Embed Size (px)
Citation preview

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin: A Second-Generation Platelet ConcentrateJoseph Choukroun and Richard J. Miron
Abstract
Almost two decades have passed since platelet rich fibrin (PRF) was first introduced. Initially, theprimary objective was to develop a therapy where platelet concentrates could be introduced intowounds by effectively utilizing the body’s natural healing capacity. This was achieved by collectinggrowth factors derived from blood in a natural way. Platelet rich plasma (PRP) and platelet richgrowth factor (PRGF) had been commercialized, yet both contained secondary byproducts thatwere both unnatural and known inhibitors of wound healing. By removing these anti-coagulantsand modifying centrifugation protocols, PRF was introduced some years later with the potential tomarkedly impact many fields of medicine including dentistry. Many aspects important for tissue re-generation have since been revealed including the important role of fibrin as well as the preferentialrelease of growth factors over longer periods of time from PRF. Furthermore, by introducing a newset of cells into platelet concentrates (namely leukocytes), a marked impact on tissue regenerationand wound healing was observed. Over the past 5 years, further modifications to centrifugationspeed and time have additionally improved PRF into a concept now known as the “low-speed cen-trifugation concept.” Investigators began to modify surgical techniques to favorably treat patientswith PRF with improved clinical outcomes. Together, many key opinion leaders from around theglobe have been gathered to share their experiences and knowledge in many educational coursesand seminars in what we now know as platelet rich fibrin. In this first chapter, we highlight thediscovery of PRF and the studies leading to its first use in regenerative medicine. We focus specifi-cally on its properties for wound healing and how its presented advantages over previous versionsof platelet concentrates have favorably enhanced the regenerative potential of platelet concentratesin dentistry.
Highlights
� Introduction of Platelet Rich Fibrin� Reasons for its invention two decades ago� Its variations from the formally known
platelet concentrate “platelet rich plasma”or “PRP”
� The first case treated with PRF� Properties important for wound healing
. Introduction
Wound healing is a complex biological pro-cess where many cellular events taking placesimultaneously leading to the repair or regen-eration of damaged tissues [1–4]. Manyattempts have been made in the field oftissue regeneration with the aim of pre-dictably repairing, regenerating, or restoring
Platelet Rich Fibrin in Regenerative Dentistry: Biological Background and Clinical Indications, First Edition.Edited by Richard J. Miron and Joseph Choukroun.© 2017 John Wiley & Sons Ltd. Published 2017 by John Wiley & Sons Ltd.
COPYRIG
HTED M
ATERIAL

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin in Regenerative Dentistry
damaged and diseased tissues [1–4]. Theseinclude strategies with foreign materialsoften derived from allografts, xenografts, orsynthetically produced alloplasts to regener-ate host tissues [1–4]. While many of thesematerials have shown promise in variousaspects of regenerative medicine, it is impor-tant to note that all create a “foreign bodyreaction,” whereby a foreign material is intro-duced into human host tissues.
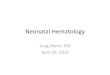
Platelet concentrates collected from wholeblood was first introduced over 20 years ago.The concept was developed with the aim ofutilizing human blood proteins as a source ofgrowth factors capable of supporting angio-genesis and tissue ingrowth based on thenotion that blood supply is a prerequisitefor tissue regeneration [5]. Four aspects ofwound healing have since been described askey components for the successful regener-ation of human tissues (Figure 1.1). Theseinclude 1) hemostasis, 2) inflammation, 3)proliferation, and 4) maturation. Each phaseencompasses various cell types. One of themain disadvantages of currently utilized bio-materials in the field of tissue engineering isthat the great majority are typically avascu-lar by nature, and therefore do not provide
the necessary vascular supply to fully obtainsuccessful regeneration of either soft or hardtissues [5].
It must further be noted that in general,wound healing demands the complex inter-action of various cell types with a three-dimensional extracellular matrix as well assoluble growth factors capable of facilitat-ing regeneration [6]. Certainly, one area ofresearch in dentistry that has gained tremen-dous momentum in recent years is that ofrecombinant growth factors where a num-ber have been used to successfully regener-ate either soft or hard tissues [7–9]. Table 1.1provides a list of currently approved growthfactors along with their individual roles intissue regeneration and clinical indicationssupporting their use. Similarly, a numberof barrier membranes with various func-tions and resorption properties have alsobeen commonly utilized in regenerative den-tistry formulated from either synthetic oranimal-derived materials [10]. Lastly, manybone-grafting materials are brought to mar-ket every year, all characterized by their spe-cific advantages and disadvantages duringtissue regeneration. While each of the above-mentioned biomaterials have been shown to
Figure . Four phases of wound healing including 1) hemostasis, 2) inflammation, 3) proliferation, and 4)maturation. Noteworthy are the overlaps between each of the phases and the population of cells found in eachcategory. Whereas lymphocytes typically arise at 7 days, the ability for PRF to introduce a high number at day 0acts to speed the regenerative phase during this process.

