Embed Size (px)
Citation preview
![Page 1: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/1.jpg)
1General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Pleural Tuberculosis and Application of Video-Assisted Thoracoscopic Surgery in the
Diagnosis and Therapy
ABSTRACTMycobacterium tuberculosis (TB) is one of the main etiologies of lymphocytic pleurisy.
Tuberculous pleural effusion (TPE) occurs in approximately 5% of patients with a pulmonary TB infection. The definitive diagnosis of TPE depends on the demonstration of acid-fast bacilli in the pleural fluid or pleural biopsy specimens. The diagnosis can be established in a majority of patients from the clinical features, pleural fluid examination, including biochemistry, bacteriology, mycobacteriology, cytology and pleural biopsy. Nevertheless, diagnosis of TPE is difficult because of its nonspecific clinical presentation and insufficiency of traditional diagnostic methods. Polymerase chain reaction (i.e., GeneXpert assay) has relatively low sensitivity but high specificity in identifying the presence of TB bacilli and remains suboptimal in the diagnosis of TPE. Thoracoscopic pleural tissue histopathology with GeneXpert assay provides the highest diagnostic yields. A number of pleural fluid biomarkers such as adenosine deaminase (ADA), interferon-gamma (IFN-γ), regulatory cytokines, such as interleukin-27 (IL-27, a member of the IL-12 cytokine family), and chemokine receptor CXCR3 ligands such as the chemokines of IFN-γ-
Yee-Huang Ku1, Yin-Ching Chuang2 and Wen-Liang Yu3,4*1Division of Infectious Disease, Department of Internal Medicine, Chi Mei Medical Center-Liouying, Tainan City, Taiwan2Department of Medical Research, Chi Mei Medical Center, Tainan City, Taiwan3Department of Intensive Care Medicine, Chi Mei Medical Center, Tainan City, Taiwan4Department of Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei City, Taiwan
*Corresponding author: Wen-Liang Yu, Department of Intensive Care Medicine, Chi Mei Medical Center, N0. 901 Chuang Hwa Road, Yung Kang District, 710 Tainan City, Taiwan, Tel: 886-6-281-2811, ext. 52605; Fax: 886-6-251-7849, Email: [email protected]
Published Date: July 25, 2018
Gr upSM
![Page 2: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/2.jpg)
2General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
induced protein-10 KDa (IP-10/CXCL10) and monokine induced by interferon-γ (MIG/CXCL9) have shown promise for the rapid diagnosis of TPE. However, only combination of ADA with other biomarkers would be considered a mainstay investigative tool for clinical decisions, particularly in areas with medium to high TB prevalence. Of several pleural fluid parameters studied, ADA and IFN-γ have the best diagnostic yield. The role of surgery is confined to the treatment of the sequelae of pleural TB with dense adherences and loculations. Video-assisted thoracoscopic surgery (VATS) for decortication could achieve full lung reexpansion with minimal invasiveness. VATS is also effective and safe for lobectomy to resect concurrent lung abscess or cavity in advanced pulmonary TB infections.
INTRODUCTIONActive pulmonary Mycobacterium tuberculosis (TB) infections present a broad spectrum of
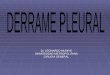
clinical manifestations, resulting in the diagnostic difficulty. Between 3% and 25% (approximately 5%) of patients with pulmonary TB infections will have pleural involvement [1,2]. Pleural TB is the leading etiology of extra pulmonary TB. Tuberculous pleural effusion (TPE) is the most common form of pleural effusion in many developing countries. Pleural TB is mainly a medical disease. Symptoms may include prolonged dry cough, easy fatigability, breathlessness, painful breathing, pleuritic chest pain, discomfort while lying down, low grade night fever, loss of appetite and unintentional weight loss [1]. Patients may lack a history of pulmonary TB or deny any exposure to a patient with pulmonary TB. Respiratory examination reveals reduced breath sounds with decreased vibration over the lesion lobe and stony dullness on percussion. Ultra sonography shows an abnormal accumulation of fluid in the pleural space. The chest computed tomography (CT) findings of pleural TB include circumferential pleural thickening (33%), mediastinal pleural involvement (32%), nodular thickening (9%), and pleural thickening >1cm (2%), for example, as demonstration in one of our cases (Figure 1). However, nodular pleural thickening particularly with nodules >1cm is significantly associated with malignant pleural dissemination [3].
Figure 1: The computed tomography of the chest is showing right-sided pleural effusion with pleural thickness and diffusely thickening pericardium in a patient with pulmonary tuberculosis,
supporting the diagnosis of tuberculous pleura pericarditis.
![Page 3: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/3.jpg)
3General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Thoracocentesis or ultrasound-guided pleural aspiration could confirm an exudative pleural effusion and thus the symptoms of dyspnea and cough might be relieved. Gram stain usually reveals no organisms. Culture confirms no bacterial growth after 48-hour incubation. The cause of TPE is a delayed hypersensitivity response to mycobacterial antigens in the pleural space. However, stains of pleural fluid are only rarely positive for acid-fast bacilli. Histology of pleural biopsy may identify multiple scattered necrotizing granulomatous inflammations with very occasional acid-fast bacilli using Ziehl-Neelsen or Kinyoun stains. In a study of 104 cases with confirmed pleural TB in Brazil, acid-fast staining in pleural fluid was negative in all cases. Pleural fluid cultures were positive in less than 10%. Cultures for the pleural biopsy specimens and granuloma were positive in 58% and 95%, respectively. The best accuracy of predictor was the activity of adenosine deaminase (ADA) in pleural fluid [4].
Light’s Criteria:
Mainly according to Light’s criteria, a pleural effusion is likely exudative if at least one of the following exists:
1. The ratio of pleural fluid protein to serum protein is greater than 0.5 [5]
2. A pleural fluid lactic dehydrogenase (LDH) greater than 200IU/L [5]
3. The ratio of pleural fluid LDH and serum LDH is greater than 0.6 [5]
4. Pleural fluid LDH is greater than 0.6 or two-thirds times the upper limit of normal for serum LDH [5, 6].
Differentiating exudates from transudates by the classical Light’s criteria helps knowing the pathogenic mechanism resulting in pleural effusion, and it is also useful for differential diagnosis purposes. A diagnosis of exudate was less likely when all Light’s criteria were absent. The presence of an increased inflammatory marker, such as C-reactive protein, together with the presence of over 50% of neutrophils is highly suggestive of parapneumonic pleural effusion. If, in these cases, the pH is <7.20, then the likelihood of complicated pleural effusion is high. Most TPEs are exudates with high ADA, a predominance of lymphocytes, straw-colored and free flowing, with a low yield on mycobacterial culture. The easiest way to diagnose TPE in a patient with lymphocytic pleural effusion is to demonstrate a pleural fluid ADA level above 40 U/L [1,7]. An ADA>40 (or 45) U/L, >50% lymphocytes and few mesothelial cells is suggestive of pleural TB. In hospitals where ADA is not available, pleural biopsies to evaluate for caseating granulomas are a standard diagnostic approach [8], for example, as demonstrated in two of our cases (Figures 2 and 3).
![Page 4: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/4.jpg)
4General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
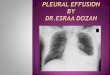
Figure 2: Pleural fluid serial analysis reveals lymphocytic predominance, few mesothelial cells and exudate nature, which was primarily based on relatively high protein content (3.5g/dL).
