Embed Size (px)
Citation preview
Play therapy and Expressive Art: An Ethical Approach to Building Resilience and Post-Traumatic Growth in Children of Refugee
StatusTLPCA/TNAMFT Conference 2018
Dr. Anna EdgestonMarisol Rosas-Biser
Kate Worley Lydia Yau
Suzanne Blackwood
Objectives• Following this presentation, participates will be able
to:– understand how the Adverse Childhood Experiences
(ACEs) study provides a basis of understanding the trauma and challenges experienced by children of refugee status;
– discuss play therapy techniques and interventions, specifically child-centered approaches and trauma informed techniques;
– identify and navigate through ethical challenges when counseling children of refugee status.
Background Information
Marisol Rosas-Biser
Internally Displaced: Defined• An internally displaced person (IDP) is someone who is
forced to flee his or her home but who remains within his or her country's borders.
Asylum Seeker: Defined• An asylee is a person who meets the definition of refugee and
is already present in the United States or is seeking admission at a port of entry. Refugees are required to apply for Lawful Permanent Resident (“green card”) status one year after being admitted, and asylees may apply for green card status one year after their grant of asylum.
Refugee: Defined• According to the U.S. Department of Homeland Security:
– A refugee is a person outside his or her country of nationality who is unable or unwilling to return to his or her country of nationality because of persecution or a well-founded fear of persecution on account of race, religion, nationality, membership in a particular social group, or political opinion.
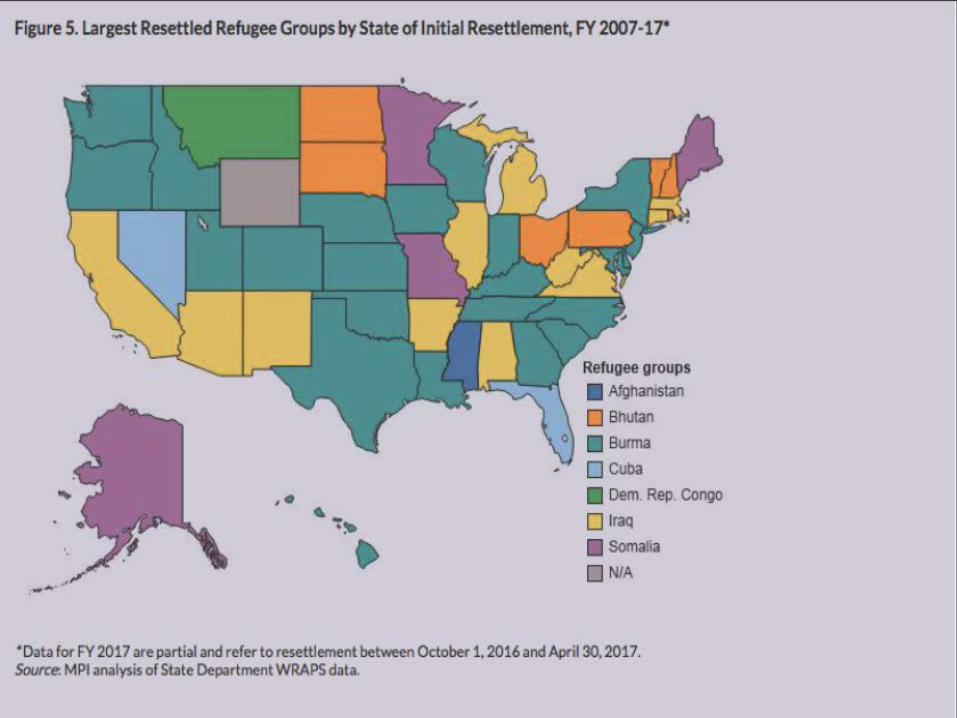
Refugees: Statistics• At the end of 2016, the estimated refugee population worldwide
stood at 22.5 million, with 17.2 million under the mandate of the United Nations High Commissioner for Refugees (UNHCR). This represents an increase of 1.1 million refugees under UNHCR mandate in one year.
• Over 90% of refugees referred for resettlement were referred to USA, Australia, and Canada.
• The USA leads the world in providing humanitarian aid to crises overseas and also accepts more refugees for resettlement through the UNHCR than any other country.
• In 2015, 64% of UNHCR-referred refugees who were resettled, were resettled in the USA.
(Bureau of Population, Refugees, and Migration, 2017)
During the 2016 commemoration of World Refugee Day, the former U.S. president (Barack Obama) said:– “This year’s commemoration comes as the UN High
Commissioner for Refugees reports that more people are displaced by rising violence, insecurity, and persecution than at any time on record. More than 65 million people around the world – more than the population of France, or California and Texas combined – have been driven from their homes. More than half are children. The scale of this human suffering is almost unimaginable; the need for the world to respond is beyond question.”
