Embed Size (px)
Citation preview
Planning impairments in frontal lobe dementia and frontal lobelesion patients
Danielle Carlina, Joy Bonerbaa, Michael Phippsa, Gene Alexanderb, Mark Shapirob,Jordan Grafmana,*
aCognitive Neuroscience Section, National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, Maryland, USAbLaboratory of Neuroscience, National Institute of Aging, National Institutes of Health, Bethesda, Maryland, USA
Received 18 February 1999; accepted 27 July 1999
Abstract
Patients with frontal lobe brain damage are reportedly impaired on tasks that require plan development and execution. In thisstudy, we examined the performance of 15 patients diagnosed with frontal lobe dementia and 14 patients with focal frontal lobelesions on the Tower of London planning task. Patients with frontal lobe dementia committed a signi®cantly higher number ofrule violations, made more moves, and demonstrated longer solution time latencies compared to their matched controls. Patients
with frontal lobe lesions demonstrated signi®cantly delayed solution times and also made more moves compared to theirmatched controls. Frontal lobe lesion patient performance suggests an impairment in execution-related processes, while frontallobe dementia patients appear to be impaired in both plan development and execution. Despite these ®ndings, the identi®cation
of a speci®c cognitive impairment that induces these planning problems remains elusive. Published by Elsevier Science Ltd.
Keywords: Planning; Tower of London; Frontal lobe lesion; Frontal lobe dementia
1. Introduction
Human planning requires the cooperation of a num-ber of cognitive processes including a look-aheadmechanism designed to generate multiple sequences ofhypothetical events and their consequences, the devel-opment of stored structured event complexes that canguide movement from an initial to a goal state, ex-ecution-linked anticipation of future events, and recog-nition of goal attainment. All of these processes arethought to depend on the prefrontal cortex [1].
The planning processes described above appearnecessary for adequate performance on the Tower ofLondon test of planning ability designed by Shallice[2]. The task was created as a measure of the Supervi-
sory Attention System (SAS) proposed by Normanand Shallice [3]. In Norman and Shallice's model ofattention, two processing systems exist to handle noveland routine situations. ``Contention scheduling''induces the processing and retrieval of mental schema'sfor routine situations. In the case of non-routine situ-ations, a more ¯exible system induces the developmentof novel goal directed schemas. Norman and Shallicehypothesized that this latter system, the SAS, wasimpaired in patients with frontal lobe lesions whoinstead had to rely upon environmental stimuli forclues on how to act in non-routine situations.
The basic Tower of London (TOL) test involvesmoving three disks, initially situated on three pegs, toa pre-de®ned goal ``state''. The constraints are few,only one disk may be moved at a time, all disks notbeing moved must remain on one of three di�erentlysized pegs-each peg capable of holding either one, two,or three disks. TOL tests may vary by the number ofmoves required to achieve the goal state and by mech-
Neuropsychologia 38 (2000) 655±665
0028-3932/00/$ - see front matter Published by Elsevier Science Ltd.
PII: S0028-3932(99 )00102 -5
www.elsevier.com/locate/neuropsychologia
* Corresponding author. Tel.: +1-301-496-0220; fax: +1-301-480-
2909.
E-mail address: [email protected] (J. Grafman).

anism of administration. The adequacy of a subject'sperformance on the TOL is determined by number ofproblems solved, the total number of moves madeabove the minimum required to reach the goal state,response latencies, and errors. Because the subjectneeds to complete each problem in a speci®ed numberof moves, performance on the Tower of Londonrequires a component of planning called the ``look-ahead'' function. This function allows the subject todevelop a solution path, hold the path in workingmemory, and to use this mental model of the path toguide performance.
Shallice [2] reported that left anterior frontal lobelesions were associated with de®cits in TOL perform-ance. This ®nding was partly con®rmed in a laterstudy [4] in which frontal lobe lesion patients werefound, in comparison to controls, to have signi®cantde®cits in planning performance. But this study didnot ®nd, as Shallice's did, any signi®cant associationbetween the side of lesion and planning ability. Thatis, neither performance accuracy or e�ciency werea�ected di�erentially by a lesion restricted to the rightor left side of the frontal lobes [4].
Researchers using either position emission topogra-phy (PET) or single photon emission computed tom-ography (SPECT) have reported activation in speci®careas of the prefrontal cortex during performance onthe Tower of London task [5±8] including the prefron-tal, premotor, prestriate and insular/opercular cortices.Greater accuracy in performance on the most di�cultTOL levels (four and ®ve move problems) has alsobeen correlated with higher rCBF values in the dorso-lateral, ventrolateral and mesial prefrontal areas andthe basal ganglia [7]. One study even found thatincreased ``initial'' planning time was correlated withhigher left prefrontal rCBF levels, while increased ``sol-ution'' time was associated with lower left prefrontalrCBF levels [6].
The above ®ndings, along with numerous anecdotalstories of frontal lobe planning impairments (e.g., seePen®eld and Evans [9]), reinforce the identi®cation ofthe frontal lobes with ``look-ahead'' planning processesand corroborate that the Tower of London appearsable to measure such an ability. The story, however, ismore complicated. E�orts by Shallice to replicate hisown 1982 results were unsuccessful [10]. In addition,recent studies using the TOL have had con¯ictingresults. Some studies suggest that patients with frontallobe lesions only fail on the most di�cult TOL pro-blems but one study found no signi®cant di�erence inperformance between frontal lobe lesion patients andcontrols [11].
Interpreting the variables of response latency ande�ciency is also complicated by the con¯icting resultsseen in past TOL studies. The TOL allows measure-ment of both planning and solution times. Given anec-
dotal evidence of impulsiveness in frontal lobe lesionpatients [9], it would be expected that patients withfrontal lobe lesions would have shorter planning timesthan controls. A number of TOL studies, however,have shown no signi®cant di�erence in planning timebetween patients and controls [2,4,11,12]. It has beensuggested that patients with frontal lobe lesions tendto initiate action without a coordinated, goal oriented,sequence of moves in mind [13]. This would notnecessarily be re¯ected in planning times, but wouldprobably result in longer solution times and less accu-rate performance.
The TOL has also been utilized in a variety of othersubject groups as a measure of ``look-ahead'' planningability and as a measurement of executive function.These include normal children [14], patients withobsessive compulsive disorder [15], closed-head injury[16±18], Autism [19], Parkinson's disease [12], andmood-disorders [20].
Although the TOL results seen in Parkinson's dis-ease patients appear consistent across studies, frontallobe lesion studies reveal more varied results. Thereare several possible reasons for this inconsistencyincluding heterogeneity of patient etiology, mechanismof administration (recent e�orts have been made tostandardize the Tower of London task administrationprocedures [21]), and adequacy of lesion location/volume loss assessment methods. Given these discre-pancies and the purported importance of the humanprefrontal cortex for planning processes, we haveadministered the TOL task to two di�erent patientpopulations with frontal lobe impairment: patientswith frontal lobe dementia or focal frontal lobelesions. The aims of the study reported below were tomeasure, compare and contrast Tower of London per-formance in two separate populations with frontallobe impairment, compare performance on the TOL tooverall performance on the Tower of Hanoi (TOH),and appraise whether performance on the TOL can bedistinguished from a general impairment in cognitivedysfunction.