The LDH level was not greater than 0.6 or 2⁄3 times the normal upper limit for serum. Pleural effusion acid-fast stain and mycobacterial culture were negative for tuberculous bacilli. All
the results of acid-fast stain, GeneXpert and mycobacterial culture for sputum samples were positive. The pleural tissue biopsy reported granulomatous inflammation, supporting the
diagnosis of pulmonary and pleural tuberculosis.
Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin levels in pleural effusions were low in transudative pleural effusions (0.188 ± 0.077ng/mL) and TB pleurisy (0.130 ± 0.069ng/mL), but high in empyema (5.147 ± 3.056ng/mL), and para-pneumonic effusion (1.091 ± 0.355ng/mL) [9]. Thus, the procalcitonin level is not a useful parameter for the diagnosis of TB pleurisy [10].
![Page 5: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/5.jpg)
5General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 3: Chest x-ray film is showing right-sided pleural effusion with a meniscus sign and blunting of the right costophrenic angle. Pleural fluid analysis revealed lymphocytic predominance, few mesothelial cells and exudate nature which was primarily based on high LDH level (469 IU/L) and a ratio of pleural fluid protein to serum protein greater than 0.5 (3.4/5.8= 0.58).Sputum and pleural effusion acid-fast stain were negative for tuberculous bacilli. Nonetheless, both the sputum and pleural fluid mycobacterial cultures yielded Mycobacterium tuberculosis complex, confirming the diagnosis of pulmonary and pleural tuberculosis.
Tuberculous Empyema
Thoracic empyema is a disease with significant morbidity and mortality, especially in the developing world where tuberculosis remains a common cause. Of a prospective study in India, tuberculous empyema was responsible for near 40% ofthoracic empyema [11]. TB pleurisy can present as loculated pleural effusions with neutrophil predominance which mimic parapneumonic effusions. Then, they can progress to frank TB empyema, containing an abundance of mycobacteria. Up to 80% of patients have concurrent parenchymal involvement on the chest imaging [7].
Compared the nontuberculous empyema patients (mostly due to Staphylococcus aureus and Gram-negative bacilli), tuberculous empyema was more frequent association with younger population, longer duration of illness and mean duration of chest tube drainage, more presence of parenchymal lesions as well as more often requiring surgical drainage procedures for bronchopleural fistula [11]. Compared to those with patients with free-flowing effusion, patients with organized effusion (fibrous thickening of the pleura) or tuberculous empyema were older, higher incidence of TB reactivation with concurrent pulmonary TB, and higher positive rates of pleural fluid culture and larger number of acid-fast bacillus in staining due to direct spread of pulmonary TB [12].
![Page 6: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/6.jpg)
6General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Chronic tuberculous empyema is characterized by a collection of grossly purulent pus in pleural cavity and persistent pleural infections, resulting in marked thickening, even calcification of the visceral and parietal pleura [13]. The inflammatory process may be present for years with rare clinical symptoms. A patient often visits clinical services at the time of a routine chest radiograph or after the development of fibrocavitary lung disease, bronchopleural fistula or empyema necessitans, i.e., extension of empyema out of the thorax and into the chest wall and soft tissues [11,14]. The diagnosis of tuberculous empyema is suspected on the chest CT imaging by finding a thick, calcific pleural plaques and rib thickening surrounding loculated pleural fluid. The pleural purulent fluid is smear-positive for acid-fast bacilli [15]. With the implementation of pleural tissue culture obtained at surgery, the novel combination of sputum, pleural fluid, and pleural tissue culture provides an excellent diagnostic yield [16]. Various status of the disease may indicate different treatment strategies. Open drainage leads to better outcomes with complete drainage of pleural pus and resolution of pleural infections [17].
Hidden Tuberculous Pleurisy
The clinical presentations of TB pleurisy are usually nonspecific and have an insidious course in concomitance with other organisms, thus resulting in diagnostic challenges. For example, Pseudomonas oryzihabitans, a rarely encountered human pathogen, was reported to cause a concurrent bacteremia hiding with TB pleurisy, which was finally diagnosed by histopathologic and microbiologic studies [18]. On the other hand, lung cancers hidden behind tuberculous empyema may present an advanced tumor stage, and the diagnosis could be delayed. The most common lung cancer is squamous cell carcinoma [19]. We experienced a patient with concurrent Escherichia coli bacteremia with insidious TB pleurisy, which was diagnosed by pleural biopsy revealing caseating granuloma, epithelioid histiocytes and Langhans’ giant cells (Figure 4).
Figure 4: A patient with tracheostomy and pleural effusion developed concurrent Escherichia coli bacteremia with insidious tuberculous pleurisy, which was diagnosed by pleural biopsy
reporting caseating granulomas, epithelioid histiocytes and Langhans’ giant cells.
![Page 7: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/7.jpg)
7General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
In similar, a patient manifested with right lower lung pneumonia patches showing on the chest x-ray film, and his sputum culture yielded Pseudomonas aeruginosa. The patient initially received anti-Pseudomonas antibiotic therapy with poor clinical response. Then, the CT of the chest reveled necrotizing pneumonia with lobulated pleural effusion. The pleural histopathology suggested tuberculous empyema (Figure 5).
Figure 5: Tuberculous empyema is hidden behind Psudomonas aeruginosa pneumonia. The computed tomography scan of the chest is showing necrotizing pneumonia with lobulated pleural effusion.The acid-fast stain and mycobacterial cultures of the sputum and pleural effusion were all negative.Surgical decortications and wedge resection for empyema and lung abscess were performed by video-assisted thoracoscopic surgery (VATS). The pleural histopathology disclosed granulomatous inflammation, epithelioid histiocytes and multinucleated giant cells, suggesting tuberculous empyema. Subsequent anti-tuberculous chemotherapy achieved good outcome.
DIAGNOSISConventional Diagnosis of Pleural TB
The diagnosis of active pleural TB disease remains a challenge, especially in high-burden areas. In about two-thirds of the cases the diagnosis depends on clinical suspicion along with pleural fluid biochemistries (i.e., LDH and lymphocytic exudates) and exclusion of other potential causes for the effusion [8]. Pleural TB is one of the main etiologies of lymphocytic pleurisy. However, diagnosis is difficult if based on mycobacteriology using solid Lowenstein-Jensen media or Mycobacterial Growth Indicator Tube (MGIT) culture that is time-consuming and not sensitive enough, or relied on histology that requires invasive biopsy procedure [8]. The tuberculin test (TST) has a sensitivity of 99 % and a specificity of 95 % for TB diagnosis. In high TB burden areas,
![Page 8: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/8.jpg)
8General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
the sensitivity and specificity of TST for pleural TB were 69% and 87%, respectively [20]. To further confirm the disease, sputum induction (in addition to pleural fluid) for acid-fast bacilli by a microscopy of direct smears and culture is a recommended procedure in all patients with suspected pleural TB. The most common staining techniques used are Ziehl-Neelsen and Kinyoun stains, and the fluorescent technique, auramine-rhodamine stains. The sputum positive for acid-fast bacilli was low in free-flowing effusion group (9.3%) and increasing with the severity of pleural effusion in 25% of multiloculated effusion and 46% of organized effusion [12]. Mycobacteria are detected in less than 50% of pleural samples [21]. TB culture of pleural fluid had low sensitivity with a range from 12% to 70%; and 42% from the organized effusion group [12]. The culture is the gold standard and it has a sensitivity of 80 % and a specificity of over 90 %, but the results take weeks. The polymerase chain reaction (PCR) for tuberculous nucleic acid amplification test has an overall sensitivity and specificity of 85% and 97%, respectively. PCR directed to the IS6110 sequence of TB organism in pleural fluid was 74% sensitive and 90% specific for pleural TB that had been confirmed by either culture or pleural biopsy specimens [22]. The characteristic pleural involvement, granulomas with or without caseous necrosis, is evident in 56 to 80% of cases from samples obtained by percutaneous pleural biopsy [21]. Percutaneous closed pleural biopsy for culture has a sensitivity of 85 %, which becomes 98 % if it is taken by thoracoscopy, which provides the highest diagnostic yield [23].