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
1 Platelet Rich Fibrin
Table . List of growth factors used for the regeneration of periodontal intrabony defects with listedadvantages and disadvantages.
Growth factor Advantages Disadvantages
Enamel Matrix Derivative – Mimics the formation of rootdevelopment
– Amelogenin proteins improvesPDL cell adhesion, proliferationand differentiation
– Adsorbs to the root surface up to4 weeks post-surgery
– Histologically demonstrated as“true” periodontal regenerationwith formation of Sharpey’s fibers
– Gel formulation unable to preventflap collapse
– Adsorption to other materialsuncertain
Platelet-Derived GrowthFactor
– Growth factor with the strongestpotential to recruit progenitorcells
– Strong proliferative potential
– Necessitates a carrier system– No specific function in
periodontal regeneration
Bone MorphogeneticProteins
– Growth factor with the strongestpotential to regenerate alveolarbone
– Also some potential to recruitmesenchymal progenitor cells andinduce cell proliferation
– Strong tendency to causeankylosis
– Lack of clinical trialsdemonstrating any use inperiodontal regeneration
Platelet Rich Plasma andFibrin
– Supernatural concentration ofgrowth factors
– Autologous source– Used for a variety of procedures
and easily obtainable
– PRP contains anticoagulants– Typically requires the use of a
bone grafting material to maintainvolume
Growth andDifferentiation Factor-5
– Recently demonstrated clinicalsafety and efficacy
– Histologically shown to improveperiodontal regeneration
– Less known about its mode ofaction
– Need for more clinical trialsdemonstrating its validity
carry properties necessary for the repair andregeneration of various tissues found in theoral cavity, very few possess the potential topromote blood supply/angiogenesis directlyto damaged tissues.
Wound healing has therefore previouslybeen characterized as a four-stage processwith overlapping phases [7–9]. What is note-worthy is the fact that platelets have beendescribed as key components affecting theearly phases of tissue regeneration impor-tant during hemostasis and fibrin clot forma-tion [6]. Platelets have also been shown tosecrete a number of important growth fac-tors including platelet-derived growth fac-tor (PDGF), vascular endothelial growth
factor (VEGF), coagulation factors, adhe-sion molecules, cytokines/chemokines, anda variety of other angiogenic factors capableof stimulating the proliferation and activa-tion of cells involved in the wound healingprocess including fibroblasts, neutrophils,macrophages, and mesenchymal stem cells(MSCs) [11].
Interestingly, in the mid- to late 1990s, twoseparate strategies were adopted to regen-erate human tissues based on these con-cepts. First, the main growth factor secretedfrom platelets (PDGF) was commercializedinto a recombinant growth factor (rhPDGF-BB). This has since been FDA-approved forthe regeneration of numerous tissues in the

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin in Regenerative Dentistry
human body including intrabony defects inthe field of periodontology. A second strategywas proposed around the same time to col-lect supra-physiological doses of platelets byutilizing centrifugation. Since blood is natu-rally known to coagulate within minutes, theadditional use of anti-coagulants was addedto this process to maintain a liquid consis-tency of blood throughout this procedure. Apositive correlation between platelet countand the regenerative phase was thereforeobserved for tissue wound healing. In fact, ithas also been shown that the simple combi-nation of bone grafting materials with bloodalone is known to enhance angiogenesis andnew bone formation of bone grafts whencompared to implanted bone grafts alone thatare not pre-coated [12]. Based on these find-ings, several research groups across manyfields of medicine began in the 1990s to studythe effects of various platelet concentratesfor tissue wound healing by adapting variouscentrifugation techniques and protocols withthe aim of improving tissue regeneration.
. Brief history of plateletconcentrates
It is interesting to point out that the useof platelet concentrates have dramaticallyincreased in popularity over the past decadesince the discovery of PRF. Despite this, itis important to understand that growth fac-tors derived from blood had been used inmedicine for over two decades [13]. Thesefirst attempts to use concentrated plateletgrowth factors was derived from the fact thatsupra-physiological doses could be obtainedfrom platelets to promote wound healingduring and following surgery [14,15]. Theseconcepts were later established into what isnow known as “platelet rich plasma” (PRP),which was later introduced in the 1990sin dentistry with leading clinician-scientistssuch as Whitman and Marx [16,17]. Themain goal of PRP was to isolate the highestquantity of platelets and ultimately growth
factors associated with their collection andre-use them during surgery. Typical pro-tocols ranged in time from 30 minutes tomore than 1 hour based on their respectivecollection methods. It has been well docu-mented that their formulation contains over95% platelets; cells having a direct effecton osteoblasts, connective tissue cells, peri-odontal ligament cells and epithelial cells[18,19].
