Embed Size (px)
Citation preview

Thorax (1969), 24, 91.
Pleuro-pulmonary amoebiasisB. T. LE ROUX
From the Thoracic Surgical Unit, Wentworth Hospital, University of Natal
Experience with amoebic infestation of the pleural space and the lung in an area whereamoebiasis is endemic is described. The manifestations of pleuro-pulmonary amoebiasis are out-lined, and, for completeness, a note is added on pericardial amoebiasis and the technique ofpericardiocentesis.
From a retrospective scrutiny of 500 consecutivecase records, which related to patients withempyema thoracis, over a 13-year period in arelatively closed community of one and a halfmillion in the south-east region of Scotland (leRoux, 1965), it emerged that, in 50% of patients,empyema was related to non-specific pulmonaryinfection for which a persisting cause was notfound, and that this was the commonest singlecause for empyema in this region. Trauma was arare cause, and amoebic empyema was notencountered. On completion of this survey theopportunity arose to establish a thoracic surgicalunit which would serve the Province of Natal inSouth Africa. The population of this Provinceis some three million, of whom two millionare Africans, half a million are Asiatics,and half a million are of Caucasian stock.Empyema thoracis in the first 200 examples of thisdisease (80% of which were in relatively youngmen) seen in this new community was a late andprobably iatrogenic complication of traumatichaemothorax in 50%, and in nearly all thesepatients the trauma was a stab wound. In theremainder the commonest cause of empyema wasamoebiasis and in most of these patients thepleural infection was an extension from the liver.The purpose of this paper is to relate the naturalhistory of amoebiasis which has extended into thepleural space or the lung.
Extension of amoebiasis from the liver to thelungs and pleura is well documented, and theproblems which relate to amoebiasis in clinicalpractice have been described by Wilmot (1962).Pleuro-pulmonary amoebiasis may, develop as aconsequence of:
(1) Direct extension (either abruptly by ruptureof a liver abscess, or insidiously) from the liverthrough the diaphragm either (a) to involve thepleura, here promoting the symptoms and signs
91
of pleurisy, or with the development of a serouseffusion or an empyema; or (b) into the lungwith the development of pulmonary consolidation,lung abscess or broncho-hepatic fistula.
(2) Haematogenous dissemination to the lungsfrom the bowel or liver, with either single or mul-tiple pulmonary abscesses, or localized or diffuseareas of pulmonary consolidation.With regard to direct extension from the liver
into the pleural space or lung, it is common tohear a pleural rub in a patient with an amoebicliver abscess. Such a rub may disappear withspecific anti-amoebic treatment, or may be a pre-lude to the development of a serous pleuraleffusion or an amoebic empyema, the consequenceof rupture of an amoebic abscess of the liver orsub-phrenic space into the pleural space. Rub andserous effusion are not inevitable precursors tothe development of an empyema. Amoebic empy-ema thoracis may also result from direct extensionof an amoebic lung abscess to the pleura. Thedevelopment of amoebic empyema may be abruptor insidious; an insidious onset is more usual, butsometimes the onset is acute, with severe painand shock, followed quickly by death. The rightpleural cavity is more often involved (Figs 1 and2) but occasionally a left-sided amoebic empyemais found (Figs 3, 4, 5, and 6).There are well-documented cases of left amoebic
empyema which has developed as a complicationof amoebic pericarditis, itself the manifestation ofdirect extension of hepatic amoebiasis through thediaphragm into the pericardium. Pus obtained atthoracentesis in a patient with an amoebicempyema is usually 'anchovy' in colour but maybe yellow or green; it must be examined bothfor pathogenic bacteria and, by appropriate tech-niques, for amoebae. Drug therapy for amoebiasis,in conjunction with intermittent closed drainage,is more often successful in amoebic empyema
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

B. T. le Roux
FIG.1
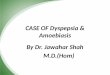
FIGS 1 and 2. Postero-anterior and lateral views show a large right empyema inwhich there is a level. Pus shown to contain Entamoeba histolytica was aspiratedfrom the right pleura. Management was by continuous closed drainage and anti-amoebic drugs. Convalescence was uneventful and the empyema rapidly diminishedin size. Other surgical action was not required. When the empyema was greatlvreduced in size, bile discharged into the water-seal for a few days. The biliaryfistiula had closed before the intercostal tube was removed.
thoracis than in other forms of empyema; con-tinuous closed drainage may be necessary, andoccasionally open drainage, sometimes with drain-
......._age also of the sub-phrenic lesion._ 2 _ Of 200 patients with empyema thoracis managed
over a period of two years, 37 were established asamoebic. All the patients were of African orAsiatic stock; they represent only a small propor-tion of the total number of patients with amoebicempyema seen in the Province, and include thosein whom standard medical management (by appro-priate drugs and intermittent closed drainage byaspiration) had failed, or in whom the diagnosisof amoebiasis had not been entertained. Of the37 patients, management by continuous closeddrainage in conjunction with the exhibition ofemetine and chloroquine in 30 resulted in rapidclinical improvement and only slightly less rapidrestoration of the radiographic appearances tonearly normal. Of the remaining seven patients,two were admitted moribund and died despiteclosed drainage and the exhibition of appropriatedrugs. In two patients the amoebic empyema wasFIG. 2
92
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

