Embed Size (px)
DESCRIPTION
slide pituitary disorders
Citation preview

Dr. Made Ratna Saraswati, SpPDDr. Made Ratna Saraswati, SpPD
Faculty of Medicine, Udayana University, 2009
THE PITUITARY GLAND AND DISORDERS
Block Endocrine System, Metabolism, and Disorders

Further reading
David G Gardner, Dolores Shoback. Greenspan’s Basic and Clinical Endrocrinology 8th ed. Lange. McGraw Hill 2007.
Harrison’s Principles of Internal Medicine 17th ed. McGraw Hill 2008. (Part 15 Endocrinology and Metabolism)

Anatomy
The pituitary gland lies on the base of the skull in a portion of the sphenoid bone called the sella tursica.
Anterior pituitary is the most richly vascularized of all mammalian tissue (0.8 ml/g/min).

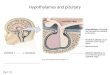
Fig. Anatomic relationships and blood supply of the pituitary gland
Greenspan’s Basic and Clinical Endrocrinology 8th ed. Lange, 2007. p. 104

Fig. Venous drainage of the pituitary gland
Greenspan’s Basic and Clinical Endrocrinology 8th ed. Lange, 2007. p. 105

Hypothalamic nuclei produce hormones that traverse to the portal system and impinge on anterior pituitary cells to regulate pituitary hormone secretion.
Posterior pituitary hormones are derived from direct neural extensions.

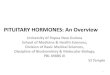
Neuroendocrine cell nuclei
Superior hypophyseal artery
Long portal vessels
Trophic hormone secreting cell
Anterior Pituitary
Posterior Pituitary
Short portal vessels
Inferior hypophyseal artery
Fig. Diagram of hypothalamic – pituitary vasculature
Harrison’s Principles of Internal Medicine, 17th ed. p. 2197
Hypothalamus
Stalk

The hypothalamic hormones
The hypothalamic hormones can be divided into: those secreted into hyppophysial portal blood vessels those secreted by the neurohypophysis directly into
the general circulation.

The hypophysiotropic hormones regulate the secretion of anterior pituitary hormones, include: Growth hormone-releasing hormone (GHRH) Somatostatin Dopamine Thyrotropin-releasing hormone (TRH) Corticotrophin-releasing hormone (CRH) Gonadotropoin-releasing hormone (GnRH).

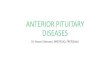
The anterior pituitary hormones
The six major anterior pituitary hormones are: Adrenocorticotropic hormone (ACTH) Growth hormone (GH) Prolactin (PRL) Thyroid-stimulating hormone (TSH) Luteinizing hormone (LH) Follicle-stimulating hormone (FSH)

The anterior pituitary is often referred to as the master gland because, together with the hypothalamus, it orchestrates
the complex regulatory functions of multiple other endocrine glands.

Fig. Diagram of pituitary axes
Harrison’s Principles of Internal Medicine, 17th ed. p. 2196

The posterior pituitary hormones
Antidiuretic hormone (ADH) Oxytocin

Hormonal feedback regulatory systems
The hypothalamus and pituitary gland form a unit which exerts control over the function of several endocrine glands: thyroid, adrenal, and gonads, as well as a wide range physiologic activities. This unit constitutes a paradigm of neuroendocrinology: brain-endocrine interactions

Fig. Feedback regulation of endocrine axes
Feedback control, both negative and positive, is a fundamental feature of endocrine system.
Each of the major hypothalamic - pituitary hormone axes is governed by negative feedback, a process that maintains hormone levels in the normal range
Harrison’s Principles of Internal Medicine, 17th
ed. p. 2192

Hormonal rhythms
The feedback regulatory systems are superimposed on hormonal rhythm that are used for adaptation to the environment,i e: seasonal changes, daily occurence of the light-dark cycle, sleep, meal, stress, etc.

