Embed Size (px)
DESCRIPTION
PMTCT overview: current-scale up efforts and challenges in operations and implementation. Dr Angela Mushavi National PMTCT and Pediatric HIV Care and Treatment Coordinator: Zim IAS 2011, Rome: Italy 17/07/2011. Outline of Presentation. Background and epidemiology of HIV in Zimbabwe - PowerPoint PPT Presentation
Citation preview

PMTCT overview: current-scale up efforts and challenges in operations
and implementation
Dr Angela MushaviNational PMTCT and Pediatric HIV Care
and Treatment Coordinator: ZimIAS 2011, Rome: Italy
17/07/2011
Outline of PresentationBackground and epidemiology of HIV in
ZimbabwePMTCT Program performance in 2010Current scale-up efforts and challenges with
implementationAnd so wither Zimbabwe?

Background of ZimbabwePopulation: ~12 millionAdult HIV prevalence: 13.7% ANC sero-prevalence : 16.1%An estimated 1,1 mil
Zimbabweans are HIV positive*
Of these, 151, 749 are children 0-14 years*
New pediatric HIV infections are estimated at 14,976* (90% from MTCT)
1,090 patients dying weekly due to AIDS Source: DHS 2005/6 & MOHCW HIV estimates 2009*
Background of Zimbabwe94% of pregnant women received ANC (ZDHS 05/06)
68% of pregnant women delivered in Health Institutions (ZDHS 05/06) MNCH indices of Zimbabwe
398,889 expected pregnancies in 2010; of these, 47,494 are to HIV infected pregnant women
In the last 10 years, MMR has increased555/1000,000: ZDHS 2005/6 725/100,000: MOHCW 2007 Maternal and Perinatal Mortality StudyHIV/AIDS is leading contributor to high MMR (26%)
21% of the Under 5 Mortality Rate (<5MR) is attributed to HIV/AIDS (MIMS 2009)

National PMTCT ProgramPMTCT started as a 3 site pilot in 1999PMTCT program rolled-out in 2002Initially using only SD NVP for both the HIV infected
mothers and their HIV exposed infantsPiloted the use of more efficacious regimens (MER)
as per 2006 WHO Guidelines in 2007Roll-out of MER only started in 2009 Zimbabwe has officially adopted the 2010 WHO
guidelines (Option A) and roll-out is in progress

