Embed Size (px)
Citation preview

British /ourno1 of Ho~mutoloq{, 1988, 68, 181-1 X 7
Platelet peroxidase-positive blast cells in transient myeloproliferative disorder with Down’s syndrome
J ~ J N K O S U D A , ’ MITSCJOKI E G U C H I , ’ TAKEBITMI OZAWA,’ TOSHIHARU F U R I J K A W A , ~ YASUHIDE HAY AS HI,^
A N D TOSHIO Sl lDA7 ‘The Second Department of Pediatrics, Dokkyo University School of Medicine, Tochigi-ken, ’Department of Hematology and Oncology, Saitama Children’s Medicul Center, Saitarna-ken, 3Department of I’ediufrics. Iapunese Red Cross Nagoya First Hospital, Nagoya. 4The Blood Transfusion Service, University of Tokyo, Tokyo, ’Department of Medicine und Physical Therapy, University of Tokyo, ‘Division of Hematology, Department of Mediciiw, lichi Medicul School, l’ochigi-ken. 71nstitutu of HtJrnutoiog!g, Jichi Medical School, Japan
S E I J I K O J I M A , 3 HIROO M A E D A , 4 K E N J I ‘ rADOKOR0, ’ YUKO SATO,’ YASUSADA MIIJRA,‘ AKIRA O H A R A 7
Krwiviid 19 May 1987; accepted for publicntion 20 August 1987
Summary. Transient myeloproliferative disorder accompa- nied by Down’s syndrome has been characterized as exhibit- ing self-limiting haematological abnormalities. We studied six patients suffering from this disorder in order to clarify the biological nature of their blast cells. Metaphases of leucocytes stimulated with phytohaemagglutinin (PHA) showed trisomy 2 1 in all patients except one. The exception was constitutionally trisomy 21 mosaic ( 4 6 , X Y = 89,’ 47,XY, + 2 1 = 1 1 ). However, metaphases from the peripheral blood cells (blast cells: 70%) without PHA stimulation showed exclnsively trisomy 2 I . Simultaneous examination for morphology and chromosomal analysis on single colonies revealed that granulocyte-macrophage (GM) colonies and a n erythroid colony contained only cells with the trisomy 2 1 karyotype.
In general, children and adolescents with Down’s syndrome appear to have a 10-30-fold increased incidence of leukae- mia (Robinson et al, 1984). In 1978, Breton-Gorius et a1 established the identity of megakaryoblastic acute leukaemia by an ultrastructural cytochemical study of platelet peroxi- dase localization. Since a report by Lewis (1981) , an association between megakaryoblastic lenkaemia and Down’s syndrome has been emphasized.
It has also been noted that transient myeloproliferative disorder. which can masquerade as congenital leukaemia, frequently occurs in Down’s syndrome neonates (Koss et al, 1963: Kosner 6; Lea, 1972). Transient myeloproliferative disorder is characterized by increased numbers of blast cells in the peripheral blood, but there is usually no anaemia,
Correspondence: I)r Junko Suda. The Second Department of Pedia- trics. Dokkyo University School of Medicine. Mibu, Tochigi-ken. 32 1-02, Japan.
The blast cells showed positive reactions for platelet peroxidase (PPO) and with monoclonal antibodies against platelet-megakaryocyte antigen (TP 80 and TI’ X2). In methylcellulose and liquid culture systems. high plating efficiencies were observed, and mainly mature basophils containing histamine developed in the presence of W A - stimulated leucocyte conditioned medium (PHA-LCM). Itr
vivo. mature neutrophils, basophils, eosinophils or mega- karyocytes coexisted with PPO-positive blast cells in the peripheral blood of some patients with this disorder.
These findings suggest that transient myeloproliferative disorder is characterized by a proliferation of PPO-positive blast cells with trisomy 2 1, although some heterogeneity may be seen.
neutropenia or thrombocytopenia. Furthermore. this dis- order is unique in that the haematological abnormality is self- limiting, though it has not yet been clarified whether it is due to a n abnormality in haemopoietic regulation.
In this paper, we studied six cases of transient myeloproli- ferative disorder in Down’s syndrome including one with trisomy 21 mosaic. The nature of the blast cells were characterized by ultrastructural cytochemical and immuno- logical studies using monoclonal antibodies directed against platelet glycoproteins. Proliferation and differentiation cap+ cities of blast cells were examined by in vitro culture methods. Sequential cytogenetic studies were also conducted in cells of the trisomy 21 mosaic case.
