Embed Size (px)
Citation preview

PLASMA CERAMIDESA NOVEL BIOMARKER OF UNSTABLE ATHEROSCLEROTIC CARDIOVASCULAR DISEASE

C A R D I O L O G Y A T M A Y O C L I N I C
M A Y O M E D I C A L L A B O R A T O R I E S . C O M / C E R A M I D E S
WHICH TEST SHOULD I ORDER?} Plasma Ceramides (Mayo ID: CERAM)
WHEN SHOULD I ORDER?Ordering this test is helpful for establishing an individual’s risk or determining whether a residual risk remains. Specific ordering scenarios include:
} Patients with established coronary artery disease.
} Patients with history of or clinical suspicion for acute coronary syndrome or a myocardial infarction.
} Patients with intermediate or undetermined atherosclerotic cardiovascular risk, as 19.4% cardiovascular events occur in the absence of traditional risk factors.8
WHAT ARE CERAMIDES?Ceramides are complex lipids that play a central role in cell membrane integrity, cellular stress response, inflammatory signaling, and apoptosis. Synthesis of ceramides from saturated fats and sphingosine occurs in all tissues. Ceramides accumulate in tissues not suited for lipid storage during conditions of metabolic dysfunction and dyslipidemia. Three specific ceramides have been identified as highly linked to cardiovascular disease: Cer(16:0), Cer(18:0), Cer(24:1).
PLASMA CERAMIDES AND RISK OF CARDIOVASCULAR EVENTS
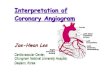
Plasma ceramides are elevated in patients with coronary artery disease (CAD), insulin resistance, and type 2 diabetes mellitus.1,2 Elevations of plasma ceramides are significantly higher among patients with acute coronary syndromes and unstable angina compared to stable CAD.3 Plasma ceramides are predictors of adverse cardiovascular events resulting from unstable atherosclerotic plaque. Risk conferred by ceramides is independent of traditional biomarkers including age, sex, smoking status, and history of CAD.
ELEVATED PLASMA CERAMIDE CONCENTRATIONS ARE A RISK FACTOR FOR:
} Myocardial infarction.
} Emergency coronary revascularizations (PCI and CABG).
} Acute coronary syndrome hospitalizations.
} Cardiovascular mortality.
} Cerebrovascular accidents (stroke).
WHY ORDER PLASMA CERAMIDES OVER OTHER BIOMARKER TESTS THAT PREDICT RISK?
} Plasma ceramides predict adverse cardiovascular events.
– Within 1 year among patients with established coronary artery disease.4
– Within 3 to 5 years for patients with suspected CAD and/or chronic heart failure.4–6
} Risk conferred by plasma ceramides is independent of LDL cholesterol, HDL cholesterol, C-reactive protein, LDL particles, HDL particles, and Lp-PLA2 (concentration and activity).
} Plasma ceramides are a modifiable risk marker.6,7
– Standard statin therapies (simvastatin and rosuvastatin) significantly reduce plasma ceramides within 5 weeks.
– Plasma ceramides are significantly lower among patients with reduced PCSK9 activity.

C U S T O M E R S E R V I C E F O R C L I N I C A L S P E C I A L I S T S / 8 5 5 - 5 1 6 - 8 4 0 4
P L A S M A C E R A M I D E S T E S T I N G
RESEARCH IN SUPPORT OF CERAMIDES TESTING
A NESTED CASE CONTROL FROM THE COROGENE STUDY4
} The Corogene study is a prospective cohort study consisting of patients assigned to coronary angiogram.5
} Cases (n=80) included stable patients with CAD, who had experienced CV death within an average follow-up of 2.5 years.
} Controls (n=80) were selected from patients who survived the follow-up period and were matched for age, sex, smoking, type 2 diabetes and statin use at study entry.
} Cer(16:0), Cer(18:0), and Cer(24:1) were highly predictive of CV death.
SPECIAL PROGRAM AY UNIVERSITY MEDICINE - ACUTE CORONARY SYDROMES (SPUM-ACS) AND BERGEN CORONARY ANGIOGRAPHY COHORT (BECAC) STUDIES4
} SPUM-ACS: 51 CV deaths recorded during one-year follow-up among 1,637 ACS patients enrolled at four Swiss university hospitals.
} BECAC: 81 CV deaths during a median follow-up of 4.6 years among 1,580 adults referred to elective coronary angiography.
} A significant increase in actual events is observed when patients are stratified according to the Ceramide Risk Score.
BECAC (5-YEAR RISK) SPUM-ACS (1-YEAR RISK)
SCORE DEATHS (n) % RELATIVE RISK SCORE DEATHS (n) % RELATIVE RISK
0–2 15/549 2.7% 1.0 0–2 9/575 1.6% 1.0
3–6 29/601 4.8% 1.8 3–6 16/611 2.6% 1.7
7–9 20/288 6.9% 2.5 7–9 9/270 3.3% 2.1
10–12 17/149 11.4% 4.2 10–12 17/181 9.4% 6.0
BIO
MA
RK
ER
SIG
NIF
ICA
NC
E
p-va
lue
1e-009
1e-008
1e-007
1e-006
1e-005
0.0001
0.001
0.01
0.1
1
Cer(24:1) / Cer(24:0)
Cer(16:0) / Cer(24:0)
Cer(18:0) / Cer(24:0) CRP
HDL-C
-30 -20 -10 0 10 20 30 40 50 60
TC
LDL-CLDL-P
TG
ApoBLp-PLA2
Lp(a)
Case (stable CAD at entry) vs. control, mean relative difference (%)