2. Materials and methods
2.1. Subjects
A total of 29 patients with prefrontal cortex damageparticipated in this study. Fifteen patients were diag-nosed with frontal lobe dementia (FLD) according tothe Lund and Manchester [22] criteria. Fourteenpatients had sustained focal lesions to the prefrontalcortex (FLL).
The FLD group was comprised of ®fteen subjects(mean age: 60.5 years; gender (M:F) 8:7, education:14.9 years). Disease duration was on average 3.2 years
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665656

(sd 2.7 years) at the time of testing. We determined thelocation of FLD atrophy using structural MR imagingat the time of their evaluation. Based on MR imaging,®ve of ®fteen patients had bifrontal atrophy only.Four patients had both bifrontal and bi-anterior tem-poral atrophy. One patient had left frontal atrophyonly and one patient had right frontal atrophy only.The remaining four patients had various combinationsof frontal and anterior temporal lobe atrophy. Thepatients were matched by gender, age and years ofeducation to a group of ®fteen normal volunteers(mean age: 60.7 years; gender: (M:F) 8:7, education:15.3 years). A two way unpaired T-test con®rmed thatthe patients and controls were well matched in termsof age, years of education and gender (see Table 1).Two of the ®fteen FLD patients could be consideredmoderately demented based on their Mattis DementiaRating Scale total scores, the remaining FLD patientshad scores that fell into the normal and mildly demen-ted range of scores. We anticipated that the FLDpatients, because of more widespread atrophy in theprefrontal cortex and because of active disease pro-gression, would perform worse on the TOL than FLLpatients.
Of the fourteen FLL patients (mean age: 59.9 years;gender: (M:F) 10:4, education: 16.4 years), seven hadlesions con®ned to the left hemisphere, ®ve had lesionscon®ned to the right hemisphere and two had bilateraldamage. Seven of the fourteen patients had su�eredpenetrating missile injuries to the frontal lobes duringthe Vietnam War and were tested approximately 30years post-injury. Among the remaining seven patients,one patient had su�ered a stroke, three had tumorsremoved, and the remaining three patients had sus-tained focal hematomas. The patient group wasmatched by gender, age and years of education to agroup of ®fteen normal volunteers (mean age: 57.5years; gender: (M:F) 11:4, education: 16.4 years). Two-way unpaired T-tests con®rmed that the patients andcontrols were well matched in terms of age, years ofeducation and gender. See Table 1 for details. Thiswas also true when patients were split into groups bylesion location. Examples of lesion sites and lateralityfor left, right and bilateral lesion patients are presented
in Table 2. Structural neuroimaging data (CT scans)placing the lesions within Brodmann areas was avail-able for nine of the fourteen patients [23].
The FLD and FLL patient groups were not directlycompared to each other. The signi®cant di�erence ingender balance, marginal di�erences in age (the FLDsubjects were generally older than the FLL subjects),di�erences in lesion type (head injury vs active pro-gressive disease), and marginal di�erences in attainededucational level would have been di�cult to partialout given the relatively small number of subjects ineach group.
The Wechsler Adult Intelligence Scale-Revised(WAIS-R) [24] and Tower of Hanoi (TOH) tests [25]were also administered to all patients. Mattis Demen-tia Rating Scale Total Scores [26] were obtained onlyfrom the FLD patients.
2.2. The Tower of London task
The Tower of London (TOL) task was given manu-ally and all timing was carried out using a stopwatch.The test was made up of thirteen problems ranging indi�culty from two to ®ve moves and conducted usinga stand of three pegs, each of a di�erent height. Threecolored rings, (red, blue and green) ®t on the pegs.The subject was presented with a start ``state'' of rings(i.e., the rings were placed on the pegs in a certain pat-tern) and given a goal ``state'' (i.e., a ®nal pattern ofrings on the pegs) to achieve in a speci®ed number ofmoves. The goal state was depicted on index sizedcards, with colored pictures to represent the pegs andcorresponding rings. The subject was given the rules atthe beginning of the session. Each ring could only bemoved from one peg to another, only a speci®ed num-ber of rings could be placed on each peg at a time andonly one peg could be moved at a time. The subjectswere reminded of the rules when they were broken andasked to restart their plan execution on that problem.For a subject to achieve a ``correct'' response, theywere required to reach the goal con®guration. Tomove on to the next TOL problem, however, the goalstate had to be reached within the speci®ed minimumnumber of moves. Three attempts to solve each pro-
Table 1
Patient and control characteristicsa
Group Age Education Gender M:F Handedness R:L:A WAIS-R-VIQ WAIS-R-PIQ WAIS-R-FSIQ Mattis dementia rating scale
(MDRS)
FLL 59.9 (12.6) 16.4 (3.2) 10:4 12:2:0 106.6 (14.7) 102.6 (15.3) 106.1 (16.1)
NC 57.5 (16.6) 16.4 (3.1) 11:4 13:1:1 119.4 (8.9) 114.2 (7.2) 119.3 (8.6)
FLD 60.5 (11.5) 14.9 (7.5) 8:7 11:4:0 91.5 (16.0) 93.5 (10.9) 91.6 (13.5) 120.6 (14.5)
NC 60.7 (12.6) 15.3 (2.5) 8:7 13:2:0 114.1 (13.2) 112.1 (7.3) 114.3 (10.8) 140.6 (3.3)
a Means (and standard deviations) are shown.
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665 657
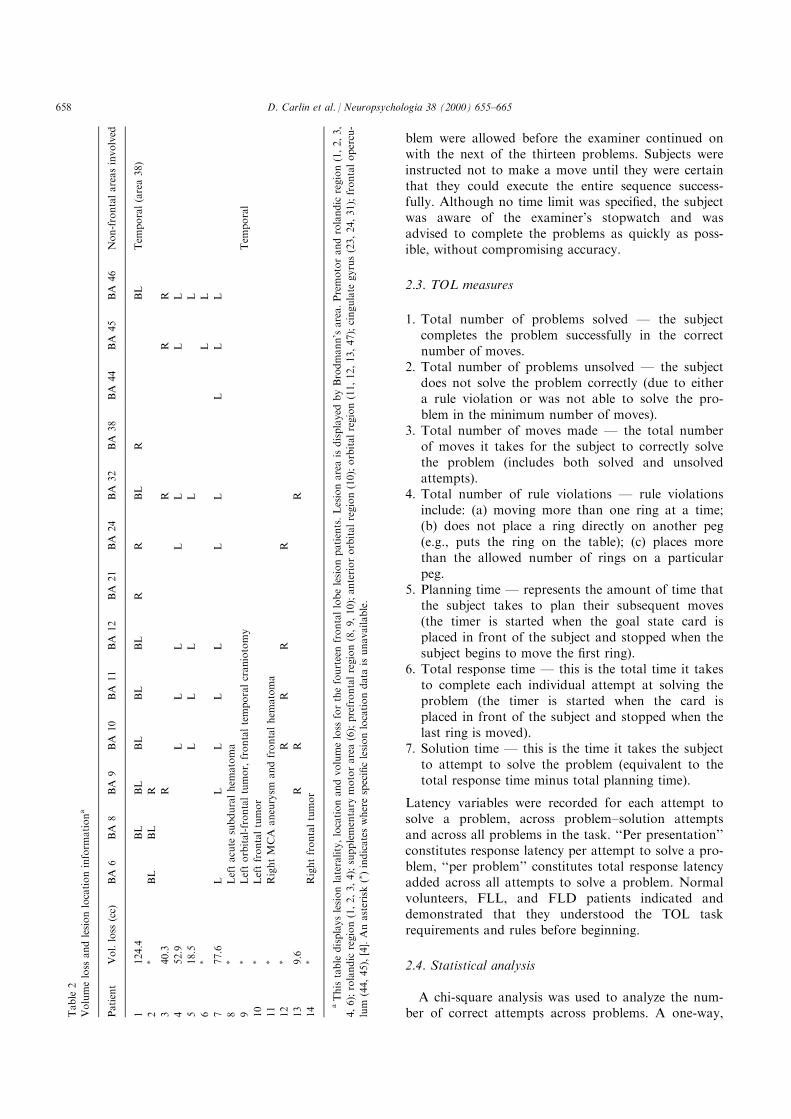
blem were allowed before the examiner continued onwith the next of the thirteen problems. Subjects wereinstructed not to make a move until they were certainthat they could execute the entire sequence success-fully. Although no time limit was speci®ed, the subjectwas aware of the examiner's stopwatch and wasadvised to complete the problems as quickly as poss-ible, without compromising accuracy.
