Embed Size (px)
Citation preview

Case reports
Pleural extramedullary haematopoiesis in myelosclerosis
H. C. ANTONM.B., Ch.B., D.M.R.D., F.F.R.
G. P. LEWISM.D., B.Sc., M.R.C.P.(Ed.)
Stobhill General Hospital, Glasgow
J. B. P. FERGUSONM.B., Ch.B.
DESPITE the extensive literature on myelosclerosisand extramedullary haematopoiesis (myeloid meta-plasia), reference to the pleura as being the site ofextramedullary haematopoiesis is not made ineither the standard medical and pathology text-books or in the radiological literature. We haverecently encountered a case of myelosclerosis inwhich aspiration of what appeared on both clinicaland radiological grounds to be a pleural effusionfailed to reveal the presence of fluid. Subsequentpleural biopsy carried out at the same site showedtissue, at first regarded as tumour, but later shownto be a manifestation of extramedullary haema-topoiesis. Because such a lesion when it occurs atthis particular site is liable to be misinterpreted, wefeel that a description of this case is justified.
Myelosclerosis may be regarded as a form ofmyelofibrosis with thickening of the bonytrabeculae of the marrow on histological exam-ination. The diagnosis of myelofibrosis is madewhen the presence of fibrosis on bone marrowbiopsy is associated with a leuco-erythroblasticanaemia. A mild increase in bone trabeculationmay cause an osteosclerosis visible on X-rayexamination.
Myelofibrosis may be a complicating feature ofmany diseases including lymphoma, metastaticcarcinoma, leukaemia and aplastic anaemia, underwhich conditions it is termed secondary myelo-fibrosis (Pitcock et al., 1962). They emphasize thatin secondary myelofibrosis, evidence of the under-lying disorder may be found on examination ofbone-marrow sections as well as the presence offibrous tissue. Furthermore, in such cases, theblood picture may be distinctive. Myelofibrosiswithout an associated haematological, reticulo-endothelial or neoplastic disorder is classed asbeing idiopathic. The above authors, however,consider that myelofibrosis following poly-cythaemia vera should be included in the idiopathic
myelofibrosis group, because it cannot be differen-tiated pathologically once fibrosis has developed inthe bone marrow. The case to be described belongsto the idiopathic myelofibrosis category.
Extramedullary haematopoiesis accompaniesmany types of bone marrow disease includingidiopathic myelofibrosis, carcinomatosis, lym-phoma, leukaemia, marble bone disease, erythro-blastosis, haemolytic anaemia, pernicious anaemia,thalassaemia, Gaucher's disease, osteitis deformans,osteomalacia, osteitis fibrosa cystica, tuberculosisand exposure to toxic agents such as benzene,fluorine and irradiation. In a recent report, sickle-cell anaemia was found to be associated withextramedullary haematopoiesis (Seidler & Becker,1964). Rarely, extramedullary haematopoietictissue may occur in patients not suffering fromdiseases of the blood or bone marrow. Dodge &Evans (1956) describe a presacral retroperitonealfatty tumour with haematopoietic foci, for whichthey suggest myelolipoma as a suitable descriptiveterm. It should be pointed out that extramedullaryhaematopoiesis does not necessarily occur inmyelofibrosis: Korst, Clatanoff & Schilling (1956)found it in only eleven of their twenty-three cases.
