Embed Size (px)
Citation preview

Plenary 5 Prevention – What Are the Options for Prevention Now and in the Future?
June 25, 2016 1:30 p.m. - 3:00 p.m.
Moderators: Tom Stanton, MPP, Danny Did Foundation and Henry Smithson, M.D., University College Cork
• Family Speaker: Margaret Storey
• Seizure Monitoring and Devices - Tobias Loddenkemper, M.D., Boston Children’s Hospital
• Disclosing and Managing Risk - Jane Hanna, SUDEP Action
• Tools Not Rules for Discussing SUDEP - Jeff Buchhalter, M.D., Ph.D., FAAN, Alberta
Children’s Hospital
• Living With and Managing Epilepsy - Barbara Jobst, M.D., Dartmouth-Hitchcock Medical Center
• Panel Discussion:
Where are the gaps? Are there clear opportunities for engagement between groups on the needs that
are identified from this session? Is there a place for families and generalists to discuss the best way to provide
this information and how it can be used at an epilepsy review to reduce future personal risk?
What can families do now to engage? Are any of these interventions ready for primetime? What would be needed to get them to patients?

2015 AES Annual Meeting www.AESnet.org
1
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Plenary 5 ‐What Are the Options for Prevention Now and in the
Future?
Moderators:
Henry Smithson, MD, University College Cork
Tom Stanton, MPP, Danny Did Foundation
JUNE 2016
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Disclosures
Henry Smithson Advisor to SUDEP Action
Tom Stanton None
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Agenda
• Seizure Monitoring and DevicesTobias Loddenkemper, MD, Boston Children’s Hospital
• Disclosing and Managing RiskJane Hanna, SUDEP Action
• Tools Not Rules for Discussing SUDEPJeff Buchhalter, MD, PhD, FAAN, Alberta Children’s Hospital
• Living With and Managing EpilepsyBarbara Jobst, MD, Dartmouth‐Hitchcock Medical Center
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA
pameAESnet.org

Plenary 5 What Are the Options for Prevention
Now and in the Future?
Seizure Monitoring and Devices Tobias Loddenkemper, M.D. Boston Children’s Hospital
Slides Not Available

2015 AES Annual Meeting www.AESnet.org
1
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Disclosing and Managing Risk
Jane Hanna OBE
SUDEP Action
JUNE 2016
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Disclosure
None
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Learning Objectives
• Addressing the relationship between risk communication and potential prevention
• How urgent is this issue ?
• How can we speed up ? An examination of two case studies which illustrate two contrasting pathways to improvement ?
• References in this presentation are simplified. For full references: https://sudep.org/sudep‐action‐pame
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
A personal reflection
• “Sudden Unexpected Death in people with epilepsy was recognized in the early twentieth century along with identified risks and recommendation for its prevention; however by the 1960’s a myth had gained hold in the medical literature that epilepsy was not fatal…” (Panelli et al 2015, Nashef 1995)
• The culture has changed and will continue to do so
References in this presentation are simplified. For full references https://sudep.org/sudep‐action‐pame
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
How close are we do cracking it ?
“Educational campaigns regarding sudden infant death syndrome and fires, which kill far fewer Americans than epilepsy, have been widely implemented. We have done too little to prevent epilepsy‐related deaths”
Devinsky et al (2015)
“The majority of people with epilepsy and their families want to know about SUDEP….. If we can determine that SUDEP knowledge improved adherence and self‐management, then education may be the most accessible tool we have to impact mortality in epilepsy” Donner et al (2016)
“In response to calls for disclosure and discussion, many health professionals are unsure how to respond. This suggests that the philosophy of self‐management and informed decision‐making have not been universally adopted into epilepsy care. If this framework was in place it would be a short step to include SUDEP in usual risk communication” Panelli et al (2015)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Framework: Risk Communication
• Core information needed. Weinstein (1999):
• Identity and severity of harm;
We know that people with epilepsy are at a higher risk of fatality(SUDEP, status, accidents, drownings, suicide)
• Likelihood of harm under various circumstances
That the risk of dying increases with known (? overlapping) risk factors –generalised tonic‐clonic seizures; frequency of seizures; sleep seizures; depression (Tomson 2016)
• Possibility of reducing the harm
e.g. medications; seizure interventions, mental health interventions; safety with water (showers; supervised swimming)

2015 AES Annual Meeting www.AESnet.org
2
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
What do UK families say
An who may have to manage risky seizures
All require awareness, education and confidence
Kennelly & Riesel 2002:• 78 semi‐structured indepth telephone interviews
• <1% knew about risk of death
• 50% reported gaps in service
• Majority (68) supported tailored information on or soon after diagnosis
• Most reported trauma, devastation, guilt, anger, and loneliness
Epilepsy Deaths Register UK (March 2016)
• 527 international reports
• 251 UK semi‐structured questionnaire
• < 46% knew about risk of death
• 37% report gaps in service
https://sudep.org/sudep‐action‐pame
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Disclosure
Studies with bereaved families outside UK all supporting communication of risk
• Donner et al, Epilepsia 2016
• Ramachandran 2016 (Canada)
• Rillotta F, Seizure 2015 (Australia)
• North American SUDEP Registry (NASR) 2016
Studies with people with epilepsy also support communication of risk
“The majority of people with epilepsy and their families want to know about SUDEP” Donner et al 2016 (special supplement review)
Guidelines all support communication of risk (with significant variations)• Scotland: SIGN 2015 discussion by an appropriate `specialist’• NICE 2004 `every professional providing care` should be able to discuss
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
What hinders disclosure ?
