Embed Size (px)
Citation preview

Plato Versus Aris tot le : Categor ica l and D i m e n s i o n a l Mode l s for C o m m o n Menta l D i s o r d e r s
David Goldberg
There are two quite different ways of conceptualizing common mental disorders: as categorically distrib- uted or as dimensions. In the former case, individuals wi th " sub th resho ld " disorders may contain a smal l proportion of "true cases"; while in the latter, they are seen as having the same basic disorder, but in insuffi- cient degree to warrant a diagnostic label. The categori- cal school postulates the phenomenon of "comorbid- ity" to account for those who are both depressed and anxious. The dimensional school regards t hem as cases of "anxious depression," and observes that the 2 dimensions are highly correlated with one another. This article considers 3 levels of severity of cases satisfying research diagnostic criteria for depression: mild, moderate, and severe. At ascending levels of
initial severity, there is increasing disability, and a worse outcome at 12 months, The only positive t reat- ment effect is that favoring antidepressants over sedatives at 3 months, and th is ef fect is related to initial severity--being much greater for the "severe" group of depressions. Initial severity is linearly related to disability, and there is no disjunction at the usual division between "non-cases" and "cases" of depres- sion. Clinicians are obliged to use categorical con- cepts, as they must decide who is sufficiently ill to justify treatment. But in our ef for ts to understand the relationships between social and biological variables, dimensional models are far more appropriate. Copyright © 2000 by W.B. Saunders Company
T HE SYMPTOMS of common mental disorders are continuously distributed in consulting
populations. If they were not, our task would be so much easier. However, despite these continuous distributions, there are two fundamentally different approaches to diagnoses.
THE PLATONIC APPROACH
This is the traditional continental approach, associated with the names of Kahlbaum and Krae- pelin, recently given a new lease on life by the DSM system in the United States. It endows diagnoses with a mysterious independent existence but holds that they are, at least for the time being, unobservable. We can acquire information about them only indirectly, by observing symptoms. With an increasing number of symptoms, we consider it increasingly more probable that we have somehow trapped the underlying phenomenon. For this ap- proach to diagnosis, at around the threshold num- ber of symptoms given in the DSM-IV system, there is (it is hoped) a sharply increasing probabil- ity that the net will be found to contain a fish. According to this school, populations of people with "subthreshold" levels of symptoms perhaps contain some true cases but we may not notice them, as the effect may be lost in the noise
From the Institute of Psychiatry, King's College, London, UK. Address reprint requests to Sir David Goldberg, Institute of
Psychiatry, King's College, De Crespigny Park, London SE5 8AF, UK.
Copyright © 2000 by W.B. Saunders Company 0010-440X/00/4102-1002510. 00/0
produced by the false-positives--the symptomatic people who could easily be mistaken for cases and who are generally muddying the waters.
It is this school that tends to reify the concept of caseness, and which often assumes that each diag- nostic concept will be found to correspond to a particular biological derangement. The real differ- ence between the two camps arises when a group of individuals are found to manifest two different sets of symptoms. Here, the Platonists assert that these individuals have had the misfortune to be afflicted with two different illnesses, and the concept of "comorbidity" is born. To the extent that different Platonic processes have common antecedents, they cannot be truly different processes, and the Platonic theorist is discomforted. Either the individual has two illnesses simultaneously, with two quite sepa- rate, unrelated biological processes underlying the two sets of symptoms (and thus, "comorbidity"), or perhaps they are the same underlying process and are different only in epiphenomenal appear- ance. In the latter case, the Platonist will of course withdraw the concept of comorbidity.
In the last 20 years, the (Platonic) classifications offered by the official taxonomies for common mental disorders have changed considerably. In the ICD-8, which was current in the 1970s, mixed states of anxious depression were classified, to- gether with pure depression, as "neurotic depres- sion." In the DSM-III, major depressive episode and dysthymic disorder replaced neurotic depres- sion. While one could qualify for major depression in just 2 weeks, both dysthymic disorder and
8 Comprehensive Psychiatry, Vol. 41, No. 2, Suppl. 1 (March/April), 2000: pp 8-13

PLATO VERSUS ARISTOTLE 9
generalized anxiety disorder were defined as last- ing for more than 6 months. The most recent taxonomies, DSM-IV and ICD-10, require two diagnoses to be made if both anxious and depres- sive symptoms are present in sufficient degree. Only the ICD-10 has a concept of "mixed anxiety- depression," but this is defined as a subthreshold condition for either group of disorders, but with sufficient symptoms in total to justify a diagnosis; it is therefore by definition a mild disorder. Unfortu- nately for the taxonomists, mixed states are ex- tremely common, and the severest disorders seen in primary care have both sets of symptoms: thus, it is by no means a mild disorder. The Platonists have to deal with this by declaring that the patients are comorbid for 2 disorders.