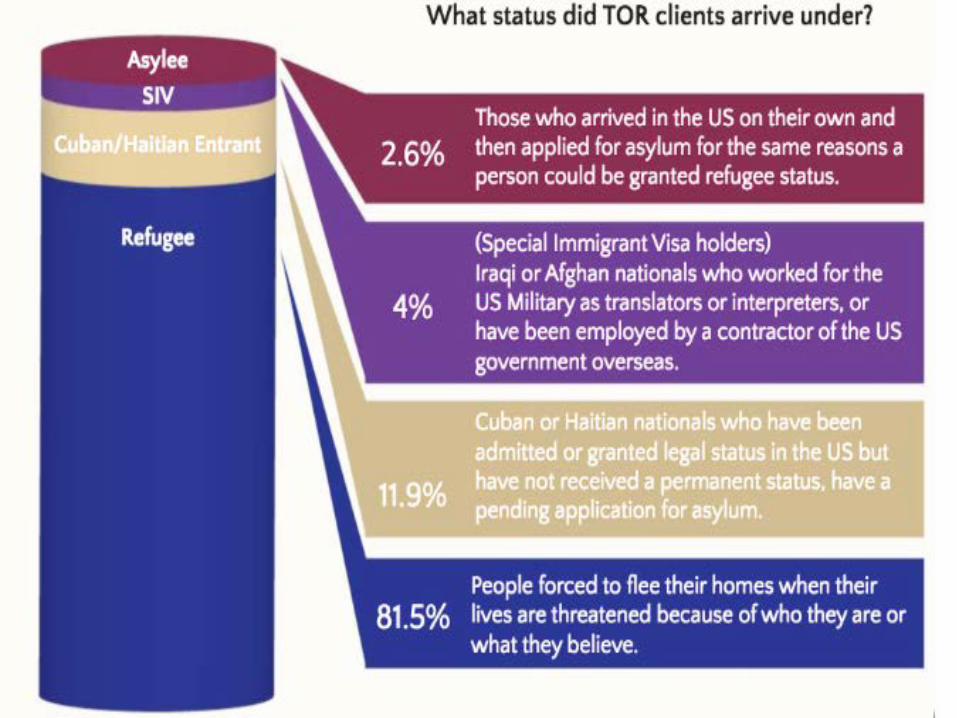
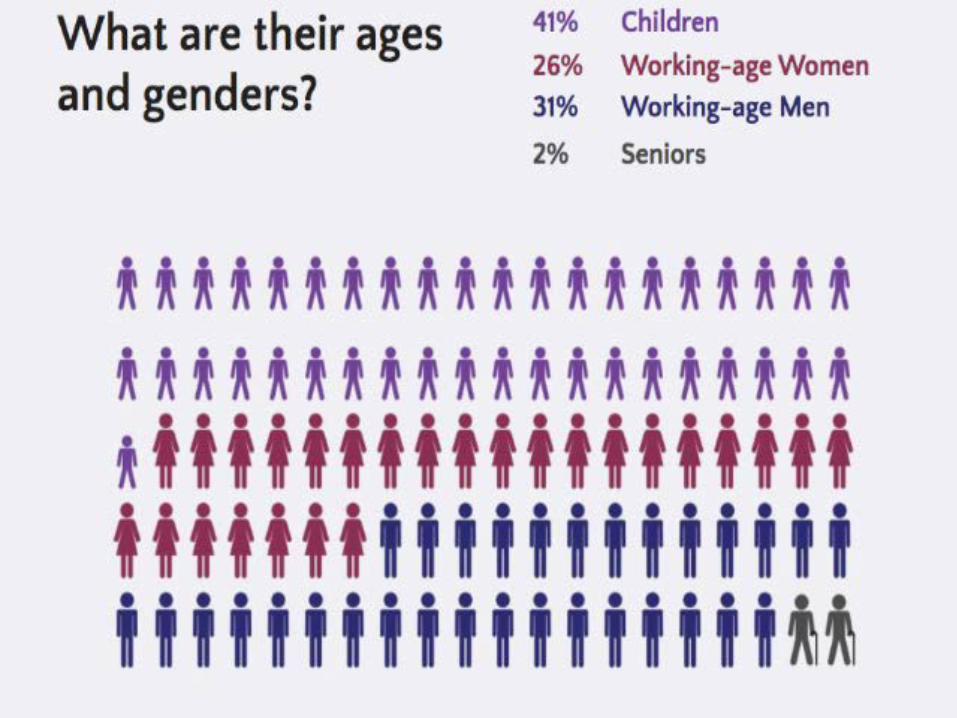
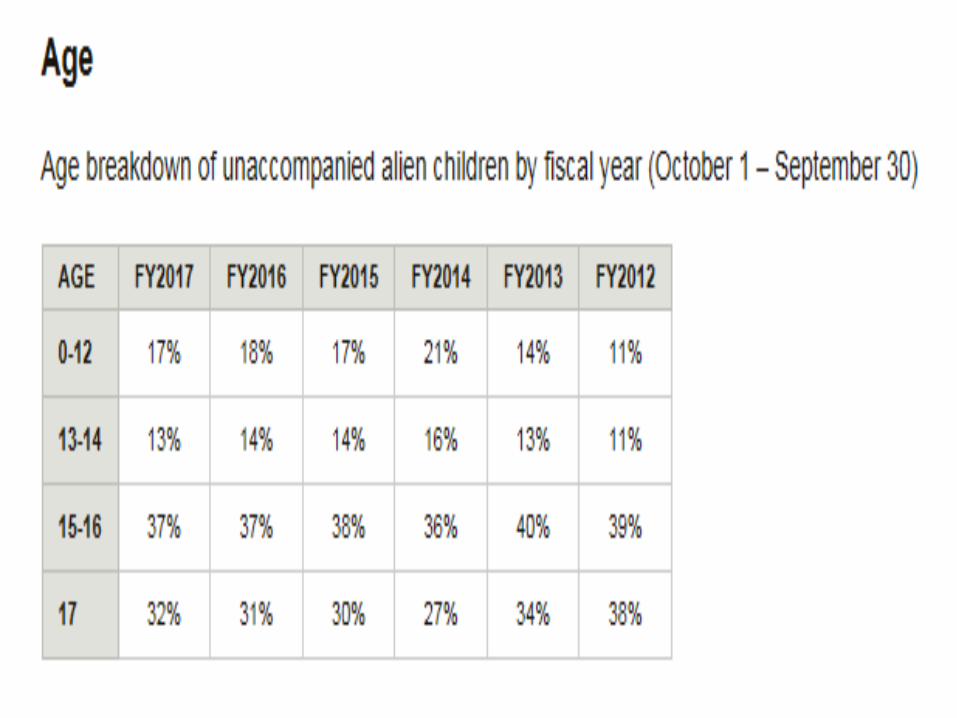
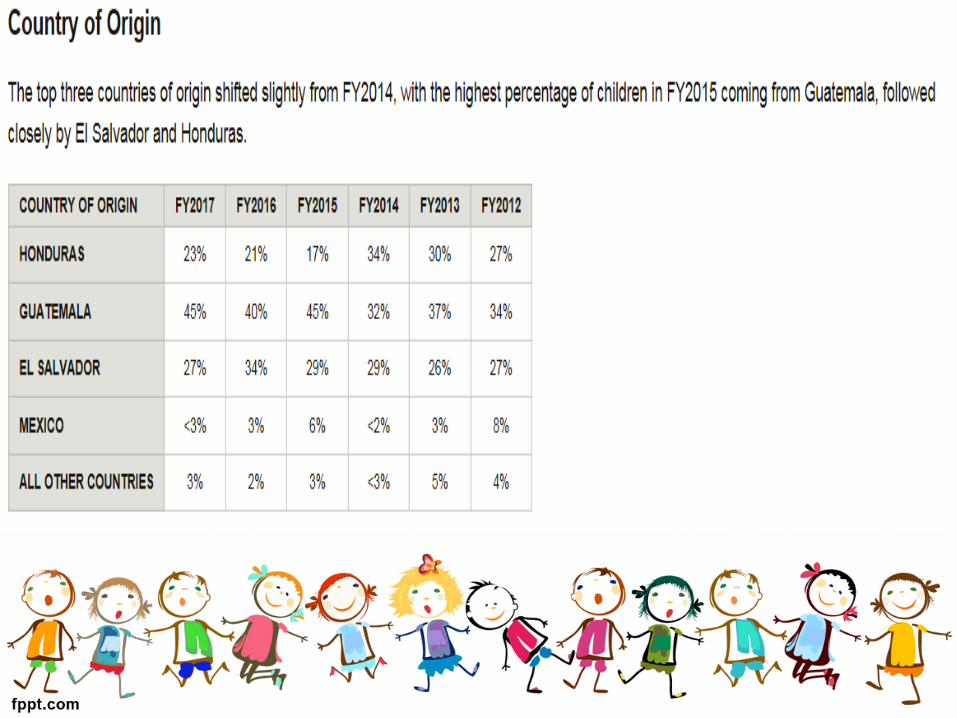
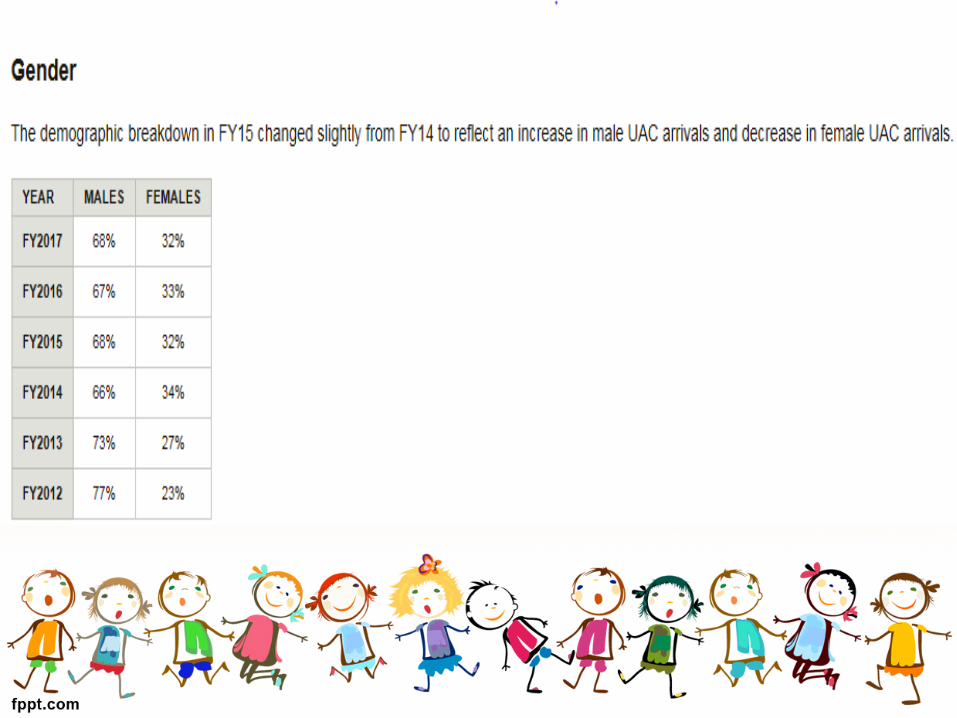
Tennessee Office for Refugees 2016 statistics
The Office of Refugee Resettlement and Office of the Administration for Children &
Families provided the following report about unaccompanied minors:
Children of Refugee Statusand Trauma
Anna Edgeston
Adverse Childhood Experiences (ACEs)
“Childhood experiences, both positive and negative, have a tremendous impact on future violence victimization and perpetration, and lifelong health and opportunity. As such, early experiences are an important public health issue. Much of the foundational research in this area has been referred to as Adverse Childhood Experiences (ACEs)”.