• Many surveys and only a few audits mostly focused on SUDEP all find huge variation in individual practice. Some suggested barriers in the literature:
• Professionals with less experience of epilepsy
• Professionals with less experience in practice
• Lack of experience of SUDEP
• Fatalistic views regarding lack of any measures to prevent
• Concern about negative responses from patients
(Donner et al 2016 (expert review); Stzelczyk 2016)
• Connections between quality measures and improvements identify two contrasting pathways to change through accountability or learning and find measures are not enough. Barriers need to be tackled. These include lack of capacity among organisations and individuals acting in them. (Berwick 2003)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
How urgent is disclosure and risk management in 2016 – A UK perspective
An who may have to manage risky seizures
All require awareness, education and confidence
• 42% of epilepsy deaths annually were potentially avoidable in a national clinical audit (1/3 never saw a specialist; 41% had not been reviewed in 2 years before death; 18% cases of drug management was poor)
& <1% with recorded discussion of risk ((Hanna et al 2002)
“While there remains a critical need for more effective treatments, especially ones that affect the actual process of epileptogenesis, the UK audit emphasises that many patients with epilepsy—perhaps most—could benefit substantially if only current knowledge and available therapeutic options were applied effectively”. Pedley T,
Hauser A (2002 Lancet)
Access to report and Lancet editorial: https://sudep.org/sudep‐action‐pame
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Accountability and Learning in the aftermath of the National Clinical Audit in UK
• The Audit was powerful and continues to influence in 2016 in UK. It was a catalyst to national guidelines in 2004 which included SUDEP and also helped in case for national financial payment to GPs for annual review of people with epilepsy.
• Guidelines on communication of risk increased documented discussion of risk from less than 1% in 2002 to about 4% in a few centres that did audits/research by 2012. National survey of doctors and nurses found wide variation but issue not a priority for research funding bodies.