GeneXpert MTB/RIF
The GeneXpert MTB/RIF assay (Xpert) is a PCR test that can identify both TB and rifampicin resistance. Xpert assay is an innovative tool, for prompt detection of pulmonary TB and drug resistance. It is an attractive test, with high sensitivity and specificity along with turnaround time of 2 hours, which facilitates timely diagnosis and appropriate management of TB cases.
Xpert assay is a sensitive method for rapid diagnosis of TB, especially in smear negative cases and in extra pulmonary TB as compared to the conventional Ziehl-Neelsen staining [24]. Xpert of effusion samples showed high sensitivity (84.3%), specificity (100%), with positive predictive value (PPV, 100%), and negative predictive value (NPV, 97%), for diagnosis of TB pleuritis and pericarditis [25]. The Xpert can also dramatically improve the rapid diagnosis of the extra pulmonary TB. In a study of 521 non respiratory specimens (91 urine, 30 gastric aspirate, 245 tissue, 113 pleural fluid, 19 cerebrospinal fluid, and 23 stool specimens), the combined sensitivity and specificity of the Xpert were calculated to be 77% and 98%, respectively. The systematic use of Xpert will increase early TB case confirmation [26].
However, some reports showed substantially low sensitivity of Xpert on pleural fluid that limits the usefulness of Xpert to diagnose pleural TB. Xpert sensitivity and specificity in pleural fluid was 23% and 98% respectively, if based on TB culture and/or histopathology by pleural biopsy as the reference standard [27]. In similar, Xpert has a sensitivity of 46% and a specificity of 99% in diagnosing TPE [28]. The multiplex PCR (M-PCR) targeting mpb64 (Rv1980c)/ IS6110
![Page 9: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/9.jpg)
9General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
and Xpert in pleural fluids for pleural TB diagnosis show the sensitivities of 90 and 33%, and specificities of 97 and 100%, respectively. M-PCR showed superiority over Xpert assay and may facilitate an efficient diagnosis of pleural TB [29]. Thoracoscopic pleural tissue provids higher yields than pleural fluid in both Xpert and TB culture. One study showed that TB was found in 14% of pleural fluid Xpert and in 17% of pleural fluid culture. Thoracoscopic pleural biopsy results in increased sensitivity on Xpert testing, which provided a higher diagnostic yield than pleural tissue culture in TB detection (45% versus 39%) and substantially improved yield compared with closed pleural biopsy [23].
Advanced Diagnosis of Pleural TB
Pleural TB remains difficult to diagnose despite numerous diagnostic tools. The accuracy of currently available same-day diagnostic tools (smear microscopy and nucleic acid amplification tests) for pleural TB is sub-optimal. The conventional acid fast bacilli smear and TB culture of pleural effusion and TST in TB pleurisy are unable to meet clinical needs because of their low sensitivities and specificities. Even when acid-fast bacilli staining and PCR for effusion samples tested negative, TB should be included in the differential diagnosis [30] and pleural biopsy should be performed to confirm the diagnosis. Newer technologies may offer alternatively improved detection.
Adenosine Deaminase (ADA)
The ADA can be determined in pleural fluid with a sensitivity and specificity of 95%.The specificity of ADA increases if only lymphocytic exudates are considered [31]. Where the prevalence of TB is high the presence of a lymphocyte-predominant exudate with a high ADA has a PPV of 98%. The pleural fluid ADA levels greater than 40U/L is strongly suggestive of pleural TB. In low prevalence areas, the absence of an elevated ADA and lymphocyte predominance makes TB very unlikely [7,31]. Therefore, pleural ADA should be routinely used to rule in TB in areas with moderate to high TB prevalence or to rule out TB in areas with low TB prevalence, respectively [32]. Pleural fluid ADA >35U/L yielded 93% sensitivity and 90% specificity for the diagnosis of TB among lymphocytic exudates [32]. With a cutoff value of 15.35 IU/L, the sensitivity and specificity of ADA for the diagnosis of TPE were 93% and 96%, respectively [33]. A higher ADA level can occur in neutrophilic than lymphocytic TBE (111.6U/L versus 62.4U/L), p=0.002 [32]. However, other disorders, such as empyema and rheumatoid pleural effusions might also demonstrate significantly higher activities of ADA than parapneumonic, nonspecific and malignant pleural effusions [34]. An extremely high ADA activity should raise suspicion of empyema or lymphoma [32]. The other shortcoming of the ADA test is its inability to provide culture and drug sensitivity information, which is important in countries with a high degree of resistance to anti-TB drugs [31].
![Page 10: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/10.jpg)
10General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Probably originated from the monocytes and macrophages, the rise in ADA and its isoenzyme of ADA2 activity in the pleural fluid of TB pleurisy patients, with diagnostic thresholds of 47 and 40U/L, has the sensitivities for tuberculosis of 100%, 100%; specificities 91%, 96%; and efficiency of 93%, 97%; respectively. Thus ADA-2 is a more efficient diagnostic marker of TB pleurisy than total ADA activity, although the difference is not statistically significant [35]. Other study also showed higher diagnostic value of ADA2 than ADA with respective sensitivities of 97% and 92%;as well as specificities of 94% and 90% [28]. A predominate ADA2 of total ADA may increase the sensitivity and specificity of the ADA measurement slightly in diagnosing TB pleuritis [1].
Interferon-Gamma (IFN-γ) by Enzyme-Linked Immuno Sorbent Assay (ELISA)
Several reports have shown that tuberculous infection elicits a Th1-like immune response with increased levels of interferon-gamma (IFN-γ) cytokine. Activated CD4+ T lymphocytes release IFN-γ that increases the mycobactericidal activity of macrophages [1]. The blood IFN-γ level accurately identifies TB in all patients and the pleural fluid IFN-γ level is an accurate marker for the diagnosis of pleural TB [36]. Estimation of IFN-γ levels in pleural fluid done by ELISA technique is a useful diagnostic modality for TPE. The increased level of pleural IFN-γ has a sensitivity of 95% and a specificity of 83% for diagnosis of pleural TB [37]. Based on TB culture and/or histopathology by pleural biopsy as the reference standard, the sensitivity and specificity of IFN-γ (107.7pg/ml; rule-in cut-point) was 93% and 96% respectively. IFN-γ has significantly better sensitivity than Xpert [27]. A cut off 138pg/ml provides the best sensitivity and specificity for diagnosis of TB. The sensitivity, specificity, NPV, and PPV were found to be 90%, 97%, 86%, and 98%, respectively [38]. The pleural fluid IFN-γ levels and ADA levels in TB effusions were significantly higher than the non-TB effusions, which are excellent diagnostic strategies and good alternatives to the conventional invasive diagnostic tests [39]. The statistical differences in pleural fluid levels (mean) of ADA (83.3U/L vs 25.8U/L, p<0.0001) and IFN-γ (137 IU/mL vs 0.41 IU/mL, p<0.0001) between pleural TB and other causes of effusion were significant [40]. In a recent study, concentration of INF-γ in pleural effusion of patients with TB pleurisy was 468.6 ± 24.8ng/l, which was significantly higher than that in control groupof non-TB pleurisy (131.3±18.7ng/l), p<0.05 [41]. In patients with lymphocyte-predominant pleural exudates, the combination of ADA ≥40 IU/L and IFN-γ ≥75pg/mL levels in pleural effusion yielded a specificity of 100%, implying a very high probability of TB pleurisy [42].