2.3. TOL measures
1. Total number of problems solved Ð the subjectcompletes the problem successfully in the correctnumber of moves.
2. Total number of problems unsolved Ð the subjectdoes not solve the problem correctly (due to eithera rule violation or was not able to solve the pro-blem in the minimum number of moves).
3. Total number of moves made Ð the total numberof moves it takes for the subject to correctly solvethe problem (includes both solved and unsolvedattempts).
4. Total number of rule violations Ð rule violationsinclude: (a) moving more than one ring at a time;(b) does not place a ring directly on another peg(e.g., puts the ring on the table); (c) places morethan the allowed number of rings on a particularpeg.
5. Planning time Ð represents the amount of time thatthe subject takes to plan their subsequent moves(the timer is started when the goal state card isplaced in front of the subject and stopped when thesubject begins to move the ®rst ring).
6. Total response time Ð this is the total time it takesto complete each individual attempt at solving theproblem (the timer is started when the card isplaced in front of the subject and stopped when thelast ring is moved).
7. Solution time Ð this is the time it takes the subjectto attempt to solve the problem (equivalent to thetotal response time minus total planning time).
Latency variables were recorded for each attempt tosolve a problem, across problem±solution attemptsand across all problems in the task. ``Per presentation''constitutes response latency per attempt to solve a pro-blem, ``per problem'' constitutes total response latencyadded across all attempts to solve a problem. Normalvolunteers, FLL, and FLD patients indicated anddemonstrated that they understood the TOL taskrequirements and rules before beginning.
2.4. Statistical analysis
A chi-square analysis was used to analyze the num-ber of correct attempts across problems. A one-way,T
able
2
Volumeloss
andlesionlocationinform
ationa
Patient
Vol.loss
(cc)
BA
6BA
8BA
9BA
10
BA
11
BA
12
BA
21
BA
24
BA
32
BA
38
BA
44
BA
45
BA
46
Non-frontalareasinvolved
1124.4
BL
BL
BL
BL
BL
RR
BL
RBL
Tem
poral(area38)
2�
BL
BL
R
340.3
RR
RR
452.9
LL
LL
LL
L
518.5
LL
LL
L
6�
LL
777.6
LL
LL
LL
LL
LL
8�
Leftacute
subduralhem
atoma
9�
Leftorbital-frontaltumor,frontaltemporalcraniotomy
Tem
poral
10
�Leftfrontaltumor
11
�RightMCA
aneurysm
andfrontalhem
atoma
12
�R
RR
R
13
9.6
RR
R
14
�Rightfrontaltumor
aThistable
displayslesionlaterality,locationandvolumeloss
forthefourteenfrontallobelesionpatients.Lesionareaisdisplayed
byBrodmann'sarea.Premotorandrolandic
region(1,2,3,
4,6);rolandic
region(1,2,3,4);supplementary
motorarea(6);prefrontalregion(8,9,10);anteriororbitalregion(10);orbitalregion(11,12,13,47);cingulate
gyrus(23,24,31);frontalopercu-
lum
(44,45),[4].Anasterisk(�)indicateswherespeci®clesionlocationdata
isunavailable.
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665658
unpaired T-test was employed to compare TOL per-formance between patients and controls. Spearman'srank order correlation procedure was used for correlat-ing subject performance on other neuropsychologicaltests to TOL performance and a factorial repeatedmeasures analysis of variance was used to compareperformance across problems between patients andcontrols. Statview 5.0 [27] was used for all analyses.
3. Results
3.1. FLD patients compared to controls
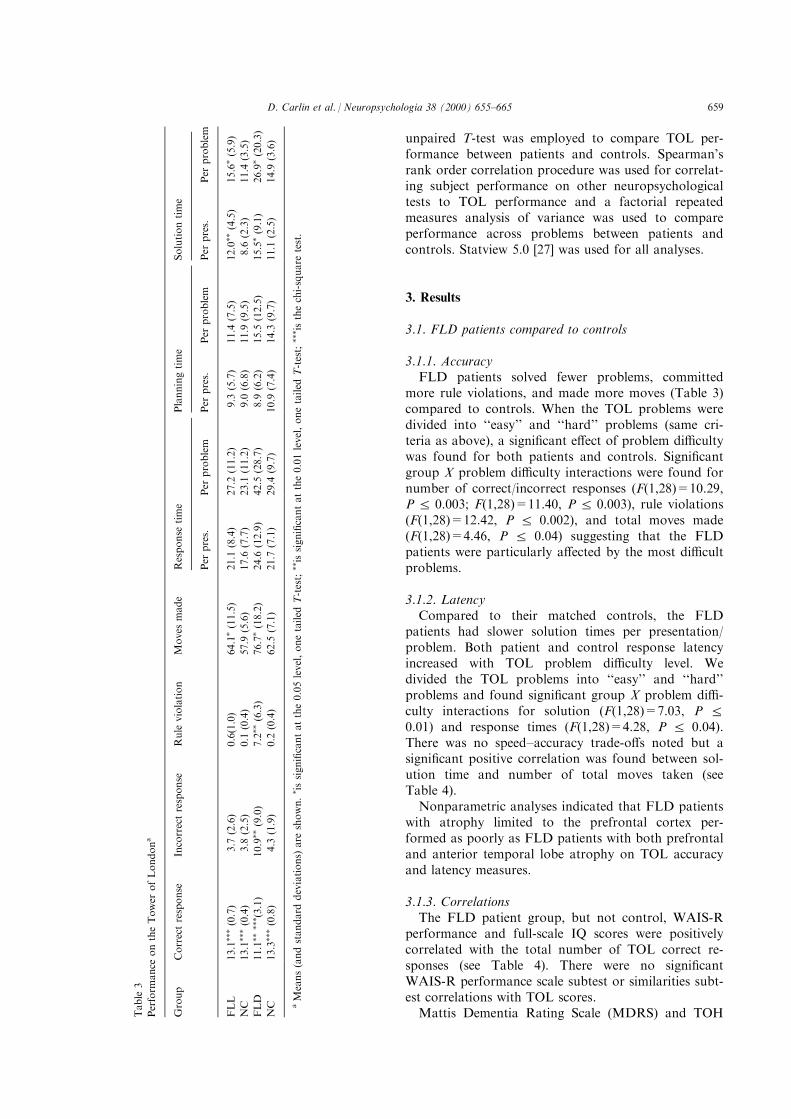
3.1.1. AccuracyFLD patients solved fewer problems, committed
more rule violations, and made more moves (Table 3)compared to controls. When the TOL problems weredivided into ``easy'' and ``hard'' problems (same cri-teria as above), a signi®cant e�ect of problem di�cultywas found for both patients and controls. Signi®cantgroup X problem di�culty interactions were found fornumber of correct/incorrect responses (F(1,28)=10.29,P R 0.003; F(1,28)=11.40, P R 0.003), rule violations(F(1,28)=12.42, P R 0.002), and total moves made(F(1,28)=4.46, P R 0.04) suggesting that the FLDpatients were particularly a�ected by the most di�cultproblems.