Case reportThe patient, a female aged 65, was admitted to
hospital with a 6-month history of loss of weightand appetite, weakness and severe diarrhoea. Aradium menopause had been carried out 20 yearspreviously for menorrhagia.On examination there was pigmentation of ex-
posed areas of skin, pallor of mucous membranesand marked oedema of the legs and anteriorabdominal wall, but no ascites. The spleen waspalpable and firm and the liver grossly enlargedand tender with some nodularity. There wereclinical signs of a left pleural effusion. This wasconfirmed by a chest X-ray which also showed a
428
copyright. on January 30, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.43.500.428 on 1 June 1967. Dow
nloaded from

Case reports 429
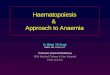
marked sclerosis of bone (Fig. 1). Subsequently theleft pleural reaction diminished on X-ray follow-up, but did not disappear, and later a right-sided
i:·:·:
··i··::..·:··:··:·:
iiiiii::i'::'·:"::;:ibi.lig.i.sllll' .S.I.F.L Icllliliiiii::i:i
iii:::::
li".iti:··:'''';:':
I":i·I'
'::'::::'
.e.slslg.a.::. .:: ::
: .,.·
I:%::.81B._-···i:;i:ii·:··i·ii:.·:·
::··:· :····· ·'·
:r·:··
.:::;·::
···
·.?·:i;
·'· ·::·::··:·:··:··::r::"..: :. :: ::i ::ii::i;:iiiii8li:·
:'··:· ··:· ·· ·· :· ·. :.:::'.:l.:::i:: ··.· :i:P:: ·::·:::··:· ··: '' ': :' ··i:··:I':'· :· ·· '·' ·'-':"- ·····i··I:lii· iil,i·:i: ·ii :: ::: 'ii:iiBCiii;di·.i;:::''''
FIG. 1. Moderate pleural reaction at left lower zone.Patchy osteosclerosis.
i· jjE. _P ·'' .: '# 1 t:
_ i
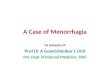
w.i.sflw 4s..* ~~~~FIG. 2. Original pleural biopsy. High power. Markedanisocytosis and poikilocytosis of cells with hyper-chromatic nuclei also varying in size and shape.
pleural reaction developed. Although the first im-pression of one of us was that the bone sclerosiswas probably due to osteoplastic metastases, filmsof the spine and pelvis were later reported as show-ing myelosclerosis. A pleural tap of the left lungbase attempted 1 week after admission failed toreveal the presence of fluid. Because of this, pleuralbiopsy was carried out.The pathology report described a cellular
'tumour' with giant cells, small cells with darknuclei, and a few lymphocytes and eosinophils(Fig. 2). Subsequently a retrospective diagnosis ofmyeloid metaplasia was made. As it seemed likelythat the 'tumour' was secondary, numerous in-vestigations were carried out to locate a primarysource, including IVP and barium studies, but noevidence of a primary focus was found. A sternalpuncture was reported as follows: 'Sections showdense bone, no marrow, a few fat spaces andyoung fibrous tissue replacement. This is highlysuggestive of myelofibrosis.' This diagnosis wasconfirmed by a trephine biopsy of sternum (Fig. 3).Throughout most of her illness the haemoglobin
ranged from 8-2 to 9-5 g/100 ml but terminallyfell to 7-5 g/100 ml. The PCV averaged 29% andthe MCHC varied from 29% to 33%. Reticulo-cytes, at first 2%, reached 5% in the late stages of
iiii.ii:;··:.:·i:.
··'..·:
iisii a:l.%.:·..
6illi.ii.s.'.ii%iOl:ii;.·.:3""%..b.k...en::·:::
.:.. !:i·i·:···: ···:el::: ·.;s.P.pt· :..?;:'
li..P::;dl;il ..j.:i..".:::::···:'-:I..m::.·i..:ii ii81i:: '..:. ..
:::"':':'i:s X- ,;;;,;; _.-IL.ICb:lgl"i :-:.ii.iiii.i:···-:·:;l·:-:·· ·*::. ··.ii:..;:.: :.....
la?:lp-·:·-i siii.vr··· *·· -....-_.i-s!C .:'i* ':'lia·i·; ZiB:;il" r
W.::.·,i·f I·:·.1 .:ti:ir·.·i:··li.l;: :.··· ·:··. b· ::.·.· .·d a:w"i" s..:· :"*r ..i.F,.;:.,..