Fig. The hypothalamic-pituitary-adrenal axis, ilustrating negative feedback by cortisol (F)
Greenspan’s Basic and Clinical Endrocrinology 8th ed. Lange,
2007. p. 114

Essentially all pituitary hormone rhythm are entrained to sleep and to the circadian cycle, generating reproducible patterns that are repeated approximately every 24 hours.
Recognition of this rhythm is important for endocrine testing and treatment.

Fig. The episodic, pulsatile pattern of ACTH secretion and its concordance with cortisol secretion in healthy human subject during the early morning
Greenspan’s Basic and Clinical Endrocrinology 8th ed. Lange, 2007. p. 115

Fig. Sleep associated changes in prolactine (PRL) and growth hormone (GH) secretion in human
Greenspan’s Basic and Clinical Endrocrinology 8th ed. Lange, 2007. p. 118

Peak levels of GH occur during sleep stages 3 or 4; The increase in PRL is observed 1 -2 hours after
sleep begins and is not associated with a specific sleep phase.

Pituitary and Hypothalamic disorders

Hypothalamic and pituitary lesions present with a variety of manifestations, including: pituitary hyper- and hyposecretion sellar enlargement visual loss.

Etiology
In adult, the most common cause of hypothalamic and pituitary disfunction is pituitary adenoma (the great majority is hypersecreting)
In children, the most frequent lesions causing hypothalamic and pituitary disfunction is craniopharyngioma, and other hypothalamic tumor.

Early manifestations
The earliest symptoms of such tumors are due to endocrinologic abnormalities, the most frequent manifestation: hypogonadism. Endocrine disturbance manifestation in children: low GH level, delayed puberty, diabetes insipidus).
Endocrinologic problem precede sellar enlargement and local manifestation (headache, visual loss) which are late manifestation (seen in patient with larger tumors or suprasellar extension)

Common and later manifestations
Pituitary hypersecretion Pituitary insufficiency Enlarged sella tursica Visual field defect Diabetes insipidus

1. Pituitary hypersecretion
PRL hypersecretion is the most common endocrine abnormality due to hypothalamic-pituitary disorders, and PRL is the hormone most commonly secreted in excess by pituitary adenoma.
GH-secreting adenomas are second in frequency to prolactinoma and cause the classic syndromes of acromegaly and gigantism.
ACTH hypersecretion leads to Cushing’s disease

2. Pituitary insufficiency
Panhypopituitarism is a classic manifestation of pituitary adenoma (but only present in less than 20% of cases because of earlier diagnosis)
The earliest manifestation in adult: hypogonadism secondary to elevated levels of PRL, GH, or ACTH and cortisol
In children the most frequent clinical manifestation is short stature (GH-deficiency should be considered).

3. Enlarged sella tursica
May cause by: pituitary adenoma or empty sella syndrome
Other less common cause: craniopharyngioma, lymphocytic hypophysitis, carotid artery aneurysm
Evaluation should include pituitary function: PRL, thyroid, and adrenal function.

4. Visual field defect
Manifestation: bitemporal hemianopsia, unexplained visual field defect, or visual loss considered to have hypothalamic or pituitary disorders until proved otherwise.
In addition to visual field defect, large pituitary lesion may extend laterally into the cavernous sinus, compromising the function of the third, fourth, or sixth cranial nerve, leading to diplopia.

5. Diabetes insipidus
DI is a common manifestation in hypothalamic disorder but rare in primary pituitary lesions.

Prolactinoma is the most common type (60%)GH hypersecretion (20%)ACTH excess (10%)Hypersecretion of TSH or the gonadotropin are unusual
Pituitary Adenoma
Pituitary microadenoma = intrasellar adenoma <1cmPituitary macroademo

Fig. Pituitary adenoma
Coronal T1-weighted postcontrast MR image shows a homogeneously enhancing mass (arrowheads) in the sella tursica and suprasellar region compatible with a pituitary adenoma; the small arrows outline the carotid arteries
Harrison’s Principles of Internal Medicine, 17th ed. p. 2202