3.1.2. LatencyCompared to their matched controls, the FLD
patients had slower solution times per presentation/problem. Both patient and control response latencyincreased with TOL problem di�culty level. Wedivided the TOL problems into ``easy'' and ``hard''problems and found signi®cant group X problem di�-culty interactions for solution (F(1,28)=7.03, P R0.01) and response times (F(1,28)=4.28, P R 0.04).There was no speed±accuracy trade-o�s noted but asigni®cant positive correlation was found between sol-ution time and number of total moves taken (seeTable 4).
Nonparametric analyses indicated that FLD patientswith atrophy limited to the prefrontal cortex per-formed as poorly as FLD patients with both prefrontaland anterior temporal lobe atrophy on TOL accuracyand latency measures.
3.1.3. CorrelationsThe FLD patient group, but not control, WAIS-R
performance and full-scale IQ scores were positivelycorrelated with the total number of TOL correct re-sponses (see Table 4). There were no signi®cantWAIS-R performance scale subtest or similarities subt-est correlations with TOL scores.
Mattis Dementia Rating Scale (MDRS) and TOHTable
3
Perform
ance
ontheTower
ofLondona
Group
Correctresponse
Incorrectresponse
Rule
violation
Moves
made
Response
time
Planningtime
Solutiontime
Per
pres.
Per
problem
Per
pres.
Per
problem
Per
pres.
Per
problem
FLL
13.1���(0.7)
3.7
(2.6)
0.6(1.0)
64.1�(11.5)
21.1
(8.4)
27.2
(11.2)
9.3
(5.7)
11.4
(7.5)
12.0��
(4.5)
15.6�(5.9)
NC
13.1���(0.4)
3.8
(2.5)
0.1
(0.4)
57.9
(5.6)
17.6
(7.7)
23.1
(11.2)
9.0
(6.8)
11.9
(9.5)
8.6
(2.3)
11.4
(3.5)
FLD
11.1����� (3.1)
10.9��
(9.0)
7.2��
(6.3)
76.7�(18.2)
24.6
(12.9)
42.5
(28.7)
8.9
(6.2)
15.5
(12.5)
15.5�(9.1)
26.9�(20.3)
NC
13.3���(0.8)
4.3
(1.9)
0.2
(0.4)
62.5
(7.1)
21.7
(7.1)
29.4
(9.7)
10.9
(7.4)
14.3
(9.7)
11.1
(2.5)
14.9
(3.6)
aMeans(andstandard
deviations)
are
shown.� issigni®cantatthe0.05level,onetailed
T-test;��issigni®cantatthe0.01level,onetailed
T-test;��� isthechi-square
test.
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665 659

scores were also compared to TOL performancemeasures. For the FLD group, signi®cant negative cor-relations were found between total TOH score (alower score implies a worse performance) and severalTOL variables including number of incorrect re-sponses, rule violations, moves made, and solutiontime per problem (see Table 4). MDRS total or subtestscores were not associated with any TOL performancemeasure.
3.2. FLL patients compared to controls
3.2.1. AccuracyFLL patients made signi®cantly more moves than
controls (T = 1.848, P R 0.038), but no other signi®-cant accuracy impairments were found (i.e., FLLpatients generally solved as many problems as controlsalthough they may have made more overall moves inorder to solve the problem Ð see Table 3). To exam-ine performance across level of TOL problem di�-culty, we next split the thirteen problems into ``easy''and ``hard'' groups (see Table 5). The easy group con-sisted of problems one through ®ve (required 2 or 3moves) and the hard group of problems six throughthirteen (required 4 or 5 moves). Both patient and con-trol performance accuracy decreased when problemsincreased in di�culty. A signi®cant group X accuracyinteraction was found for number of moves made(F(1,28)=4.94, P R 0.03) with FLL patients makingsigni®cantly more moves compared to controls as pro-blem di�culty increased.
3.2.2. LatencyFLL patients had signi®cantly slower solution times
than controls for both presentation and problem (T=2.587, P R 0.0077) variables. When TOL problem levelwas split into ``easy'' and ``hard'' groups, both patientsand controls demonstrated slower times as problemdi�culty increased (see Table 5). A signi®cant group Xaccuracy interaction was found for solution time(F(1,28)=8.52, P R 0.007). In comparison to controls,FLL patients demonstrated longer solution times asproblem di�culty increased (compatible with theresults indicating that they also made signi®cantlymore moves than controls). No speed±accuracy trade-o� was noted for either FLL patients or controls.