(CDC, 2016, para. 1)
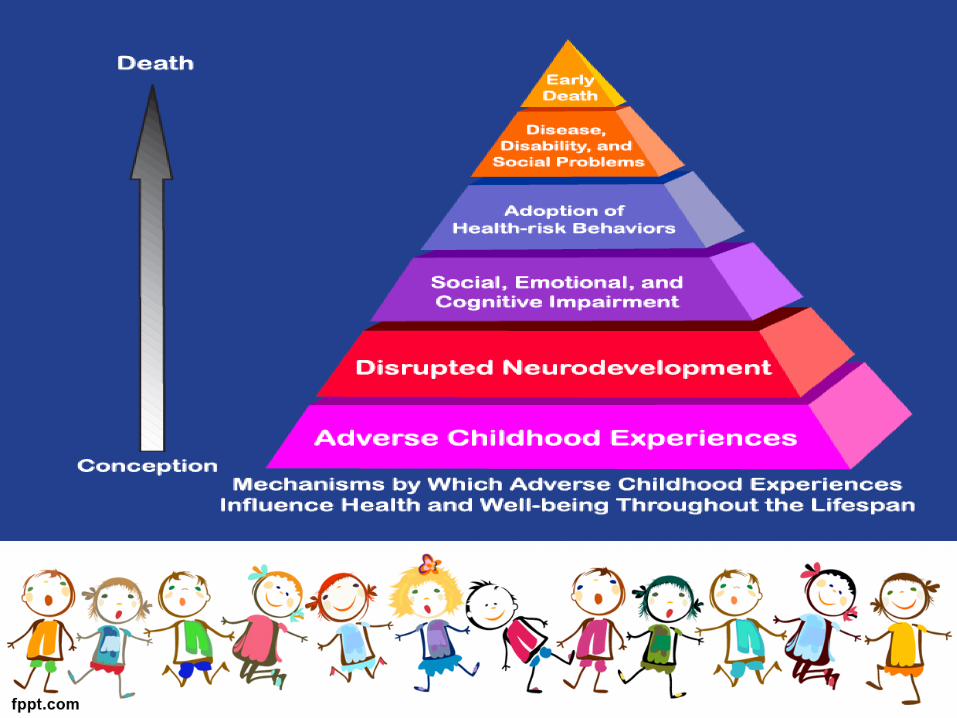
ACEs Cont…• Adverse Childhood Experiences have been
linked to– risky health behaviors,– chronic health conditions,– low life potential, and– early death.
• As the number of ACEs increases, so does the risk for these outcomes.
(CDC, 2016)
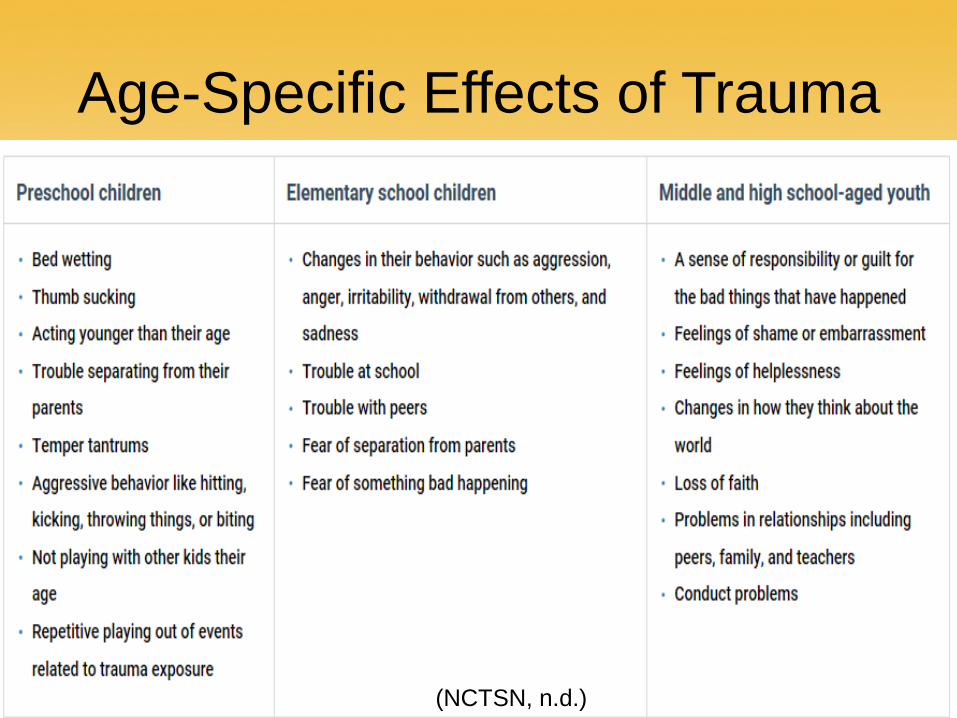
Age-Specific Effects of Trauma
(NCTSN, n.d.)
Unique Stressors Experienced by Children of Refugee Status
• Traumatic Stress• Acculturation Stress• Resettlement Stress• Isolation
(NCTSN, n.d.)
Unique Traumatic Experiences• Violence (as witnesses, victims,
and/or perpetrators)• War• Lack of food, water, and shelter• Physical injuries, infections, and
diseases• Torture• Forced labor• Sexual assault• Lack of medical care• Loss of loved ones
• Disruption in or lack of access to schooling
• Living in refugee camps• Separation from family• Loss of community• Uncertainty about the future• Harassment by local
authorities• Traveling long distances by
foot• Detention
(NCTSN, n.d.)
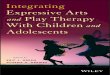
Posttraumatic Growth and Resilience
• “Adverse experiences and other trauma in childhood, however, do not dictate the future of the child. Children survive and even thrive despite the trauma in their lives”.
(American Academy of Pediatrics, 2014, p. 4).