* .rnyl·_;%'*: ···i·. ·e ·r? t. "· T·:'·:iHi
'*tL·:.·?p:1
i:::::ia ,··r .;
:m161:ie: ii: 1;·'a.':::-·:···p6.;:*· ···:· .li.il iYiCilt?:pl:::: a:; IFiK:;IBil.:i;i ·:··:;·i:
1··-·-·-·-i:i: I::I:I::si i:I:
Kii:Bli.e::11· :k":.i
;i.;.··:···
:-::i::w:·i::-:::::
FIG. 3. Sternal marrow. Normal marrow replaced byyoung loose fibrous tissue with capillary spaces con-taining primitive red cells. Increased trabeculation ofbone gives a mosaic appearance.
copyright. on January 30, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.43.500.428 on 1 June 1967. Dow
nloaded from

Case reports
her illness. White cell counts ranged from 8400 to15,800/mm3. The white cells showed immatureforms, mostly myelocytes but with a few blastcells. Terminally the proportion of primitive cellsrose considerably. Films showed the red cells to bewell haemoglobinated but there was moderateanisocytosis and poikilocytosis. Nucleated red cellswere present. Platelets were increased up to820,000/mm3 and were unusually varied in sizeand shape, some being described as massive.
Other haematological tests showing abnormalityincluded a serum vitamin B12 level of 25 pg/mland a serum iron of 6 tug/100 ml (TIBC 300g/g/100 ml).During the course of her illness, the patient ex-
hibited proteinuria of moderate degree. On thefirst admission the serum urea was 55 mg/100 mlbut with deterioration in her condition graduallyrose so that terminally it was 156. There was mildhyperchloraemia and hyperkalaemia. The totalserum proteins showed a persistent moderate re-duction; the albumin-globulin ratio was normal.Liver function tests were at all times normal apartfrom a raised alkaline phosphatase (35 KAU/100 ml).Oedema and anaemia persisted in spite of
therapy with diuretics, vitamin B12, blood trans-fusion and oral and parenteral iron. In the summerof 1965 her poor general state was complicated bythe development of haematemesis. At the time ofher final admission in August 1965, ascites wasmanifest. She subsequently underwent gradualdeterioration and died 18 months after her firstadmission.
NecropsyThere was clear amber fluid in both pleural
cavities. Over the visceral pleural surfaces of bothlower lobes and in the case of the right, especiallythe diaphragmatic surface, there were discrete flatwhite nodules with serrated edges, measuring from1 to 2 cm in diameter. In places they had becomeconfluent forming large plaques. The lungs wereoedematous and congested and the heart showedslight brown atrophy.Marked peritoneal adhesions and slight ascites
were present. The spleen (1070 g) was greatly en-larged and cut section revealed a diffusely paleinfiltrated surface. The liver (2450 g) was alsogreatly enlarged and on section there were largenodules of white 'tumour' tissue surrounding theporta hepatis. In the right lobe there were discretewhite nodules surrounding the portal tracts,measuring from 1 to 5 cm in diameter. Enlargedglands were present along the line of the portalvein but there were no enlarged glands elsewhere.The kidneys were small, the capsules were removed
with difficulty and revealed a slightly granular sur-face. On section there was 'pouting' of vessels andnarrowing of the cortices. There was pale marrowin the vertebrae but the sternal marrow wasreplaced by fibrous tissue. Other systems showedno abnormality.
Histologically, the marrow was replaced by loosefibrous tissue permeated by capillaries with smallfoci of erythropoiesis and some bizarre mega-karyocytes, i.e. the typical findings of myelofibrosis.There was also an increased trabeculation of bone.The spleen showed extramedullary haemato-
poiesis in the red pulp, fibrosis, bizarre giant cellsprobably megakaryocytes, a moderate degree ofhaemorrhage and slight subcapsular iron deposi-tion. Liver sections showed that the nodules wereformed of young fibrous tissue with small foci ofprimitive haematopoiesis and megakaryocytes. Thenormal liver architecture was not destroyed outsidethe nodules but groups of granulopoietic anderythropoietic cells were identified in and arounddilated sinusoids. Similar histological appearancesto that of the liver nodules were present in thelymph nodes and in the pleural nodules. Thekidneys showed features of chronic pyelonephritis,diffuse membranous glomerulo-nephritis andmoderate arterio and arteriolar sclerosis. Foci ofmyeloid metaplasia were present in the interstitialtissue.