MATERIALS AND METHODS
Patients. Six patients in this study were diagnosed at the Hospital of Dokkyo University School of Medicine and other
181

182 Junk0 Suda et a1
hospitals between November 1985 and August 1986. Sam- ples of peripheral blood or bone marrow from patients were transferred at 4°C within 24 h.
Cytogenetic studies. Cytogenetic analyses with Q or trypsin Giemsa banding techniques were performed on peripheral blood cells obtained at the time of diagnosis with or without phytohaemagglutinin (PHA, Difco Laboratories. Detroit) stimulation. In case 1, bone marrow cells and skin fibroblasts were also examined in order to clarify the percentage of trisomy 2 1 mosaic cells. In each case, at least 20 metaphases were analysed. In cases 1 and 4, more than 30 metaphases were analysed. Analysis on single colonies was also carried out using the method described previously (Sato et al, 1986). The karyotypes were described according to the International System for Human Cytogenetic Nomenclature (ISCN. 19 78).
Cell culture. Peripheral blood mononuclear cells were separated by Ficoll-Paque (Pharmacia Fine Chemicals, Upp- sala, Sweden) density centrifugation; the interface cells were harvested and washed twice in Iscove’s modified Dulbecco’s medium (IMDM, Gibco, Grand Island, NY).
Methylcellulose culture was performed in 3 5-mm non- tissue culture dishes (Falcon, Oxnard, Calif.). A 1 ml of mixture of various concentration of peripheral blood mono- nuclear cells, IMDM, 1.2% methylcellulose (Dow Chemical Co., Midland, Mich.), 30% platelet poor plasma (PPP), 1% bovine serum albumin (BSA, Sigma Chemical Co., St Louis), 1 unit of erythropoietin (Toyobo, Osaka, Japan) and 5% PHA- LCM was incubated at 3 7°C in a humidified atmosphere of 5% CO, in air. PHA-LCM was prepared as described previously (Suda et al, 1985).
Liquid culture was carried out as follows: cells were suspended in IMDM with 5% PHA-LCM and 10% fetal calf serum (FCS). They were incubated at 1 x 105/ml in 2 5 cml tissue culture flasks (Corning Glass. Corning, N.Y .) at 3 7°C in a humidified atmosphere of 5% C 0 2 in air. Half of the culture medium was replaced once or twice a week with freshly prepared medium. The histamine content of liquid cultured cells in case 3 was measured by the method described previously (Suda P t a / , 1985). Histamine release following the stimulation with the calcium ionophore A2 3 1 87, compound 48/80 and formyl-L-methionyl-leucyl-L-phenylalanine (FMLP) was also examined.
Cytochemical studies. Cells were stained for alkaline phos- phatase and peroxidase activities, and with Sudan black B,
periodic acid Schiff and toluidine blue stains. Non-specific esterase and chloroacetate esterase stainings were performed by the method described by Yam et a1 (1981).
Electron microscopic studies. Ultrastructural studies were performed on fresh peripheral blood cells of all cases. The cells were divided into two aliquots, one of which was fixed with glutaraldehyde for subsequent ultrastructural morphological and myeloperoxidase examination. The other cell portion was fixed in a mixture of paraformaldehyde, glutaraldehyde and tannic acid for detection of platelet peroxidase activity as described by Breton-Gorius & Guichard (1972). All speci- mens were post-fixed with osmium tetroxide, dehydrated and processed into epoxy resin for transmission electron micros- COPY.
Immunological studies. Reactivity of the peripheral mono- nuclear cells with murine monoclonal antibodies (TP 80 and TP 82) was assayed by an indirect immunofluorescence technique. TP 80 reacts only with platelets and megakaryo- cytes except those with Glanzmann’s thrombasthenia. The specificity of TP 80 binding to glycoprotein IIb/III, has been confirmed (Higashihara et al, 198 5 ) . TP 82 binds to platelets, megakaryocytes and common acute lymphoblastic leukae- mia cells. TP 82 indices platelet aggregation by binding on the platelet membrane (Sato et al, 1986).
Fluorescein isothiocyanate (F1TC)-conjugated goat anti- mouse globulin serum (Cooper Biochemical, Inc., Malvern. Pa.) was used at a dilution of 1:20. Fluorescence was examined with a Nikon optiphot microscope equipped with epi-fluorescence attachments.