Despite the growing success and use ofPRP in the initial years following its launch,there were several reported limitations thatprevented its full potential. The techniqueitself was lengthy and therefore required theadditional use of anti-coagulant factors toprevent clotting using bovine thrombin orCaCl2, both known inhibitors of wound heal-ing. These drawbacks in combination withthe lengthy harvesting/centrifugation prepa-ration times were then frequently being uti-lized in large maxillofacial surgeries, whereasthe typical dental or medical practitioner wasresistant to its use due to lengthy preparationtimes.
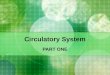
One of the other drawbacks of PRP was thefact that it was liquid by nature, and there-fore required its combination with other bio-materials including bone grafts derived fromhuman cadavers (allografts) or animal prod-ucts (xenografts), thereby further combin-ing its use with other “unnatural” products.Interestingly, very recent data from withinour laboratories has pointed to the quick“burst” release of growth factors from PRP(Figure 1.2) [20]. It has since been suggestedthat a preferential release of growth factorsmay be obtained by a more slowly-releasingcurve over time as opposed to a quick andshort burst as found using PRP [20–22].
In summary, the combination of several ofthese limitations has forced others to inves-tigate new modalities for successful regen-eration. From this perspective, a second-generation platelet concentrate, without theuse of anti-coagulants, was therefore devel-oped with shorter preparation times termedplatelet rich fibrin (PRF) [23]. During thisharvesting procedure, many of the cells

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
1 Platelet Rich Fibrin
8000
6000
4000
2000
015 min
****
**** **
60 min
PD
GF-
AB
acc
umul
ated
prot
ein
over
tim
e-pg
/mL
8 hrs 1 day 3 days 10 days
L-PRFPRP
A-PRF
Figure . Growth factor release of PDGF-AB from A-PRF, L-PRF, and PRP. Notice the initial burst of growthfactor increase from PRP; however, after a 10-day period, significantly higher growth factors are released fromA-PRF. (∗∗ signifies p<0.01). Source: Kobayashi et al. 2016 [20]. Reproduced with permission of Springer.
(which now include additional leukocytes)were trapped within the fibrin matrix alongwith growth factors [24]. PRF (which waslater renamed leukocyte PRF or L-PRF dueto its additional leukocyte content) contains avariety of cells, which have individually beenstudied for their role in the regeneration pro-cess later described throughout this book.
. The development of PRFfrom PRP
In the early 2000s, the focus of researchin the Pain Clinic in Nice, France was totry and solve blood-flow–related issues tolarge ulcers often leaving patients with largechronic wounds that potentially resulted inamputation. At the time, certain researchgroups were suggesting that PRP, whichwas mainly utilized as a supra-physiologicaldose of blood-derived growth factors, couldenhance wound healing. Despite this, a desireto develop a new platelet concentrate withoutthe use of anti-coagulants (known inhibitorsof wound healing) was a primary objec-tive. With these concepts in mind, furtherresearch in the early 2000s was undertakento develop what is now known as a second-generation platelet concentrate withoututilizing anti-coagulation factors [23]. Theprotocol was developed using a simpler cen-trifugation protocol requiring only 1 cycle of12 minutes at 2700 rpm (750 g). The original
objective was to spin at high centrifugationspeeds in order to phase separate the layersbetween the red corpuscle base and theoverlaying clear liquid containing leukocytesand plasma. As no anti-coagulants wereutilized, the resultant formulation came witha three-dimensional fibrin scaffold termedPRF [25–27]. PRF has now been highlyresearched with over 500 publications on itstopic, many of which are discussed withinthis textbook.
Additional research from various groupsaround the world have since shown themarked impact of white blood cells foundwithin the fibrin matrix and their involve-ment in the wound healing process. Forthese reasons, an improved defense to for-eign pathogens has been observed whensurgery is performed with PRF leading tothe more favorable clinical results resultingin lower infection rates [28–33]. Addition-ally, macrophages and neutrophils containedwithin PRF are naturally one of the first cellsfound within infected wounds. For these rea-sons, the use of PRF during surgery increasestheir numbers at the initial stages of healingthereby playing a central role in the phagocy-tosis of debris, microbes and necrotic tissues,as well as directing the future regeneration ofthese tissues through release of cytokines andgrowth factors.