• Financial payment to GPs is cut in 2014. In 2015 national editorial on mortality is supported by clinical leaders in the UK Preventing premature deaths in epilepsy. General Practice is the place to start and there is much to do ? (Ridsdale 2015)
• Over this entire period 2002 to 2016 two contrasting pathways have been used to to progress disclosure and management of risk. Pathway 1 is Accountability and Pathway 2 is Learning. Both require overcoming resistance to changing status quo (Berwick 2003)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
The NHS Plan• UK studies present picture of people dying out of
contact with specialists, poor adherence, depression and risk not understood in the community (Ridsdale 2011, 2015, Shankar 2014, Sander 2016)
• Emergency admissions - 73% not getting seizure management advice (National Audit Seizures in Hospitals)
• Top 10 causes of premature deaths
What we know about the UK Problem in 2016
2015 AES Annual Meeting www.AESnet.org
3
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
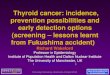
Which non‐specialists deal with risk ?
People who have seizures Family Carers
Advocates Professional carers
Emergency professionals Police
Maternity Mental health
Community Physicians Community nurses
Coroners Bereaved families
How can people at the front line try to reduce risk if they are not equipped to understand risk ?
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
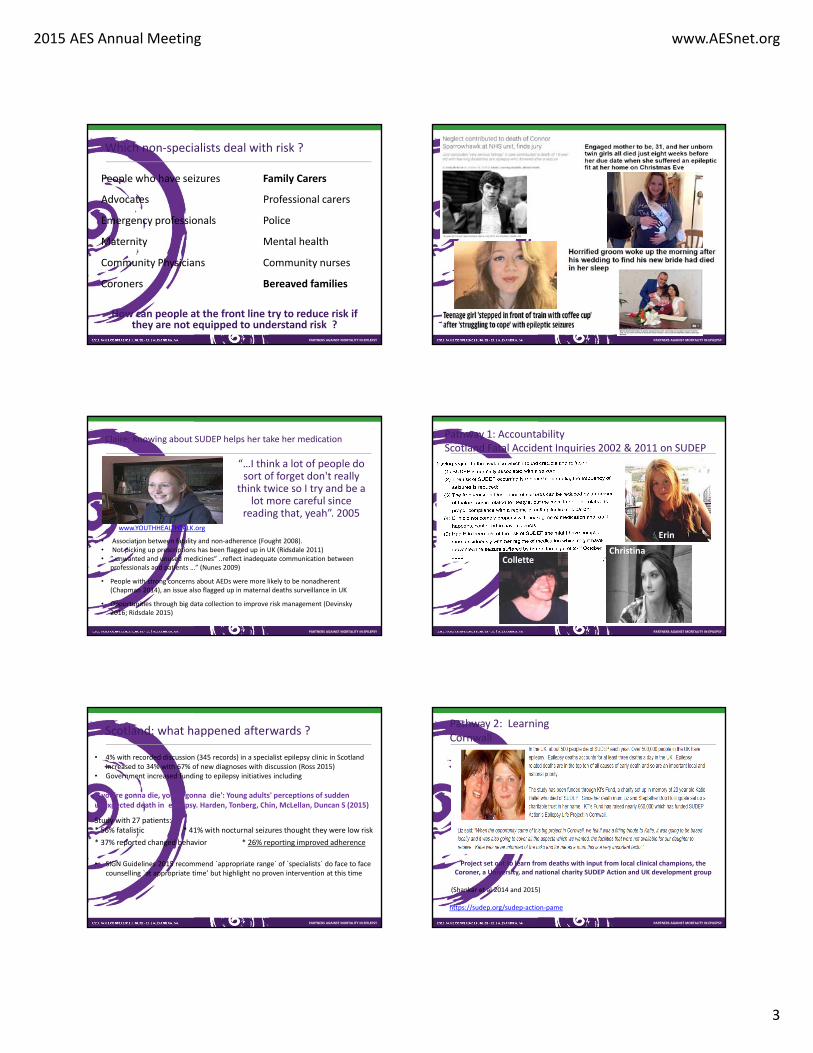
Claire: Knowing about SUDEP helps her take her medication
“…I think a lot of people do sort of forget don't really
think twice so I try and be a lot more careful since
reading that, yeah”. 2005www.YOUTHHEALTHTALK.org
• Association between fatality and non‐adherence (Fought 2008). • Not picking up prescriptions has been flagged up in UK (Ridsdale 2011)• ” unwanted and unused medicines” ..reflect inadequate communication between
professionals and patients …” (Nunes 2009)
• People with strong concerns about AEDs were more likely to be nonadherent(Chapman 2014), an issue also flagged up in maternal deaths surveillance in UK
• Opportunities through big data collection to improve risk management (Devinsky2016; Ridsdale 2015)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
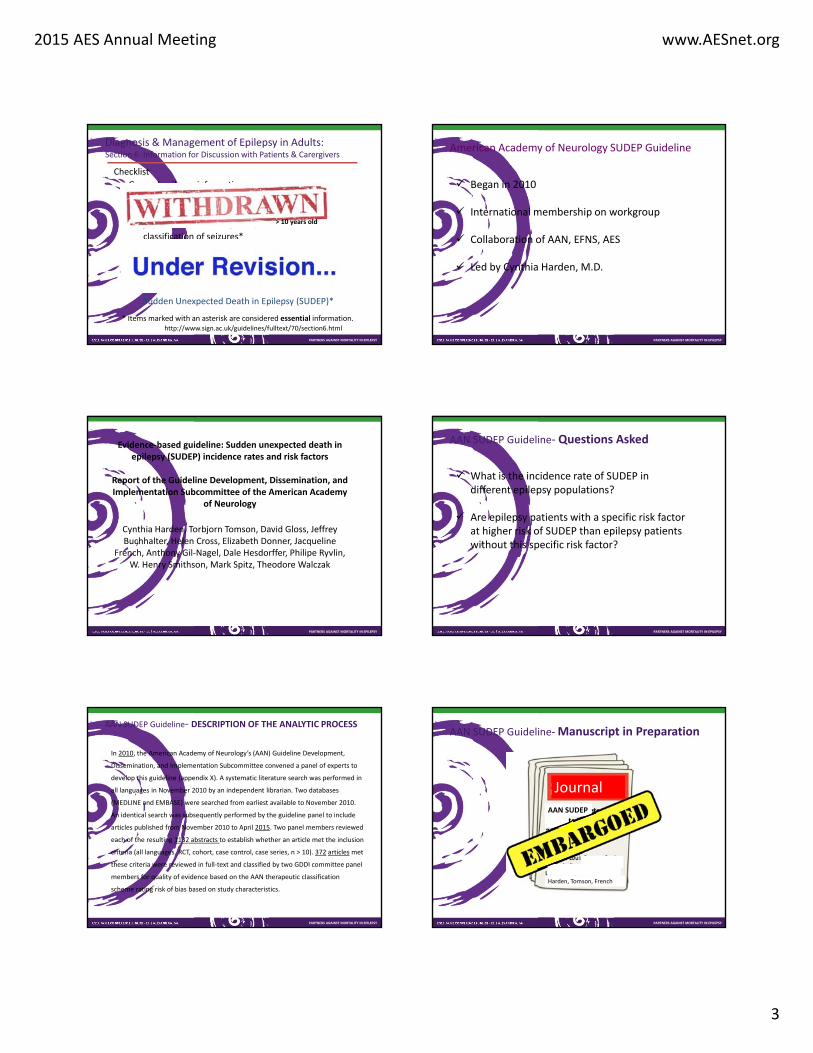
Pathway 1: Accountability Scotland Fatal Accident Inquiries 2002 & 2011 on SUDEP
Collette
Erin
Christina
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Scotland: what happened afterwards ?