Interferon-Gamma Release Assay (IGRA)
The release of IFN-γ by T lymphocytes increases at a localized site of infection with TB antigen. The interferon-gamma release assay (IGRA) by using rechallenge with TB antigen to T lymphocytes is established for identifying latent tuberculosis. IGRA measures IFN-γ release by sensitized T-cells from peripheral blood or pleural fluid when T-cells react with highly specific
![Page 11: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/11.jpg)
11General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
TB-specific antigens, such as early secretory antigen (ESAT)-6 and culture filtrate protein (CFP)-10 [43]. IGRA is a promising method for diagnosing TB in low TB burden countries. Currently it is still evolving in the diagnosis of active extra pulmonary tuberculosis [44]. The IGRA seems less effective than unstimulated IFN-γ and ADA activity for TPE with a sensitivity of 75% and a specificity of 82% in blood and a sensitivity of 80% and a specificity of 72% in pleural fluid [28].
Besides, the specificity of IGRAs for diagnosis of active TB disease is limited by an inability to distinguish latent disease. Because the diagnostic performance for active pleural TB was highly variable between studies and settings, there was inadequate evidence to support the use of IGR As in the diagnosis or exclusion of active pleural TB [45]. From19 studies of systematical analysis for the diagnostic performance of blood- and pleural fluid-based IGRAs in TPE, the pooled sensitivity and specificity for the blood assays were 77% and 71% respectively. The pooled sensitivity and specificity for the pleural fluid assays were 72% and 78% respectively. Thus it seems that the commercial IGRAs, performed either on blood or pleural fluid samples, have poor diagnostic accuracy in patients suspected to have TPE [44]. Nonetheless, in a recent meta-analysis of 24 articles, for extra sanguinous body fluids, the pooled sensitivity and specificity were 87% and 89% respectively. The pooled sensitivity and specificity for the peripheral blood were 83% and 74% respectively. IGRAs performed on extra sanguinous body fluids exhibited a better diagnostic accuracy in diagnosing TB compared to IGRAs performed on peripheral blood [46]. For the detection of the release of IFN-γ in blood samples there are currently two tests available: Quanti FERON-TB Gold In-Tube (sensitivity 70% and specificity 90%), and T-SPOT.TB (Oxford Immunotec Ltd, Abingdon, UK) with enzyme-linked immune spot (ELISPOT) method (sensitivity 90% and specificity 93%).
Quanti FERON-TB Gold In-Tube (QFT-GIT)
The sensitivity and specificity using the Quanti FERON-TB Gold In-Tube (QFT-GIT) in pleural fluid for the diagnosis of TPE were 49% and 79% respectively. QFT-GIT test has poor accuracy in the diagnosis of TPE, largely because of a high number of indeterminate results due to high background IFN-γ production in the TPE [47]. The QFT-GIT may be more useful in diagnosing TPE in some countries, for example, with sensitivity, specificity, PPV, and NPV, respectively, of 77%, 61%, 74%, and 65% in Korea [48]. However, in some high tuberculosis prevalence area, the sensitivity and specificity of QFT-GIT were 93.1% and 90.0%, respectively. The sensitivity and specificity of TB-specific nested-PCR in pleural effusion were 95% and 90%, respectively. Furthermore, combined QFT-GIT and nested-PCR detection improves the specificity to 100% with a sensitivity of up to 90% [20]. This combination of immunoassay and molecular detection enhances the clinical diagnosis of pleural TB. The whole blood QFT-GIT assay is not superior to pleural ADA in the diagnosis of TPE and combined whole blood QFT-GIT and pleural ADA detection can improve the diagnosis of TPE with both the specificity and PPV to 100% [33]. Positive QFT-GIT tests were significantly more frequent in patients with confirmed pleural TB, as
![Page 12: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/12.jpg)
12General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
compared to patients with an alternative diagnosis, both in blood (78 vs. 37%, p=0.006) and in pleural effusion (83% vs. 47%, p=0.02). In blood samples, QFT-GIT had 78% sensitivity and 63% specificity, resulting in 56% PPV and 82.6% NPV. In pleural effusion samples, QFT-GIT sensitivity was 83% and specificity 53% (PPV 52% and NPV 84%). QFT-GIT might have a role in ruling out pleural TB in clinical practice [49].
T Cell Enzyme-Linked Immune Spot for Tuberculosis (T-SPOT.TB)
The T-SPOT.TB assay produced less indeterminate results than the QFT-GIT did in both pleural fluid and peripheral blood. The pleural fluid T-SPOT.TB test could be the most useful test among the IGRAs for diagnosing TB pleurisy in an area with an intermediate prevalence of TB infection [50]. The sensitivity of T-SPOT.TB test for pleural fluid and peripheral blood was similar (96.3% and 92.7%, respectively). In contrast, the specificity of pleural fluid T-SPOT.TB (94.5%) was significantly higher than that of peripheral blood T-SPOT.TB (76.1%) (p=0.002). The diagnostic accuracy of peripheral blood T-SPOT.TB is low in high TB burden countries due to latent tuberculosis infection. Besides, advanced age and immune suppression are independently associated with weak positive T-SPOT.TB responses [51]. Pleural fluid T-SPOT.TB is a relatively useful and relatively accurate supplementary assay for the diagnosis of pleural TB in high TB burden countries, and the combination of pleural fluid ADA and T-SPOT.TB is of diagnostic value [52]. T-SPOT.TB in pleural fluid performed better than that in peripheral blood and the ADA activity test in pleural fluid for TB pleurisy diagnosis. Parallel combination of T-SPOT.TB and ADA activity test in pleural fluid showed increased sensitivity (97%) and specificity (88%), whereas serial combination showed increased specificity (98%) [53].
T-SPOT.TB is useful for a rapid and reliable diagnosis of pleural TB using pleural fluid mononuclear cells (PFMC) in clinical practice, especially in area with high TB burden [54]. The sensitivity, specificity, PPV, and NPV of the IGRA ELISPOT assay using PFMC for the diagnosis of pleural TB were 100%, 89%, 98%, and 100%, respectively [55]. Another study in the European Tuberculosis Network reported that the sensitivity and specificity of T-SPOT.TB for the diagnosis of active pleural TB when performed on PEMCs were 95 and 76%, respectively [56].
Chemokine Receptor CXCR3 and Chemokines
Cytokines and chemokines are important in the pathogenesis of TB. The chemokines CXCL9, CXCL10 and CXCL11, also known as monokine induced by interferon-γ (MIG), interferon-inducible protein-10 KDa (IP-10) and interferon-inducible T cell α-chemoattractant (I-TAC), respectively, were ligands of a common primary receptor CXCR3, a member of the CXC chemokine family. They are Th1-associated chemoattractants and are strongly induced by cytokines, particularly IFN-γ, during infection, which specifically chemoattract activated T cells by signaling through the chemokine receptor CXCR3. The CXCR3 ligands are useful clinical markers for the TB diagnosis and for the evaluation of early treatment response [57]. Levels of CXCR3 ligands in pleural effusion are useful for diagnosing TPE. Moreover, the biomarker levels of ADA activity, IFN-γ,
![Page 13: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/13.jpg)
13General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
CXCR3 ligands, in serum samples and pleural fluid were significantly higher in the TPE than non-TB conditions. Combining the levels of CXCL9, IFN-γ and ADA in pleural fluid improved the diagnostic performance [58].
