Embed Size (px)
Citation preview

Virtual Journal Club
Ovarian Cancer
Platinum-Sensitive Recurrent Ovarian Cancer:
Making the Most of Emerging Targeted Therapies
Discussants:
Mansoor R. Mirza, MDCopenhagen University Hospital
Rigshospitalet
Copenhagen, Denmark
Ignace Vergote, MD, PhDUniversity Hospitals Leuven
Leuven, European Union
Reference Slides

Recurrent Ovarian Cancer
• Patients relapsing after >6 months are treated
with subsequent lines of platinum-based
therapy until resistance or death
– Successive lines of treatment associated
with lower response to treatment, increase
in tumor burden, and increase in
cumulative drug toxicity
– Median overall survival (OS) after first
recurrence is 2-3 years
• Maintenance therapy with bevacizumab or
olaparib remains the only non-
chemotherapeutic option in this setting
Hennessey BT, et al. Lancet. 2009;374(9698):1371-1382. Hanker LC, et al. Ann Oncol. 2012;23:2605-2612. National Comprehensive Cancer Network.
NCCN Clinical Practice Guidelines. Available at: https://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed: December 1, 2016.
80% of women with ovarian cancer relapse on first-line treatment
with platinum-based chemotherapy

Lig3XRCC1
PolßPNK
Poly (ADP-Ribose) Polymerase (PARP)
• PARP plays a key role in the repair of DNA single-strand breaks through
the base excision repair pathway
• Binds directly to sites of DNA damage and generates large, branched
chains of poly (ADP-ribose) polymers on multiple target proteins
• Recruits other DNA repair enzymes
Plummer ER, et al. Clin Cancer Res. 2007;13:6252-6256. Farmer H, et al. Nature. 2005;434:917-921.

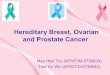
BRCA and PARP
• BRCA genes are critical for DNA damage repair and cells with
defective BRCA genes are more susceptible to DNA-damaging
therapy, including PARP inhibition
• In cells that are BRCA-1 and BRCA-2 deficient in the presence of a
PARP inhibitor, there is a marked decrease in the ability of cells to
repair themselves and, as a result, the concentration of the cells
diminishes over time
• Having both PARP inhibition as well as an abnormality in homologous
repair results in greater cell death
• PARP inhibitors have demonstrated activity as maintenance therapy in
recurrent, platinum-sensitive ovarian cancer with BRCA mutations or
deficiencies in homologous recombination (HRD)
Plummer ER, et al. Clin Cancer Res. 2007;13:6252-6256. Farmer H, et al. Nature. 2005;434:917-921.

PARP Inhibitor Mechanism of Action
Iglehart JD, et al. N Engl J Med. 2009;361(2):189-191.

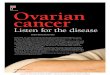
PARP Inhibitors in Ovarian Cancer
Ledermann J, et al. N Engl J Med. 2012;366:1382-1392.
Months Since Randomization
Hazard ratio, 0.35 (95% CI, 0.25-0.49)
P < .001
Pro
ba
bil
ity o
f P
rog
res
sio
n-F
ree
Su
rviv
al
Olaparib
Placebo

PARP Inhibitors in Ovarian Cancer
PARP inhibitor Route Target Current status in ovarian cancer
Olaparib (AZD2281)1 PO PARP-1,
PARP-2,
PARP-3
Approved as maintenance therapy for recurrent,
platinum-sensitive, BRCA mutated ovarian cancer
Veliparib (ABT-888)2 PO PARP-1,
PARP-2
Phase II trial complete; phase III trial ongoing
Rucaparib (CO338, AGO14699
and PF01367338)3
PO PARP-1,
PARP-2,
PARP-3
Phase II trial complete; phase III trial ongoing
Niraparib (MK4827)4 PO PARP-1,
PARP-2
Phase III trial completed
Talazoparib (BMN 673)5 PO PARP-1,
PARP-2
Phase II trial ongoing
1. Ledermann J, et al. N Engl J Med. 2012;366:1382-1392. 2. Coleman RL, et al. Gynecol Oncol. 2015;137(3):386-391. 3. Drew Y, et al. Br J Cancer.
2016;114(7):723-730. 4. Mirza MR, et al. N Engl J Med. 2016;375:2154-2164. 5. Meehan RS, et al. Gynecol Oncol Res Pract. 2016;3:3.