KESULTS
Clinical and laboratory data The haematological profiles are summarized in Table I. ‘The patients’ age at the time of diagnosis of transient myeloproli- ferative disorder ranged from 0 to 15 d. All showed hepatosplenomegaly. Neither severe infection nor haemoly- sis was observed in any case. The male/female ratio was 4/2. Leucocyte counts ranged from 31 x 1 Oy to 180 x IOy/l, and the percentage of blast cells in peripheral blood ranged from 24%) to 74%). In all cases, the percentage of blast cells in bone marrow was lower than that in peripheral blood. The duration of the presence of blast cells in peripheral blood ranged from 1 to 8 weeks. Two cases are still alive and the
Table 1. Haernatological profile of the patients with transient rnyeloprolif’erative disorder
Age WBC Blasts RBC Hb Hct’ Ret’ Fb13 Plt4 Cdse Sex (d) ( x 10q/l) (y)) ( x 1O1*/I) (g/dl) (x,) (y,) ( / I 0 0 WBC) ( x 1 Oy/l) Uurdtion’ Comments
1 T K M 0 101 70 296 1 2 1 3 8 1 4 6 9 80 8 wk Alive Eosinophilia 2 H T M 0 64 6 74 530 1 7 3 5 1 8 1 0 0 403 46 d Alive 3 0 J M 15 8 2 1 45 532 1 8 h 3 5 259 2 6 d Dead 4 F H F 2 180 24 406 1 5 6 45 5 X O 32 281 1 7 d Dedd 5 I A F 7 160 45 472 1 5 5 4 7 0 7 2 6 1075 4 wk Dead Thrornbocythaemia 6 r Y M 0 31 40 575 2 0 0 6 4 5 7 0 260 4 wk Dead Basophilia
~ ~~
Haematocrit Reticolocyte count Crythroblast count on the smear of peripheral blood Platelet count Duration of the presence of blast cells
Transient Myeloproliferative Disorder 18 3
5 0 loo Days
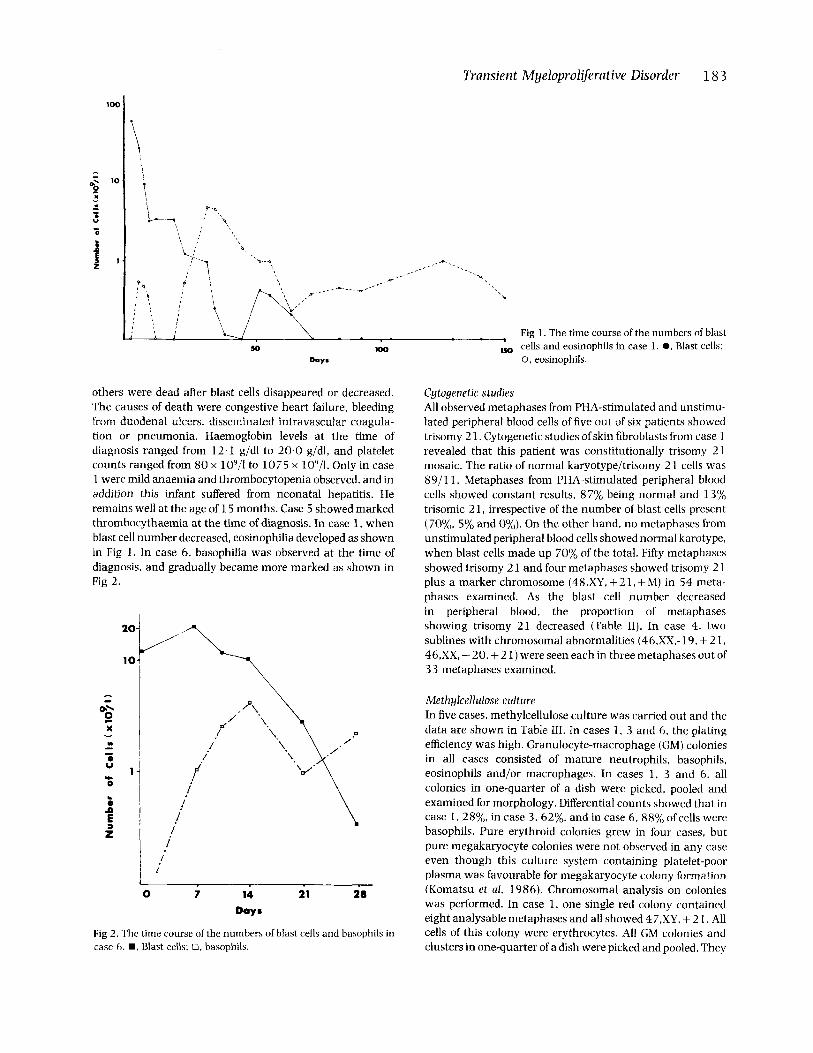
others were dead after blast cells disappeared or decreased. The causes of death were congestive heart failure, bleeding from duodenal ulcers, disseminated intravascular coagula- tion or pneumonia. Haemoglobin levels at the time of diagnosis ranged from 12.1 g/dl to 20.0 g/dl, and platelet counts ranged from 80 x 10y/l to 1075 x l O Y / l . Only in case 1 were mild anaemia and thrombocytopenia observed, and in addition this infant suffered from neonatal hepatitis. He remains well at the age of 1 5 months. Case 5 showed marked thrombocythaemia at the time of diagnosis. In case 1, when blast cell number decreased, eosinophilia developed as shown in Fig 1. In case 6. basophilia was observed at the time of diagnosis. and gradually became more marked as shown in Fig 2.
