Pneumatic retinopexy Pneumatic retinopexy (PR) is an
office-based nonincisional procedure that has become a
well-accepted alternative to scleral buckling and vitrectomy for
the repair of selected cases ofrhegmatogenous retinal detachment,
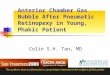
as depicted in the images below.[1, 2]Patient with a rhegmatogenous
retinal detachment secondary to a single horseshoe tear prior to
pneumatic retinopexy.Patient with a rhegmatogenous retinal
detachment secondary to a single horseshoe tear 24 hours after
pneumatic retinopexy; the retina is completely attached. Notice the
intraocular gas bubble.Pneumatic retinopexy is a 2-step procedure.
In the first step, an expanding gas bubble is injected into the
vitreous cavity and the patient is positioned so that the bubble
closes the retinal break, permitting resorption of subretinal
fluid. The second step entails induction of a chorioretinal
adhesion around all retinal breaks with cryopexy, laser, or
both.[3, 4, 5]The main advantage of pneumatic retinopexy over
scleral buckling is the minimization of complications such as
inadvertent scleral perforation by scleral sutures, postoperative
refractive error changes, strabismus, and the complications
associated with the drainage of subretinal fluid.The initial
success rate of pneumatic retinopexy is lower than that of scleral
buckling, but the final anatomic and functional results are
comparable. The lower initial success rate is due to a higher
frequency of new retinal breaks and missed retinal breaks.However,
an initial failure of pneumatic retinopexy does not affect the
final visual outcome.[6, 7, 8, 9, 10, 11]In a comparative trial of
eyes with rhegmatogenous retinal detachment involving the macula
for 14 or less days, the visual outcomes following pneumatic
retinopexy were statistically better than those following scleral
buckling.[12]A recent study showed that if pneumatic retinopexy
were more popular, significant cost savings may be
achieved.[13]IndicationsNot all patients with a rhegmatogenous
retinal detachment are good candidates for pneumatic retinopexy
(PR). Case selection is an important determinant of success.In
general, the best candidates for pneumatic retinopexy are those who
have a single retinal break or group of retinal breaks that are not
larger than 1 clock hour (30) and that are located in the superior
8 clock hours of the globe. Furthermore, the patient must have the
ability to maintain a proper head position for at least 16 hours
per day for 5 days or more.Patients with a retinal detachment not
satisfying these criteria are expected to have much poorer
responses to pneumatic retinopexy than those who do. Predictors of
treatment failure for pneumatic retinopexy include eyes with a
vitreous hemorrhage, a retinal detachment extending more than 4.5
clock hours, pseudophakia, proliferative vitreoretinopathy, visible
vitreous traction on a tear, and/or a retinal break greater than 1
clock hour.[13, 14, 15]ContraindicationsPresence of retinal breaks
within the lowest 4 clock hours of the inferior quadrantsFor an
average eye, 0.3 mL of gas covers 90 of the retinal surface in an
emmetropic eye. In contrast, 1.6 mL of intraocular gas is necessary
to cover 150 of the retinal surface.[4, 5]Thus, even after full
expansion of a 0.3-mL bubble of pure perfluoropropane (C3F8) to 1.2
mL, the inferior retina will not be covered by the gas bubble
unless the patient assumes an extreme head position.Most patients
cannot tolerate the 90 neck flexion or hyperextension position
required for proper gas tamponade of the retinal breaks in the
inferior quadrants.[4, 16]Even though some reports showed the
successful repair of selected cases of retinal detachments along
the inferior 4 clock hours (4 to 8 oclock),[17]pneumatic retinopexy
(PR) usually fails to repair such detachments.Presence of
proliferative vitreoretinopathy grade C or DA retinal detachment
with substantial proliferative vitreoretinopathy (PVR) that exerts
considerable retinal traction is not a good candidate for pneumatic
retinopexy. For an optimal outcome, the basic criteria for
pneumatic retinopexy require the absence of PVR grade C or D.