Three main components of PRF havebeen noted as being key components assist-ing in tissue regeneration. As illustrated inFigure 1.3, PRF not only contains host cells,

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin in Regenerative Dentistry
Figure . Three main components of PRF include 1) cell types (platelets, leukocytes, and red blood cells), 2) aprovisional extracellular matrix three-dimensional scaffold fabricated from autologous fibrin (includingfibronectin and vitronectin) and 3) a wide array of over 100 bioactive molecules including most notably PDGF,VEGF, IGF, EGF, TGF-beta, and BMP2. Source: Miron et al. 2016 [54]. Reproduced with permission of Elsevier.
but also contains a three-dimensional fib-rin matrix containing various growth fac-tors. These include transforming growthfactor beta (TGF-beta), PDGF and VEGF,insulin growth factor (IGF), and epidermalgrowth factor (EGF). Recent research hasmore specifically shown how leukocytes (asopposed to platelets) are the main implica-tors in the tissue wound healing process capa-ble of further enhancing new blood vessel for-mation (angiogenesis) and tissue formation[25–27, 30, 34].
It is also important to note that PRF hasnot solely been utilized in dentistry andmuch research has been dedicated to itsuse in various other fields of medicine.Recently, PRF has shown effectiveness forthe clinical management of hard-to-heal legulcers including diabetic foot ulcers, venousleg ulcers, and chronic leg ulcers [35–39].Furthermore, PRF has had positive outcomesfor hand ulcers [40], facial soft tissue defects
[41], laparoscopic cholecystectomy [42],deep nasolabial folds, volume-depletedmidfacial regions, facial defects, superficialrhytids, and acne scars [43]. Its use hasalso been extended toward the induction ofdermal collagenesis [44], vaginal prolapserepair [45], urethracutaneous fistula repair[46,47], lipostructure surgical procedures[48], chronic rotator cuff repair [49], andacute traumatic ear drum perforation healing[50]. It goes without further mention thatby increasing blood flow to defect sites fromvarious etiology, favorable wound healingand tissue regeneration may take place. Wenow know that PRF serves all three impor-tant criteria for tissue regeneration including1) serving as a three-dimensional fibrinscaffold, 2) includes autologous cells such asleukocytes, macrophages, neutrophils, andplatelets, and 3) serves as a reservoir of natu-ral growth factors that may be released overa 10- to 14-day period. Research has now

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
1 Platelet Rich Fibrin
demonstrated that each of these three indi-vidual components of tissue regeneration areimportant during wound healing with PRF.
1. Major cell types in PRFThe aim of this introductory chapter isnot to introduce the important cell-typesfound in PRF. This will be described laterin Chapter 2. However, it is importantto note that PRF contains a numberof cells including platelets, leukocytes,macrophages, granulocytes, and neu-trophils. Following the centrifugationcycle, the majority of these cells aretrapped within the three-dimensionalfibrin matrix. As stated previously, theaddition of blood alone to bone bio-materials has been shown to drasticallyimprove wound angiogenesis [12]. Oneof the main differences between PRF andpreviously utilized PRP is the incorpora-tion of leukocytes in PRF. Several studieshave shown their key importance duringanti-infectious pathogen resistance aswell as their implications in immuneregulation [51–53]. Furthermore, theyplay a significant role during host tissue-to-biomaterial integration [31,33,54]. Dueto the added benefits of leukocytes, it isnot surprising to learn that extractionof third molars have specifically shownup to a 10-fold decrease in osteomyelitisinfections as well as greater wound healing
following simple placement of PRF intoextraction sockets [55]. Therefore, theinfluence of autologous cells containedwithin PRF, most noteworthy leukocytes,should be considered a major advantageduring regenerative therapy.
2. A natural fibrin matrix and its biologicalpropertiesA second major difference between PRFand PRP as previously mentioned is thelack of anti-coagulants thus resulting in afibrin matrix (Figure 1.4). Naturally with-out anti-coagulants blood will clot andfor these reasons, centrifugation musttake place immediately following bloodcollection. Initial protocols were estab-lished whereby 10-mL of blood was col-lected and centrifuged for 12 minutes at2700 rpm (750g). In Chapter 3, the biolog-ical concept of utilizing lower centrifuga-tion speeds and time will be discussed.
Nevertheless, what was once thoughtto be simply a carrier for growth factorsand cells, the fibrin matrix has since beenshown to be a main feature of PRF. ThePRF matrix acts as a key component of tis-sue wound healing as highlighted in morescientific detail in Chapter 2.
3. Cytokines contained within PRFThe third primary advantage of PRF isthe fact it contains natural growth factorsfound in blood. While their individualbiological roles will be explained in the
Acellular Plasma (PPP)
Fibrin Clot (PRF)
Red corpuscules base
Figure . Platelet Rich Fibrin (PRF) clot formed in the upper third of glass tubes after centrifugation.