This is an unsatisfactory solution, for two rea- sons. The first of these is that the two disorders have common genetic origins, 1-3 and the second is that the disorders do not "breed true" from one episode to another. 4-6 The unstable nature of the disorders over t ime favors the model stipulating that small changes in the balance between anxious and depressive symptoms will produce different diagnoses on different occasions. The different combinations of anxious and depressive symptoms are more parsimoniously accounted for by different kinds of life experience between the different episodes of illness .7.8
Despite almost 100 years of tampering with the ideal classification, no ideal way of classifying even the common disorders has emerged. Rather than carving nature at the joints, we appear to be drawing lines in the fog. For the social researcher, there are serious problems with this approach. However, for the working clinician, Plato is the best we have, provided that we remember not to take him seriously.
THE ARISTOTELEAN APPROACH
The alternative approach to diagnoses is associ- ated with the work of Adol f Meyer and the psychobiological school, and is often used in recent times by both social researchers and clinical psy- chologists. Aristotle asserted that the only reality resides in the evidence of our senses, so followers of this school assert that all we have are the symptoms, and they generally prefer dimensional models to account for covariation between groups of symptoms. Where two groups of symptoms commonly occur together, adherents of this ap-
proach merely want to know what the determinants of each set of symptoms are so that they can understand how overlap between the two sets can occur in a population. Of course, both camps are interested in this; the difference between them here is mainly presentational. The Platonists, of course, cannot understand why anyone should want to use a dimensional approach, since it is at best a misconceived view of the world. Categorical and dimensional models are merely alternative ways of looking at the same data; it is not that one is right and the other wrong.
In fact, not only correlated biological processes but also correlated social phenomena are easier to assimilate to a dimensional model of symptoms. Diagnoses, according to the Aristoteleans, are man- made abstractions, liable to be discarded or modi- fied according to their usefulness. And the uses can be quite different: the scientific use may not be the same as the practical use, and the practical use may not be the same as the political use.
An example may make this clearer. If we were trying to relate the effects of some social va r i ab l e - - for example, being physically abused during child- hood by one's ca reg iver - -wi th the later develop- ment of depressive symptoms, we might choose a different level to define what we mean by depres- sion than a clinician would use in deciding whether to offer a patient an antidepressant. And the thresh- old used to define drug treatment might not be the same as that used to define "major depressive disorder," this being an impressive-sounding diag- nosis that justifies payment by an insurance com- pany. In practice, everyone tends to keep quiet about this and to use the same thresholds for scientific, clinical, and political purposes; but there is really no reason that they should do so--unless , of course, they are followers of Plato. Followers of Aristotle are quite comfortable with dimensional approaches to symptoms, as a dimensional model is clearly just a different way of thinking about symptoms, probably more suitable for scientific purposes, and pretty hopeless for clinical purposes.
Earlier work using the short version of the Present State Examination has shown that in con- suiting samples in primary care, most of the variance between mental symptoms can be ac- counted for by two highly correlated d ime ns ions - - those of anxious symptoms, on one hand, and depressive symptoms, on the other. 9 They can even use their dimensions to compare various Platonic

10 DAVID GOLDBERG
concepts of diagnosis and can demonstrate where these concepts are located in a dimensional symp- tom space and how discriminant between subjects the various concepts are at these locations. 1° More recent work has shown that to achieve factor invariance between countries, it may be necessary to consider the existence of a third dimension-- phobic symptoms/1 However, this work was per- formed by investigators using the same diagnostic instrument, and this interview does not include items dealing with the use of drugs or alcohol, has no detailed questions concerning somatic symp- toms, does not ask about conduct disorders, and--in the short form of the interview--does not even ask about psychotic experiences. While many of these shortcomings have been remedied in the much longer Schedules for Clinical Assessment of Neuro- psychiatric Disorders (SCAN) interview, it is clear that the inclusion of extra test items dealing with very different types of morbid experience would likely produce different symptom dimensions.