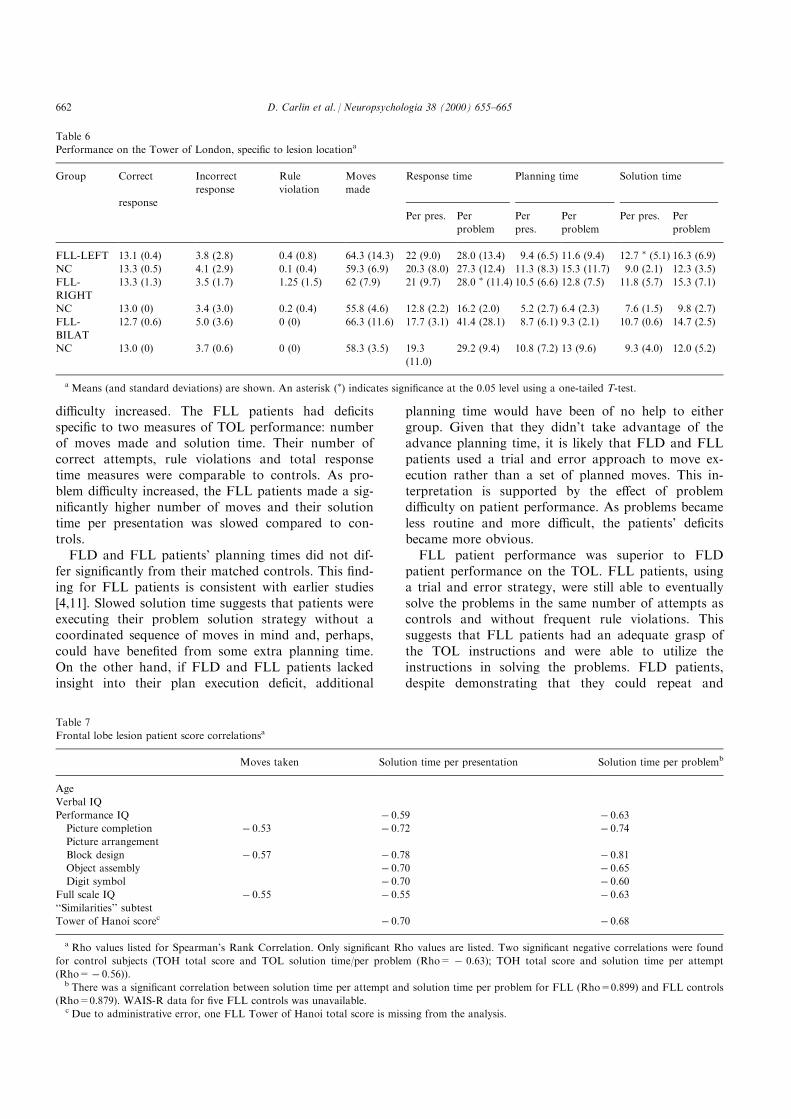
3.2.3. Lesion locationWe then divided the FLL patients into three groups
according to whether they had a left or right unilateralor bilateral lesion (see Table 6). There were seven leftfrontal, ®ve right frontal and two bilateral frontallesion patients. Left FLL patients had signi®cantlyslower solution latencies per presentation, but not perproblem (T = 1.781, P R 0.0496) compared to con-trols. Right FLL patients had signi®cantly slower totalresponse times per problem (T = 2.012, P < 0.0496)than controls. In contrast, the two FLL patients withbilateral damage were not signi®cantly impaired in anyspeci®c area of TOL performance. There were nobetween FLL group di�erences for any of themeasures. Problem di�culty a�ected the three groupssimilarly in regards to both accuracy and latency.
We had considered further breakdowns of the FLLgroup by Brodmann area a�ected or whether the
Table 4
Frontal lobe dementia patient score correlationsa
Correct
response
Incorrect
response
Rule
violation
Moves
taken
Solution time per
presentation
Solution time per problem
Age
Verbal IQ
Performance IQ 0.77
Picture
completion
Picture
arrangement
Block design
Object assembly
Digit symbol
Full scale IQ 0.61
``Similarities''
subtest
Tower of Hanoi
score
ÿ 0.78 ÿ 0.85 ÿ 0.58 ÿ 0.63
a Only signi®cant Rho values are listed (Spearman's rank correlation). Only one of these correlations (TOH total score and number of incorrect
attempts (Rho=0.515)) was signi®cant for the frontal lobe dementia controls. There was a signi®cant correlation between solution time per
attempt and solution time per problem for FLD patients (Rho=0.863) and FLD controls (Rho=0.944).
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665660
lesion was lateral or medial but the total number ofsubjects per group was too small for any meaningfulcomparisons.
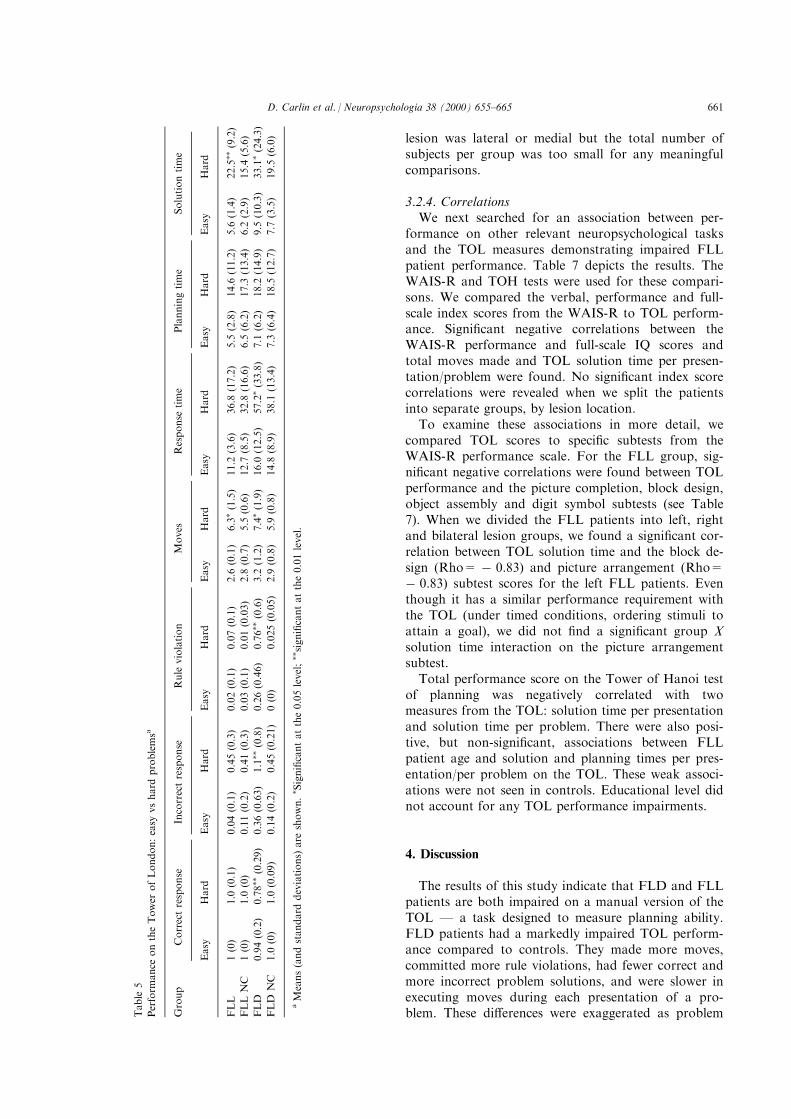
3.2.4. CorrelationsWe next searched for an association between per-
formance on other relevant neuropsychological tasksand the TOL measures demonstrating impaired FLLpatient performance. Table 7 depicts the results. TheWAIS-R and TOH tests were used for these compari-sons. We compared the verbal, performance and full-scale index scores from the WAIS-R to TOL perform-ance. Signi®cant negative correlations between theWAIS-R performance and full-scale IQ scores andtotal moves made and TOL solution time per presen-tation/problem were found. No signi®cant index scorecorrelations were revealed when we split the patientsinto separate groups, by lesion location.
To examine these associations in more detail, wecompared TOL scores to speci®c subtests from theWAIS-R performance scale. For the FLL group, sig-ni®cant negative correlations were found between TOLperformance and the picture completion, block design,object assembly and digit symbol subtests (see Table7). When we divided the FLL patients into left, rightand bilateral lesion groups, we found a signi®cant cor-relation between TOL solution time and the block de-sign (Rho= ÿ 0.83) and picture arrangement (Rho=ÿ 0.83) subtest scores for the left FLL patients. Eventhough it has a similar performance requirement withthe TOL (under timed conditions, ordering stimuli toattain a goal), we did not ®nd a signi®cant group Xsolution time interaction on the picture arrangementsubtest.
Total performance score on the Tower of Hanoi testof planning was negatively correlated with twomeasures from the TOL: solution time per presentationand solution time per problem. There were also posi-tive, but non-signi®cant, associations between FLLpatient age and solution and planning times per pres-entation/per problem on the TOL. These weak associ-ations were not seen in controls. Educational level didnot account for any TOL performance impairments.