BRCA Wild-Type Ovarian Cancer
• Most studies of PARP inhibitors in ovarian cancer have focused
on patients with germline BRCA mutations and/or HRD
• For patients without these mutations, platinum chemotherapy
followed by watchful waiting is the only available treatment option
• Niraparib, a potent, oral, selective PARP 1-2 inhibitor, has
demonstrated antitumor activity in both BRCA mutated and
BRCA mutation-negative high-grade serous ovarian cancer
Meehan RS, Chen A. Gynecol Oncol Res Pract. 2016;3:3.

Niraparib Early Phase Clinical Trial
• Efficacy of niraparib was evaluated in a phase I dose
escalation trial in sporadic cancer, including ovarian cancer
• Overall response rate (ORR) was 40% in BRCA mutated
ovarian cancer and 50% in platinum-sensitive BRCA mutants
• 3 of 4 (75%) patients with platinum-sensitive ovarian cancer
receiving the recommended dose of 300 mg responded
• Median PFS was 63 weeks both in patients with BRCA
mutations and those without BRCA mutations
Sandhu SK, et al. Lancet Oncol. 2013;14(9):882-892. Michie CO, et al. J Clin Oncol. 2013;suppl: Abstract 2513.

Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.

ENGOT-OV16 NOVA Trail
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.
Germline BRCA Mutant (gBRCA mut) Non Germline BRCA Mutant
P <
.05
P <
.05;
P <
.05

ENGOT-OV16 NOVA Trail: Patient Demographics and Baseline Characteristics
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.

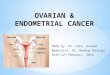
PFS: Germline BRCA Mutation
21.0 months
5.5 months
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.
P < .001

PFS: Germline BRCA Mutation Negative
9.3 months
3.9 months
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.
P < .001

PFS: Germline BRCA Mutation Negative, HRD Positive
12.9 months
3.8 months
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.
P < .001

PFS Subgroup Analysis
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.

Secondary Efficacy Endpoints
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.
Chemotherapy-free interval
• Germline BRCA mutation: HR 0.26 (22.8 months vs 9.4 months; 95% CI: 0.169, 0.414; P < .0001
• Non germline BRCA mutation: HR 0.50 (12.7 months vs 8.6 months; 95% CI: 0.370, 0.666; P < .0001
Time to first subsequent treatment
• Germline BRCA mutation: HR 0.31 (21.0 months vs 8.4 months; 95% CI: 0.205, 0.481; P < .0001
• Non germline BRCA mutation: HR 0.55 (11.8 months vs 7.2 months; 95% CI: 0.412, 0.721; P < .0001
Progression-free survival 2 (data are immature)
• Germline BRCA mutation: HR 0.48 (25.8 months vs 19.5 months; 95% CI: 0.280, 0.821; P = .0062
• Non germline BRCA mutation: HR 0.69 (18.6 months vs 15.6 months; 95% CI: 0.494, 0.964; P = .0293
Overall survival (data are immature)
• <20% patients death in either treatment arm; HR 0.73 (95% CI, 0.480 to 1.125; P = .1545

Adverse Events
Treatment-emergent grade 3/4 adverse events occurring in ≥5% of patients
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.
*There are no grade 5 events.
AML, acute myeloid leukemia; MDS, myelodysplastic syndrome

Dose Adjustments Due to Treatment-Emergent Adverse Events
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.

Conclusions• There is an unmet need in platinum-sensitive, recurrent ovarian cancer for treatments that
prolong survival and improve patient quality-of-life
• The currently approved PARP inhibitor, olaparib, improves outcomes in patients with BRCA
mutations and/or HRD deficiencies
• In a randomized, double-blind, placebo-controlled phase III trial, maintenance treatment with
the selective PARP 1/2 inhibitor niraparib significantly improved PFS in all patient subgroups
examined, regardless of BRCA mutation or HRD status
– gBRCA mut: HR 0.27
– No gBRCA mut: HR 0.45
– No gBRCA mut, HRD positive: HR 0.38
• Hematologic laboratory abnormalities were the most common adverse events and were
managed through dose reduction
– The 1.4% rate of MDS/AML is similar to other PARP inhibitors currently used in this
setting.
• Niraparib represents a novel approach to management of recurrent, platinum-sensitive
ovarian cancer and opens the door for PARP inhibitor therapy in patients without
BRCA mutations