• 4% with recorded discussion (345 records) in a specialist epilepsy clinic in Scotland increased to 34% with 67% of new diagnoses with discussion (Ross 2015)
• Government increased funding to epilepsy initiatives including
If you're gonna die, you're gonna die': Young adults' perceptions of sudden unexpected death in epilepsy. Harden, Tonberg, Chin, McLellan, Duncan S (2015)
Study with 27 patients:* 56% fatalistic * 41% with nocturnal seizures thought they were low risk
* 37% reported changed behavior * 26% reporting improved adherence
• SIGN Guidelines 2015 recommend `appropriate range` of `specialists` do face to face counselling `at appropriate time’ but highlight no proven intervention at this time
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Pathway 2: Learning Cornwall
Project set out to learn from deaths with input from local clinical champions, the Coroner, a University, and national charity SUDEP Action and UK development group
(Shankar et al 2014 and 2015)
https://sudep.org/sudep‐action‐pame

2015 AES Annual Meeting www.AESnet.org
4
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY 2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Cornwall
• About 1% of UK population (60 million). • 2012 local neurology service with 10% documented discussion of risk.• Stakeholders highly motivated by deaths in the community including a highly experienced
local coroner • 48 SUDEPs• Used risk factors flagged in medical literature to check against local deaths. Findings
supported generalized tonic‐clonic seizures; surveillance, increased seizure‐frequency; adherence, surveillance
• 98% positive feedback from clinicians and patients across the care pathway community and specialist adult settings
• UK development group updated to include risks of fatality found in UK surveillance from flags for other causes of epilepsy mortality from general practice population data and additional/overlapping flags for all cause mortality from the general practice research data base –seizures, missed prescriptions; depression; alcohol and national surveillance on maternal deaths (medicines adherence)
• Used in telehealth and community‐based general practice audit (Shankar 2015, 2016)• Steps to prevent SUDEP: the validity of risk factors in the SUDEP and Seizure Safety
CheckList: a case control study (Shankar 2016 Journal of Neurology June 24 2016)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
UK DevelopmentLead ‐ Dr Rohit Shankar, Consultant in Adult Developmental Neuropsychiatry, Cornwall Partnership NHS Foundation Trust
Secretariat – SUDEP Action (Hanna, Panelli and Ashby) Wantage, Oxfordshire
Development groupDr Brendan McLean, Consultant Neurologist, The Royal Cornwall Hospitals NHS Trust
Professor Mathew Walker, Professor of Neurology and Clinical Epilepsy, UCL Institute of Neurology
Professor Josemir W Sander, Professor of Neurology and Clinical Epilepsy, UCL Institute of Neurology
Dr Craig Newman, Clinical Psychologist, Plymouth University
Professor Phil Smith, President Association of British Neurologists, University Hospital of Wales
Dr John Craig, Consultant Neurologist, Belfast Health and Social Care Trust
Dr David Cox, Consultant Neuropsychiatrist Cornwall Partnership NHS Foundation Trust
Dr John‐Paul Leach, Consultant Neurologist, Southern General Hospital, Glasgow
Professor Henry Smithson, Professor of General Practice, University College Cork & University of Sheffield (Hon)
Dr Tamsyn Anderson, GP Partner and board member of NHS Kernow, NHS Kernow CCG
Professor Leone Ridsdale, Professor of Neurology & General Practice, Kings College LondonCaryn Jory, Epilepsy Specialist Nurse, Cornwall Partnership NHS Foundation Trust
Mary Parratt, Epilepsy Specialist Nurse, The Royal Cornwall Hospitals NHS Trust
Juliet Ashton, Epilepsy Specialist Nurse, Norfolk
Dr Emma Carlyon, HM Coroner, Cornwall
Simon Lees, Person with Epilepsy, Advisor with lived experience, Derby
Nathan Trevena, Person with Epilepsy, Advisor with lived experience, Cornwall
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
SUDEP and Seizure Safety Checklist
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
“A comprehensive and innovative
approach to reduce sudden death in patients with epilepsy.”
British Medical Journal Judges
Recognition as Neurology Team of the Year 2016
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Clinical early adopters

2015 AES Annual Meeting www.AESnet.org
5
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY 2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Impact on Clinical Care and Practice
• Learning model shows inclusivity and learning from deaths anddemonstrates a successful systematic approach to the challenge of disclosure and management of risk
• Community based multi‐disciplinary collaboration • Whole continuum of care • Updated by UK expert development group as new research
emerges • Validated good practice by national health bodies • Driven and adopted by professional champions in front‐line
services • Inclusive of families making alternative ways of seeking
accountability less necessary after a death• Standardised tools to support professionals • Using technology to speed up change. • Development group will be informed by engagement with adopters • Can work alongside all other initiatives and measures to tackle
mortality
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA
pameAESnet.org

2015 AES Annual Meeting www.AESnet.org
1
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Tools Not Rules for Discussing SUDEP (The role of guidelines)
JUNE 2016
• Jeffrey R. Buchhalter MD, PhD
• Section of Pediatric Neurology• Alberta Children’s Hospital
• University of Calgary
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Disclosures
American Academy of Neurology‐ speaker
Eisai, Ltd‐ consultant
Upsher‐Smith, Labs‐ consultant
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Learning Objectives
Following participation in this activity, learners should
be able to understand:
Definition of clinical practice guidelines
Current status of SUDEP guidelines & relationship to
other epilepsy guidelines
Unintended consequences of guidelines
Evidence that adherence to guidelines can improve
outcomes
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
What is a Clinical Practice Guideline?