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin in Regenerative Dentistry
following chapter, PRF contains TGF-beta, a known agent responsible forthe rapid proliferation of various celltypes found in the oral cavity [56,57].Its other major growth factor is PDGF,an essential regulator for the migration,proliferation, and survival of mesenchy-mal cells. A third important growthfactor in PRF is VEGF responsible forangiogenesis and future blood flow todamaged tissues [58]. Other growthfactors are epidermal growth factor andinsulin-like growth factor, both regulatorsof the proliferation and differentiationof many cells types later described inChapter 2.
The combination of 1) host cells, 2)a three-dimensional fibrin matrixand 3) growth factors containedwithin PRF act to synergisticallyenhance faster and more potenttissue wound healing and regene-ration.
. Effect of PRF on periosteumbehavior
Following years of practice with the use ofPRF, one biological property observed withalmost every surgical technique has been itsstimulation of the capacity of blood supplywithin the periosteum. From this point ofview, direct contact of PRF with periosteumsubstantially improves the blood supply tothe keratinized soft tissue favoring its thick-ness, as well as improves blood supply to theunderlying bone tissues. This has been oneof the key activities of PRF, whereby stimu-lation with growth factors over a long periodof release.
. The first case treated with PRF
The most appropriate way to conclude thisfirst chapter is by introducing the concept of
PRF utilized in regenerative medicine in thefirst years. Leg ulcers are a common reportedproblem in diabetic patients often resulting inamputation. In my pain clinic, a patient withobvious skin necrosis caused by Lyell syn-drome with repeated failed antibiotic treat-ment was referred to me (Figure 1.5). Fromthis perspective, patients were often directedto my pain clinic in Nice, France to receivetreatment for pain. Over the years, sci-ence has shown that infection was often asecondary problem to poor blood supply.Therefore, to improve treatment outcomes,attempts were being made to see if PRFfibrin clots could be utilized to regeneratethese defects (Figure 1.6). The idea was thatby introducing supra-physiological doses ofgrowth factors from blood, one could poten-tially re-introduce blood flow into these tis-sues. To our great interest, wounds that wereinitially covered with PRF and plastic “Saran”wrap began to heal in as early as 10 days,and infection had disappeared. By 30 days,great clinical improvements could be visu-alized and this was achieved utilizing PRFalone even in the absence of antibiotics (Fig-ure 1.7). Similar clinical outcomes could alsobe observed following foot amputation whereresulting wounds were extremely difficult toheal. The application of PRF alone couldre-introduce blood flow into these defects,improving significantly tissue regeneration(Figures 1.8 and 1.9). Most interesting isat which point the body’s natural abilityproves to treat these defects in a physiolog-ical way with 100% naturally derived humanblood.
Following these early treatments, it wasobvious that the potential for PRF to be uti-lized across many fields of medicine wasclear. The concept was later introduced tothe dental field where a much larger num-ber of regenerative procedures could be per-formed on a yearly basis. From there, expertclinicians have attempted to use PRF in vari-ous regenerative procedures in dentistry laterdiscussed in this textbook and the field hasbeen expanding ever since.

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
1 Platelet Rich Fibrin
Figure . Patient presenting to the Pain Clinic in Nice, France with Lyell syndrome. Antibiotic therapy in suchcases is not always effective (Case performed by Dr. Joseph Choukroun).
Figure . Patient from Figure 1.5 with Lyell syndrome treated with PRF. PRF membranes were placed on thedefects, wrapped in a plastic wrap, and allowed to heal without use of antibiotic therapy (Case performed byDr. Joseph Choukroun).

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin in Regenerative Dentistry
Figure . Patient from Figures 1.5 and 1.6 with Lyell syndrome treated with PRF. After 10 and 30 days of healing,notice the marked improvement in tissue revascularization and wound healing (Case performed by Dr. JosephChoukroun).
Figure . Diabetic foot amputation with infection after 15 days. Right photo demonstrates PRF clots that areapplied to the wound (Case performed by Dr. Joseph Choukroun).

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
1 Platelet Rich Fibrin
Figure . Diabetic foot amputation (patient from Figure 1.8) following 7 and 30 days of healing (Caseperformed by Dr. Joseph Choukroun).
. Conclusion
The use of PRF has seen a large and steadyincrease in popularity since it was firstintroduced in medicine for the treatment ofhard-to-heal leg ulcers and wounds. Whiledescribed as a second-generation plateletconcentrate, one of the main advantages ofPRF is the fact that it is produces withoutuse of anti-coagulants or other unnaturalby-products that prevent the coagulationcascade and is therefore considered 100%
autologous and natural. While PRF con-tains three important aspects for tissuewound healing, including 1) host cells, 2) athree-dimensional fibrin matrix, and 3) accu-mulation of growth factors, its synergisticeffects has frequently been recognized indentistry most notably for the healing of softtissues. Future strategies to improve PRFformulations and techniques are continu-ously being investigated to further enhancethe clinical outcomes following regenerativeprocedures utilizing this technology.
