Embed Size (px)
Citation preview
PM6 Assignment
Preparation time Discussion time Demonstration time All based on cases in PM6
Multiple Sclerosis
Janet Rooney
2006
Definition
“A common idiopathic inflammatory demyelinating disease of the central nervous system (brain and spinal cord) characterised by discrete lesions (plaques) scattered throughout the CNS with symptoms resulting from impaired conduction through the demyelinated and transected axons”
(Giovannoni and Miller, 1999; Ko Ko, 1999; Schwid, 2003; Lazoff, 2005; Dangond, 2006; Multiple Sclerosis Society, 2006)
Prevalence
Most common cause of progressive neurological disability in the United Kingdom
Giovannoni and Miller, 1999
Lifetime risk = 1:400 Compston and Coles, 2002
350,000 cases in the United States, more than 2.5 million worldwide
Dangond, 2006
Prevalence
100-130/100,000 in the United Kingdom Craig et al, 2003; NICE, 2003
52-85,000 people in the United Kingdom NICE, 2003; Multiple Sclerosis Society, 2006
Incidence
25,000 persons newly diagnosed with MS in the United States, more than 1 million worldwide
Lazoff, 2005
3-7/100,000 diagnosed with MS each year in the United Kingdom
NICE, 2003
Early adulthood with a peak onset between the ages of 20 and 45
Ko Ko, 1999
Female to male ratio 2:1 Predominantly northern Europeans Familial recurrence rate of about 15%
Compston and Coles, 2002
Diagnosis
Expert panel McDonald et al, 2001
An ‘attack’ Exacerbation/relapse Episode of neurological disturbance Lasts at least 24 hours Not ‘pseudo-attack’
Diagnosis
Magnetic resonance imaging Cerebro-spinal fluid examination
Oligoclonal bands on electrophoresis Presence of an elevated IgG
Visual Evoked Potentials Slow but with well-preserved wave form
Clinical subtypes
Relapsing remitting 65-75% evolve into secondary progressive )
Dangond, 2006; Multiple Sclerosis Society, 2006
Chronic progressive Primary progressive Relapsing progressive Secondary progressive
Acute fulminant/Malignant Benign
Lazoff, 2005; Multiple Sclerosis Society, 2006
Symptoms
Primary Neurological
Secondary Consequence of immobility Consequence of impairment Consequence of Disability
Tertiary Consequence of Handicap
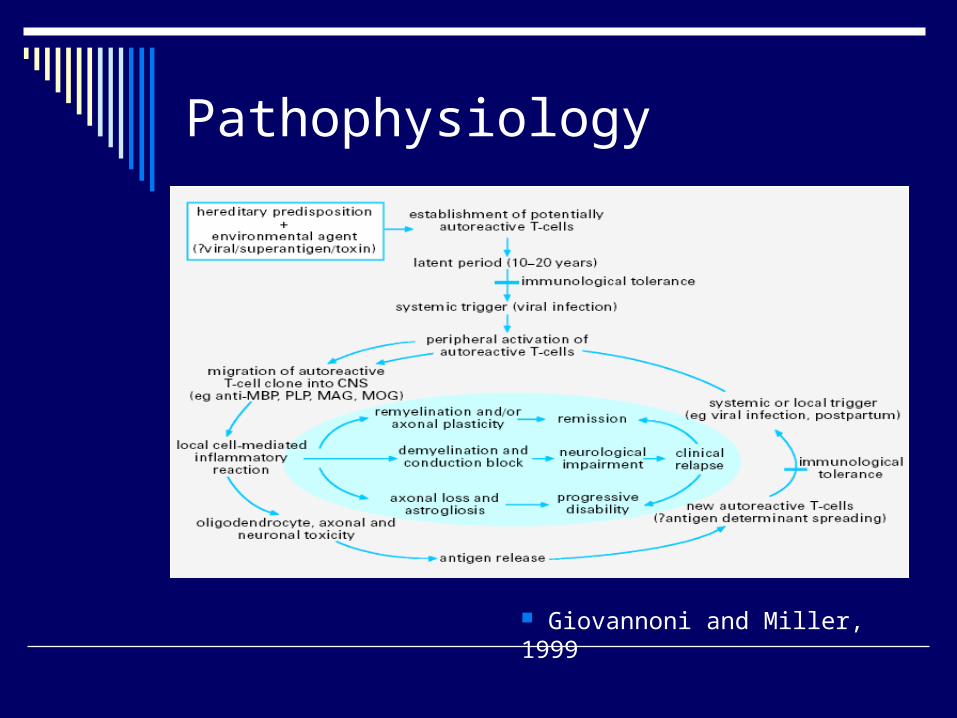