Child-Centered Approach:Play Therapy
Kate Worley
Play Therapy“A form of counseling or psychotherapy in which play is used as means of helping both children & adults express
or communicate their feelings.”
Child-Centered Play Therapy• The creation of a warm, friendly relationship with the client. • Accept the child as he/she is. • A feeling of permissiveness is established.• The therapist is aware of the child’s expression of feelings
and is able to reflect those feelings. • The therapist recognizes that the client has the ability to solve
his/her own problems. • Therapy is child-led.• The therapeutic process is not rushed.• The therapist only establishes limits that are necessary.
(Axline, 1947)
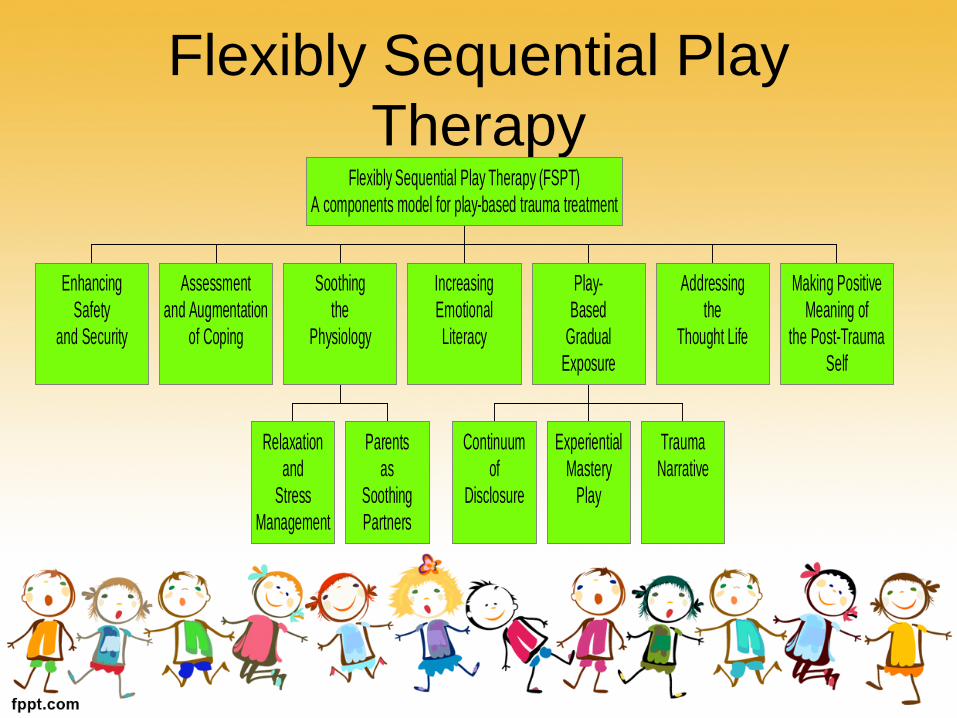
Flexibly Sequential Play Therapy
EnhancingSafety
and Security
Assessmentand Augmentation
of Coping
Relaxationand
StressManagement
Parentsas
SoothingPartners
Soothingthe
Physiology
IncreasingEmotionalLiteracy
Continuumof
Disclosure
ExperientialMastery
Play
TraumaNarrative
Play-Based
GradualExposure
Addressingthe
Thought Life
Making PositiveMeaning of
the Post-TraumaSelf
Flexibly Sequential Play Therapy (FSPT)A components model for play-based trauma treatment
Dynamic Posttraumatic Play• Non-directive and directive techniques are effective in
this type of play therapy. • Dynamic posttraumatic play is characterized by the client
feeling in control of the play outcome, the play ending with resolution, negative affect being expressed in an uninhibited manner, and when a cognitive reworking of the event occurs.
• Children are able to heal through this type of play. (Gil, 2017)
Play Disruptions• A “dyadic dance” in which the child moves towards and
away from trauma content.• Play disruptions occur when a child abruptly shifts away
from dynamic posttraumatic play either physically or emotionally.
• An attuned clinician responds to the child’s need by moving away, as well.
(Goodyear-Brown, 2010)

Experiential Activity

Child-Centered Approach: Sandtray Therapy
Lydia Yau
Sandplay Therapy
• Sandplay was developed by Dora Kalff in Switzerland and influenced by Carl Jung, a personal friend.