References
Coury AJ. Expediting the transition fromreplacement medicine to tissueengineering. Regenerative biomaterials.2016;3(2):111–3.
Dai R, Wang Z, Samanipour R, Koo KI,Kim K. Adipose-Derived Stem Cells forTissue Engineering and RegenerativeMedicine Applications. Stem cellsinternational. 2016;2016:6737345.
Rouwkema J, Khademhosseini A.Vascularization and Angiogenesisin Tissue Engineering: Beyond CreatingStatic Networks. Trends Biotechnol.2016.
Zhu W, Ma X, Gou M, Mei D, Zhang K,Chen S. 3D printing of functionalbiomaterials for tissue engineering.Current opinion in biotechnology.2016;40:103–12.
Upputuri PK, Sivasubramanian K, MarkCS, Pramanik M. Recent developments invascular imaging techniques in tissueengineering and regenerative medicine.BioMed research international. 2015;2015:783983.
Guo S, Dipietro LA. Factors affectingwound healing. J Dent Res. 2010;89(3):219–29.
Gosain A, DiPietro LA. Aging and woundhealing. World journal of surgery.2004;28(3):321–6.
Eming SA, Brachvogel B, Odorisio T, KochM. Regulation of angiogenesis: woundhealing as a model. Progress inhistochemistry and cytochemistry.2007;42(3):115–70.
Eming SA, Kaufmann J, Lohrer R, Krieg T.[Chronic wounds. Novel approaches in

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin in Regenerative Dentistry
research and therapy]. Der Hautarzt;Zeitschrift fur Dermatologie, Venerologie,und verwandte Gebiete. 2007;58(11):939–44.
Zhang Y, Zhang X, Shi B, Miron R.Membranes for guided tissue and boneregeneration. Annals of Oral &Maxillofacial Surgery. 2013;1(1):10.
Nurden AT. Platelets, inflammation andtissue regeneration. Thrombosis andhaemostasis. 2011;105 Suppl 1:S13–33.
Barbeck M, Najman S, Stojanovic S, MiticZ, Zivkovic JM, Choukroun J, et al.Addition of blood to a phycogenic bonesubstitute leads to increased in vivovascularization. Biomedical materials(Bristol, England). 2015;10(5):055007.
de Vries RA, de Bruin M, Marx JJ, Hart HC,Van de Wiel A. Viability of plateletscollected by apheresis versus theplatelet-rich plasma technique: a directcomparison. Transfusion science. 1993;14(4):391–8.
Anfossi G, Trovati M, Mularoni E,Massucco P, Calcamuggi G, Emanuelli G.Influence of propranolol on plateletaggregation and thromboxane B2production from platelet-rich plasma andwhole blood. Prostaglandins, leukotrienes,and essential fatty acids. 1989;36(1):1–7.
Fijnheer R, Pietersz RN, de Korte D,Gouwerok CW, Dekker WJ, Reesink HW,et al. Platelet activation during preparationof platelet concentrates: a comparison ofthe platelet-rich plasma and the buffy coatmethods. Transfusion. 1990;30(7):634–8.
Whitman DH, Berry RL, Green DM.Platelet gel: an autologous alternative tofibrin glue with applications in oral andmaxillofacial surgery. Journal of oral andmaxillofacial surgery. 1997;55(11):1294–9.
Marx RE, Carlson ER, Eichstaedt RM,Schimmele SR, Strauss JE, Georgeff KR.Platelet-rich plasma: growth factorenhancement for bone grafts. Oral Surgery,Oral Medicine, Oral Pathology, OralRadiology, and Endodontology. 1998;85(6):638–46.
Jameson C. Autologous plateletconcentrate for the production of plateletgel. Lab Med. 2007;38:39–42.
Marx RE. Platelet-rich plasma: evidence tosupport its use. Journal of oral andmaxillofacial surgery : official journal of theAmerican Association of Oral andMaxillofacial Surgeons. 2004;62(4):489–96.
Kobayashi E, Fluckiger L,Fujioka-Kobayashi M, Sawada K, SculeanA, Schaller B, et al. Comparative release ofgrowth factors from PRP, PRF, andadvanced-PRF. Clinical oral investigations.2016.
Lucarelli E, Beretta R, Dozza B, Tazzari PL,O’Connel SM, Ricci F, et al. A recentlydeveloped bifacial platelet-rich fibrinmatrix. European cells & materials. 2010;20:13–23.