Pathophysiology
Giovannoni and Miller, 1999
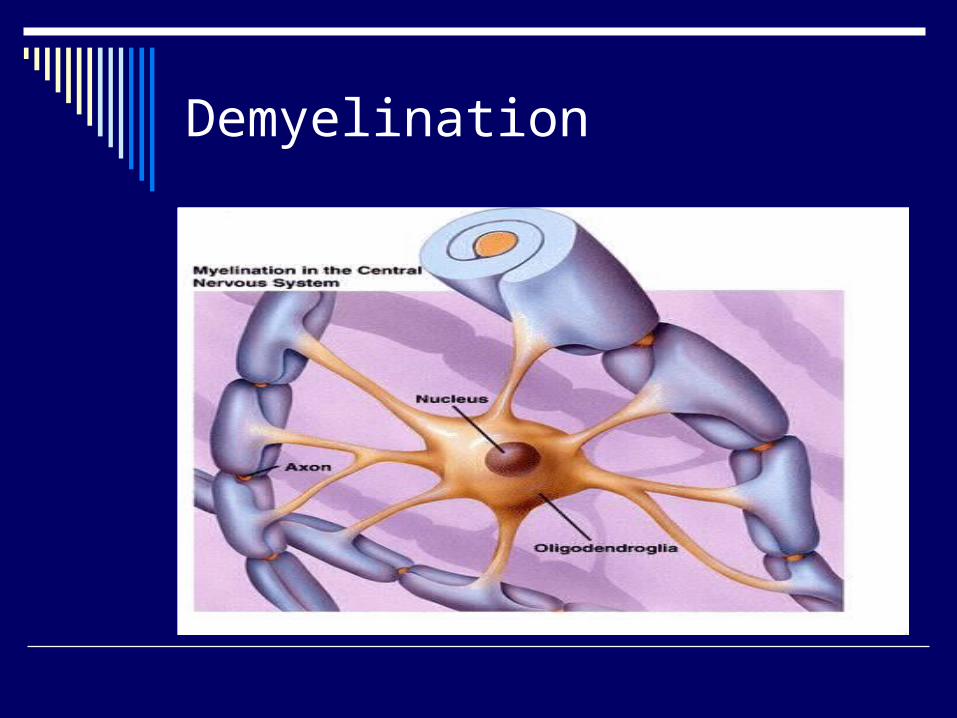
Demyelination
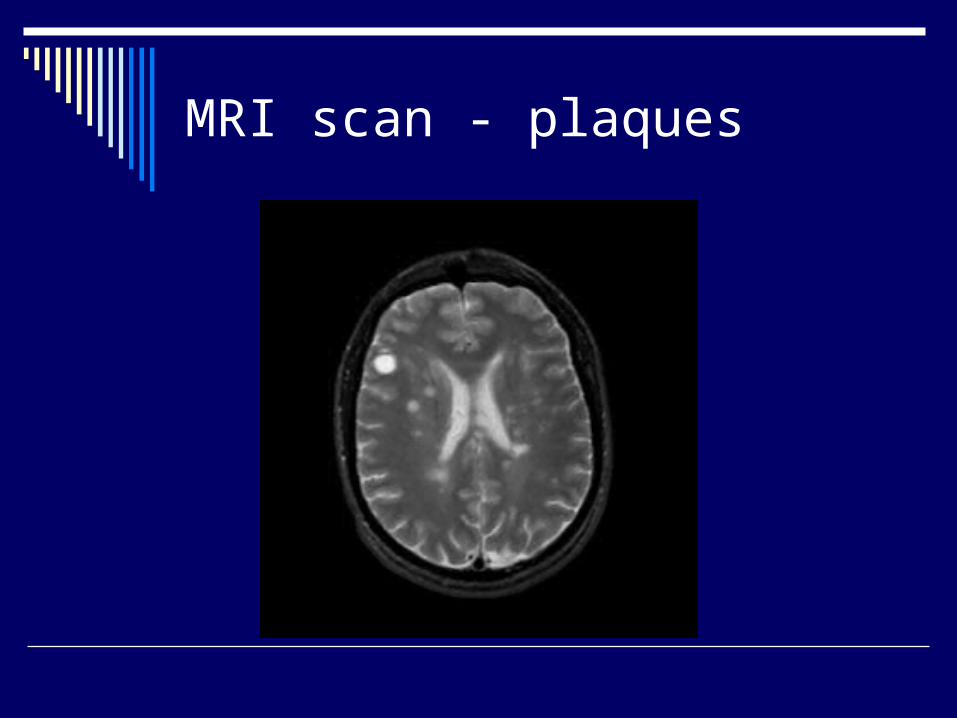
MRI scan - plaques
Impact
Career and aspirations, social and family life
Muscle weakness Spasticity Altered or reduced sensation Visual loss Dysarthria/dysphagia Respiratory dysfunction
Impact
Loss of coordination/ataxia Cognitive impairment Anxiety and depression Fatigue, Heat intolerance Pain/sensory disturbance Loss of bladder and bowel control
Ko Ko, 1999; Thompson, 2001
Fatigue
75%-95% of individuals with MS experience variable degrees of fatigue
50%- 60% report fatigue as one of their worst problems
Multiple Sclerosis Council for Clinical Guidelines, 1998; Dangond, 2006
Fatigue
Contractile force 30-70% lower than controls
Reduced muscle oxidative capacity Decreased ability to activate their
muscle/failure of muscle activation A portion of the weakness in MS can be
attributed to disuse Lambert et al, 2001, Surakka et al, 2004
Spasticity
Contributes to poor hygiene Pressure sores Difficulty in sexual activity Painful spasm Contractures of limbs Can be a good thing
Urinary tract dysfunction
Causes distress, disability and handicap Urgency, frequency and incontinence
combined with poor mobility Disturbance of sleep Tissue breakdown Pressure sores Spasticity
Ko Ko, 1999
EDSS
Kurtzke Expanded Disability Status Scale
Measure of disease progression Dangond, 2006
Severity scored on a scale of 1-10 Reliable, valid but not responsive
Sharrack et al , 1999
Heat sensitivity
Uthoff’s phenomenon Conduction block through partially
demyelinated nerves increases steadily as temperature increases
Cooling demyelinated nerves can reduce conduction block
Patients in Schwid et al study reported less fatigue during cooling
Schwid, 2003
Morbidity/Mortality
Life expectancy of someone with MS is reduced on average by 6 – 11 years
Multiple Sclerosis Society, 2006
Live 25 years from diagnosis Compston and Coles, 2002
Will manage without walking aids for 15 years from diagnosis
Autonomic Disturbance
Bladder dysfunction Bowel dysfunction Sexual dysfunction Cardiovascular autonomic dysfunction Thermoregulation Sweating Pupillary function
Merkelbach et al, 2006
Neuroplasticity