MC2775-107rev0616
@mayocliniclabs/mayocliniclabsnews.mayomedicallaboratories.commayomedicallaboratories.com
DIRECTORS1 LINNEA BAUDHUIN, PH.D.2 LESLIE DONATO, PH.D.3 ALLAN JAFFE, M.D.4 JOSEPH MALESZEWSKI, M.D.5 JEFF MEEUSEN, PH.D.
1 2 3
5
TAP INTO THE EXPERTISE OF MAYO CLINIC
The Cardiovascular Laboratory Medicine Group
within Mayo Clinic works to accommodate the
growing demand for development, validation,
and use of analytes to predict risk for both
primary and secondary prevention.
Focused on acute-care cardiology, risk
stratification, and genomics, the group integrates
laboratory cardiology with its colleagues in
cardiology, pediatric cardiology, genetics,
cardio-thoracic and vascular surgery—as well
as cerebrovascular specialists in neurology.
FOR MORE INFORMATION ABOUT CARDIOVASCULAR TESTING, VISITMayoMedicalLaboratories.com/ceramides
4
6 7
CARDIOLOGY-FOCUSED GENETIC COUNSELORS6 MICHELLE KLUGE, M.S., CGC7 KATE KOTZER, M.S., CGC
REFERENCES
1. Meikle PJ, Wong G, Tsorotes D, et al: Plasma lipidomic analysis of stable and unstable
coronary artery disease. Arterioscler Thromb Vasc Biol 2011 Nov;31(11):2723-32
2. Bergman BC, Brozinick JT, Strauss A, et al: Serum sphingolipids: relationships to
insulin sensitivity and changes with exercise in humans. Am J Physiol Endocrinol
Metab. 2015 Aug;309(4):E398-408
3. Pan W, Yu J, Shi R, et al: Elevation of ceramide and activation of secretory acid
sphingomyelinase in patients with acute coronary syndromes. Coron Artery Dis. 2014
May;25(3):230-5
4. Laaksonen R, Ekroos K, Sysi-Aho M, et al: Plasma ceramides predict cardiovascular
death in patients with stable coronary artery disease and acute coronary syndromes
beyond LDL-cholesterol. Eur Heart J. 2016 April;28: pii: ehw148. [Epub ahead of print]
5. Yu J, Pan W, Shi R, et. al: Ceramide is upregulated and associated with mortality in
patients with chronic heart failure. Can J Cardiol. 2015 Mar;31(3):357-63
6. Tarasov K, Ekroos K, Suoniemi M, et al: Molecular Lipids Identify Cardiovascular RIsk
and Are Efficiently Lowered by Simvastatin and PCSK9 Deficiency. J Clin Endocrinol
Metab. 2014 Nov;99(11):E45-52
7. Ng TW, Ooi EM, Watts GF, et al: Dose-dependent effects of rosuvastatin on the
plasma sphingolipidome and phospholipidome in the metabolic syndrome. J Clin
Endocrinol Metab. 2014 Nov;99(11):E2335-40
8. Khot UN, Khot MB, Bajzer CT, et al: Prevalence of conventional risk factors in patients
with coronary heart disease. JAMA 2003 Aug;290(7)898-904