DiscussionThe clinical presentation and course of this
patient's illness is consistent with the diagnosis ofmyelosclerosis with associated extramedullaryhaematopoiesis. The occurrence of intractable andpersistent oedema is difficult to explain on thebasis of hypoalbuminaemia alone. The subsequentdemonstration at post-mortem of chronic pyelo-nephritis with diffuse membranous glomerulo-nephritis helps to clarify this puzzling feature. It isof interest that renal disease of slight to moderatedegree, not characterized by calculi formation, wasfound in five of eight autopsies described byPitcock et al. (1962). The bone sclerosis observedin this case could not, however, have resulted fromrenal disease because of the absence of both un-calcified osteoid seams and osteoclastic erosions,features normally found in uraemic osteodystrophy(Follis & Jackson, 1943; Craven, 1964). Further-more X-ray of the lumbar vertebrae failed toreveal the 'Rugger Jersey' sign of renal osteodys-trophy (band-like increases in the density of theupper and lower parts of the vertebral bodies) des-cribed by Dent (1955).When first seen at the outpatient department the
marked degree of cachexia exhibited by the patientled to a presumptive diagnosis of neoplastic
430
copyright. on January 30, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.43.500.428 on 1 June 1967. Dow
nloaded from

Case reports
disease. This erroneous impression was laterapparently confirmed by the demonstration of'neoplastic tissue' in the specimen obtained bypleural biopsy. During the post-mortem examina-tion the identification of enlarged glands in theregion of the porta hepatis and obvious intra-hepatic nodules seemed again to support thisdiagnosis. That myelofibrosis can mimic carcino-matous metastases of osteoblastic type has beenpointed out by Wyatt & Sommers (1950). Theseauthors emphasize that the metastatic lesions canbe distinguished by the presence of tumour massesin the liver and elsewhere. It therefore came as asurprise when detailed histological studies showedthe tumour-like deposits affecting the glands of theporta hepatis and the liver to be solely foci ofhaematopoietic tissue with an unusual degree offibrotic reaction.The radiological signs in this case correspond to
the description of twenty-five cases of myelo-fibrosis by Leigh et al. (1959). They emphasize thecentral distribution of the osteosclerosis with spar-ing of the peripheral bones and state that whilethe bone density is often diffusely increased, inmore severe cases discrete sclerotic foci are present.As well as osteosclerosis they list splenomegaly andhepatomegaly as other radiological signs, but donot describe lesions in other sites due to extra-medullary haematopoiesis. That unusual sites ofextramedullary haematopoiesis may be mistakenfor other pathological entities has been reportedby many. Close, Taira & Cleveland (1958) describea case of spinal cord compression demonstrated onmyelography later shown to be due to extraduralmyeloid metaplasia associated with myelosclerosis.Similar cases have been reported by Lowman,Bloor & Newcomb (1963) and Appleby et al.(1964).
Intrathoracic extramedullary haematopoiesisshowing on chest X-ray as fairly large, well-defined, lobulated masses located posteriorly inthe paravertebral gutters can present a difficultdiagnostic problem. Such a picture may occur inseminoma metastases and reticulosis (Shanks &Kerley, 1962) but a suspicion of such lesions beingdue to tumour-simulating extramedullary haema-topoiesis may be raised by the blood findings, orby radiological evidence of bone marrow disease.Early reports of intrathoracic tumour-simulatingextramedullary haematopoiesis were based onautopsy findings. The first diagnosis on clinico-radiological grounds, in a patient with acholuricjaundice, was presented by Ask-Upmark (1945).Another case was described by Knoblich (1960) inwhich an initial diagnosis of intrathoracic neuro-fibromata was made. In two cases of congenitalhaemolytic anaemia with paravertebral masses
demonstrated by chest X-ray, thoracotomy wasconsidered mandatory to exclude neoplasticdisease (Hanford, Schneider & MacCarthy, 1960).Two further cases associated with congenitalhaemolytic anaemia have been described in thepaper by Lowman et al. (1963). Malamos, Papa-vasiliou & Avramis (1962) describe a case ofCooley's anaemia showing on chest X-ray charac-teristic rib thickening but with, in addition,tumour-like masses in the paravertebral gutters.Aspiration biopsy of these masses confirmed thatthey were due to extramedullary haematopoiesis.