Pleuro-pulmonary amoebiasis
FIG. 3
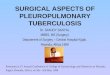
FIGs 3 and 4. The left pleural lesion shown in the postero-anterior and lateral filmswas ultimately established as an amoebic empyema and management was byclosed drainage with appropriate drug therapy.
secondarily infected with E. ccli and managementwas first by closed and then by op.-n drainage. Inthree patients secondary infection was with avariety of organisms, probably of iatrogenicorigin, and management by closed drainage wasfollowed by decortication. In one of these patientsthe amoebic empyema was left-sided and at decor-tication the empyema space was seen to com-municate directly with the pericardial space, its-lfthe site of amoebic infection, and there was, com-munication between the pericardial space and theleft lobe- of the liver. Thirty-two of the 37 amoebicempyemata were right-sided, four were left-sided,and one was bilateral. In three of the four left-sided empyemata, amoe-bic pericarditis was aclinically recognized feature of the disease or wasdemonstrated at thoracotomy. In the patient withbilateral amoebic empyemata and in five of thepatients with right-sided amoebic empyema therewas unequivocal evidence (by pericardiocentesis) ofamoe-bic pericarditis. In five patients it was neces-sary to manage hepatic amoebiasis by aspiration;FIG. 4
93
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

B. T. le Roux
FIG. 5. Left amoebic empyema with amoebic pericarditis. Management was byclosed drainage of the left pleural space and aspiration of the pericardium.
FIG. 6. This patient was knownto have had amoebiasis and theleft empyema was established asamoebic. The pleural shadowpersisted despite closed drain-age, and ultimately Escherichiacoli was grown from the pus.Decortication was undertaken, atwhich it was established thatthere was a communicationbetween the pericardial sac andthe left pleura, that there was anextensive amoebic pericarditis,and that the pericardium com-municated directly with the leftlobe of the liver, in which therewas an incompletely closedamoebic abscess cavity.
94
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

Pleuro-pulmonary amoebiasis
FIG. 7 U
For legends to Figs 7 to 1O see p. 96 (overleaf).
in none was it necessary to manage an hepaticcollection of amoebic pus by open drainage, andin only one was a subphrenic collection of pusdrained surgically (Figs 7, 8, 9, and 10).
Trans-diaphragmatic migration of amoebaefrom th_ liver to the lung in lymphatic channels,without macroscopic evidence of rupture throughthe diaphragm, probably occurs. Pulmonarylesions and cavitation are most common in eitherthe middle (Figs 11 and 12) or the right lowerlobe (Figs 13, 14, 15, and 16), sometimes withabscess formation (Figs 17 and 18). The left lowerlobe or the lingular segment of the left upper lobemay be the site of amoebic lung abscess; pul-monary involvement is occasionally bilateral. Theusual manner of extension is by perforation of asubphrenic or hepatic abscess through the dia-phragm, across an obliterated pleural space, withpulmonary consolidation or abscess; or, morecommonly, direct ext_nsion to a bronchus withlittle involvement of the pulmonary parenchymaand evacuation of the subdiaphragmatic lesion byFIG. 8
95
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

FIG.99
FIGS 7, 8, 9, and 10. Radiographs of the same patient made at intervals of one week. Presentation was withcough and purulent sputum. The right lower opacity in Figs 7 and 8 contains a level. The gel diffusion test waspositive. The patient was presumed to have an amoebic lung abscess. In Figs 9 and 10 the level has disappeared.Response to anti-amoebic drugs was unimpressive clinically and radiographically, and the possibility of anothercause for the 'pulmonary' lesion was considered an indication for exploratory thoracotomy. The lesion was shownto be a subphrenic abscess in which there were amoebae.
coughing. There is, in these circumstances, anhepato-bronchial fistula. Repeated small haem-optyses may precede the expectoration of charac-teristic dark, reddish-brown sputum in which E.histolytica may be found. Radiographically, thereis usually some evidence of a pulmonary lesion,and the diaphragm is elevated; a triangularshadow with its base on the diaphragm is said, incircumstances of known hepatic amoebiasis, to becharacteristic. The prognosis is good. With appro-priate treatment recovery is rapid in the patientwith an hepato-bronchial fistula, but more pro-tracted if there is a related pulmonary abscess.Complications such as empyema, metastaticabscess, and residual pulmonary fibrosis mayoccur. Surgical drainage is required only when thepatient, to whom adequate medical treatment hasbeen exhibited, deteriorates or fails to progress,and the decision to embark on a surgical proce-
FIG. 10 dure must not be made prematiArely. Emetine,
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