4. Discussion
The results of this study indicate that FLD and FLLpatients are both impaired on a manual version of theTOL Ð a task designed to measure planning ability.FLD patients had a markedly impaired TOL perform-ance compared to controls. They made more moves,committed more rule violations, had fewer correct andmore incorrect problem solutions, and were slower inexecuting moves during each presentation of a pro-blem. These di�erences were exaggerated as problemT
able
5
Perform
ance
ontheTower
ofLondon:easy
vshard
problemsa
Group
Correctresponse
Incorrectresponse
Rule
violation
Moves
Response
time
Planningtime
Solutiontime
Easy
Hard
Easy
Hard
Easy
Hard
Easy
Hard
Easy
Hard
Easy
Hard
Easy
Hard
FLL
1(0)
1.0
(0.1)
0.04(0.1)
0.45(0.3)
0.02(0.1)
0.07(0.1)
2.6
(0.1)
6.3�(1.5)
11.2
(3.6)
36.8
(17.2)
5.5
(2.8)
14.6
(11.2)
5.6
(1.4)
22.5��
(9.2)
FLLNC
1(0)
1.0
(0)
0.11(0.2)
0.41(0.3)
0.03(0.1)
0.01(0.03)
2.8
(0.7)
5.5
(0.6)
12.7
(8.5)
32.8
(16.6)
6.5
(6.2)
17.3
(13.4)
6.2
(2.9)
15.4
(5.6)
FLD
0.94(0.2)
0.78��
(0.29)
0.36(0.63)
1.1��
(0.8)
0.26(0.46)
0.76��
(0.6)
3.2
(1.2)
7.4�(1.9)
16.0
(12.5)
57.2�(33.8)
7.1
(6.2)
18.2
(14.9)
9.5
(10.3)
33.1�(24.3)
FLD
NC
1.0
(0)
1.0
(0.09)
0.14(0.2)
0.45(0.21)
0(0)
0.025(0.05)
2.9
(0.8)
5.9
(0.8)
14.8
(8.9)
38.1
(13.4)
7.3
(6.4)
18.5
(12.7)
7.7
(3.5)
19.5
(6.0)
aMeans(andstandard
deviations)
are
shown.� Signi®cantatthe0.05level;��signi®cantatthe0.01level.
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665 661
di�culty increased. The FLL patients had de®citsspeci®c to two measures of TOL performance: numberof moves made and solution time. Their number ofcorrect attempts, rule violations and total responsetime measures were comparable to controls. As pro-blem di�culty increased, the FLL patients made a sig-ni®cantly higher number of moves and their solutiontime per presentation was slowed compared to con-trols.
FLD and FLL patients' planning times did not dif-fer signi®cantly from their matched controls. This ®nd-ing for FLL patients is consistent with earlier studies[4,11]. Slowed solution time suggests that patients wereexecuting their problem solution strategy without acoordinated sequence of moves in mind and, perhaps,could have bene®ted from some extra planning time.On the other hand, if FLD and FLL patients lackedinsight into their plan execution de®cit, additional
planning time would have been of no help to eithergroup. Given that they didn't take advantage of theadvance planning time, it is likely that FLD and FLLpatients used a trial and error approach to move ex-ecution rather than a set of planned moves. This in-terpretation is supported by the e�ect of problemdi�culty on patient performance. As problems becameless routine and more di�cult, the patients' de®citsbecame more obvious.
FLL patient performance was superior to FLDpatient performance on the TOL. FLL patients, usinga trial and error strategy, were still able to eventuallysolve the problems in the same number of attempts ascontrols and without frequent rule violations. Thissuggests that FLL patients had an adequate grasp ofthe TOL instructions and were able to utilize theinstructions in solving the problems. FLD patients,despite demonstrating that they could repeat and
Table 6
Performance on the Tower of London, speci®c to lesion locationa
Group Correct
response
Incorrect
response
Rule
violation
Moves
made
Response time Planning time Solution time
Per pres. Per
problem
Per
pres.
Per
problem
Per pres. Per
problem
FLL-LEFT 13.1 (0.4) 3.8 (2.8) 0.4 (0.8) 64.3 (14.3) 22 (9.0) 28.0 (13.4) 9.4 (6.5) 11.6 (9.4) 12.7 � (5.1) 16.3 (6.9)
NC 13.3 (0.5) 4.1 (2.9) 0.1 (0.4) 59.3 (6.9) 20.3 (8.0) 27.3 (12.4) 11.3 (8.3) 15.3 (11.7) 9.0 (2.1) 12.3 (3.5)
FLL-
RIGHT
13.3 (1.3) 3.5 (1.7) 1.25 (1.5) 62 (7.9) 21 (9.7) 28.0 � (11.4) 10.5 (6.6) 12.8 (7.5) 11.8 (5.7) 15.3 (7.1)
NC 13.0 (0) 3.4 (3.0) 0.2 (0.4) 55.8 (4.6) 12.8 (2.2) 16.2 (2.0) 5.2 (2.7) 6.4 (2.3) 7.6 (1.5) 9.8 (2.7)
FLL-
BILAT
12.7 (0.6) 5.0 (3.6) 0 (0) 66.3 (11.6) 17.7 (3.1) 41.4 (28.1) 8.7 (6.1) 9.3 (2.1) 10.7 (0.6) 14.7 (2.5)
NC 13.0 (0) 3.7 (0.6) 0 (0) 58.3 (3.5) 19.3
(11.0)
29.2 (9.4) 10.8 (7.2) 13 (9.6) 9.3 (4.0) 12.0 (5.2)
a Means (and standard deviations) are shown. An asterisk (�) indicates signi®cance at the 0.05 level using a one-tailed T-test.
Table 7
Frontal lobe lesion patient score correlationsa
Moves taken Solution time per presentation Solution time per problemb
Age
Verbal IQ
Performance IQ ÿ 0.59 ÿ 0.63
Picture completion ÿ 0.53 ÿ 0.72 ÿ 0.74
Picture arrangement
Block design ÿ 0.57 ÿ 0.78 ÿ 0.81
Object assembly ÿ 0.70 ÿ 0.65
Digit symbol ÿ 0.70 ÿ 0.60
Full scale IQ ÿ 0.55 ÿ 0.55 ÿ 0.63
``Similarities'' subtest
Tower of Hanoi scorec ÿ 0.70 ÿ 0.68
a Rho values listed for Spearman's Rank Correlation. Only signi®cant Rho values are listed. Two signi®cant negative correlations were found
for control subjects (TOH total score and TOL solution time/per problem (Rho= ÿ 0.63); TOH total score and solution time per attempt
(Rho=ÿ 0.56)).b There was a signi®cant correlation between solution time per attempt and solution time per problem for FLL (Rho=0.899) and FLL controls
(Rho=0.879). WAIS-R data for ®ve FLL controls was unavailable.c Due to administrative error, one FLL Tower of Hanoi total score is missing from the analysis.
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665662

remember task instructions, were unable to properlyexecute a plan of action and demonstrated impairedretrieval of shorter fragments of move sequences (con-sistent with their rule violations). FLD patients mademore moves and required more time to solve even theeasiest TOL problems.