Evidence of potentially adaptive cortical plasticity that increases with brain injury in patients with multiple sclerosis
Reddy et al, 2002; Reddy et al, 2000
Training dependent changes in the brain can be demonstrated using MRI scanning technology
Limited task specific reductions in activation in the brain following training in patients vs. normals
Morgen et al, 2004
Interventions for MS
Evolves and changes as disease progresses Education Therapy input
Neurorehabilitation to minimize disability and handicap and to maintain the role of each individual in the family, workplace and community
Alleviation of symptoms Drug treatment
Treatments that modify the course of the disease by changing its natural history
Ko Ko, 1999; Thompson, 2001
Which intervention
Pills and potions Steroids Beta interferon Glatiramer acetate
Group exercise Freeman and Allison, 2004
Home exercise Surakka et al, 2004
Which intervention
Bobath concept Facilitation approach
Motor relearning approach (Carr & Shepherd) Task-oriented approach
Lord et al, 1998
Which intervention
Yoga Oken et al, 2004
‘Rehabilitation’ Craig et al, 2003
Supportive technologies Cattaneo et al, 2002
Effectiveness
Depends what you mean 65% of patients made functional gains Only 18% improved neurologically Reduction in distress
Ko Ko 1999
The more the merrier Slade et al 2002
Guidelines
National Institute for Clinical Excellence (2003) Multiple Sclerosis: national clinical guideline for diagnosis and management in primary and secondary care [online] available from http://www.rcplondon.ac.uk/pubs/books/MS/MSfulldocument.pdf [accessed 16/10/2006]
Guidelines
National Institute for Clinical Excellence (2002), Multiple sclerosis – beta interferon and glatiramer acetate for the treatment of multiple sclerosis, NICE Technology Appraisal Guidance No. 51. London, National Institute for Clinical Excellence [online] available from the World Wide Web at http://www.nice.org.uk
Guidance
Multiple Sclerosis Society (2006), A guide to MS for GPs and primary care teams, London, Multiple Sclerosis Society [online] available from the World Wide Web at http://www.mssociety.org.uk/document.rm?id=1077 [accessed 16/10/2006]





