Pleuro-pulmonary amoebiasis
FIG. IluI
FIGS 11 and 12. There is a middle lobar opacity and a right pleural effusion.This patient was known to have hepatic amoebiasis. The pulmonary and pleurallesions cleared with appropriate drug therapy. E. histolytica was found inthe sputum.
chloroquine, and postural drainage will cure mostamoebic lung abscesses; secondary bacterial con-tamination of the lung abscess may require appro-priate chemotherapy. Resolution is the rule;occasionally, irreversibly damaged lung, withbronchiectasis or a chronic cavity, may requireresection. Since an amoebic liver abscess isoccasionally in communication with the biliarysystem, it sometimes happens that rupture of anabscess into the bronchus is followed by abroncho-biliary fistula which is recognized by theexpectoration of bile-stained sputum; recoverywith conservative management is again the rul_.
In the community in the south-east region ofScotland, a persistent peripheral pulmonaryopacity in the right lower lobe was so likely tobe a carcinoma that, after an appropriate periodof chemotherapy and after there had becomeavailable a sufficiently large series of radiographsto establish that the lesion was not clearing, man-agement was usually by pulmonary resection. InFIG. 12
97
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

FIG.13
For legends to Figs 13 to 16 see opposite page
Natal, among Indian and African patients, a per-sistent pulmonary opacity in the right lower lobeis so commonly amo_bic that it is the rule tomanage patients with such an opacity by theexhibition of appropriate anti-amoebic drugtherapy and confidently to expect that the lesionwill clear. After initial error in two patients, inwhom a persisting right pulmonary opacity wasmanaged by right lower lobectomy, this error hasnot again been made-to operate on a patient withan amoebic pulmonary lesion, whether cavitatedor not. In 29 patients in whom it was judged thata pulmonary lesion was amoebic, this diagnosiswas established in only five who coughed up largevolumes of amoebic pus, and in the remainderthe diagnosis was accepted on the basis of apositive gel diffusion test (Maddison, 1965); inall, the lesion cleared radiographically with appro-priate drug therapy.
In the management of a patient in an area inwhich amoebiasis is endemic, and in any patientexposed by travel to the possibility of infestationby E. histolytica, it is important to keep in mindthe possibility of pulmonary or pleural amoebiasiswhen faced with the need to treat a right lowerpulmonary or pleural lesion which resists standard
FIG. 14 management for an acute infection.
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

FIG. 15 m
FIGS 13, 14, 15, and 16. These radiographs are typical of the pulmonary and pleural changes which accompanyhepatic amoebiasis which has extended through the diaphragm into pleura and lung. The appearances are non-specific and the diagnosis of pleural and pulmonary amoebiasis is most likely to be achieved when the indexof clinical suspicion is high, where it is known that amoebiasis is endemic or that there may have been exposureto infection elsewhere.
There is both clinical and necropsy evidence ofthe occurrence of pulmonary amoebiasis in theabsence of hepatic amoebiasis.A lesion may develop in an area of the lung
:| remote from the diaphragm, and this may reflecthaematogenous spread, or transbronchial spreadby aspiration or 'bronchial embolism', where thereis a broncho-hepatic fistula. Many reports of pul-monary lesions attributed to amoebiasis are basedon the association of a bowel infestation with
-,1k * a E. histolytica, the disappearance of radiologicalopacities following the exhibition of emetineor chloroquine together with other therapy,or the demonstration of degenerate amoebae
......in the sputum. The validity of such accountsj must be accepted with caution. Bowel infesta-
tion with E. histolytica is common in endemicareas and may co-exist with many otherdiseases; when infestation with E. histolyticaco-exists with areas of pulmonary consolida-tion, the aetiology of which is never estab-lished, the apparent therapeutic effect of emetine
FIG. 16 may be no more than coincidental; and particular
-:s.
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

M FIG. 17
FIGS 17 and 18. A right lower amoebic pulmonary abscess from which (over a 24-hour period) three pints ofamoebic pus was evacuated by coughing. The interval between the films is four days. The appearance of the puswas typical and it was shown to contain E. histolytica.
FIG. 18
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from