CXCL10/IP-10 and CXCL9/MIG had the highest diagnostic values in distinguishing TB from latent tuberculosis infection. However, IP-10 and MIG levels in plasma are not different between TB and non-TB lung disease. In contrast, the IP-10 and MIG in the pleural effusion show promising diagnostic values and can be used as a marker in discriminating TB and non-TB pleural effusion. A longitudinal study showed that the plasma levels of IP-10, MIG, and IFN-γ decreased after successful treatment of TB [59]. Activated bronchial epithelium is an important source of IP-10 and MIG, which may play an important role in the recruitment of activated T cells in pulmonary TB diseases [60]. The combined IFN-γ, IP-10, MIG multiplex detection had improved diagnostic performance for tuberculosis [61]. Furthermore, the activated T cells, Th1 cytokines, CXC receptors and IP-10 chemokines in TB pleural fluid were significantly higher compared to blood, also supporting diagnostic values of IP-10 in TB pleurisy [62]. Besides, expression of soluble CD26 activated T cells in pleural fluid was correlated with levels of ADA and IFN-γ in the TPE, which is implicated in Th1-like immune response, and may be a useful marker for TB pleurisy [63].
In addition, CXCL12 (a ligand of chemokine receptor CXCR4) level in TB effusion (4456±1013pg/mL) was significantly higher than non-TB effusion (2851±1229pg/mL), p<0.01. On the other hand, serum CXCL12 level showed no significant differences among TB pleurisy, non-TB pleurisy, and normal healthy subjects. With a cut-off value of 4600pg/mL, the sensitivity and specificity of CXCL12 in pleural fluid for the diagnosis of TB pleurisy was 60.0% and 93.2%, respectively. As the source of CXCL12, pleural mesothelium, endothelium of pulmonary vessels, bronchial epithelium, multinucleated giant epithelioid cells and macrophages were all positive for CXCL12 staining. A diagnostic strategy including CXCL12 level in pleural fluid could be promising for diagnosis of TB pleurisy [64].
Interleukin (IL)-27
In a recent study, concentration of IL-27, a member of the IL-12 cytokine family, in pleural effusion of patients with TB pleurisy was 423.4±37.2ng/l, which was significantly higher than that in control group of non-TB pleurisy (116.2±15.5ng/l, p<0.05) [41]. Concentration of IL-27 in serum of patients with TB pleurisy were 41.7±10.6ng/l, which was significantly higher than those in the control group (35.3±8.4ng/l, p<0.05). Besides, relative expression levels of IL-27 mRNA in patients with TB pleurisy were significantly higher than those in control group (p<0.05) [41].
Galectin-9
A matricellular protein galectin-9 (Gal-9) level in pleural effusion is largely increased than that of plasma level (936 versus 3pg/mL) in patients with pleural TB. The pleural fluid cell culture supernatant exhibited higher concentration of Gal-9 compared to peripheral blood mononuclear
![Page 14: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/14.jpg)
14General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
cells. Furthermore, Gal-9 alone could stimulate IFN-γ synthesis in pleural fluid cell culture or T-SPOT.TB ELISPOT assay, which may promote apoptosis and necrosis. These findings suggest that Gal-9 could modulate immune responses and participate in immunopathology of pleural effusion during TB infections [65].
Surgical Diagnosis of Pleural TB
An undiagnosed exudative pleural effusion is often a difficult diagnostic dilemma that needs further histological study for a definitive etiological diagnosis. The advent of video-assisted thoracic surgery allows a new approach of diagnosis by tissue pathology. The majority of diagnostic interventions and selected cases requiring lung resection can be performed through a mini-invasive approach. There are two specific problems regarding TB pleural effusions: for diagnosis, 15-25% of them remain undiagnosed using the conventional methods of diagnosis; and for treatment, there have a tendency for the sequelae of dense adherences and loculations. Mini-invasive surgical techniques with video assistance by thoracoscopic surgery (VATS) or through a minithoracotomy may help in the management of TB pleurisy with minor risks of morbidity and mortality, a high definitive diagnostic accuracy and effective treatment of pleural effusions [66]. The surgical indications for a diagnostic purpose in patients include pleural, pericardial, lung, mediastinal or thoracic wall involvement or lymph node biopsy and 14% of the VATS detected pleura pulmonary tuberculosis [67]. VATS is safe and effective in achieving the diagnosis of tuberculosis through pleural biopsies or wedge lung resection of undefined causes of pulmonary nodules or abscesses; it is particularly useful for those patients who are debilitated, thus making them poor candidates for conventional open surgery [67].
SURGICAL MANAGEMENTUltrasound guided pigtail catheter insertion with large-bore tube drainage has become the
best initial treatment for the patients with free-flowing TPE [12]. Surgery has been the unique therapeutic tool for a long time before the advent of specific anti tuberculous drugs. The role of surgery was confined to the treatment of the sequelae of pleural TB and their complications. Some cases may require operative interventions and may represent a challenge for the thoracic surgeon. The surgical indications for therapeutic purposes were management of pleurisy with multi loculated effusion, organized TPE or empyema, pleura pericarditis, pulmonary nodules, fibrocavitary tuberculosis with lung abscess or cavity. Pleural empyema is one of the most common reasons for surgical treatment on patients with pulmonary TB [68,69].
Video-Assisted Thoracoscopic Surgery (VATS)
Pleural fluid loculations due to tubercular effusion can be managed either by VATS or less invasive approach of intra pleural fibrinolytic therapy (IPFT). If used early in loculated pleural effusion, IPFT can break loculations and early pleural peel, thereby facilitating pleural space drainage with a response rate of 63% [70]. But for multi loculated and organized TPE, IPFT with
![Page 15: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/15.jpg)
15General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
streptokinase irrigation can improve only about 30% of patients [12]. In patients with trapped lung or tuberculous empyema, VATS could achieve full lung reexpansion with minimal morbidity [67]. If therapeutic lung resection by lobectomy is indicated for a tuberculous lung abscess or cavity, VATS lobectomy is an effective and minimally invasive method for treatment, as demonstrated in one of our cases (Figure 5). VATS therapeutic resection could be safely performed in selected patients with medically failed pulmonary TB as an effective adjunct with satisfactory results [71]. It could be safely performed using multi-incision thoracoscopic segmentectomy by two-port approach or three-port triangular approach. The bidigital technique could be used in order to achieve greater room for exploration [72]. The operation time, postoperative complications, postoperative pain index at 24 hours after surgery, postoperative parenteral narcotics requirement and postoperative hospital stay were all significantly less in the VATS group than the open lobectomy group by conventional thoracotomy [67,73].
Thoracic empyema cases can be divided into three stages based on disease development: stage I is an exudative phase characterized by a clear, thin, and sterile pleural effusion; stage II represents a transitional or fibri-nopurulent phase, in which the fluid becomes thick, infected, and purulent; stage III is an organizing or consolidation phase, which involves the formation of granulation tissue and lung encasement. Stage III patients have chest CT scan features of extensive adhesion, separation, fiberboard, or incomplete lung re-expansion [74].