- - I
I
0 7 14 21 28 Days
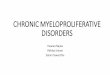
Fig 2 . The time course of the numbers of blast cells and basophils in case 6. W , Blast cells: 0. basophils.
--. .- ..
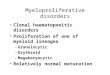
Fig 1. The time course of the numbers of blast :w cells and eosinophils in case 1 . 0. Blast cells:
0, eosinophils.
Cytogenetic studies All observed metaphases from PHA-stimulated and unstimu- lated peripheral blood cells of five out of six patients showed trisomy 2 1 . Cytogenetic studies of skin fibroblasts from case 1 revealed that this patient was constitutionally trisomy 2 1 mosaic. The ratio of normal karyotype/trisomy 2 1 cells was 89/11. Metaphases from PHA-stimulated peripheral blood cells showed constant results, 87% being normal and 13% trisomic 2 1, irrespective of the number of blast cells present (70%. 5% and 0%). On the other hand, no metaphases from unstimulated peripheral blood cells showed normal karotype, when blast cells made up 70% of the total. Fifty metaphases showed trisomy 2 1 and four metaphases showed trisomy 2 1 plus a marker chromosome (48,XY, + 2 1 , + M) in 54 meta- phases examined. As the blast cell number decreased in peripheral blood, the proportion of metaphases showing trisomy 21 decreased (Table 11). In case 4 , two sublines with chromosomal abnormalities (46,XX,-19, + 2 1 , 46,XX, - 20, + 2 1) were seen each in three metaphases out of 3 3 metaphases examined.
Methylcellulose culture In five cases, methylcellulose culture was carried out and the data are shown in Table 111. In cases 1 , 3 and 6 , the plating efficiency was high. Granulocyte-macrophage (GM) colonies in all cases consisted of mature neutrophils, basophils, eosinophils and/or macrophages. In cases 1, 3 and 6, all colonies in one-quarter of a dish were picked, pooled and examined for morphology. Differential counts showed that in case 1. 28%. in case 3 , 62%. and in case 6, SS(j0 of cells were basophils. Pure erythroid colonies grew in four cases, but pure megakaryocyte colonies were not observed in any case even though this culture system containing platelet-poor plasma was favourable for megakaryocyte colony formation (Komatsu et a/. 1986). Chromosomal analysis on colonies was performed. In case 1. one single red colony contained eight analysable metaphases and all showed 47,XY. + 2 1. All cells of this colony were erythrocytes. All GM colonies and clusters in one-quarter of a dish were picked and pooled. They

184 Junk0 Suda et a1 Table 11. Cytogenetic studies in case 1
Source (total number of metaphases)
0 0
37 52
100 144 1 5 5
PHA-stimulated peripheral blood (1 00) IJnstimulated peripheral blood (54) Unstimulated bone marrow (1 7) PHA-stimulated peripheral blood (50) Unstimulated bone marrow (50) Skin fibroblasts ( 1 00) PHA-stimulated peripheral blood (9 7)
70 87 70 0
4 64 5 8 7 1 94
~ 89 0 8 7
47,XY. + 2 1 48,XY. + 21, + M (%I (%)
13 0 93 7 36 0 1 3 0
6 0 11 0 1 3 0
Table Ill. Colony formation in methylcellulose culture
Cell no. Case per dish
1 1x103 2 5~ 104 3 1x104
6 I 104
4 1 x l o 4 5 N.D.