It is clear that all is not well with the Aristote- leans, despite the general reasonableness of their approach. Furthermore, as a grid for the working clinician rather than the researcher, Aristotle is probably a nonstarter.
THE THRESHOLD FOR CASENESS
The strict Platonic view is that an illness is rather like the concept of pregnancy--you either have it or you don't. You cannot be a little pregnant any more than you can be intensely pregnant. The best that they can do is to suggest that at subthreshold levels of observable symptoms, there is a decreas- ing probability that there will be cases of Platonic disorders present. The Aristoteleans have no prob- lems with subthreshold caseness, since they take a dimensional view of disorder, and the concept of severity of illness is also easy to assimilate with their model.
An opportunity to study the problem of individu- als with subthreshold symptom levels arose when the World Health Organization (WHO) decided to study psychological disorders as they occur in general medical settings/2 This is because such populations inevitably contain large numbers of individuals with scores around the threshold for case identification, and they have not been either selected or self-selected to attend clinics operated by psychiatrists. One of the objectives of the WHO Study of Psychological Disorders in General Health
Care was to investigate the thresholds used by psychiatrists in a different setting, to discover the natural history of those disorders that were just "subthreshold" in the conventional diagnostic sys- tem.
Moily examined the effects of lowering the conventional threshold by two symptoms for each diagnosis (S. Moily, personal communication, No- vember 1998). While the usual threshold identified 35.6% of the patients as psychiatric cases, the subthreshold disorders accounted for an additional 13.3% of the attenders. A simple, linear dimen- sional model would predict that if one knows the prevalence of a particular disorder in a population, one should be able to predict the number of subthreshold cases in that population. Interestingly, the subthreshold disorders were not found to be in a fixed relationship to the above-threshold disorders, so the proportion of subthreshold disorders could not be confidently predicted from a knowledge of prevalence.
As one would expect, general practitioners recog- nized more cases above the threshold (50%) than just below it (43%). Subthreshold cases were found to be associated with an appreciable disability, and were often associated with chronic physical ill- health. Patients with subthreshold disorders rated their own general physical health as excellent to fair; of those with subthreshold anxiety and depres- sive disorders, almost 90% did so, although fewer (66%) of the somatic disorders did so (P < .005). Discussion or counseling were the most common treatments given, although drugs were also used--- antidepressants were more likely to be given for subthreshold anxiety (23%) than for subthreshold depression (8%). The data are consistent with a
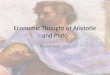
% - :t ,o,re--°, depressed [u UntreatedJ t year later
Mild Moderate Severe
Fig 1. Proportion of patients still depressed 1 year later according to whether they were recognized and treated with drugs by their general practitioner or did not receive drug treatment, by initial severity of depression.

PLATO VERSUS ARISTOTLE
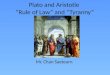
go ] I r~ II: l~p_~t~nl_q~rl I
%
M i l d M o d e r a t e S e v e r e
Fig 2. Proportion of patients still depressed I year later according to whether they were recognized by their general practitioner or unrecognized, by initial severity of depression.
dimensional view, and no marked disjunctions occurred between non-cases and cases for any variable studied.
THE (ARISTOTELEAN) CONCEPT OF SEVERITY
If we divide recognized diagnosable depressed patients into three groups--mild, moderate, and severe---depending on the number of depressive symptoms at baseline, then we see that the drug- treated mild and moderate groups have, if anything, a worse prognosis than patients who were not prescribed drugs, but severely depressed patients (more than 12 depressive symptoms) had a worse prognosis if they did not receive drug treatment (Fig 1).
If we now compare these recognized depressed patients with unrecognized depressions detected by the two-stage screening procedure, then, once more, the outlook is fairly similar for the mild and moderate depressions, but the unrecognized severe depressions were improved 12 months later (Fig 2). There are several possible explanations for these data, and it is not possible to say which is true; however, we see that severity is a factor to be taken into account.
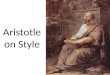
6
0 or 1 Some Sub- Above symptom symptoms threshold threshold
Fig 3. Number of disability days on the Groningen Disabil- i ty Schedule at onset by degree of mental disturbance.