It was traditionally suggested that VATS for tuberculous empyema is effective only for stage II disease, and open thoracotomy with decortication are indicated for stage III empyema [75]. Nowadays, thoracoscopic decortication of advanced tuberculous empyema is feasible, safe, and effective with good outcomes in selected patients [76]. Even thick fibers (1-2cm) in stage III could be cured after decortication by VATS. Nonetheless, the complications in stage III cases (44%) were higher compared with other individuals (5%). This might result from: (1) poor nutritional status and decreased immune function in patients; (2) intraoperative damage to pleural tissue and lung parenchyma; (3) difficulty in stripping the thickened fiberboard and easily damaged peripheral tissue; (4) possible drug resistance during anti-tuberculosis treatment. Early recurrence might mainly be caused by inadequate stripping of the fiberboard [77]. Differential penetration of anti-TB drugs between serum and pleural fluid might explain the reasons of acquired drug resistance in TB empyema. Simultaneous administration of oral and intrapleural anti-TB drugs could achieve a cure result [78]. The combination of tube thoracostomy or catheter drainage and high-dosing anti-TB drugs that reach the high end of the normal range in serum level increase the chances of successful treatment [13].
Conventional Thoracotomy and Robotic Lobectomy
Some cases may require conventional open thoracic surgery. For example, multiple cavities, multiple aspergillomas, multilobar tuberculoma, extensive pleural thickening, and peribronchial lymph node calcification may limit the use of VATS [71,79]. Pulmonary tuberculosis associated
![Page 16: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/16.jpg)
16General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
with dense pleural and vascular adhesionsis indicated for open thoracotomy surgery. Currently, thoracotomy is the standard access to perform lung resections for tuberculosis, despite of the widespread use of the VATS technique. Robotic surgical system aimed to perform successfully minimally invasive operations for these lesions has increasingly received world-wide acceptance. The main elective indications for surgery using the DaVinci Si surgical system in advanced pulmonary tuberculosis are persistent cavitary tuberculosis after four to 6 months of supervised anti-tuberculosis chemotherapy, failure of anti-tuberculosis chemotherapy in cases with multi-drug resistant and extensively drug-resistant tuberculosis, complications and sequelae of the tuberculosis process [80]. Robot-assisted lobectomy generally demonstrates efficacy and safety in standard lobectomy with pulmonary tuberculosis.
CONCLUSIONExtra pulmonary TB accounts for ~15% of all TB patients, while pleural TB is the most
common form of extrapulmonary TB. Pleural TB should be considered in a patient who presents with undiagnosed pleural effusion, particularly with lymphocytic predominance. Measurement of pleural fluid ADA and IFN-γ levels is useful in the diagnosis of TB pleurisy. In patients with lymphocytic pleural effusion, pleural fluid levels of greater than 40 U/L ADA and 75pg/mL IFN-γ are suggestive of a diagnosis of TB pleuritis, especially in areas with a high prevalence of tuberculosis. The PCR assays in pleural fluid demonstrate high specificity but poor sensitivity in identifying TB. Thoracoscopic pleural biopsy provides a high diagnostic yield in confirming pleural TB. Furthermore, VATS can effectively treat complicated TB pleuritis, empyema or lung abscess by decortication, wedge resection and/or lobectomy with improved outcome.
ACKNOWLEDGEMENTWe declare compliance with ethical standards and no financial funding for this work. No
potential conflicts of interest were disclosed.
References1. Cohen LA, Light RW. Tuberculous pleural effusion. Turk Thorac J. 2015; 16: 1-9.
2. Gopi A, Madhavan SM, Sharma SK, Sahn SA. Diagnosis and treatment of tuberculous pleural effusion in 2006. Chest. 2007; 131: 880-889.
3. Kim JS, Shim SS, Kim Y, Ryu YJ, Lee JH. Chest CT findings of pleural tuberculosis: differential diagnosis of pleural tuberculosis and malignant pleural dissemination. Acta Radiol. 2014; 55: 1063-1068.
4. Neves DD, Dias RM, Cunha AJ. Predictive model for the diagnosis of tuberculous pleural effusion. Braz J Infect Dis. 2007; 11: 83-88.
5. Light RW, Macgregor MI, Luchsinger PC, Ball WC. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med. 1972; 77: 507-513.
6. Heffner J, Brown L, Barbieri C. Diagnostic value of tests that discriminate between exudative and transudative pleural effusions. Primary Study Investigators. Chest.1997; 111: 970-980.
7. Shaw JA, Irusen EM, Diacon AH, Koegelenberg CF. Pleural tuberculosis: A concise clinical review.ClinRespir J. 2018.
8. Porcel JM. Advances in the diagnosis of tuberculouspleuritis. Ann Transl Med. 2016; 4: 282.
![Page 17: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/17.jpg)
17General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
9. Wang CY, Hsiao YC, Jerng JS, Ho CC, Lai CC, et al. Diagnostic value of procalcitonin in pleural effusions. Eur J ClinMicrobiol Infect Dis. 2011; 30: 313-318.
10. Cakir E, Deniz O, Ozcan O, Tozkoparan E, Yaman H, et al. Pleural fluid and serum procalcitonin as diagnostic tools in tuberculous pleurisy. ClinBiochem. 2005; 38: 234-238.
11. Kundu S, Mitra S, Mukherjee S, Das S. Adult thoracic empyema: A comparative analysis of tuberculous and nontuberculous etiology in 75 patients. Lung India. 2010; 27: 196-201.
12. Xiong Y, Gao X, Zhu H, Ding C, Wang J. Role of medical thoracoscopy in the treatment of tuberculous pleural effusion. J Thorac Dis. 2016; 8: 52-560.
13. Long R, Barrie J, Peloquin CA. Therapeutic drug monitoring and the conservative management of chronic tuberculous empyema: case report and review of the literature. BMC Infect Dis. 2015; 15: 327.
14. Dunphy L, Shetty P, Kavidasan A, Rice A. Unusual cause of chest pain: empyema necessitans and tubercular osteomyelitis of the rib in an immunocompetent man. BMJ Case Rep. 2016.
15. Sahn SA, Iseman MD. Tuberculous empyema. Semin Respir Infect 1999; 14: 82-87.
16. Ong K, Rajapaksha K, Ong CS, Fazuludeen AA, Ahmed ADB. Triple cultures increase the diagnostic sensitivity of Mycobacterial Tuberculosis Empyema. Tuberc Res Treat. 2017; 4362804.
17. Sonmezoglu Y, Turna A, Cevik A, Demir A, Sayar A, et al. Factors affecting morbidity in chronic tuberculous empyema. Thorac Cardiovasc Surg. 2008; 56: 99-102.
18. Lin TY, Wu SW, Lin GM, Chen YG. Hidden diagnosis of Tuberculous pleurisy masked by concomitant Pseudomonas oryzihabitans bacteremia. Respir Care. 2012; 57: 298-301.
19. Xu H, Koo HJ, Lee HN, Lim S, Lee JW, et al. Lung cancer in patients with tuberculousfibrothorax and empyema: Computed tomography and 18F-Fluorodeoxyglucose positron emission tomography findings. J Comput Assist Tomogr. 2017; 41: 772-778.