GM colonies -~
24f 3 3 f l
200f 36 20+ 5
N.D. 328 f 8
Erythroid Mixed bursts colonies
2 f l 0 6 f 2 0 I f 1 0 I + I l i l N.D. N . D . 0 0
Peripheral blood mononuclear cells were plated and colonies were counted on the 10th or 12th day of culture. Mixed colonies refers to colonies con- taining myeloid and erythroid lineages. N.U. =not done.
contained 24 analysable metaphases and all showed 47,XY, + 2 1. These cells were mature neutrophils. basophils and macrophages. A normal karyotype was not observed in any colony.
Liquid culture Liquid culture in the presence of PHA-LCM was performed in four cases. In case 1, megakaryocytes and basophils were observed on the sixth day of culture. In case 2, the cell number increased eight-fold during a 7 d culture period, all cells remaining blastic. After then, however, the cells degen- erated. In case 3, the cell number increased 10-fold during the same period. On the seventh day of culture, the cells were mononuclear and had large basophilic granules. On the 1 1 th day the nucleus was segmented, and 70% of cells were toluidine blue positive. These cells contained 2.8 pg/cell histamine which could be released by stimulation with the ionophore A23 187 or chemical agents, compound 48/80 and FMLP. In blast cells the histamine content was less than 0.01 pg/cell. In case 4, basophils. megakaryocytes and blast cells were observed on the seventh day of culture.
Morphological and cytochemical studies Mononuclear cells separated by Ficoll-Paque density centri- fugation from all cases but no. 6 consisted of more than 90%
blast cells. These had large nuclei with a few nucleoli and basophilic cytoplasm. Specific stainings for dual esterase, alkaline phosphatase and peroxidase, and with Sudan black B, periodic acid Schiff were negative in the blast cells in all cases. In cases 2 , 4 and 5, some blast cells had pseudopods. In case 6 . 30% mononuclear cells contained large basophilic granules.
Ult rust r uc t ural studies In all cases except no. 6.90% of the mononuclear cells were blastic, with round indented nuclei. Small mitochondria and moderately developed endoplasmic reticulum were observed in the extensive cytoplasm. They lacked granules except for a few which had a small number of large basophil-like or very small granules (Fig 3A). Blast cells were positive for PPO reaction in all cases, although the percentage was exception- ally low in case 6 (Table IV). PPO reaction was observed in the nuclear envelope and endoplasmic reticulum but not in the Golgi apparatus (Fig 3B). Myeloperoxidase was not detected in the blast cells. In case 1 , 7% of mononuclear cells showed demarcation membranes and small granules (Fig 3C). I n case 6, 30% of mononuclear cells had large amor-
Table IV. Characteristics of the blast cells
PPO’ Case ((g)
1 70 2 61 3 48 4 72 5 78 6 2
~~
TP80’ TP82’ (%) (%)