Clinical practice guidelines are statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options. Jun 1, 2014
https://www.guideline.gov/about/inclusion‐criteria.aspx
The U.S. Congress, through the Medicare Improvements for Patients and Providers Act of 2008, asked the IOM to undertake a study on the best methods used in developing clinical practice guidelines. The IOM developed eight standards for developing rigorous, trustworthy clinical practice guidelines. 2011
http://www.nationalacademies.org/hmd/Reports/2011/Clinical‐Practice‐Guidelines‐We‐Can‐Trust.aspx
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
National Institute for Clinical Excellence
The Epilepsies, 2004; Clinical Guideline 20
1.3.1 Information‐ “… should be given and have access to sources of information about (where appropriate): SUDEP (16 on list of 20)
1.3.11 SUDEP
Include in literature relating to seizure control
Tailored discussion re: relative risk
Refer to support groups for those affected
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Epilepsies: diagnosis and management:
NICE guidelines [CG137]
Published date: January 2012 Last updated: February 2016

2015 AES Annual Meeting www.AESnet.org
2
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
NICE 2012 NICE clinical guideline 137
1.3 Information
1.3.1 Children, young people and adults with epilepsy and their families and/or
carers should be given, and have access to sources of, information about
(where appropriate):
epilepsy in general
diagnosis and treatment options
medication and side effects
seizure type(s), triggers and seizure control
management and self‐care
risk management
first aid, safety and injury prevention at home and at school or work
psychological issues
social security benefits and social services
insurance issues
education and healthcare at school
employment and independent living for adults
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
road safety and driving
prognosis
sudden death in epilepsy (SUDEP)
status epilepticus
lifestyle, leisure and social issues (including recreational drugs, alcohol, sexual activity and
sleep deprivation)
family planning and pregnancy
voluntary organisations, such as support groups and charitable organisations, and
how to contact them. [2004]
https://www.nice.org.uk/guidance/cg137/ifp/chapter/sudden‐unexpected‐death‐in‐epilepsy‐sudep
NICE 2012 NICE clinical guideline 137
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
1.3.2 The time at which this information should be given will depend on the certainty
of the diagnosis, and the need for confirmatory investigations. [2004]
1.3.3 Information should be provided in formats, languages and ways that are suited
to the child, young person or adult's requirements. Consideration should be
given to developmental age, gender, culture and stage of life of the person. [2004]
1.3.4 If children, young people and adults, and their families and/or carers, have not
already found high‐quality information from voluntary organisations and other
sources, healthcare professionals should inform them of different sources
(using the Internet, if appropriate: see, for example, the website of the Joint
Epilepsy Council of the UK and Ireland, www.jointepilepsycouncil.org.uk). [2004]
1.3.5 Adequate time should be set aside in the consultation to provide information,
which should be revisited on subsequent consultations. [2004]
https://www.nice.org.uk/guidance/cg137/ifp/chapter/sudden‐unexpected‐death‐in‐epilepsy‐sudep
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Sudden unexpected death in epilepsy (SUDEP)
1.3.11 Information on SUDEP should be included in literature on epilepsy to show why preventing seizures is important. Tailored information on the person's relative risk of SUDEP should be part of the counselling checklist for children, young people and adults with epilepsy and their families and/or carers. [2004]
1.3.12 The risk of SUDEP can be minimised by:• optimising seizure control• being aware of the potential consequences of nocturnal seizures. [2004]
1.3.13 Tailored information and discussion between the child, young person or adult with epilepsy, their family and/or carers (as appropriate) and healthcare professionals should take account of the small but definite risk of SUDEP. [2004]
1.3.14 Where families and/or carers have been affected by SUDEP, healthcare professionals should contact families and/or carers to offer their condolences, invite them to discuss the death, and offer referral to bereavement counselling and a SUDEP support group. [2004]
https://www.nice.org.uk/guidance/cg137/ifp/chapter/sudden‐unexpected‐death‐in‐epilepsy‐sudep
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Diagnosis & Management of Epilepsy in Children & Young People, A national clinical guideline
4.2.2 DEATH IN EPILEPSYThere is no general consensus on when the risk of SUDEP or other causes of premature death should be discussed with families, but it may be appropriate to discuss this issue with parents of children with symptomatic epilepsies or drug resistant epilepsies with tonic‐clonic seizures.
D. Families should be advised if the child has an increased risk of SUDEP. They can be reassured if the risk is considered to be low.Scottish Intercollegiate Guideline Network, March 2005, pg 14
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Diagnosis & Management of Epilepsy in Adults:Section 6: Information for Discussion with Patients & Carergivers
Checklist
General epilepsy information
explanation of what epilepsy is*
probable cause
explanation of investigative procedures
classification of seizures*
syndrome
epidemiology
prognosis*
genetics
Sudden Unexpected Death in Epilepsy (SUDEP)*
http://www.sign.ac.uk/guidelines/fulltext/70/section6.html
* Items marked with an asterisk are considered essential information.
2015 AES Annual Meeting www.AESnet.org
3
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Diagnosis & Management of Epilepsy in Adults:Section 6: Information for Discussion with Patients & Carergivers
Checklist
General epilepsy information
explanation of what epilepsy is*
probable cause
explanation of investigative procedures
classification of seizures*
syndrome
epidemiology
prognosis*
genetics
Sudden Unexpected Death in Epilepsy (SUDEP)*
http://www.sign.ac.uk/guidelines/fulltext/70/section6.html
* Items marked with an asterisk are considered essential information.
> 10 years old
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Began in 2010
International membership on workgroup
Collaboration of AAN, EFNS, AES
Led by Cynthia Harden, M.D.
American Academy of Neurology SUDEP Guideline
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Evidence‐based guideline: Sudden unexpected death in epilepsy (SUDEP) incidence rates and risk factors
Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy
of Neurology
Cynthia Harden, Torbjorn Tomson, David Gloss, Jeffrey Buchhalter, Helen Cross, Elizabeth Donner, Jacqueline
French, Anthony Gil‐Nagel, Dale Hesdorffer, Philipe Ryvlin, W. Henry Smithson, Mark Spitz, Theodore Walczak
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
What is the incidence rate of SUDEP in different epilepsy populations?
Are epilepsy patients with a specific risk factor at higher risk of SUDEP than epilepsy patients without this specific risk factor?
AAN SUDEP Guideline‐ Questions Asked
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
In 2010, the American Academy of Neurology’s (AAN) Guideline Development,
Dissemination, and Implementation Subcommittee convened a panel of experts to
develop this guideline (appendix X). A systematic literature search was performed in
all languages in November 2010 by an independent librarian. Two databases
(MEDLINE and EMBASE) were searched from earliest available to November 2010.
An identical search was subsequently performed by the guideline panel to include
articles published from November 2010 to April 2015. Two panel members reviewed
each of the resulting 1132 abstracts to establish whether an article met the inclusion
criteria (all languages, RCT, cohort, case control, case series, n > 10). 372 articles met
these criteria were reviewed in full‐text and classified by two GDDI committee panel
members for quality of evidence based on the AAN therapeutic classification
scheme rating risk of bias based on study characteristics.