Treatment
1. Surgery2. Irradiation3. Drug to supress hypersecretion by the
adenoma or its growth

Fig. Transsphenoidal resection of pituitary mass via the endonasal approach
Harrison’s Principles of Internal Medicine, 17th ed. p. 2203

GH hypersecretion is usually the result of a somatotrope adenoma, but may rarely caused by extrapituitary lesions
Acromegaly and Gigantism

Presentation and diagnosis
Manifestation of GH and IGF-1 hypersecretion are indolent and often are not clinically diagnosed for 10 years or more.
Acral bony overgrowth result in frontal bossing, increased hand and foot size, mandibular enlargement with prognathism, and widened space between the lower incisor teeth.
In children and adolescent, initiation of GH hypersecretion prior to epiphyseal long bone closure is associated with development of pituitary gigantism,

Soft tissue swelling: increased heel pad thickness, increased shoe or glove size, ring tightening, characteristic coarse facial features, including hyperhidrosis, deep and hollow sounding voice, oily skin, arthropathy, kyphosis, carpal tunnel syndrome, proximal muscle weakness and fatigue, acanthosis nigricans, and skin tags.
Generalized visceromegaly occurs including cardiomegaly, macroglossia, and thyroid enlargement.

Fig. Features of acromegaly/gigantism
A 22 year-old man with gigantism due to excess growth hormone is shown to the left of his identical twin. The increased height and prognathism of the affected twin are apparent. Their clinical features began to diverge at the age of 13 years.
Harrison’s Principles of Internal Medicine, 17th ed. p. 2210. Journal: R Gagel, IE McCutcheon, N Engl J Med 324:524;1999.

Enlarged hand and foot

Laboratory investigation
Age and gender matched serum IGF-1 levels (elevated)
Failure of GH supression to <1 µg/L within 1 - 2 h of oral glucose load (75g)
Ultrasensitive GH assay (nadir GH <0,05 µg/L) PRL should be test (25% with elevated PRL) Thyroid function, gonadotropin, and sex steroid
may be attenuated because of tumor mass effects.

• DI is the excretion of a large volume of urine (diabetes) that is hypotonic, dilute, and tasteless (insipid).
• Patient present with polyuria, the 24 hours urine volume is >50 ml/kg body weight, the osmolarity is <300 mosmol/L
• Other cause of polyuria such as osmotic diuresis that occur in diabetes mellitus or intrinsic renal disease must be excluded.
Vasopressin insufficiency: Diabetes Insipidus

The major effect of ADH is to increase the water permeability of the luminal membrane of the collecting duct in the kidney.
Diabetes insipidus is a disorder resulting from deficient ADH action and is characterized by the passage of amounts of very dilute urine.

GROUP DISCUSSION

Case 1: a woman with increasing shoe size
A 40 year old female has noticed an increase in her shoe size from 38 to 42, and her weight also increased from 68 to 80 kg. Her menstrual period has stopped 6 months ago. She also complained of acne on her face.
Physical examination found her 158 cm, blood pressure 140/80 mmHg. Neck demonstrated diffuse thyromegaly, but the TSHs and FT4 test was normal. Her face demonstrated thickening of the nasolabial fold and prominence of the supraorbital ridge. Compare to her picture 5 years before, her face showed a striking change in facial feature. She did not show hirsutism. Her hands and feet had a rubbery consistency.

Assignment:
What is the most likely disorder of this woman? What may cause this disorder? What laboratory and radiology test would you do
for the patient to workup the diagnosis? Is she has thyroid problem? Why? Why she stopped menstruating?

Self assessment:
1. Explain the hypothalamus – pituitary – target organ axis
2. Summarize the course and the condition associated with pituitary adenoma, including prolactinoma, acromegaly, gigantisme, growth hormone deficiency.
3. Summarize the normal physiologic hormone function of posterior pituitary
4. Describe the clinical features of diabetes insipidus

THANK YOU