30 30 N.D. N.D. 44 70 40 40 60 60 16 48
~~
N.D.: not done. ’ Platelet peroxidase reaction
was examined by electron micro- scopic studies. ’ Activity for monoclonal antibodies was as- sayed by indirect immunofluores- cence technique.
Transient ~ ~ e l o ~ r o l ~ e r a ~ ~ v e Disorder 18 5
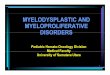
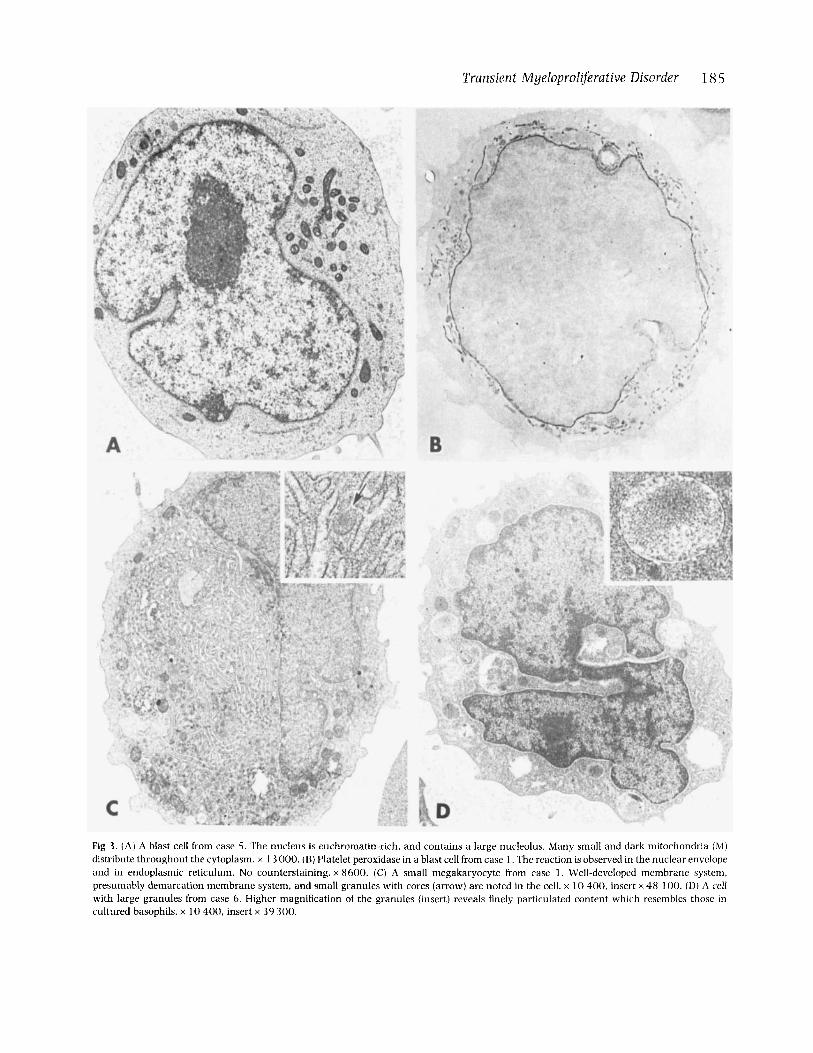
Fig 3 . (A) A blast cell from case 5. The nucleus is euchromatin-rich, and contains a large nucleolus. Many small and dark mitochondria (M) distribute throughout the cytoplasm. x 1 3 000. (B) Platelet peroxidase in a blast cell from case 1 . The reaction is observed in the nuclear envelope and in endoplasmic reticulum. No counterstaining. x 8600. (C) A small megakaryocyte from case I. Well-developed membrane system, presumably demarcation membrane system, and small granules with cores (arrow) are noted in the cell. x 10 400. insert x 48 1 0 0 . (D) A cell with large granules from case 6 . Higher magnification of the granules (insert) reveals finely particulated content which resembles those in cultured basophils. x 10 400, insert x 39 300.

186 Junko Suda et a1 phous granules which resembled the atypical granules of cultured basophils (Eguchi et al, 1985) (Fig 3D).
Immunological studies Peripheral mononuclear cells of all cases reacted (16-60%) with murine monoclonal antibody against platelet glycopro- tein IIb/IIIa as shown in Table IV. Cells of all patients also reacted with TP 82 (30-70%). FITC-conjugated goat anti- mouse globulin serum alone did not induce mononuclear cell fluorescence.
DISCUSSION
Transient myeloproliferative disorder accompanied by Down’s syndrome is interesting as regards the question of whether this disorder is a clonal haemopathy or caused by abnormalities in haemopoietic regulators. In the study on the patient with trisomy 21 mosaic (case l), when blast cells made up 70% of the total, all metaphases from unstimulated peripheral blood cells showed trisomy 2 1. As the blast cell number decreased in peripheral blood, the proportion of metaphases showing trisomy 2 1 decreased. These cytogene- tic data are consistent with those reported previously by other investigators (Brodeur et al, 1980: Heaton et al, 1981; Weinburg et al, 1982; Seibel et a!, 1984). Moreover, simulta- neous karyotypic and morphological analyses of colonies revealed that cells grown in methylcellulose cultures showed trisomy 21 exclusively. These data suggested that this disorder was the result of selective proliferation of chronio- some 21 trisomic blast cells, perhaps caused by the trisomy 21 cells gaining a proliferative advantage over the normal cells. It is thus unlikely that the transient myeloproliferative disorder is caused by abnormalities of haemopoietic factors. However, it has not yet been clarified whether these trisomy 2 1 cells are monoclonal or polyclonal in this study.