Current geographic coverage of PMTCT
Total # of health facilities: 1643 Total # of ANC providing PMTCT: 1560 (95%)
Comprehensive PMTCT 1200 (77%) (Both on site HIV testing & ARV prophylaxis) Minimum PMTCT sites 360(No on-site HIV testing but have ARV prophylaxis) 883 sites (57%) of all ANC sites in the 62 districts offer MER while
366 sites (23%) collect DBS for HIV DNA PCR (EID)
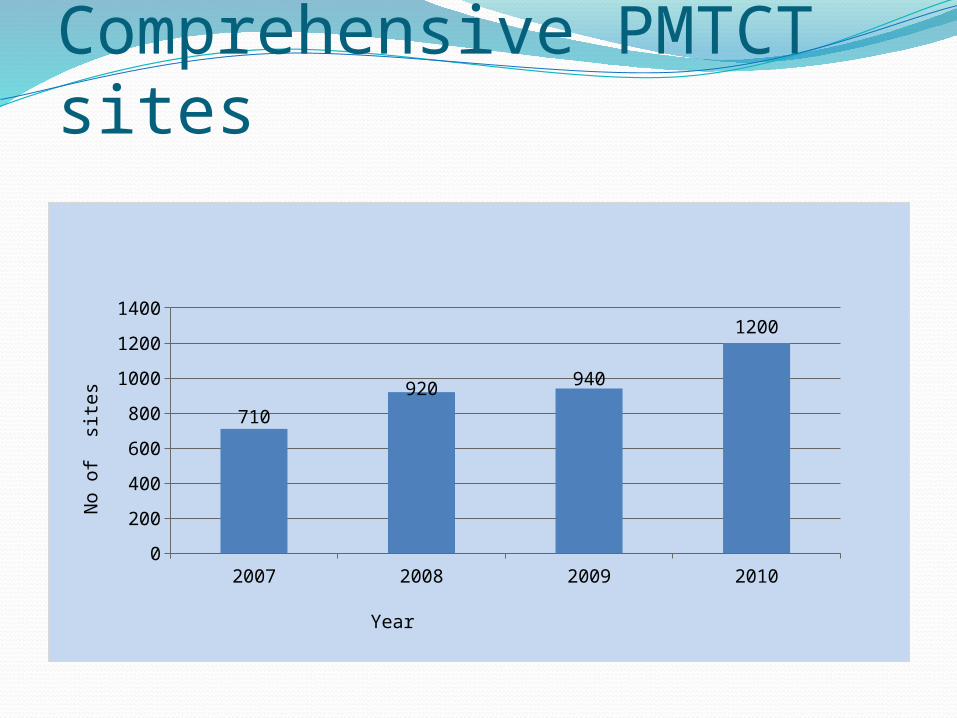
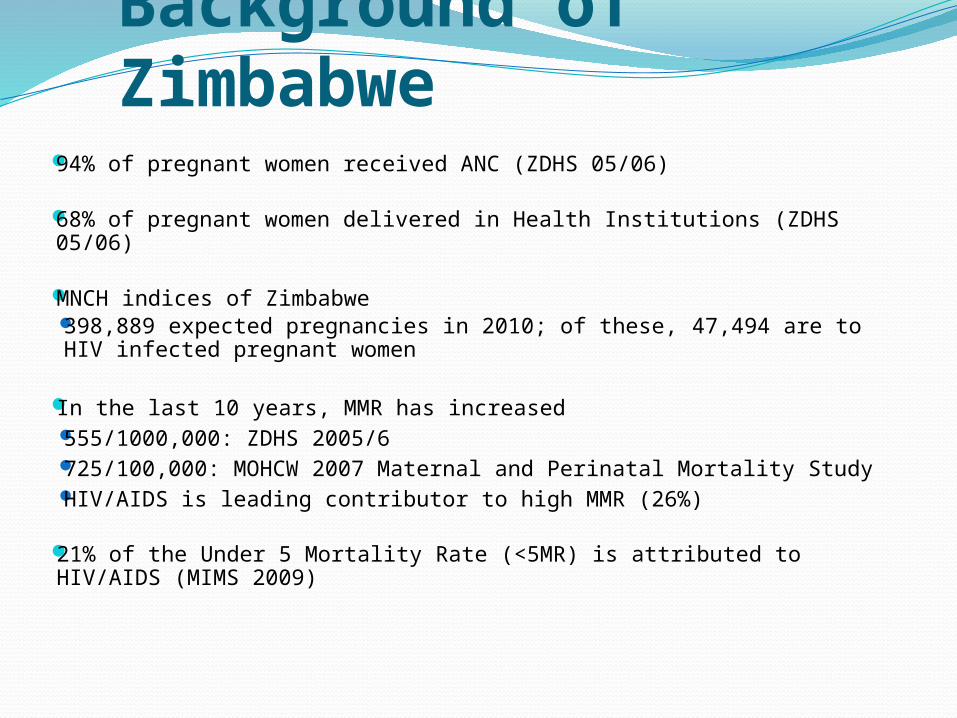
Comprehensive PMTCT sites
2007 2008 2009 20100
200
400
600
800
1000
1200
1400
710920 940
1200
Year
No
of s
ites

Estimated pregnancies versus actual seen in ANC
2009 20100
50000
100000
150000
200000
250000
300000
350000
400000
450000
500000
450 000
398 264
270 527
325 476
229 104
295 629
Expected Pregnancies Pregnant women booked for first ANC visitPregnant women HIV tested in ANC