20. Gao Y, Ou Q, Huang F, Wang S, Shen L, et al. Improved diagnostic power by combined interferon-gamma release assay and nested-PCR in tuberculous pleurisy in high tuberculosis prevalence area. FEMS Immunol Med Microbiol. 2012; 66: 393-398.
21. Ferrer J. Tuberculous pleural effusion and tuberculous empyema. Semin Respir Crit Care Med. 2001; 22: 637-646.
22. Villegas MV, Labrada LA, Saravia NG. Evaluation of polymerase chain reaction, adenosine deaminase, and interferon-gamma in pleural fluid for the differential diagnosis of pleural tuberculosis. Chest. 2000; 118: 1355-1364.
23. Christopher DJ, Dinakaran S, Gupta R, James P, Isaac B, et al. Thoracoscopic pleural biopsy improves yield of Xpert MTB/RIF for diagnosis of pleural tuberculosis. Respirology. 2018.
24. Iram S, Zeenat A, Hussain S, Wasim Yusuf N, Aslam M. Rapid diagnosis of tuberculosis using Xpert MTB/RIF assay - Report from a developing country. Pak J Med Sci. 2015; 31: 105-110.
25. Saeed M, Ahmad M, Iram S, Riaz S, Akhtar M, et al. A breakthrough for the diagnosis of tuberculous pericarditis and pleuritis in less than 2 hours. Saudi Med J. 2017; 38: 699-705.
26. Hillemann D, Rüsch-Gerdes S, Boehme C, Richter E. Rapid molecular detection of extrapulmonary tuberculosis by the automated GeneXpert MTB/RIF system. J Clin Microbiol. 2011; 49: 1202-1205.
27. Meldau R, Peter J, Theron G, Calligaro G, Allwood B, et al. Comparison of same day diagnostic tools including Gene Xpert and unstimulated IFN-γ for the evaluation of pleural tuberculosis: a prospective cohort study. BMC Pulm Med. 2014; 14: 58.
28. Mollo B, Jouveshomme S, Philippart F, Pilmis B. Biological markers in the diagnosis of tuberculous pleural effusion. Ann BiolClin (Paris). 2017; 75: 19-27.
29. Sharma S, Dahiya B, Sreenivas V, Singh N, Raj A, et al. Comparative evaluation of GeneXpert MTB/RIF and multiplex PCR targeting mpb64 and IS6110 for the diagnosis of pleural TB. Future Microbiol. 2018; 13: 407-413.
30. Del Cueto-Aguilera Á, Ibarra-Sifuentes HR, Delgado-García G, Atilano-Díaz A, Galarza-Delgado DÁ. Chylothorax and chylous ascites due to Mycobacterium tuberculosis in an AIDS patient whose PCR tested negative. Pneumologia. 2016; 65: 161-163.
31. Porcel JM. Tuberculous pleural effusion. Lung. 2009; 187: 263-270.
32. Porcel JM, Esquerda A, Bielsa S. Diagnostic performance of adenosine deaminase activity in pleural fluid: a single-center experience with over 2100 consecutive patients. Eur J Intern Med. 2010; 21: 419-423.
33. Liu Y, Ou Q, Zheng J, Shen L, Zhang B, et al. A combination of the Quanti FERON-TB Gold In-Tube assay and the detection of adenosine deaminase improves the diagnosis of tuberculous pleural effusion. Emerg Microbes Infect. 2016; 5: e83.
![Page 18: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/18.jpg)
18General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
34. Pettersson T, Ojala K, Weber TH. Adenosine deaminase in the diagnosis of pleural effusions. Acta Med Scand. 1984; 215: 299-304.
35. Valdés L, San José E, Alvarez D, Valle JM. Adenosine deaminase (ADA) isoenzyme analysis in pleural effusions: diagnostic role, and relevance to the origin of increased ADA in tuberculous pleurisy. EurRespir J. 1996; 9: 747-751.
36. Chegou NN, Walzl G, Bolliger CT, Diacon AH, van den Heuvel MM. Evaluation of adapted whole-blood interferon-gamma release assays for the diagnosis of pleural tuberculosis. Respiration. 2008; 76: 131-138.
37. Fernández de Larrea C, Duplat A, Giampietro F, de Waard JH, Luna J, et al. Diagnostic accuracy of immunological methods in patients with tuberculous pleural effusion from Venezuela. Invest Clin. 2011; 52: 23-34.
38. Sharma SK, Banga A. Diagnostic utility of pleural fluid IFN-gamma in tuberculosis pleural effusion. J Interferon Cytokine Res. 2004; 24: 213-217.
39. Sharma SK, Banga A. Pleural fluid interferon-gamma and adenosine deaminase levels in tuberculosis pleural effusion: a cost-effectiveness analysis. J Clin Lab Anal. 2005; 19: 40-46.
40. Aoe K, Hiraki A, Murakami T, Eda R, Maeda T, et al. Diagnostic significance of interferon-gamma in tuberculous pleural effusions. Chest. 2003; 123: 740-744.
41. Zhang M, Xiong D, Li H, Wang Z, Li R. Diagnostic value of T-Spot TB combined with INF-γ and IL-27 in tuberculous pleurisy. ExpTher Med. 2018; 15: 1871-1874.
42. Keng LT, Shu CC, Chen JY, Liang SK, Lin CK, et al. Evaluating pleural ADA, ADA2, IFN-γ and IGRA for diagnosing tuberculous pleurisy. J Infect. 2013; 67: 294-302.
43. Thillai M, Pollock K, Pareek M, Lalvani A. Interferon-gamma release assays for tuberculosis: current and future applications. Expert Rev Respir Med. 2014; 8: 67-78.
44. Aggarwal AN, Agarwal R, Gupta D, Dhooria S, Behera D. Interferon gamma release assays for diagnosis of pleural tuberculosis: a systematic review and meta-analysis. ClinMicrobiol. 2015; 53: 2451-2459.
45. Hooper CE, Lee YC, Maskell NA. Interferon-gamma release assays for the diagnosis of TB pleural effusions: hype or real hope? CurrOpinPulm Med. 2009; 15: 358-365.
46. Wen A, Qu XH, Zhang KN, Leng EL, Ren Y, et al. Evaluation of interferon-gamma release assays in extrasanguinous body fluids for diagnosing tuberculosis: A systematic review and meta-analysis. Life Sci. 2018; 197: 140-146.
47. Ates G, Yildiz T, Ortakoylu MG, Ozekinci T, Erturk B, et al. Adapted T cell interferon-gamma release assay for the diagnosis of pleural tuberculosis. Respiration. 2011; 82: 351-357.
48. Chung JH, Han CH, Kim CJ, Lee SM. Clinical utility of QuantiFERON-TB GOLD In-Tube and tuberculin skin test in patients with tuberculous pleural effusions. DiagnMicrobiol Infect Dis. 2011; 71: 263-266.
49. Losi M, Bocchino M, Matarese A, Bellofiore B, Roversi P, et al. Role of the quantiferon-TB test in ruling out pleural tuberculosis: a multi-centre study. Int J ImmunopatholPharmacol. 2011; 24: 159-165.
50. Kang JY, Rhee CK, Kang NH, Kim JS, Yoon HK, et al. Clinical utility of two interferon-gamma release assays on pleural fluid for the diagnosis of tuberculouspleurisy.TubercRespir Dis (Seoul). 2012; 73: 143-150.