Sandplay Therapy: Overview
https://www.youtube.com/watch?v=BTlKJ-7JDrI&feature=youtu.be
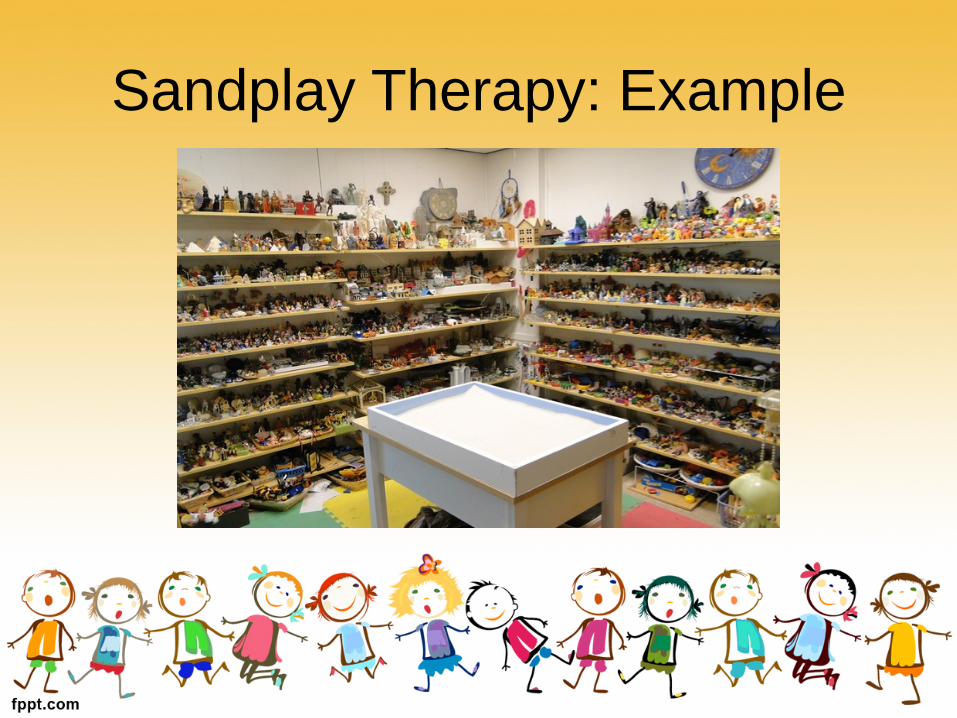
Sandplay Therapy: Example
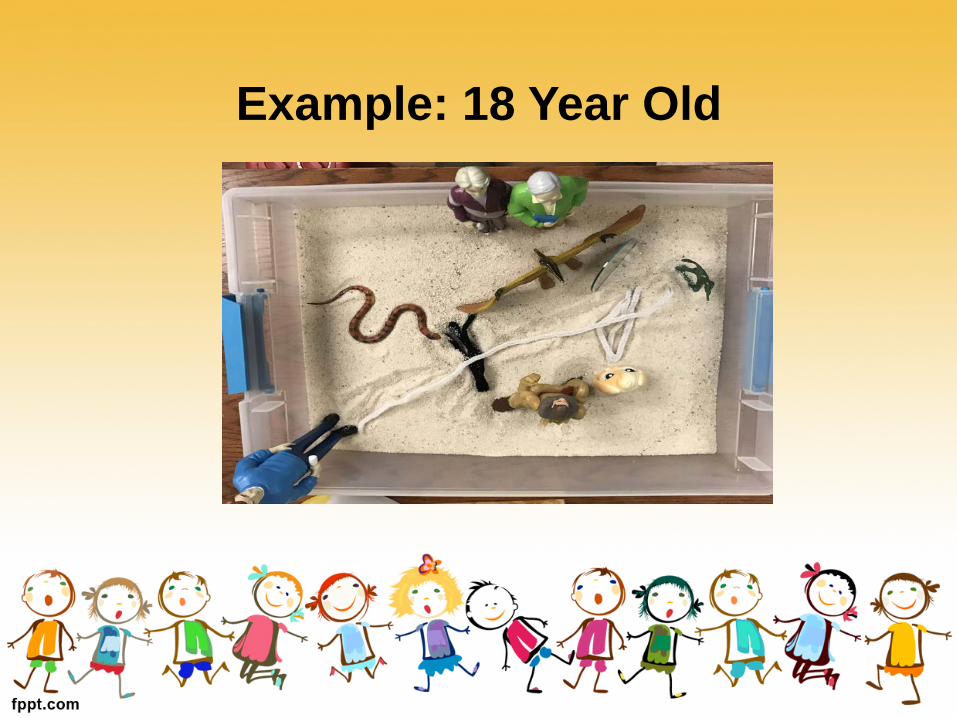
Example: 18 Year Old
“Often the hands will solve a mystery that the intellect has struggled with in vain” “...it is not only possible but fairly probable, even, that psyche and matter are two different
aspects of one and the same thing.” – Carl Jung
• https://junginla.org/education/what_is_sandplay• http://www.sandplayohio.com/what-is-sandplay.html

Demonstration
Ethical Considerations
Suzanne Blackwood
Kitchener’s Five Moral Principles
• Autonomy • Justice• Beneficence• Nonmaleficence• Fidelity
Ethical Decision Making Model
C.2.e. Consultations on Ethical ObligationsCounselors take reasonable steps toconsult with other counselors, theACA Ethics and Professional StandardsDepartment, or related professionalswhen they have questions regardingtheir ethical obligations or professionalpractice.
(American Counseling Association, 2014)
AAMFT Code of Ethics, Preamble, Seeking ConsultationSeeking Consultation The absence of an explicit reference to a specific behavior or situation in the Code does not mean that the behavior is ethical or unethical. The standards are not exhaustive. Marriage and family therapists who are uncertain about the ethics of a particular course of action are encouraged to seek counsel from consultants, attorneys, supervisors, colleagues, or other appropriate authorities.
(American Association for Marriage and Family Therapy, 2015)
Ethical Decision Making ModelsSteps in Making Ethical Decisions
– Identify the problem or dilemma – Identify the potential issues– Review relevant codes for guidance– Know the applicable laws and regulations– Seek consultation– Brainstorm possible courses of action– List the consequences of various decisions & reflect on the implications– Decide on what appears to be the best possible course of action– Follow up to evaluate the outcomes and decide if further action if
required (Newsome & Gladding, 2014, pp. 53-54)
Ethical Considerations:Group Discussion
https://www.huffingtonpost.com/2014/07/29/syrian-children-refugee_n_5618339.html
Client Welfare
A.1. Client WelfareA.1.a. Primary Responsibility
The primary responsibility of counselorsis to respect the dignity and promotethe welfare of clients.