However, a successful outcome with pneumatic retinopexy has been
reported for retinal detachments with limited grade C
PVR.[4]Noncompliance with required head positioningRetinal breaks
outside the 11 to 1 clock hours in the superior quadrants require
more extreme head tilt positioning following pneumatic retinopexy
that may be difficult for patients with certain physical
disabilities, neck and back problems, or mental
incompetence.[4]Severe glaucomaWith the exception of advanced
glaucoma, most eyes with concomitant retinal detachment and
glaucoma can be safely managed with pneumatic retinopexy, as long
as the intraocular pressure is closely monitored and corrective
measures taken, if necessary.[4]Hazy mediaOcular opacities such
asvitreous hemorrhageor a dense cataract may impede the
identification of all retinal breaks, lowering the success
likelihood of pneumatic retinopexy. Certain aphakic and
pseudophakic eyes with multiple small peripheral retinal breaks in
the presence of cloudy peripheral lens capsule are also poor
candidates for pneumatic retinopexy.[4]AnesthesiaMost patients
undergo pneumatic retinopexy under subconjunctival anesthesia
supplemented by topical drops.When cryotherapy is being considered,
retrobulbar anesthesia allows comfortable scleral depression,
permits cryotherapy to any quadrant, and prevents a vagal response
that may occur if the intraocular pressure is temporarily raised to
a high level.In the rare instance thatgeneral anesthesiais used,
the surgeon must remind the anesthesiologist to avoid nitrous oxide
in order to prevent postoperative shrinkage of the intraocular gas
bubble.[4, 5]EquipmentEquipment used for pneumatic retinopexy
includes the following: Cyclopentolate 1% and phenylephrine 2.5%
drops to dilate the pupil Topical anesthesia drops A lid speculum
Povidone-iodine solution drops, 5% Millipore filter, 0.22 m
Syringe, 1 mL Needle, 27 or 30 gauge C3F8or sulfur hexafluoride
(SF6) Cotton-tipped applicators Indirect ophthalmoscope Laser
and/or cryotherapyPositioningFollowing the gas injection, the
patients head is immediately positioned so that the gas bubble is
opposed directly to the break. If the retinal detachment does not
involve the macula but threatens it, the steamroller technique
should be seriously considered to prevent subretinal fluid
displacement into the macula.Steamroller techniqueIn the
steamroller technique, the patients head is initially turned to a
face-down position, as depicted in the first image below. Over
10-15 minutes, the position is gradually changed until the retinal
break is uppermost, as depicted in the second image below, causing
the bubble to roll toward the retinal break, pushing the subretinal
fluid away from the macula and back into the vitreous cavity
through the retinal break, flattening the retina. See the third
image below.Steamroller technique. A patient with a superotemporal
break in the right eye. The patient's head is initially turned to a
face-down position.Steamroller technique. A patient with a
superotemporal break in the right eye. Over 10-15 minutes, the
position is gradually changed until the retinal break is
uppermost.Steamroller technique. A patient with a superotemporal
break in the right eye. Final head position.One of the theoretical
disadvantages of the steamroller technique is the potential for
proliferative vitreoretinopathy development. Since the subretinal
fluid is displaced back into the vitreous cavity during this
maneuver, retinal pigment epithelium (RPE) cells might gain access
to the retinal surface.Yanyali et al (2007)[18]prospectively
compared the steamroller technique to the basic technique and
concluded that both techniques appear to be equally effective and
safe in terms of the development of proliferative
vitreoretinopathy. Their study was not designed to assess the
effectiveness in preventing macular detachment in high-risk
eyes.[18]It is recommended to maintain the specified head position
for up to 16 hours per day for at least 5 days.[5]TechniqueAfter
dilating the pupil, 3-5 drops of topical anesthesia are instilled
in the eye. Anesthetic is injected in the subconjunctival at the
injection site. A lid speculum is inserted, and 3 drops of 5%
povidone-iodine solution are instilled and left in place for 5
minutes. Aqueous humor (0.3-0.5 mL) is removed from the anterior
chamber via a paracentesis to lower the intraocular pressure. See
the images below.After a subconjunctival injection of lidocaine 1%
and topical anesthesia, a lid speculum is placed. A 5% povidone
iodine solution is used to clean the conjunctival surface.Aqueous
humor (0.3 to 0.5 mL) is removed from the anterior chamber via a
paracentesis to lower the intraocular pressure.Either 0.3 mL of
C3F8or 0.5 mL of SF6is filtered through a Millipore filter (0.22 m)
into a 1-mL syringe with a short (half-inch) 27- or 30-gauge
needle. See the image below. Most surgeons perform the gas
injection with the patient lying in a supine position. For some
eyes, performing the gas injection with the patient in the upright
position has certain advantages. For instance, the upright position
during gas injection reduces the tendency for gas migration and
vitreous prolapse into the anterior chamber in the setting of
elevated intraocular pressure, although this technique should be
avoided in the presence of a large retinal tear to prevent
formation of fish-egg bubbles.[4]Either 0.3 mL of C3F8 or 0.5 mL of
SF6 is filtered through a Millipore filter (0.22 m) into a 1-mL
syringe with a short (half inch) 27- or 30-gauge needle.If the
patient is aphakic or pseudophakic, the injection is placed 3 mm
posterior to the limbus. If the patient is phakic, the injection is
placed 4 mm posterior to the limbus. With the patient in the supine
position, the surgeon should inject the gas at an upper position of
the globe and point the needle perpendicular to the sclera and
downward toward the center of the vitreous cavity.[4, 18]After
inserting half of the needle into the vitreous cavity, the needle
should be partially withdrawn until only 1 mm is still in the eye.