11
18
16!
14.
12
10.
8.
6~
4.
2
0
- - Drug treated • Severe ~ - - _ - - - - Undetected • Moderate
Fig 4. Outcome at 12 months on the CIDI by initial severity of depression (mild, moderate, and severe) for depressions treated with drugs and those undetected by their general practitioner.
The relationship between severity assessed by the number of depressive symptoms and disability as measured by the Groningen Disability Schedule is straightforward and perfectly linear, with sub- threshold depressions being intermediate between those with several symptoms and those satisfying current concepts for caseness (Fig 3).
If we consider determinants of outcome at 12 months, the initial severity on the Composite International Diagnostic Interview (CIDI) inter- view bears a constant relationship to outcome at 12 months, both for those treated with drugs and the undetected group (Fig 4). Similar findings are found with the General Health Questionnaire (GHQ), with results for 3 time points (Fig 5).
The only effect of treatment is seen if we contrast depressed patients treated with antidepressants and those treated with benzodiazepines and consider the data at 3 months of follow-up (Fig 6). Here, we see a treatment effect which is proportional to the initial severity and much greater for the severe group than for the mild group. At 1-year follow-up,
15
10
5
0
- - Treated, any drug • Severe . . . . U n d e t e c t e d • M o d e r a t e
-4
3 m o n t h s 12 m o n t h s
Fig 5. Outcome of depression measured by the GHQ-28 at 3 t ime points by initial severity of depression (mild, moderate, and severe) for depressions treated with drugs and those undetected by their general practitioner.

12
2S / - - Benzos # Severe . . . . . Ant idepressants • Moderate
20 ~ ~ _ ~ . Mi ld
o ~ 0 3 months 12 months
Fig 6. Outcome of depression measured by the GHQ-28 at 3 t ime points by init ial severity of depression (mild, moderate, and severe) for depressions treated with antidepressants and those treated with benzodiazepines.
however, the differences between groups are short of statistical significance.13
Another approach is to consider the rate of loss of symptoms. If we consider depressed patients' scores at the 3-month follow-up, at each increased level of initial severity, there is an expectancy of a higher GHQ score (Fig 7). On the left side of Fig 7, the depressions are subthreshold disorders with only 4 symptoms, and as we move to the right, the depressions increase by 2 symptom increments to 12 depressive symptoms. The usual threshold is 6 symptoms. It is of interest that first episodes return to normal less quickly than subsequent episodes.
The disability at 3 months of follow-up associ- ated with each level of initial severity is shown in Fig 8. Once more, there is a steady increase in disability without any disjunction at each increased level of initial severity. It is of interest that subse- quent episodes of depression are associated with lesser degrees o f disability than the first episode, and this relationship holds until the highest level of initial i l lness--when disability is the same for first and subsequent episodes.
14
~= 12
l O
8
4
2
• First episode
• Previous episode
4 6 8 10 12
Initial severity
Fig 7. Scores on the GHQ-28 for subjects experiencing a first episode of depression, and those experiencing a recur- rent episode, by severity of initial episode of depression.
DAVID GOLDBERG
s
e
7
e
~ 5
2
1
O
.J / /
/ /
/ /
• First episode
• Previous episode
e 8 l o 12
Initial severity
Fig 8. Disabi l i ty days at 3 months for subjects experiencing a first episode of depression, and those experiencing a recur- rent episode, by severity of initial episode of depression,
It would appear that the severity of depressive illness is a major determinant of course and of associated disability. Strict Platonists do them- selves a disservice by assuming that everyone "above the line" is a member of a homogeneous group. It is clear that they will need to be loose Platonists who allow themselves to use dimen- sional concepts when it suits them. It is also of great interest that subsequent episodes of depres- sive illness are associated with lesser degrees of disability and somewhat quicker recovery than first episodes.
CONCLUSION
It turns out that both Plato and Aristotle make pretty much the same sense of our findings concern- ing depression in general practice, although for different reasons. The Aristoteleans take the view that whatever the effect of a biological treatment, it is bound to be less at each lower cutoff point, since there will be a smaller chance that there is any biological abnormality to treat. They are nonethe- less interested in what this point is when a disorder is held to be present, since it indicates a point in human misery when help from a third party might offer real advantages.