The blast cells were positive for the PPO reaction in all cases. Moreover, all cases examined contained TP 80 and TP 82 (against platelet/megakaryocyte antigens) reactive blast cells. It was reported that TP 80 was specific for glycoprotein IIb/IIIa (Sato et al, 1986) and TP 82 was specific for platelets, megakaryocytes and acute lymphoblastic leukaemia cells (Higashihara et al. 1985). A recent report suggested that glycoprotein IIb/IIIa was a marker not only for cells of platelet/megakaryocytic Lineage but also for multipotential haemopoietic stem cells (Fraser et al, 1986). In our study, these blast cells showed high proliferative and differentiation capacities in methylcellulose and liquid cultures. In methyl- cellulose cultures, four cases out of five showed normal or higher than normal colony forming abilities with maturation and differentiation into neutrophils, macrophages. basophils, eosinophils, megakaryocytes and erythrocytes. In cases 3 and 6, especially, differentiation of blast cells into basophils was obvious, but the relationship between PPO-positive cells and basophils remained unclarified. It was reported that the PPO reaction was observed in basophilic blast cells (Polli et al, 198 5). We previously showed that PPO-positive leukaemic cells have the capacity to differentiate into basophils (Suda et ul. 198 5). Thus the PPO reaction and/or glycoprotein IIb/IIIa might have a close relationship with basophil differentiation.
Recently, Coulombel et a1 (1987) have reported that blast cells in transient myeloproliferative disorder express mega- karyocyte and erythroid markers identified by electronmicro- scopic observation. However, we did not recognize ferritin in blast cells in six cases examined. From the findings of Coulombel et al, and our own, it may be concluded that PPO- positive blast cells in transient myeloproliferative disorder are not restricted to megakaryocytic lineage.
One important question is why these blast cells disappear spontaneously. One possibility is the high differentiation ability of these blast cells, differentiation into mature cells resulting in loss of their ability for self renewal, as in the case we previously reported (Suda et A!, 1987). It is essential to clarify these mechanisms and their relationship to the unlimited proliferation of true leukaemia.
It has been reported that some patients who showed spontaneous regression of congenital myeloproliferative dis- order subsequently developed acute leukaemia (Honda et al, 1964; Morgan et a], 1985). In cytogenetic studies, we observed one or two sublines in addition to the stem line with trisomy 2 1 in two cases. Although this was a small study and reports of detailed cytogenetic studies on transient myelopro- liferative disorder are rare in the literature, it is possible that clonal instability exists. More extensive cytogenetic studies on patients with this disorder and long-term follow up of their clinical courses will be necessary to clarify these problems.
In summary, transient myeloproliferative disorder accom- panied by Down’s syndrome represents a selective expansion of chromosome 21 trisomic cells, which often show PPO- positive reaction and a high capacity for differentiation into, particularly, basophils.
ACKNOWLEDGMENTS
We thank Drs Y. Toyota and K. Ohga for providing sam- ples. We also thank Ms M. Yamamoto for her excellent technical assistance. This work was supported by Grants- in-Aid for Scientific Research from the Ministry of Educa- tion, Science and Culture, Japan.
REFERENCES
Breton-Gorius, J. & Guichard, J. (1 9 7 2 ) Ultrastructural localixation of pcroxidase activity in human platelets and megakaryocytes. American Journal of Pathology, 66, 277-293.
Breton-Gorius. J., Reyes, F., Ijuhamel, G., Najman, A. & Gorin. N.C. ( I 978) Megakaryoblastic acute leukemia: identification by the ultrastructural demonstration of platelet peroxidae. Blood, 51.4 5- 60.
Brodeur, G.M.. Dahl, G.V.. Williams, D.L.. Tipton. R.E. & Kalwinsky, D.K. ( 1 980) Transient leukemoid reaction and trisomy 2 1 mosai- cism in a phenotypically normal newborn. Blood. 5 5 , 691-693.
Coulombel. I,., Deryckc. M.. Villeval. L.. Leonard. C.. Breton-Gorius. 1.. Vial. M.. Bourgeois, P. & Tchernia. G. (1987) Characterization of the blast cell population in two neonates with Down’s syndrome and transient myeloproliferative disorder. British Journal of Huerncl-
Eguchi. M., Sakakibara, H.. Iwama. Y., Ochiai. F., Furukawa, T.. Yamaguchi. K., Suda, T. & Suda. J. (1985) Ultrastructural
tolog#, 66, 69-76.

Transient Myeloproliferative Disorder 18 7 Kennedy, A. & Hammond, I). (1 984) Down syndrome and acute leukemia in children: a 10-year retrospective survey from Chil- drens Cancer Study Group. lournal of Pediatrics. 105, 235-242.
Rosner. F. & Lee, S.L. (1 972) Down's syndrome and acute leukemia: myeloblastic or lymphoblastic! American journal gf Pediatrics. 53 , 203-218.
Ross, J.D.. Molony. W.C. & Desforges. J.F. (1963) Ineffective regula- tion of granulopoiesis masquerading as congenital leukemia in a mongoloid child. Journal of Pediatrics. 63, 1-10.