Little mention has been made in the literatureto the pleura as being the site of extramedullaryhaematopoietic deposits. Brannan (1927) merelystates that myeloid activity may occur at this sitebut gives no further details. Knoblich (1960), usingBrannan (1927) as his authority, includes the pleurain his comprehensive list of possible sites for extra-medullary haematopoiesis. Pitcock et al. (1962)describing their autopsy series found diffusethickening of the pleura and peritoneum in many.They make the interesting observation that extra-medullary haematopoietic foci may present astumours, which have many of the characteristicsof intramedullary bone marrow tissue in that theycontain, together with haematopoietic tissue, vari-able amounts of fibrous tissue.More recently Lieberman, Rosvoll & Ley (1965)
describe the clinical and autopsy findings in threecases showing extramedullary myeloid tumoursout of twelve cases of myelofibrosis and myelo-sclerosis with myeloid metaplasia. In one casetumour nodules of myeloid tissue on the pleuralsurfaces, up to 1-5 cm in size, were found at post-mortem, with much larger nodules in the liver andspleen. In their third case a scalp tumour ofmyeloid tissue (at first interpreted as a reticulumcell sarcoma), was removed during life and latera 7-5 cm tumour mass in the wall of the smallintestine was excised.
It is clear that pleural involvement has beenpreviously noted at autopsy but we think that thiscase is the first in which it produced a diagnosticproblem for the clinician, radiologist and path-ologist during the life of the patient.
SummaryAn account is given of a case of myelosclerosis
with extramedullary haematopoiesis, involving thepleural surfaces. Previous reports of this phenom-enon are quoted. Other presentations of extra-medullary haematopoiesis are briefly discussed.
AcknowledgmentWe wish to thank Mr!P. S. Waldie for the illustrations.
431
copyright. on January 30, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.43.500.428 on 1 June 1967. Dow
nloaded from

432 Case reports
ReferencesAPPLEBY, A., BATSON, G.A., LASSMAN, L.P. & SIMPSON,
C.A. (1964) Spinal cord compression by extramedullaryhaematopoiesis in myelosclerosis. J. Neurol. Neurosurg.Psychiat. 27, 313.
ASK-UPMARK, E. (1945) Tumour-simulating intra-thoracicheterotopia of bone marrow, Acta radiol. (Stockh.), 26,425.
BRANNAN, D. (1927) Extramedullary hematopoiesis inanaemias. Bull. Johns Hopk. Hosp. 41 104.
CLOSE, A.S., TAIRA, Y. & CLEVELAND, D.A. (1958) Spinalcord compression due to extramedullary hematopoiesis.Ann. intern. Med. 48, 421.
CRAVEN, J.D. (1964) Renal glomerular osteodystrophy.Clin. Radiol. 15, 210.
DENT, C.E. (1955) Clinical section. Proc. roy. Soc. Med. 48,530.
DODGE, O.G. & EVANS, D. (1956) Haemopoiesis in a pre-sacral tumor (myelolipoma). J. Path. Bact. 72, 313.
FOLLIS, R.H. & JACKSON, D.A. (1943) Renal osteomalaciaand osteitis fibrosa in adults. Bull. Johns Hopk. Hosp. 72,232.