AAN SUDEP Guideline‐ DESCRIPTION OF THE ANALYTIC PROCESS
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
AAN SUDEP Guideline‐Manuscript in Preparation
JournalAAN SUDEP
Harden, Tomson, French
2015 AES Annual Meeting www.AESnet.org
4
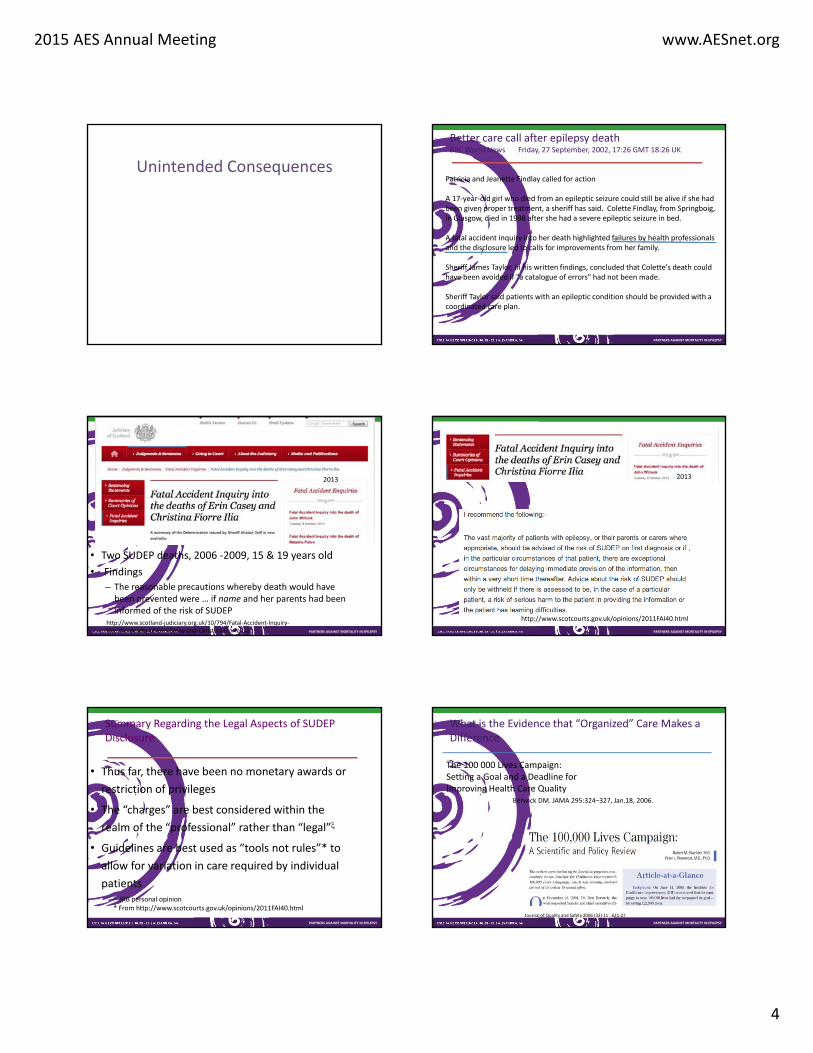
Unintended Consequences
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Better care call after epilepsy deathBBC World News Friday, 27 September, 2002, 17:26 GMT 18:26 UK
Patricia and Jeanette Findlay called for action
A 17‐year‐old girl who died from an epileptic seizure could still be alive if she had been given proper treatment, a sheriff has said. Colette Findlay, from Springboig, in Glasgow, died in 1998 after she had a severe epileptic seizure in bed.
A fatal accident inquiry into her death highlighted failures by health professionals and the disclosure led to calls for improvements from her family.
Sheriff James Taylor, in his written findings, concluded that Colette's death could have been avoided if "a catalogue of errors" had not been made.
Sheriff Taylor said patients with an epileptic condition should be provided with a coordinated care plan.
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
• Two SUDEP deaths, 2006 ‐2009, 15 & 19 years old
• Findings
– The reasonable precautions whereby death would have been prevented were … if name and her parents had been informed of the risk of SUDEP
http://www.scotland‐judiciary.org.uk/10/794/Fatal‐Accident‐Inquiry‐into‐the‐deaths‐of‐Erin‐Casey‐and‐Christina‐Fiorre‐Ilia
2013
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
http://www.scotcourts.gov.uk/opinions/2011FAI40.html
2013
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Summary Regarding the Legal Aspects of SUDEP Disclosure
• Thus far, there have been no monetary awards or
restriction of privileges
• The “charges” are best considered within the
realm of the “professional” rather than “legal”
• Guidelines are best used as “tools not rules”* to
allow for variation in care required by individual
patients JRB personal opinion* From http://www.scotcourts.gov.uk/opinions/2011FAI40.html
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
What is the Evidence that “Organized” Care Makes a Difference
Journal of Quality and Safety 2006 (32) 11 , 621‐27
The 100 000 Lives Campaign: Setting a Goal and a Deadline for Improving Health Care Quality
Berwick DM. JAMA 295:324–327, Jan.18, 2006.