There are several independent cognitive processesunderlying ``planning'' operations and one or more ofthem could be impaired in FLD and FLL patients[28]. Such processes include working memory, spatialimagery, the encoding and storage of move sequences,and an understanding of the context of the task [29].WAIS-R performance and full-scale IQ scores corre-lated negatively with TOL performance in both FLLand FLD patients but not in controls. For FLLpatients, the WAIS-R subtests most correlated withTOL performance measures (block design, digit sym-bol, object assembly, and picture completion) are pri-marily dynamic visuospatial and visual associativememory tasks suggesting at least two underlying de®-cits that could be responsible for diminished FLLplanning ability. Performance on the picture arrange-ment was also correlated with TOL performance, butonly in the group of left FLL patients. Solutionlatency on the picture arrangement subtest did not cor-relate with solution latency on the TOL.
TOL scores for FLD patients also correlated withWAIS-R full-scale and performance scores, but therewere no signi®cant correlations between WAIS-R subt-ests and TOL performance. Since the correlations withTOL performance in both the FLD and FLL patientswere speci®c to WAIS-R performance (but not verbal)scale IQ scores, it is unlikely that TOL performancede®cits can be primarily explained by impaired generalintellectual functioning. This observation is similar tothat of Owen et al. [4] who also found TOL perform-ance to be independent of general intellectual function-ing. For both FLL and FLD patients, TOH scoreswere strongly correlated with TOL performance,suggesting that similar planning abilities were beingaddressed by both tasks although there are di�erentstrategies induced by each task as well as di�erentstimulus constraints. Goel and Grafman [25] suggestedthat the TOH de®cits in their FLL patients was due toan inability to inhibit a prepotent action rather than aplanning de®cit. They thought that the TOL wouldprove to be superior to the TOH as a planning tasksince it biased subjects into planning their movesbefore execution. Instead, based on the results fromthe present study, it is probable that neither FLD norFLL patients make adequate use of the TOL pre-move``planning'' time to develop a plan.
When FLL patients were divided into groupsde®ned by lesion location or Brodmann's area(s), nosingle lesion location could account for every TOLperformance de®cit Ð although performance on
speci®c TOL measures were sensitive to laterality oflesion (right, left, bilateral; e.g., but see Baker et al.®ndings that showed strong bifrontal activation in nor-mal subjects during TOL performance [5]). This sup-ports recent ®ndings indicating that the laterality oflesion does not a�ect the overall severity of TOLimpairment [4,12], but contrasts with earlier lesion [2]and brain imaging [6] studies pointing to the left pre-frontal cortex as having a crucial role in TOL perform-ance. Neither FLD disease duration or MDRS scoreswere correlated with TOL performance suggesting thatdisease severity or progression play a smaller role thanthe location of pathology in predicting level of plan-ning ability.
Thus, there appears to be no single cause for failureon the TOL [30]. FLD or FLL patients could have dif-®culty maintaining a set of possible moves in workingmemory or have di�culty in initially compiling a seriesof individual moves into a structured event complexthat could be stored in memory and used to guidemove execution [1]. In either scenario, the FLD orFLL patient might begin to act on a plan, but beunable to inhibit the pre-potent move or alternativemove possibilities at each juncture of plan execution.Maintaining alternative move possibilities in workingmemory would drain resources away from any optimalstructured event complex that was formed to guidetheir actions. This explanation is compatible with bothFLD and FLL patient performance since both groupsdemonstrated normal planning times but signi®cantlyslowed solution times.
Patients with frontal lobe lesions who have di�cultyin performing planning tasks in the laboratory shouldalso have di�culty in real-life activities requiring plan-ning. In fact almost all daily activities require eitherforming a plan or executing a previously establishedplan. Daily routines at work are executed plans.Deciding when to go shopping and what to buyrequires planning. Deciding on what to eat at homefor dinner and how to prepare it requires planning.Some patients may have di�culty formulating andthen articulating the sequence in which activities are tobe performed. Other patients might have di�culty indeviating from a set plan in order to adapt to new cir-cumstances. Some patients might be able to execute aplan but not formulate their own plan. These distinc-tive de®cits could appear alone or in combination.Identifying these and other potential de®cit patternsrequires further study on a range of planning tasks butwould enable clinicians to better prepare patients andtheir family members for the kinds of problems thatcould occur if the patient is thrust into a real-life socialsituation that requires the development or execution ofa plan.
The major representation of plan-level knowledge inthe human brain appears to be in the prefrontal cor-
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665 663

tex. The failures in planning associated with prefrontalcortex lesions include problems in both top-down (dri-ven by ideas or thoughts) and bottom-up (driven bysensory stimuli) plan development, in the developmentand execution of novel plans, in the analogical map-ping of plans, in parallel processing of plans, in oppor-tunistic/partial-order planning (i.e., adapting to achange in plans), in time management of plan ex-ecution, in both development and execution of a com-plete plan event sequence, in discriminating betweenrelevant and irrelevant events occurring in the contextof a plan, in both well- and ill-structured planning sce-nerios, in accessing category-speci®c plans, and in theadequate successive re®nement of plans over time. Thecognitive processing de®cits that appear responsiblefor these planning failures include representationaldegradation of plans (e.g., which would make low fre-quency plans more di�cult to retrieve than high fre-quency plans), di�culty in inhibiting pre-potent totalorder plans (disinhibition), de®cits in thematic induc-tion (which can hinder top-down plan retrieval), plangrammar de®cits (leading to failures in following asequential path of actions), modality speci®c failure inplan development and retrieval (e.g., a failure to accessverbal/propositional, visual, or real-time representationof plan behavior), and impaired opportunistic, partial-order processing (i.e., similar to impaired multitaskingability). Patients with prefrontal cortex lesions mayexhibit one or more of these de®cits that would a�ecttheir ability to plan.
Based on recent research, there is evidence thatthe right prefrontal cortex is responsible for repre-senting total- and partial-order sequences/grammars,time-estimation, and abstract thematic informationabout plans. The same evidence indicates that theleft prefrontal cortex is responsible for representingpropositional information about individual eventsand their links which appears critical for opportu-nistic planning. Ventromedial prefrontal cortex isspecialized for emotional processes that are morelikely to be invoked in social cognitive planningwhereas dorsolateral prefrontal cortex is relativelyspecialized for non-emotional, more mechanisticplanning. Basal ganglia structures contribute tototal-order plans by coding sensorimotor action par-ameters in conjunction with the cognitive represen-tations in prefrontal cortex and may also impose a``value'' on individual events in order to mark theirparticular contribution or importance to a ®xedplan. Thus, the crucial cognitive aspects of plansare stored in the anterior prefrontal cortex and canbe dissociated from other forms of representationalknowledge that are more apt to be activated duringbasic language and object processing and are storedin more posterior parts of the human brain. If thisview is principally correct, then the representations
guiding plan-level units of knowledge describedabove must be bound via temporal coincidence, andanatomically linked, to representations stored else-where in the brain (e.g., words, objects or a singlescene). This linkage allows us to encode and per-ceive all the elements of a plan as a uni®ed episode[1].