(American Counseling Association, 2014)
Multicultural Counseling Competency
C.2.a. Boundaries of CompetenceCounselors practice only within theboundaries of their competence, basedon their education, training, supervisedexperience, state and nationalprofessional credentials, and appropriateprofessional experience. Whereasmulticultural counseling competency isrequired across all counseling specialties,counselors gain knowledge, personalawareness, sensitivity, dispositions, andskills pertinent to being a culturallycompetent counselor in working with adiverse client population.
(American Counseling Association, 2014)
Gifts3.9 Gifts
Marriage and family therapists attend to cultural norms when considering whether to accept gifts from or give gifts to clients. Marriage and family therapists consider the potential effects that receiving or giving gifts may have on clients and on the integrity and efficacy of the therapeutic relationship.
(American Association for Marriage and Family Therapy, 2015)A.10.f. Receiving Gifts
Counselors understand the challengesof accepting gifts from clients and recognizethat in some cultures, small giftsare a token of respect and gratitude.When determining whether to accepta gift from clients, counselors take intoaccount the therapeutic relationship, themonetary value of the gift, the client’smotivation for giving the gift, and thecounselor’s motivation for wanting toaccept or decline the gift.
(American Counseling Association, 2014)
Interpretation/Translation• If language and/or cultural barriers hinder effective communication in
therapy, it may be necessary to involve an interpreter• Client’s parent(s) should sign a release of information form• Ideally, the interpreter would be unbiased and have some familiarity
with mental health• Clinician, interpreter, and client/parents must be a good fit• Clinician should respect the interpreter as another professional• Interpreter should not have a dual relationship with the client/parents• Special care should be taken in cases with refugees because of the
potential emotional effects on interpreters
(Miller, et al., 2005; Searight & Searight, 2009; Yakushko, 2010)
Informed consent: Understand that families of
refugee status may be fearful and reluctant to sign legal forms
Informed Consent Cont…A.2.c. Developmental and Cultural Sensitivity
Counselors communicate informationin ways that are both developmentallyand culturally appropriate. Counselorsuse clear and understandable languagewhen discussing issues related toinformed consent. When clients havedifficulty understanding the languagethat counselors use, counselors providenecessary services (e.g., arranging fora qualified interpreter or translator)to ensure comprehension by clients.In collaboration with clients, counselorsconsider cultural implicationsof informed consent procedures and,where possible, counselors adjust theirpractices accordingly.(American Counseling Association, 2014; American Psychological Association, 2010;
Carnes-Holt, et al., 2016)
Informed Consent Cont…B.5.b. Responsibility to Parents and Legal Guardians
Counselors inform parents and legalguardians about the role of counselorsand the confidential nature of the counselingrelationship, consistent with currentlegal and custodial arrangements.Counselors are sensitive to the culturaldiversity of families and respect theinherent rights and responsibilities ofparents/guardians regarding the welfareof their children/charges accordingto law. Counselors work to establish,as appropriate, collaborative relationshipswith parents/guardians to bestserve clients.
(American Counseling Association, 2014)
Informed Consent Cont…A.2.d. Inability to Give Consent
When counseling minors, incapacitatedadults, or other persons unableto give voluntary consent, counselorsseek the assent of clients to servicesand include them in decision makingas appropriate. Counselors recognizethe need to balance the ethical rightsof clients to make choices, their capacityto give consent or assent to receiveservices, and parental or familial legalrights and responsibilities to protectthese clients and make decisions ontheir behalf.
(American Counseling Association, 2014)
Confidentiality and PrivacyB.1.a. Multicultural/Diversity
ConsiderationsCounselors maintain awareness and sensitivityregarding cultural meanings ofconfidentiality and privacy. Counselorsrespect differing views toward disclosureof information. Counselors hold ongoingdiscussions with clients as to how,when, and with whom information isto be shared.
(American Counseling Association, 2014; Brooks, et al., 2013; Carnes-Holt, et al., 2016)
Treatment ModalitiesC.7. Treatment Modalities
C.7.a. Scientific Basis for TreatmentWhen providing services, counselors use
techniques/procedures/modalities thatare grounded in theory and/or have anempirical or scientific foundation.
(American Counseling Association, 2014; Carnes-Holt, et al., 2016)
Diagnosing• If considering a diagnosis of PTSD, assess for specific symptoms of
the disorder and use differential diagnostic procedures• Avoid confusing with symptoms of other disorders such as
depression, grief, and various adjustment disorders• Consider ways to normalize symptoms when explaining them to
children and their parents• Remember that many children are resilient• Also, what is considered pathological in one culture may not be
considered pathological in another
(American Psychiatric Association, 2013)
Advocacy
A.7.a. AdvocacyWhen appropriate, counselors advocate at individual, group, institutional, and societal levels to address potential barriers and obstacles that inhibit access and/or the growth and development of clients.
(American Counseling Association, 2014)
AAMFT Code of Ethics, Preamble, AdvocacyCommitment to Service, Advocacy and Public Participation Marriage and family therapists are defined by an enduring dedication to professional and ethical excellence, as well as the commitment to service, advocacy, and public participation. The areas of service, advocacy, and public participation are recognized as responsibilities to the profession equal in importance to all other aspects. Marriage and family therapists embody these aspirations by participating in activities that contribute to a better community and society, including devoting a portion of their professional activity to services for which there is little or no financial return.
(American Association for Marriage and Family Therapy, 2015)

Self-Care• C.2.g. ImpairmentCounselors monitor themselves forsigns of impairment from their ownphysical, mental, or emotional problemsand refrain from offering or providingprofessional services when impaired.They seek assistance for problems thatreach the level of professional impairment,and, if necessary, they limit,suspend, or terminate their professionalresponsibilities until it is determinedthat they may safely resume theirwork. Counselors assist colleagues orsupervisors in recognizing their ownprofessional impairment and provideconsultation and assistance when warrantedwith colleagues or supervisorsshowing signs of impairment andintervene as appropriate to preventimminent harm to clients.