2015 AES Annual Meeting www.AESnet.org
5
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
More Evidence
N = 15,000 2 yrs Mortality
reduced 6.2% 930 people
34/36 articles reduced morbidity or mortality
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
How Long Will It Take? J Noebels (PAME 2016)
Knowledge
Guidelines
Implementation
ADVOCACY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Impact on Clinical Care and Practice
Guideline(s) provide an evidence‐based framework
for discussing SUDEP with patients, families and
caregivers
Providing information regarding risk factors will
hopefully result in behaviors that lower the risk of
SUDEP occurring
Providing an opportunity for advocacy to advance
care2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA
pameAESnet.org

2015 AES Annual Meeting www.AESnet.org
1
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Living with and Managing Epilepsy
Barbara C. Jobst, MDProfessor of Neurology
Dartmouth‐Hitchcock Epilepsy Center
Geisel School of Medicine at Dartmouth
Principle Investigator “Managing Epilepsy Well Network” (MEW)
JUNE 2016
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Disclosure
Neuropace, Inc.Defense Advance Research Agency (DARPA)Center of Disease Control
Research, ConsultingResearch
Research
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Learning Objectives
Following participation in this activity, learners should be able to:• Emphasize the importance of self‐management• Educate about self‐management programs in epilepsy• Be knowledegable about the importance of depression and
cognitive problems in epilepsy • Be knowledgeable how to treat epilepsy related depression
and memory
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Barriers to a life with epilepsy
Patients‘ worries1. Unexpected seizures2. Driving3. Memory4. Overall seizure control5. Burden to family6. Future7. Injury during seizures8. Medication Side effects9. Keeping a job10. Mood11. Having to take medication12. Not being able to do things alone
Doctors’ worries1. Unexpected seizures2. Overall seizure control3. Driving4. Medication side effects5. Injury during seizures 6. Having to take medications7. Burden on family8. Future 9. Medical Costs10. Keeping a job11. Embarrassment of having seizures12. Memory
McAuley, 2010
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Self‐management
2012 Institute of Medicine Report on the public health dimensions of epilepsy:Need for self‐management programs and research
From KYOH: Know your own health, UK
“Self‐care”
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Self‐management in Epilepsy‐ Some facts
Can be measured with Adult Epilepsy Self‐Management Measurement Instrument (AESMMI) (Escoffery et al. 2015)
• Females reported higher scores for medication management and information seeking.
• White had higher scores for treatment seeking behaviors. • Higher education levels predicted more information seeking and
safety behaviors.• Higher incomes correlated with information seeking, wellness,
information, symptom and treatment behaviors.• Patient with more years of epilepsy reported more stigma
management behaviors. • Increased seizure frequency correlated with lower lifestyle,
treatment and symptom management.
2015 AES Annual Meeting www.AESnet.org
2
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
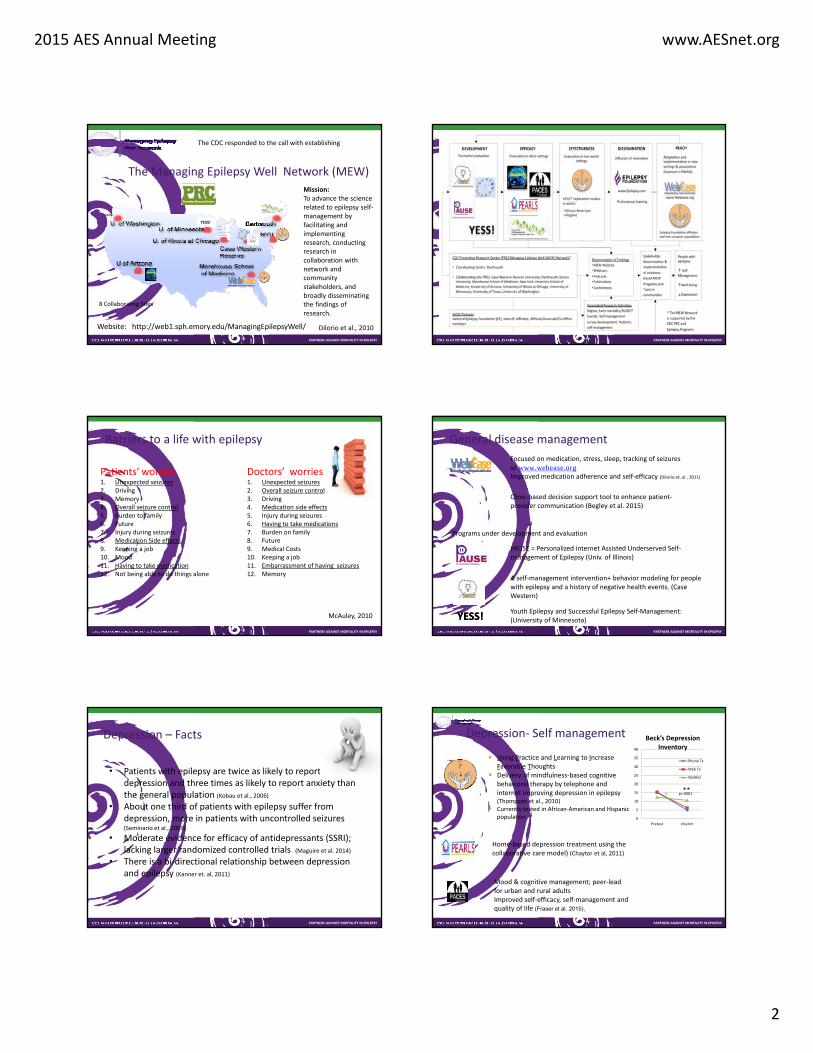
The Managing Epilepsy Well Network (MEW)
YESS!
Website: http://web1.sph.emory.edu/ManagingEpilepsyWell/
8 Collaborating Sites
Mission: To advance the science related to epilepsy self‐management by facilitating and implementing research, conducting research in collaboration with network and community stakeholders, and broadly disseminating the findings of research.