Saluja H, Dehane V, Mahindra U. PlateletRich fibrin: A second generation plateletconcentrate and a new friend of oral andmaxillofacial surgeons. Annals ofmaxillofacial surgery. 2011;1(1):53–7.
Choukroun J, Adda F, Schoeffler C,Vervelle A. Une opportunite enparo-implantologie: le PRF.Implantodontie. 2001;42(55):e62.
Dohan Ehrenfest DM, Del Corso M, DissA, Mouhyi J, Charrier JB.Three-dimensional architecture and cellcomposition of a Choukroun’s platelet-richfibrin clot and membrane. Journal ofperiodontology. 2010;81(4):546–55.
Choukroun J, Diss A, Simonpieri A, GirardMO, Schoeffler C, Dohan SL, et al.Platelet-rich fibrin (PRF): asecond-generation platelet concentrate.Part IV: clinical effects on tissue healing.Oral surgery, oral medicine, oral pathology,oral radiology, and endodontics. 2006;101(3):e56–60.
Dohan DM, Choukroun J, Diss A, DohanSL, Dohan AJ, Mouhyi J, et al. Platelet-richfibrin (PRF): a second-generation plateletconcentrate. Part I: technological conceptsand evolution. Oral surgery, oral medicine,oral pathology, oral radiology, andendodontics. 2006;101(3):e37–44.

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
1 Platelet Rich Fibrin
Dohan DM, Choukroun J, Diss A, DohanSL, Dohan AJ, Mouhyi J, et al. Platelet-richfibrin (PRF): a second-generation plateletconcentrate. Part II: platelet-relatedbiologic features. Oral surgery, oralmedicine, oral pathology, oral radiology,and endodontics. 2006;101(3):e45–50.
Martin P, Leibovich SJ. Inflammatory cellsduring wound repair: the good, the bad andthe ugly. Trends in cell biology. 2005;15(11):599–607.
Tsirogianni AK, Moutsopoulos NM,Moutsopoulos HM. Wound healing:immunological aspects. Injury. 2006;37Suppl 1:S5–12.
Adamson R. Role of macrophages innormal wound healing: an overview.Journal of wound care. 2009;18(8):349–51.
Davis VL, Abukabda AB, Radio NM,Witt-Enderby PA, Clafshenkel WP,Cairone JV, et al. Platelet-rich preparationsto improve healing. Part I: workableoptions for every size practice. The Journalof oral implantology. 2014;40(4):500–10.
Davis VL, Abukabda AB, Radio NM,Witt-Enderby PA, Clafshenkel WP, CaironeJV, et al. Platelet-rich preparations toimprove healing. Part II: platelet activationand enrichment, leukocyte inclusion, andother selection criteria. The Journal of oralimplantology. 2014;40(4):511–21.
Ghasemzadeh M, Hosseini E. Intravascularleukocyte migration through plateletthrombi: directing leukocytes to sites ofvascular injury. Thrombosis andhaemostasis. 2015;113(6):1224–35.
Dohan DM, Choukroun J, Diss A, DohanSL, Dohan AJ, Mouhyi J, et al. Platelet-richfibrin (PRF): a second-generation plateletconcentrate. Part III: leucocyte activation: anew feature for platelet concentrates? Oralsurgery, oral medicine, oral pathology, oralradiology, and endodontics. 2006;101(3):e51–5.
Danielsen P, Jorgensen B, Karlsmark T,Jorgensen LN, Agren MS. Effect of topicalautologous platelet-rich fibrin versus nointervention on epithelialization of donorsites and meshed split-thickness skin
autografts: a randomized clinical trial.Plastic and reconstructive surgery.2008;122(5):1431–40.
O’Connell SM, Impeduglia T, Hessler K,Wang XJ, Carroll RJ, Dardik H. Autologousplatelet-rich fibrin matrix as cell therapy inthe healing of chronic lower-extremityulcers. Wound repair and regeneration :official publication of the Wound HealingSociety [and] the European Tissue RepairSociety. 2008;16(6):749–56.
Steenvoorde P, van Doorn LP, Naves C,Oskam J. Use of autologous platelet-richfibrin on hard-to-heal wounds. Journal ofwound care. 2008;17(2):60–3.
Jorgensen B, Karlsmark T, Vogensen H,Haase L, Lundquist R. A pilot study toevaluate the safety and clinicalperformance of Leucopatch, an autologous,additive-free, platelet-rich fibrin for thetreatment of recalcitrant chronic wounds.The international journal of lowerextremity wounds. 2011;10(4):218–23.
Londahl M, Tarnow L, Karlsmark T,Lundquist R, Nielsen AM, Michelsen M,et al. Use of an autologous leucocyte andplatelet-rich fibrin patch on hard-to-healDFUs: a pilot study. Journal of wound care.2015;24(4):172–4, 6–8.