A slow injection of gas through the shallowly inserted needle
allows continued gas placement into the same single enlarging gas
bubble, avoiding the formation of fish-egg bubbles.[19]The gas
should also be injected away from any large retinal break to reduce
the risk of subretinal gas migration.[4]See the image below.After
inserting half of the needle into the vitreous cavity, withdraw
needle until only 1 mm is in the eye. Inject gas slowly through the
shallowly inserted needle for continued gas placement into the same
single enlarging gas bubble. Inject gas away from any large retinal
break to reduce the risk of subretinal gas migration.If multiple
bubbles are present, the patient should remain in a position to
keep the small bubbles away from a large retinal break for 24
hours. The fish-egg bubbles usually coalesce over 12-24 hours. As
the needle is withdrawn, a cotton-tipped applicator is placed over
the perforation site, and the patients head is rotated to prevent
gas from escaping through the puncture site.Afterward, the surgeon
must perform indirect ophthalmoscopy to confirm the placement of
the gas into the vitreous cavity and to assess the perfusion of the
central retinal artery. If the artery remains nonpatent and
nonpulsatile 10 minutes after gas injection, a paracentesis is
repeated to reduce the risk of ischemic retinal damage. Elevated
intraocular pressure is usually not a significant problem after the
intraocular injection of less than 0.5 mL of gas. Immediate
elevation of intraocular pressure to levels between 30 and 50 mm Hg
is common, but pressure returns to normal after 90 minutes.In
certain situations, cryopexy can be omitted and laser may be
applied a few days later when the break has flattened.Tornambe
(1997) found a single operation success rate of 55% for focal
retinopexy compared to 85% for 360 retinopexy.[20]If all breaks
have been closed, the retina usually attaches within 24 hours.[4,
5, 21]PearlsPearls for pneumatic retinopexy (PR) include the
following: Patient selection is key to success. Perform
paracentesis prior to gas injection. Avoid performing pneumatic
retinopexy in eyes in which the retinal periphery is not adequately
visualized. Insert the needle into the vitreous cavity and then
retract it so that the tip is just barely in the vitreous cavity.