The CDC responded to the call with establishing
Dilorio et al., 2010
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Barriers to a life with epilepsy
Patients‘ worries1. Unexpected seizures2. Driving3. Memory4. Overall seizure control5. Burden to family6. Future7. Injury during seizures8. Medication Side effects9. Keeping a job10. Mood11. Having to take medication12. Not being able to do things alone
Doctors’ worries1. Unexpected seizures2. Overall seizure control3. Driving4. Medication side effects5. Injury during seizures 6. Having to take medications7. Burden on family8. Future 9. Medical Costs10. Keeping a job11. Embarrassment of having seizures12. Memory
McAuley, 2010
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
General disease management
Focused on medication, stress, sleep, tracking of seizuresat www.webease.orgImproved medication adherence and self‐efficacy (Dilorio et. al , 2011)
Clinic‐based decision support tool to enhance patient‐provider communication (Begley et al. 2015)
Programs under development and evaluation
PAUSE = Personalized internet Assisted Underserved Self‐management of Epilepsy (Univ. of Illinois)
A self‐management intervention+ behavior modeling for people with epilepsy and a history of negative health events. (Case Western)
YESS!YESS!Youth Epilepsy and Successful Epilepsy Self‐Management:(University of Minnesota)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Depression – Facts
• Patients with epilepsy are twice as likely to report depression and three times as likely to report anxiety than the general population (Kobau et al., 2006)
• About one third of patients with epilepsy suffer from depression, more in patients with uncontrolled seizures (Seminario et al., 2009)
• Moderate evidence for efficacy of antidepressants (SSRI); lacking larger randomized controlled trials (Maguire et al. 2014)
• There is a bi‐directional relationship between depression and epilepsy (Kanner et. al, 2011)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Depression‐ Self management
Using Practice and Learning to Increase Favorable Thoughts
Delivery of mindfulness‐based cognitive behavioral therapy by telephone and internet improving depression in epilepsy (Thompson et al., 2010)
Currently tested in African‐American and Hispanic population
Mood & cognitive management; peer‐lead for urban and rural adults Improved self‐efficacy, self‐management and quality of life (Fraser et al. 2015),
0
5
10
15
20
25
30
35
40
Pretest Interim
Beck’s Depression Inventory
Phone Tx
Web Tx
Waitlist
p=.0001**
Home‐based depression treatment using the collaborative care model) (Chaytor et al, 2011)

2015 AES Annual Meeting www.AESnet.org
3
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Barriers to a life with epilepsy
Patients‘ worries1. Unexpected seizures2. Driving3. Memory4. Overall seizure control5. Burden to family6. Future7. Injury during seizures8. Medication Side effects9. Keeping a job10. Mood11. Having to take medication12. Not being able to do things alone
Doctors’ worries1. Unexpected seizures2. Overall seizure control3. Driving4. Medication side effects5. Injury during seizures 6. Having to take medications7. Burden on family8. Future 9. Medical Costs10. Keeping a job11. Embarrassment of having seizures12. Memory
McAuley, 2010
????
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Memory‐ Facts
• 82% of patient with drug‐resistant temporal lobe epilepsy cognitive problems in at least one domain (memory, language, executive function), 21% in all three domains (Rai et al., 2015)
• Children have a similar rate of impairment (Menlove et al. , 2015)
• Not dependent on seizure frequency (Pacagnella et al. 2015)Verydepressed
Goodmemory
Jobst et al., 2011
• Little correlation between subjective and objective memory unless related to word finding difficulties (p<0.001) or depression (p<0.05) (Sawrie et al. 1999)
• Patients rate memory difficulties more bothersome than seizures (Escoffery et al. 2015)
• Depression and memory are correlated• AED have an influence (Escoffery et al. 2015, Sawrie et. al,
1999)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
• Education about memory problems
• Program delivered for the phone
• Memory coach guides problem solving therapy for memory problems
• Domains: Disease related skills, organizational skills, social skills
• Patient comes up with own solution for problem and exercises it until the next phone call
• Education about memory strategiesCaller et. al., 2013, 2015
Measure
Quality of Life Qolie‐31 p=0.05
Cognition incl. memory RBANS p=0.009
Attention subscore P=0.005
Depression PHQ9 NS
NDDI‐E NS
Executive function BRIEF‐A NS
Now being distributed to a larger population in different centers (HOBSCOTCH 2) and evaluated for cost‐effectiveness
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Weight and Diet‐ Facts
• AEDs influence weight (Ben‐Menachem, 2007)
• Ketogenic diet is an effective treatment of epilepsy, mainly in pediatric epilepsy: 38‐67% have > 50% seizure reduction (Martin, 2016)
• Adverse Events: Non‐adherence leads to treatment failure, GI‐symptoms, weight loss (Kossoff et. a; 2007)
• Ketogenic diet also effective for adults but difficult to follow (Nei et al. 2004)
• Modified diets such as Atkins diet, modified Atkins diet are also effective but dependent on Carbohydrate content (Kossoffet al., 2003)
• Ketogenic diet may improve cognition and mood‐disturbed behavior (Iff et al. 2016)
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Other important issues
• Employment• Driving• Relationships• Education• Socio‐economic Status• Reproduction• Stigma

2015 AES Annual Meeting www.AESnet.org
4
The need for evidence
Reported improvement in working memory
And reimbursement venues for evidence‐based cognitive behavioral therapies and self‐management
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
Impact on Clinical Care and Practice
• First point• Consider depression in epilepsy• Address memory problems in epilepsy
• Second point• Consider supporting self‐management for patients in form
of self‐management programs• Discuss dietary options
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA PARTNERS AGAINST MORTALITY IN EPILEPSY
2016 PAME CONFERENCE JUNE 23 ‐ 26 | ALEXANDRIA, VA
pameAESnet.org