The Platonists consider that at each lower cutoff point, we are dredging up smaller numbers of "real fish" but count on these fish to have the same characteristics as the fish known to psychiatrists. In practice, of course, this is to make an inductive error, since they do not have similar characteris- t i c s - a s the cases seen by psychiatrists have more abnormal personalities and disturbed family struc- tures than those seen in general medical practice, and thus may need different treatments.
In clinical work, one should aim to be a skeptical

PLATO VERSUS ARISTOTLE 13
P l a t o n i s t - - n o t taking it all too seriously, and be ing
prepared to use Ar is to te lean concep t s such as
anxious depress ion , sever i ty o f i l lness, or schizoaf-
fect ive psychos is . However , in a t tempts to under-
s tand the phenomena , whe the r we are deal ing wi th
the biological substrate o f menta l d isorders or the
effects o f social variables on mental d isorders , the
best thing to do is to change m o d e s and to use
Ar is to te lean concepts . In this way, one will not
b e c o m e too puzz led when the essent ial cont inui t ies
be tween subcl inical d isorders and those sat isfying
m o d e m diagnost ic criteria are encountered .
ACKNOWLEDGMENT
Participating investigators in the Psychological Problems in General Health Care project: 0. Ozturk and M. Rezaki in Ankara; C. Stefanis and V. Mavreas in Athens; S. Channabasa- vanna and T. Sriram in Bangalore; H. Helmchen and M. Linden in Berlin; W. vanden Brink and B. Tiemens in Groningen; M. Olatawura and O. Gureje in Ibadan; O. Benkert and W. Maier in Mainz; R. Gater and S. Kisely in Manchester; Y. Nakane and S. Michitsuji in Nagasaki; Y. LeCrubier and P. Boyer in Paris; J. Costa e Silva and L. Villano in Rio de Janeiro; R. Florenzano and H. Acuna in Santiago de Chile; G. Simon and M. vonKorff in Seattle; Y. He-Quin and X. Shi-Fu in Shanghai; and M. Tansella and C. Bellantuono in Verona. Supported by grants from the World Health Organization.
REFERENCES
1. Kendler K, Heath A, Martin N, Eaves L. Symptoms of anxiety and symptoms of depression. Arch Gen Psychiatry 1987; 122:451-457.
2. Eley T. General genes: a new theme in developmental psychopathology. Curr Direct Psychol Sci 1997;6:90-95.
3. Thapar A, McGuffin P. Anxiety and depressive symptoms in childhood--a genetic study of co-morbidity. J Child Psychol Psychiatry 1997;38:651-656.
4. Andrews G, Stewart G, Morris-Yates A, Holt N, Hender- son AS. Evidence for a general neurotic syndrome. Br J Psychiatry 1990;157:13-18.
5. Goldberg D, Huxley P. Common Mental Disorders---A Biosocial Model. London, UK: Routledge, ! 992.
6. Vollrath M, Angst J. Results of the Zurich Study: course of anxiety and depression. Psychiatry Psychobiol 1989;4:307-313.
7. Brown GW, Adler Z, Bifulco A. Life events, difficulties and recovery from chronic depression. Br J Psychiatry 1988;152: 487-498.
8. Neeleman J, Oldehinkel T, Ormel J. Time to recovery from common mental disorder: the role of positive life change.
Abstract, 22nd European Conference on Psychosomatic Disor- der; August 22, 1998; Manchester, UK.
9. Goldberg DP, Bridges P, Duncan-Jones P, Grayson DA. Dimensions of neurosis seen in primary care settings. Psychol Med 1987;17:461-470.
10. Grayson DA, Bridges P, Duncan-Jones P, Goldberg DE The relationship between symptoms and diagnoses of minor psychiatric disorder in general practice. Psychol Med 1987;17: 933-942.
11. Ormel J, Oldehinkel A J, Goldberg D, Hodiamont PPG, Wilmink FW, Bridges K. The structure of common psychiatric symptoms: how many dimensions of neurosis? Psychol Med 1995;25:521-520.
12. Ustun B, Sartorius N. Mental Illness in General Health Care. An International Study. Chichester, UK: Wiley, 1995.
13. Goldberg D, Privett M, Ustun T, Simon G, Linden M. The effects of detection and treatment on the outcome of major depression in primary care: a naturalistic study in 15 cities. Br J Gen Pract 1998;48:1840-1844.