This will allow for a shallow injection. Then, inject slowly. This
will reduce the risk of fish egg bubbles. If fish egg bubbles
develop, try coalescing them into a single bubble by striking the
globe with a finger or a cotton tip applicator. If multiple breaks
are present over an area equivalent to several clock hours, treat
the most superior breaks first. Consider prophylactic 360
peripheral laser barricade to reduce the risk of new and/or missed
retinal breaks. Have a low threshold and ability to recognize when
the procedure has failed and when to move on to scleral buckling
and/or vitrectomy.ComplicationsNew or missed breaks and surgical
failureThe development of new retinal breaks with a subsequent new
retinal detachment following pneumatic retinopexy (PR) has been
reported at a rate of 7%-22%.[12, 22, 23, 24]New or missed breaks
may develop in any quadrant; however, 76% are located in the
superior 8 clock hours. The progressive vitreoretinal separation
and vitreous traction induce the formation of new breaks and the
reaccumulation of subretinal fluid.New breaks that are located in
the superior quadrants and are not widely separated (more than 1 or
2 clock hours apart) may be successfully treated with an additional
gas injection followed by cryotherapy and/or laser retinopexy.[4,
21]Likewise, the formation of a new break in the inferior quadrants
is usually an indication for scleral buckling and/or
vitrectomy.Cataract progressionCataract development and progression
is very uncommon after pneumatic retinopexy.Koch et al (1991) found
insignificant loss of lens transparency in eyes subjected to
pneumatic retinopexy compared with nonoperated eyes after 2 months
of follow-up.[25]However, by 6 months, the opacification of the
crystalline lens was more evident, particularly the anterior lens
cortex.[25]This complication can be minimized by careful placement
of the paracentesis needle over the iris and avoiding contact
between the intraocular gas and the lens.[4, 10]Subconjunctival
gasSubconjunctival gas results from either incomplete penetration
of the sclera by the needle for gas injection or outward leakage of
gas through the needle track of the gas injection. This has not
been considered to be clinically significant, and no corrective
action is required. To minimize this complication, the surgeon
should ensure proper insertion of the needle for gas injection into
the vitreous cavity and immediately place a cotton-tipped
applicator on the needle track after removal of the
needle.[4]Delayed subretinal fluid absorptionDelayed subretinal
fluid absorption is uncommon and is characterized by long-term
persistence of loculated pockets of low-lying subretinal fluid.
When involving the macula, these pockets of fluid cause prolonged
postoperative visual symptoms such as decreased visual acuity and
metamorphopsia. The presence of subretinal fluid can persist for
several months. No specific management is required, but close
follow-up is essential.[6, 10, 26]See the images below.Subretinal
fluid. This patient underwent pneumatic retinopexy and the retina
appeared to have flattened. However, the patient reported
metamorphopsia and a central scotoma. The optical coherence
tomograph shows residual submacular fluid. This submacular fluid
persisted for 9 months and then was reabsorbed.Cystoid macular
edema. A pseudophakic patient underwent pneumatic retinopexy. The
retina was attached, but the visual acuity remained low. An optical
coherence tomograph reveals cystoid macular edema. The patient was
treated with topical nepafenac for 2 months and the cystoid macular
edema resolved with a concomitant improvement in visual
acuity.Subretinal gasGas fish-egg bubbles may migrate through
retinal breaks into the subretinal space, particularly in the
presence of large breaks. Hilton and Tornambe (1991) found that any
eye retinal breaks larger than 1 clock hour are associated with an
increased risk for such bubbles.[10]In these cases, the patients
head should be positioned in such a way that the bubbles migrate
away from the tear. It usually takes 24 hours for the bubbles to
coalesce.Placing the patient in a supine position and tilting the
head so that the break is at the most superior position followed by
gentle scleral depression may release the subretinal gas into the
vitreous cavity. If this maneuver fails, vitrectomy is the most
direct and effective way of eliminating the trapped subretinal
gas.[4, 5, 10]EndophthalmitisThe incidence ofendophthalmitisas a
complication of pneumatic retinopexy is very low. Tornambe and
Hilton (1989)[12]reported one case of staphylococcal
endophthalmitis among the 103 eyes that underwent pneumatic
retinopexy.The most effective way to reduce this complication is to
be very meticulous with the sterile techniques. In particular, the
use of 5% povidone iodine solution prior to any intraocular
injection is highly recommended.[4, 10]Macular hole and other new
posterior breaksVitreomacular traction during the perioperative