Maternal and Infant ARV prophylaxis
2009 20100
10000
20000
30000
40000
50000
60000
50069 47494
29692 (59%)
39782 (84%)
23042 (46%)
35256 (74%)
ANC Women HIV positiveHIV positive pregnant women received ARV prophylaxisHIV exposed infants who received ARV prophylaxis
Year
Preg
nant
wom
en/I
nfan
t

Importance of partner support
Women HIV tested in ANC Women recived ARV in ANC Infants received ARV0%
20%
40%
60%
80%
100%
92% 94%
80%78%76%
50%
Comparison of Partner Supported and Non-Partner Supported Sites Zimbabwe MOHCW 2009 Data
EGPAF NO PARTNER

CTX prophylaxis to HEI
2007 2008 2009 20100
5000
10000
15000
20000
25000
30000
8225 (14%)
12626 (24%)
17171 (34%)
24996 (53%)
Exposed infants given cotrimoxazole
Exposed infants given cotrimoxazole

DNA PCR for Early Infant Diagnosis of HIV
YEAR Positive Negative TOTAL
2007 77 (31%) 245 322
2008 581 ( 38%) 1585 2 169
2009 901 (25%) 3597 4 498
2010 2373 ( 17%) 14159 16 532

PMTCT: Achievements
Strong PMTCT partnership forum (PPF) that supports scale-up
Transitioning to more efficacious regimens for PMTCT (moving to Option A)
Revised IMAI/IMPAC curriculum with on-going training and support supervision of staff
HIV DNA PCR for early infant diagnosis of HIV (EID) available since 2007
Support from government, donors and partners to provide resources for PMTCT scale-up; including GFATM and the National AIDS Trust Fund (AIDS levy)

Achievements of the PMTCT program
Elimination campaign officially launched in January of 2011
Strengthened efforts towards SRH/HIV integration targeting Prongs 1 and 2
Receiving increasing funding commitments from MOHCW through NAC, GFATM, EGPAF and other donors to scale-up towards elimination of new Pediatric HIV infections
Deploying Point of Care CD4 machines
Point of Care (POC) CD4 machines Evaluation of Point of Care CD4 machines: end 2009-2010
No significant difference between POC and laboratory based CD4 machines
Nurses able to operate as well as lab scientists
• MOHCW has given official go-ahead to procure and deploy these devices
• Roll out and evaluation of the machines under field conditions on-going
PMTCT: ChallengesSome progress yes; but much more needed to increase quality
and coverage towards universal access. In fact, much more needed to attain elimination of Pediatric HIV by 2015
Community mobilization and demand generation: some effort but how much is enough? Stigma and discrimination? Low male participation
Late booking, user fees and home deliveries: a missed opportunity for PMTCT
Lack of tracking of mother-infant pairs in PMTCT; and slow scale-up of EID and early treatment of HIV positive infants
M&E; including revision of tools and data quality and issues
PMTCT: ChallengesChallenge with human resources for health (HRH):
• High staff attrition rates; with constant need to train and retrain (IMAI/IMPAC)
• No official task sharing policies/strategies• Few health care workers trained in the revised 2010 WHO
guidelines for: Infant feeding in the context of HIVPMTCTAntiretroviral treatment

Challenges: PMTCTProcurement, supply chain management for PMTCT in the face
of an under-resourced health care system• Inadequate resources for ARVs, EID and other lab
support(e.g. HR, CD4 machines and consumables)• Shortages of other commodities: Cotrimoxazole, HIV Test
kits and essential equipment for the delivery of quality and comprehensive ANC and MCH services
• Minimal integration of PMTCT within the broader sexual and reproductive & maternal newborn and child health agenda: critical to helping us attain MDGs 4, 5 and 6 by 2015

And so do we give up? A most emphatic no!Understanding these challenges allows us to
design innovative and creative solutionsAnd with support from government,
multilateral and bilateral agencies including PEPFAR, GFATM, and others, we will truly reach the goal of elimination of new HIV infections in children by 2015