Pleuro-pulmonary amoebiasis
care is needed in the identification of amoebae inthe sputum, since, unless morphological charac-teristics are unequivocal or the organism containsred blood cells, the parasite may easily be con-fused with Entamoeba gingivalis, a common oralcommensal.
Single pulmonary lesions which may be haema-togenous are more commonly described than aremultiple lesions, and multiple lesions attributableto pulmonary amoebiasis are probably very un-common.Both bronchitis and asthma have been
attributed to infestation with E. histolytica. It isassumed that the parasite reaches the bronchi fromthe gut by way of the bloodstream or, alterna-tively, its presence in the body constitutes anallergen. Evidence for such an association isunconvincing.
It is convenient to include here a brief discus-sion on amoebic pericarditis. In the majority ofpatients this complication is associated with anabscess in the left lobe of the liver (Macleod,Wilmot, and Powell, 1966). Right hepatic lobelesions less often extend to the pericardium. Leftempyema may complicate amoebic pericarditisrather than exist as a direct extension from theliver.Amoebic pericarditis presents in two clinical
forms: (1) as a pericardial rub with electrocardio-graphic and radiographic evidence of pericarditisassociated with an amoebic liver abscess; or (2)as purulent pericarditis from perforation of anamoebic liver abscess into the pericardium.
In the first, prompt and successful treatment ofthe liver abscess is followed by resolution of thepericardial lesion. The second syndrome may havesuch an abrupt onset as to simulate one of thecardiac or pulmonary emergencies, and circu-latory disturbances may quickly be followed bydeath. A less dramatic onset is more common.The diagnosis is confirmed by aspiration of pusfrom the pericardium; hepatic signs and theabsence of bacteria fmom the pus should arousesuspicion that purulent pericarditis is in factamoebic, particularly in an endemic area. Therelief of cardiac tamponade is a matter ofurgency; repeated aspiration may be necessaryand open drainage is occasionally required;
specific drug therapy is essential; recovery with-out the development of constriction is usual.Where constriction has developed, secondarybacterial infection has sometimes been demon-strated and this may be the additional factor thatdetermines the development of constriction. Butconstriction may develop in the absence of recog-nized secondary infection, and may resolve with-out recourse to pericardiectomy (Lamont andPooler, 1958).
Pericardial aspiration is most safely undertakenthrough Larrey's angle or cleft (the angle betweenthe ziphisternum and the left costal margin) onthe left. The needle is introduced in a rostral andmedial direction. Pericardial aspiration is morehazardous than aspiration of other serous cavitiesbecause of the danger of transgressing myocardiumor puncturing a coronary vessel, with resultanthaemopericardium or the induction of ventricularfibrillation. If the indifferent praecordial lead on theelectrocardiograph is attached to a specially con-structed electrode which connects the aspiratingneedle to the electrocardiograph machine and theelectrocardiogram is monitored throughout theaspiration of the pericardial space, contact betweenthe tip of the aspirating needle and epicardiumwill be seen to produce a characteristic cardio-graphic pattern, with ventricular prematuresystoles or an acute 'current of injury'. Althoughthis technique does not make it impossible todamage a coronary vessel or the myocardium, itmakes this very much less likely provided thatreasonable care is taken. The use of a pericardialneedle as an exploring electrocardiograph elec-trode to recognize signs of myocardial injuryduring pericardiocentesis has been fully recordedand has had a place in clinical practice establishedfor some 10 years (Gotsman and Schrire, 1966).
REFERENCES
Gotsman, M. S., and Schrire, V. (1966). A pericardiocentesis electrodeneedle. Brit. Heart J., 28, 566.
Lamont, N. McE., and Pooler, N. R. (1958). Hepatic amoebiasis. Astudy of 250 cases. Quart. J. Med., 27, 389.
le Roux, B. T. (1965). Empyema thoracis. Brit. J. Surg., 52, 89.Macleod, I. N., Wilmot, A. J., and Powell, S. J. (1966). Amoebic
pericarditis. Quart. J. Med., 35, 293.Maddison, S. E. (1965). Characterization of Entamoeba histolytica
antigen-antibody reaction by gel diffusion. Exp. Parasit., 16, 224.Wilmot, A. J. (1962). Clinical Amoebiasis. Blackwell, Oxford.
101
on March 24, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.24.1.91 on 1 January 1969. D
ownloaded from




![1 CISER: An Amoebiasis inspired Model for Epidemic …amoebiasis is an infectious disease, some of the researchers [1] have modeled the transmission behavior of amoebiasis in human](https://img.pdfslide.us/doc/110x75/5e7b2a51e20b0d680d472d29/1-ciser-an-amoebiasis-inspired-model-for-epidemic-amoebiasis-is-an-infectious-disease.jpg)
![Right congenital pleuro-peritoneal hiatus hernia · Right congenital pleuro-peritoneal hiatus hernia 155 References [1] Adzick NS, Harrison MR, Glick PL, Nakayama DK, Manning FA,](https://img.pdfslide.us/doc/110x75/5b8bb26309d3f231638bd035/right-congenital-pleuro-peritoneal-hiatus-hernia-right-congenital-pleuro-peritoneal.jpg)