period is thought to play a role in its pathogenesis. The expansion
of the intraocular gas produces a vitreomacular detachment, and, as
a secondary mechanism, the macula suffers a period of stress by the
shifting of a large amount of subretinal fluid under it due to the
expanding gas bubble.[27]Conventional surgical techniques for
repairing idiopathic macular holes such as vitrectomy can be used
with good results.[4, 28]Cystoid macular edemaCystoid macular
edemais very uncommon after pneumatic retinopexy. Eyes with a
history of uveitis, prior cataract extraction, and macular
detachment may have a greater tendency for postoperative cystoid
macular edema.[4, 29]Avoidance of excessive retinopexy during
pneumatic retinopexy may reduce this complication. Topical
steroidal and nonsteroidal anti-inflammatory medications are
usually effective for treating this complication.[4]Intraocular
hemorrhageIntraocular hemorrhage is rare. Injections should be
performed away from the anterior ciliary vessels along the vertical
and horizontal meridians in order to reduce the chance of ocular
surface and vitreous hemorrhage. During cryotherapy, the cryoprobe
should not be removed from the eye until appropriate thawing of the
ice ball on the cryoprobe and the surrounding surface of the globe
is evident to avoid fracturing of the frozen blood vessels.[4,
10]Epimacular fibrosis and macular puckerThe multicenter pneumatic
retinopexy study reported a 4% incidence of asymptomatic epimacular
membrane, as depicted in the image below, among the 103 eyes that
underwent pneumatic retinopexy.[12]Epimacular membrane. Following
pneumatic retinopexy, the patient developed an epiretinal membrane,
which is documented in the clinical picture and the optical
coherence tomograph.No known method prevents this complication, but
the avoidance of excessive cryotherapy and laser treatment may
minimize the risk. The management of macular pucker after pneumatic
retinopexy is similar to the treatment of this condition associated
with other clinical situations, usually with good outcomes.[4, 10,
12]Proliferative vitreoretinopathyThe rate of PVR varies depending
on the clinical series.Chen et al (1988)[22]reported a 9.8%
incidence in a prospective series of 51 eyes that underwent
pneumatic retinopexy. Tornambe (1997)[20]also noted a 9.6%
incidence of PVR with no difference in the incidence of PVR between
those eyes that underwent cryotherapy versus laser.The excessive
release of RPE cells into the vitreous cavity after pneumatic
retinopexy and the gas bubbles may play a role in the formation of
PVR. Eyes with PVR after pneumatic retinopexy can be managed with
vitrectomy and membrane stripping.[4, 30]Choroidal
detachmentChoroidal detachment is uncommon after pneumatic
retinopexy. Tornambe and Hilton (1989)[12]reported an incidence of
choroidal detachment of 3%. Prolonged and severe pain shortly after
suprachoroidal gas injection is a typical manifestation of a
choroidal detachment. Stretching of the ciliary nerves by the gas
may be cause of the pain. Avoiding hypotony during paracentesis and
also reducing excessive cryotherapy could reduce this
complication.[4, 10, 31]Intraocular pressure rise and glaucomaMild
to moderate intraocular pressure rise is well tolerated by the
average eye with no or minimal corrective measures after pneumatic
retinopexy and usually does not lead to any retinal or optic nerve
damage. Careful monitoring of the central retinal artery is
recommended. In the absence or central retinal arterial reperfusion
after 10 minutes, an immediately paracentesis is advised to lower
the intraocular pressure.[4]A 0.3% incidence of ischemic optic
neuropathy was reported by Tornambe (1997).[20]Musculoskeletal
complicationsBecause of the requirement of a consistent head tilt
for a prolonged period, pneumatic retinopexy may lead to various
musculoskeletal and neurological injuries, especially among elderly
patients. Cervical spine, neck muscles, and lower back problems and
ulnar nerve injury may occur. These are minor and are typically
temporary.A pillow, cushion, a table or desk with the correct
height may provide the required support. If necessary, analgesics,
a heating pad, or muscle relaxants may be prescribed to relieve
musculoskeletal discomfort associated with pneumatic retinopexy.[4,
10, 32]Corneal wound dehiscenceFull-thickness corneal wounds never
regain their original tensile strength.[33]Immediately following an
intravitreal gas injection, the intraocular pressure rises suddenly
up to 180 mm Hg,[34]which is enough to stress and rupture the
corneal scar. Wound dehiscence has been reported to occur during
pneumatic retinopexy in pseudophakic eyes that underwent clear
corneal incisions and in an eye with a penetrating
keratoplasty.[35, 36]In these cases, a slower injection of a
smaller volume of gas should be strongly considered.DAPUS :
Pneumatic Retinopexy, Apr 01, 2014, Lihteh Wu, Erick Hernandez
Bogantes, Mary L Windle, Hampton Roy
(http://emedicine.medscape.com/article/1844217-overview#showall)