(American Counseling Association, 2014; American Psychological Association, 2010)
ReferencesAmerican Association for Marriage and Family Therapy (2015). AAMFT Code of Ethics. Alexandria,
VA: Author. Retrieved from: aamft.org/iMIS15/AAMFT/American Counseling Association (2014). ACA Code of Ethics. Alexandria, VA: Author. Retrieved from:
https://www.counseling.org/American Psychiatric Association. (2013) Diagnostic and statistical manual of mental disorders (5th
ed.). Washington DC: Author.American Psychological Association (2009). Working with refugee children and families: Update for
mental health professionals. Washington, DC: Author. Retrieved from: www.apa.org/pubs/info/reports/refugees-health-professionals.pdf
American Psychological Association (2010). Resilience and recovery after war: Refugee children and families in the United States. Washington, DC: Author. Retrieved from: http://www.apa.org/pi/families/refugees.aspx
Axline, V. (1947). Play therapy. Cambridge, MA: Houghton Mifflin.Barnett, J.E., Behnke, S.H., Rosenthal, S.L., & Koocher, G.P. (2007). In case of ethical dilemma, break
glass: Commentary on ethical decision-making in practice, Professional Psychology: Research and Practice, 38(1), 7-12. doi: 10.1037/0735-7028.38.1.7
Brooks, B., Fielder, K., Waddington, J., & Zink, K. (2013). Minors’ rights to confidentiality, when parents want to know: An ethical scenario. VISTAS 2013. Retrieved from: http://www.counseling.org/knowledge-center/vistas
ReferencesBureau of Population, Refugees, and Migration. (October 4, 2017). Proposed Refugee Admissions FY
2018. Retrieved from https://www.state.gov/j/prm/releases/docsforcongress/274613.htmCarnes-Holt, K., Maddox II, R.P., Warren, J., Morgan, M., & Zakaria, N.S. (2016). Using bookmarks:
An approach to support ethical decision making in play therapy. International Journal of Play Therapy, 25(4), 176-185. http://dx.doi.org/10.1037/pla0040380
Centers for Disease Control and Prevention (2016). About adverse childhood experiences. Retrieved from https://www.cdc.gov/violenceprevention/acestudy/about_ace.html
Etemadi, S. (December 4, 2013). Multicultural counseling with the immigrant and refugee communities. Counseling Today, n. pag. Retrieved from: ct.counseling.org/
Falicov, C. J. (2014). Latino families in therapy (2nd ed.). New York, NY, US: Guilford Press.Gil, E. (2017). Posttraumatic play in children: What clinicians need to know. New York, NY: The
Guilford Press.Goodyear-Brown, P. (2010). Play therapy with traumatized children: A prescriptive approach. Hoboken,
NJ: John Wiley & Sons. Meyers, L. (January 27, 2016). Immigration’s growing impact on counseling. Counseling Today, n.
pag. Retrieved from: ct.counseling.org/Migration Policy Institute. (June 7, 2017). Refugees and Asylees in the United States. Retrieved from
https://www.migrationpolicy.org/article/refugees-and-asylees-united-states#StatesMiller, K.E., Martell, Z.L., Pazdirek, L., Caruth, M., & Lopez, D. (2005). The role of interpreters in
psychotherapy with refugees: An exploratory study. American Journal of Orthopsychiatry, 75(1), 27-39. doi: 10.1037/0002-9432.75.1.27
ReferencesMcGoldrick, M., Giordano, J., & Garcia-Preto, N. (Eds.). (2005). Ethnicity and family therapy (3rd ed.).
New York, NY, US: Guilford Press.Newsome, D.W., & Gladding, S.T. (2014). Clinical mental health counseling in community and agency
counseling (4th Ed.). Upper Saddle River, NJ: PearsonOffice of Refugee Resettlement. (March 27, 2018). Facts and Data. Retrieved from
https://www.acf.hhs.gov/orr/about/ucs/facts-and-dataSearight, H.R. & Searight, B.K. (2009). Working with foreign language interpreters: Recommendations
for psychological practice. Professional Psychology: Research and Practice, 40(5), 444-451. doi: 10.1037/a0016788
Tennessee Immigrant & Refugee Rights Coalition. (2018). What is welcoming Tennessee? Retrieved from https://www.tnimmigrant.org/what-welcoming-tennessee/
Terr, Lenore. (1990). Too scared to cry: Psychic trauma in childhood. New York, NY: Basic Books. The National Child Traumatic Stress Network (n.d.). Retrieved from http://nctsn.org/trauma-
types/refugee-trauma/learn-about-refugee-experienceYakushko, O. (2010). Clinical work with limited English proficiency clients: A Phenomenological
exploration. Professional Psychology: Research and Practice, 41(5), 449-455. doi: 10.1037/a0020996
Resources • Play Therapy: The Art of the Relationship by Gary Landreth• Posttraumatic Play in Children: What Clinicians Need to Know by Eliana Gil• Play Therapy with Traumatized Children: A Prescriptive Approach by Paris
Goodyear-Brown• The National Child Traumatic Stress Network: https://learn.nctsn.org/• Mental Health Provide Considerations: https://www.nctsn.org/what-is-child-
trauma/trauma-types/refugee-trauma/interventions• Refugee services core stressor assessment tool:
https://www.nctsn.org/resources/refugee-services-core-stressor-assessment-tool
• Understanding refugee trauma: https://www.nctsn.org/what-is-child-trauma/trauma-types/refugee-trauma/nctsn-resources