51. Lee YM, Kim SM, Park SJ, Lee SO, Choi SH, et al. Factors associated with a strong response to the T-SPOT.TB in patients with extrapulmonarytuberculosis. Infect Chemother. 2014; 46: 248-252.
52. Liu F, Gao M, Zhang X, Du F, Jia H, et al. Interferon-gamma release assay performance of pleural fluid and peripheral blood in pleural tuberculosis. PLoS One. 2013; 8: e83857.
53. Xu HY, Li CY, Su SS, Yang L, Ye M, et al. Diagnosis of tuberculous pleurisy with combination of adenosine deaminase and interferon-γ immunospot assay in a tuberculosis-endemic population: A prospective cohort study.edicine (Baltimore). 2017; 6: e8412.
54. Zhang L, Zhang Y, Shi X, Zhang Y, Deng G, et al. Utility of T-cell interferon-γ release assays for diagnosing tuberculousserositis: a prospective study in Beijing, China. PLoS One. 2014; 9: e85030.
55. Adilistya T, Astrawinata DA, Nasir UZ. Use of pleural fluid interferon-gamma enzyme-linkedimmunospotassay in the diagnosis of pleural tuberculosis. Acta Med Indones. 2016; 48: 41-47.
56. Losi M, Bossink A, Codecasa L, Jafari C, Ernst M, et al. Use of a T-cell interferon-gamma release assay for the diagnosis of tuberculous pleurisy. EurRespir J. 2007; 30: 1173-1179.
57. Chung WY, Yoon D, Lee KS, Jung YJ, Kim YS, et al. The usefulness of serum CXCR3 ligands for evaluating the early treatment response in tuberculosis: A longitudinal cohort study. Medicine (Baltimore). 2016; 95: e3575.
![Page 19: Pleural Tuberculosis and Application of Video-Assisted ... · Pleural fluid glucose levels with TB pleuritis may be reduced but are usually similar to serum levels [1]. The procalcitonin](https://reader042.pdfslide.us/reader042/viewer/2022031513/5cd096eb88c993cc718de466/html5/page/19.jpg)
19General Thoracic Surgery | www.smgebooks.comCopyright Yu WL.This book chapter is open access distributed under the Creative Commons Attribution 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
58. Chung W, Jung Y, Lee K, Park J, Sheen S, et al. CXCR3 ligands in pleural fluid as markers for the diagnosis of tuberculous pleural effusion. Int J Tuberc Lung Dis. 2017; 21: 1300-1306.
59. Yang Q, Cai Y, Zhao W, Wu F, Zhang M, et al. IP-10 and MIG are compartmentalized at the site of disease during pleural and meningeal tuberculosis and are decreased after antituberculosis treatment.Clin Vaccine Immunol. 2014; 21: 1635-1644.
60. Sauty A, Dziejman M, Taha RA, Iarossi AS, Neote K, et al. The T cell-specific CXC chemokines IP-10, Mig, and I-TAC are expressed by activated human bronchial epithelial cells. J Immunol. 1999; 162: 3549-3558.
61. Wang X, Jiang J, Cao Z, Yang B, Zhang J, et al. Diagnostic performance of multiplex cytokine and chemokine assay for tuberculosis. Tuberculosis (Edinb). 2012; 92: 513-520.
62. Pokkali S, Das SD, R L. Expression of CXC and CC type of chemokines and its receptors in tuberculous and non-tuberculous effusions. Cytokine. 2008; 41: 307-314.
63. Oshikawa K, Sugiyama Y. Elevated soluble CD26 levels in patients with tuberculous pleurisy. Int J Tuberc Lung Dis. 2001; 5: 868-872.
64. Kohmo S, Kijima T, Mori M, Minami T, Namba Y, et al. CXCL12 as a biological marker for the diagnosis of tuberculous pleurisy.Tuberculosis (Edinb). 2012; 92: 248-252.
65. Zhao J, Shiratori B, Chagan-Yasutan H, Matsumoto M, Niki T, et al. Secretion of IFN-γ associated with galectin-9 production by pleural fluid cells from a patient with extrapulmonarytuberculosis. Int J Mol Sci. 2017; 18: E1382.
66. Beheshtirouy S, Kakaei F, Mirzaaghazadeh M. Video assisted rigid thoracoscopy in the diagnosis of unexplained exudative pleural effusion. J CardiovascThorac Res. 2013; 5: 87-90.
67. Yim AP. The role of video-assisted thoracoscopic surgery in the management of pulmonary tuberculosis. Chest. 1996; 110: 829-832.
68. Kerti CA, Miron I, Cozma GV, Burlacu ON, Tunea CP, et al. The role of surgery in the management of pleuropulmonary tuberculosis - seven years’ experience at a single institution.InteractCardiovascThorac Surg. 2009; 8: 334-337.
69. Giller DB, Giller BD, Giller GV, Shcherbakova GV, Bizhanov AB, et al. Treatment of pulmonary tuberculosis: past and present. Eur J Cardiothorac Surg. 2018; 53: 967-972.
70. Barthwal MS, Marwah V, Chopra M, Garg Y, Tyagi R, et al. A Five-year study of intrapleural fibrinolytic therapy in loculated pleural collections. Indian J Chest Dis Allied Sci. 2016; 58: 17-20.
71. Tseng YL, Chang JM, Liu YS, Cheng L, Chen YY, et al. The role of video-assisted thoracoscopic therapeutic resection for medically failed pulmonary tuberculosis. Medicine (Baltimore). 2016; 95: e3511.
72. Tseng YL, Chang CC, Chen YY, Liu YS, Cheng L, et al. From one incision to one port: The surgical technique and the evolution of segmentectomy in patients with pulmonary tuberculosis. PLoS One. 2018; 13: e0197283.
73. Han Y, Zhen D, Liu Z, Xu S, Liu S, et al. Surgical treatment for pulmonary tuberculosis: is video-assisted thoracic surgery “better” than thoracotomy?J Thorac Dis. 2015; 7: 1452-1458.
74. Molnar TF. Current surgical treatment of thoracic empyema in adults. Eur J Cardiothorac Surg. 2007; 32: 422-430.
75. Barbetakis N, Paliouras D, Asteriou C, Tsilikas C. eComment: the role of video-assisted thoracoscopic surgery in the management of tuberculous empyemas. Interact Cardiovasc Thorac Surg. 2009; 8: 337-338.
76. Kumar A, Asaf BB, Lingaraju VC, Yendamuri S, Pulle MV, et al. Thoracoscopic decortication of stage III tuberculous empyema is effective and safe in selected cases. Ann Thorac Surg. 2017; 104: 1688-1694.
77. Chen B, Zhang J, Ye Z, Ye M, Ma D, et al. Outcomes of video-assisted thoracic surgical decortication in 274 patients with tuberculous empyema. Ann Thorac Cardiovasc Surg. 2015; 21: 223-228.
78. Long R, Barrie J, Stewart K, Peloquin CA. Treatment of a tuberculous empyema with simultaneous oral and intrapleural antituberculosis drugs. Can Respir J. 2008; 15: 241-243.
79. Yen YT, Wu MH, Cheng L, Liu YS, Lin SH, et al. Image characteristics as predictors for thoracoscopic anatomic lung resection in patients with pulmonary tuberculosis. Ann Thorac Surg. 2011; 92: 290-295.
80. Yablonskii P, Kudriashov G, Vasilev I, Avetisyan A, Sokolova O. Robot-assisted surgery in complex treatment of the pulmonary tuberculosis. J Vis Surg. 2017; 3: 18.