Sato, T., Shichishima, T., Kimura, H., Uchida, T., Kariyone, S. , Ohto. H. & Maeda, H. (1986) Immunocytochemical detection of normal and abnormal megakaryocytes using monoclonal antibody to glycoprotein IIb-IIIa (TP 80). The quantitative assay in normal and in leukemic patients. Scandinavian Journal of Haemutology. 36,
Sato. Y., Suda, T., Suda. 7.. Ohsaka. A.. Kubota, K., Saito, M. & Miura. Y. (1 986) Multilineage expression of hemopoietic precursors with an abnormal clone in idiopathic myelofibrosis. British lournu1 of Haematology. 64, 657-667.
Seibel. N.L., Sommer. A. & Miser, J. (1984) Transient neonatal leukemoid reactions in mosaic trisomy 2 1 . Journal oJ Pediatrics, 104, 251-254.
Suda. J.. Eguchi, M., Akiyama, Y.. Iwama. Y.. Furukawa. T., Sato. Y., Miura, Y.. Suda. T. & Saito, M. (1987) Differentiation of blast cells from a Down's syndrome patient with transient myeloproliferative disorder. Blood, 69, 508-512.
Suda, T., Suda, J., Miura. Y.. Hayashi. Y.. Eguchi. M., Tadokoro. K . & Saito, M. (198 5) Clonal analysis of hasophil differentiation in bone marrow cultures from a Down's syndrome patient with mega- karyoblastic leukemia. Mood, 66, 1278-1283.
Weinburg, A.G., Schiller, G. & Windmiller, J. (1982) Neonatal leukemoid reaction. American {ournnl of Diseases of Children, 136, 3 10-3 1 1.
Yam, L.T., Li, C.Y. & Crosby. W.H. (1981) Cytochemical identifica- tion of monocytes and granulocytes. American Journal of Clinical Pathology, 53, 283-290.
415-423.
characterization of cells with basophilic granules in hemopoietic colonies. lournu1 of Clinical Microscopy, 18, 5-6.
Fraser. ].K., Leahy, M.F. & Berridge. M.V. (1986) Expression of antigens of the platelet glycoprotein IIb/IIIa complex on human hemopoietic stem cells. Blood, 68, 762-769.
Heaton. D.C.. Fitzgerald. P.H.. Fraser. G.J. & Abbot. G.D. (1981) Transient leukemoid proliferation of the cytogenetically un- balanced f 2 1 cell line of a constitutional mosaic boy. Blood, 57, 88 3-88 7.
Higashihara, M., Maeda, H., Shibata, Y., Kume, S. & Ohashi, T. (1985) A monoclonal anti-human platelet antibody: a new platelet aggregating substance. Blood, 65, 382-391.
Honda. F., Punnett. H.H.. Charney. E.. Miller, G. & Thiede, H A . ( 1 964) Serial cytogenetic and hematological studies on a mongo1 with trisomy-21 and acute congenital leukemia. Journal of Pedia- trics. 65. 880-887.
ISCN: International System for Human Cytogenetic Nomenclature (1978) Birth Defects, Vol. XIV, no. 8 , The National Foundation. Cytogenetics and Cell Genetics, 21, 309.
Komatsu, N.. Suda, T.. Sakata, Y., Eguchi. M.. Kaji. K., Saito, M. & Miura. Y. (1986) Megakaryopoiesis in vitro of patients with essential thrombocythaemia; effect of plasma and serum on megakaryocytic colony formation. British Journal of Haematology.
Lewis, D.S. (1 98 1) Association between megakaryoblastic leukemia and Down's syndrome. Lancet, ii, 695.
Morgan, R., Hecht. F., Cleary, M.L., Sklar, J. & Link, M.P. (1985) Leukemia with Down's syndrome: translocation between chromo- somes 1 and 19 in acute myelomonocytic leukemia following transient congenital myeloproliferative syndrome. Blood. 66, 1466-1468.
Polli. N.. O'Brien, M., Tavares de Castro, 1.. Matutes. Em.. San Miguel. J.P. & Catovsky, I). (1 985) Characterization ofblast cells in chronic granulocytic leukaemia in transformation, acute myelofibrosis and undifferentiated leukaemia. British Journal of Huematology, 59, 2 7 7-296.
Robinson. L.L.. Nesbit, M.E.. Jr , Sather, C.. Level. C., Shahidi. N.,
64,241-252.