragonimiasis
Recurrent pneumonia
• May be caused by local bronchial or pulmonary abnormality
• Obstruction due to eg, foreign body, carcinoma, lymph node
• Chronic obstructive lung disease: bronchiectasis• Neurological disorders: motor neurone disease• Structural: tracheo-oesophageal fistula• Aspiration (alcoholics): anaerobic organisms• Immunodeficiency state:
hypogammaglobulinaemia
EMPYEMA
• May arise as an acute complication of pneumonia• Characterised by collection in pleural cavity, malaise,
fever, pleuritic pain, leucocytosis• Chronic empyema usually occurs after failure to
diagnose or treat adequately an acute empyema• May be loculated, or associated with a broncho-pleural
fistula• Organisms are those causing the original pneumonia, or
anaerobes• Treat by drainage of the collection and antibiotics after
microbiological findings