HANFORD, R.B., SCHNEIDER, G.F. & MACCARTHY, J.D.(1960) Massive thoracic extramedullary hemopoiesis.New Engl. J. Med. 263, 120.
KNOBLICH, R. (1960) Extramedullary hematopoiesis pre-senting as intrathoracic tumours. Report of a case in apatient with thalassemia minor. Cancer, 13, 462.
KORST, D.R., CLATANOFF, D.V. & SCHILLING, R.F. (1956)On myelofibrosis. Arch. intern. Med. 97, 169.
LEIBERMAN, P.H., ROSVOLL, R.V. & LEY, A.B. (1965) Extra-medullary myeloid tumors in primary myelofibrosis.Cancer, 18, 727.
LEIGH, T.F., CORLEY, C.C., Jr, HUGULEY, C.M. & ROGERS,J.V., Jr (1959) Myelofibrosis. The general and radiologicfindings in 25 proved cases. Amer. J. Roentgenol. 82, 183.
LOWMAN, R.M., BLOOR, C.M. & NEWCOMB, A.W. (1963)Thoracic extramedullary hematopoiesis. Dis. Chest. 44,154.
MALAMOS, B., PAPAVASILIOU, C. & AVRAMIS, A. (1962)Tumor-simulating intrathoracic extramedullary hemo-poiesis. Report of a case. Acta radiol. (Stockh.), 57, 227.
PITCOCK, J.A., REINHARD, E.H., JUSTUS, B.W. & MENDEL-SOHN, R.S. (1962) A clinical and pathological study of 70cases of myelofibrosis. Ann. intern. Med. 57, 73.
SEIDLER, R.C. & BECKER, J.A. (1964) Intrathoracic extra-medullary hematopoiesis. Radiology, 83, 1057.
SHANKS, S.C. & KERLEY, P. (1962) A Text-book of X-rayDiagnosis by British Authors, vol. 2, 3rd edn, p. 895.Lewis, London.
WYATT, J.P. & SOMMERS, S.C. (1950) Chronic marrow failure,myelosclerosis and extramedullary hematopoiesis. Blood,5, 329.
Neurofibromatosis with pancreatic duct obstruction and steatorrhoea
K. G. WORMSLEY W. F. W. E. LOGANM.D., M.R.C.P. M.B., M.R.C.P.
V. F. SORRELL G. C. COLEM.B.(N.Z.), F.R.C.S. M.B., Ch.B.
Manchester Royal Infirmary
INVOLVEMENT of the alimentary tract is a wellrecognized and documented manifestation ofneurofibromatosis, but there appears to be norecord of steatorrhoea complicating this disorder.We have encountered two patients in whomsteatorrhoea was due to obstruction of the pan-creatic duct by neoplastic processes attributableto this disease.
Case 1F.S., male, aged 40, was admitted to hospital
for investigation of severe diarrhoea of 1 yearsduration associated with considerable weight loss.The faeces were typically fatty.Examination revealed a cachectic anaemic man
with oedema of the feet and the typical cutaneousstigmata of neurofibromatosis.
Investigation confirmed the presence of severesteatorrhoea (Table 1). Jejunal biopsy was normalbut duodenal intubation with pancreatic stimula-tion (Burton et al., 1960) showed no appreciablepancreatic secretion although the biliary fractionwas normal. Radiological studies of the alimentarytract and gall bladder were normal. The anaemia(Hb 9-6 g/100 ml) was due to thalassemia minor(/, chain type, Hb A2 4-1%, Hb F 1-5%).Laparotomy revealed a nodule (7 mm diameter)
on the medial wall of the second part of theduodenum at the orifice of the pancreatic duct,which was obstructed 1 cm from its entry into theduodenum. The pancreas was small and atrophic.The bile duct opened into the duodenum 2 cm
proximally to the pancreatic duct. The obstructingnodule was excised. Histological examination
copyright. on January 30, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.43.500.428 on 1 June 1967. Dow
nloaded from