Chignon-Sicard B, Georgiou CA, Fontas E,David S, Dumas P, Ihrai T, et al. Efficacy ofleukocyte- and platelet-rich fibrin inwound healing: a randomized controlledclinical trial. Plastic and reconstructivesurgery. 2012;130(6):819e–29e.
Desai CB, Mahindra UR, Kini YK, BakshiMK. Use of Platelet-Rich Fibrin over SkinWounds: Modified Secondary IntentionHealing. Journal of cutaneous and aestheticsurgery. 2013;6(1):35–7.
Danielsen PL, Agren MS, Jorgensen LN.Platelet-rich fibrin versus albumin insurgical wound repair: a randomized trialwith paired design. Annals of surgery.2010;251(5):825–31.
Sclafani AP. Safety, efficacy, and utility ofplatelet-rich fibrin matrix in facial plasticsurgery. Archives of facial plastic surgery.2011;13(4):247–51.

JWST852-c01 JWST852-Miron July 26, 2017 8:18 Printer Name: Trim: 10in × 7in
Platelet Rich Fibrin in Regenerative Dentistry
Sclafani AP, McCormick SA. Induction ofdermal collagenesis, angiogenesis, andadipogenesis in human skin by injection ofplatelet-rich fibrin matrix. Archives offacial plastic surgery. 2012;14(2):132–6.
Gorlero F, Glorio M, Lorenzi P,Bruno-Franco M, Mazzei C. New approachin vaginal prolapse repair: mini-invasivesurgery associated with application ofplatelet-rich fibrin. Internationalurogynecology journal. 2012;23(6):715–22.
Soyer T, Cakmak M, Aslan MK, SenyucelMF, Kisa U. Use of autologous platelet richfibrin in urethracutaneous fistula repair:preliminary report. International woundjournal. 2013;10(3):345–7.
Guinot A, Arnaud A, Azzis O,Habonimana E, Jasienski S, Fremond B.Preliminary experience with the use of anautologous platelet-rich fibrin membranefor urethroplasty coverage in distalhypospadias surgery. Journal of pediatricurology. 2014;10(2):300–5.
Braccini F, Chignon-Sicard B, Volpei C,Choukroun J. Modern lipostructure: theuse of platelet rich fibrin (PRF). Revue delaryngologie-otologie-rhinologie.2013;134(4-5):231–5.
Zumstein MA, Rumian A, Lesbats V,Schaer M, Boileau P. Increasedvascularization during early healing afterbiologic augmentation in repair of chronicrotator cuff tears using autologousleukocyte- and platelet-rich fibrin (L-PRF):a prospective randomized controlled pilottrial. Journal of shoulder and elbowsurgery/American Shoulder and ElbowSurgeons [et al]. 2014;23(1):3–12.
Habesoglu M, Oysu C, Sahin S,Sahin-Yilmaz A, Korkmaz D, Tosun A, et al.Platelet-rich fibrin plays a role on healing of
acute-traumatic ear drum perforation. TheJournal of craniofacial surgery. 2014;25(6):2056–8.
Kawazoe T, Kim HH. Tissue augmentationby white blood cell-containing platelet-richplasma. Cell transplantation. 2012;21(2-3):601–7.
Perut F, Filardo G, Mariani E, Cenacchi A,Pratelli L, Devescovi V, et al. Preparationmethod and growth factor content ofplatelet concentrate influence theosteogenic differentiation of bone marrowstromal cells. Cytotherapy. 2013;15(7):830–9.
Pirraco RP, Reis RL, Marques AP. Effect ofmonocytes/macrophages on the earlyosteogenic differentiation of hBMSCs.Journal of tissue engineering andregenerative medicine. 2013;7(5):392–400.
Miron RJ, Bosshardt DD. OsteoMacs: Keyplayers around bone biomaterials.Biomaterials. 2016;82:1–19.
Hoaglin DR, Lines GK. Prevention oflocalized osteitis in mandibularthird-molar sites using platelet-rich fibrin.International journal of dentistry.2013;2013:875380.
Border WA, Noble NA. Transforminggrowth factor beta in tissue fibrosis. TheNew England journal of medicine. 1994;331(19):1286–92.
Bowen T, Jenkins RH, Fraser DJ.MicroRNAs, transforming growth factorbeta-1, and tissue fibrosis. The Journal ofpathology. 2013;229(2):274–85.
Shamloo A, Xu H, Heilshorn S.Mechanisms of vascular endothelialgrowth factor-induced pathfinding byendothelial sprouts in biomaterials. Tissueengineering Part A. 2012;18(3-4):320–30.