Su�cient knowledge has been gained from recentTower-task studies in order to provide some promisingleads for future research. Tower tasks are novel for thesubject as they have usually never performed a similartask before. They are limited in scope as the subject isusually not forced to develop a plan before the task isexecuted, may determine their next move on a trial bytrial basis, and may fail on the task because they areseverely constrained by pre-potent action patternsrather than a planning failure. In contrast, future plan-ning research should continue to focus on how theevent sequences that make up a plan are formed,whether there is unique information that can beabstracted across a sequence of events composing aplan, whether plans are organized by category and fre-quency, more explicit depiction of the plan-level cogni-tive processes referred to above (e.g., plan grammars),and more precise mapping of the cognitive componentsof plans to sectors within the human prefrontal cortexand basal ganglia using patients and functional neuroi-maging studies to acquire evidence.
It is our view that human neuropsychologicalresearch is in a position to deliver crucial evidenceregarding both the cognitive architecture and theneural topography of plans [31]. By being able to rep-resent and execute plans, we are able to integrateevents from the past, present, and future into a singleplan-level memory unit. Planning enables us to outwitother animals and to cope with a changing environ-ment while achieving a myriad of goals. Planning isthe crowning achievement of human cognition andonce well understood will enable a complete portraitof the brain's cognitive functions to be at last attained.
In summary, our results show both FLD and FLLpatient performance de®cits on the TOL test of plan-ning. FLL patient performance indicates they areimpaired in execution-related processes, while FLDpatients appear to be impaired in both plan encodingand execution.
Acknowledgements
Many thanks go to Matthew Peterson, Pat Nelson,Joy O'Grady and Krista Wild for their help in testingsome of the patients and controls enrolled in thisstudy.
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665664
References
[1] Grafman J. Similarities and distinctions among current models
of prefrontal cortical functions. Annals of the New York
Academy of Sciences 1995;769:337±68.
[2] Shallice T. Speci®c impairments of planning. Philosophical
Transactions of the Royal Society of London 1982;298:199±209.
[3] Norman D, Shallice T. Attention to action: willed and auto-
matic control of behaviour. In: Davidson RA, Schwartz GE,
Shapiro D, editors. Consciousness and self-regulation. New
York: Plenum Press, 1986.
[4] Owen A, Downes J, Sahakian B, Poley C, Robbins T. Planning
and spatial working memory following frontal lobe lesions in
man. Neuropsychologia 1990;28:1021±34.
[5] Baker SC, Rogers RD, Owen AM, Frith CD, Dolan RJ,
Frackowiak RS, et al. Neural systems engaged by planning: a
PET study of the Tower of London task. Neuropsychologia
1996;34(6):515±26.
[6] Morris RG, Ahmed S, Syed GS, Toone BK. Neural Correlates
of planning ability: frontal lobe activation during the Tower of
London test. Neuropsychologia 1993;31(12):1367±78.
[7] Owen AM, Doyon J, Petrides M, Evans AC. Planning and
spatial working memory: a positron emission tomography study
in humans. European Journal Neuroscience 1996;8(2):353±64.
[8] Rezai K, Andreason NC, Allinger R, Cohen G, Swayze V,
O'Leary DS. The Neuropsychology of the prefrontal cortex.
Archives of Neurology 1993;50:636±42.
[9] Pen®eld W, Evans J. The frontal lobe in man: a clinical study
of maximum removals. Brain 1935;58:115±33.
[10] Shallice T. From neuropsychology to mental structure.
Cambridge: Cambridge University Press, 1988.
[11] Cockburn J. Performance on the Tower of London test after
severe head injury. Journal of the International
Neuropsychological Society 1995;1(6):537±44.
[12] Owen A, Sahakian B, Hodges J, Summers B, Polkey C,
Robbins T. Dopamine-dependent frontostriatal planning de®cits
in early Parkinsons disease. Neuropsychology 1995;9:126±40.
[13] Drewe EA. Go±no go learning after frontal lobe lesions in
humans. Cortex 1975;11(1):8±16.
[14] Luciana M, Nelson CA. The functional emergence of prefron-
tally-guided working memory systems in four- to eight-year-old
children. Neuropsychologia 1998;36(3):273±93.
[15] Veale DM, Sahakian BJ, Owen AM, Marks IM. Speci®c cog-
nitive de®cits in tests sensitive to frontal lobe dysfunction
in obsessive-compulsive disorder. Psychological Medicine
1996;26(6):1261±9.
[16] Levin H, Mendelsohn D, Lilly M, Fletcher J. Tower of London
performance in relation to Magnetic Resonance Imaging follow-
ing closed head injury in children. Neuropsychology
1994;8(2):171±9.
[17] Levin H, Fletcher J, Kufera J, Harward H. Dimensions of cog-
nition measured by the Tower of London and other cognitive
tasks in head-injured children. Developmental Neuropsychology
1996;12(1):17±34.
[18] Levin HS, Song J, Scheibel RS, Fletcher JM, Harward H, Lilly
M, et al. Concept formation and problem-solving following
closed head injury in children. Journal of the International
Neuropsychological Society 1997;3(6):598±607.
[19] Hughes C, Robbins T, Russell J. Evidence for executive dys-
function in Autism. Neuropsychologia 1994;32(4):477±92.
[20] Elliot R, Baker SC, Rogers RD, O'Leary DA, Paykel ES, Frith
CD, et al. Prefrontal dysfunction in depressed patients perform-
ing a complex planning task: a study using positron emission
tomography. Psychological Medicine 1997;27:931±42.
[21] Krikorian R, Bartok J, Gay N. Tower of London procedure: a
standard method and developmental data. Journal of Clinical
and Experimental Neuropsychology 1994;16(6):840±50.
[22] The Lund, Manchester Groups. Clinical and neuropathological
criteria for frontotemporal dementia. Journal of Neurology,
Neurosurgery, and Psychiatry 1994;57(4):416±8.
[23] Damasio AR, Damasio H. Lesion analysis in neuropsychology.
New York City: Oxford University Press, 1989.
[24] Wechsler DA. Wechsler adult intelligence scale Ð revised man-
ual. New York City: The Psychological Corporation, 1981.
[25] Goel V, Grafman J. Are the frontal lobes implicated in ``plan-
ning'' functions? Interpreting data from the Tower of Hanoi.
Neuropsychologia 1994;33(5):623±42.
[26] Mattis S. Dementia Rating Scale (DRS). Odessa, Florida:
Psychological Assessment Resources, 1988.
[27] Statview 50. In: Cary, editor. Statistical analysis program.
North Carolina: SAS Institute, 1998.
[28] Goel V, Grafman J, Tajik J, Gana S, Danto D. A study of the
performance of patients with frontal lobe lesions in a ®nancial
planning task. Brain 1997;120:1805±22 (Pt 10).
[29] Kafer KL, Hunter M. On testing the face validity of planning/
problem-solving tasks in a normal population. Journal of the
International Neuropsychological Society 1997;3(2):108±19.
[30] Dehaene S, Changeux JP. A hierarchical neuronal network for
planning behavior. Proceedings of the National Academy of
Sciences USA 1997;94(24):13,293±8.
[31] Spector L, Grafman J. Planning, neuropsychology and arti®cial
intelligence: cross-fertilization. In: Boller F, Grafman J, editors.
Handbook of neuropsychology, vol. 9, 1994. p. 377±92.
D. Carlin et al. / Neuropsychologia 38 (2000) 655±665 665