Embed Size (px)
Citation preview
Pituitary And Thyroid
Pharmacology Team
Naim Kittana, Suhaib Hattab, Ansam Sawalha, Adham Abu Taha, Waleed Sweileh, Ramzi Shawahneh
Faculty of Medicine & Health SciencesAn-Najah National University 1
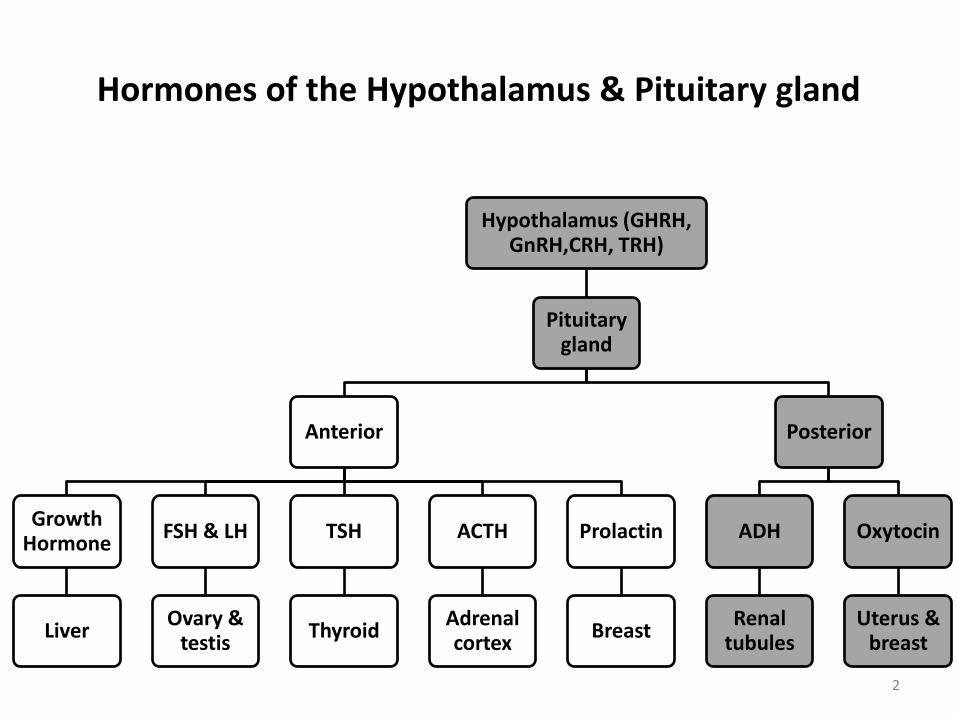
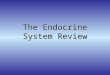
Hormones of the Hypothalamus & Pituitary gland
Hypothalamus (GHRH, GnRH,CRH, TRH)
Pituitary gland
Anterior
Growth Hormone
Liver
FSH & LH
Ovary & testis
TSH
Thyroid
ACTH
Adrenal cortex
Prolactin
Breast
Posterior
ADH
Renal tubules
Oxytocin
Uterus & breast
2
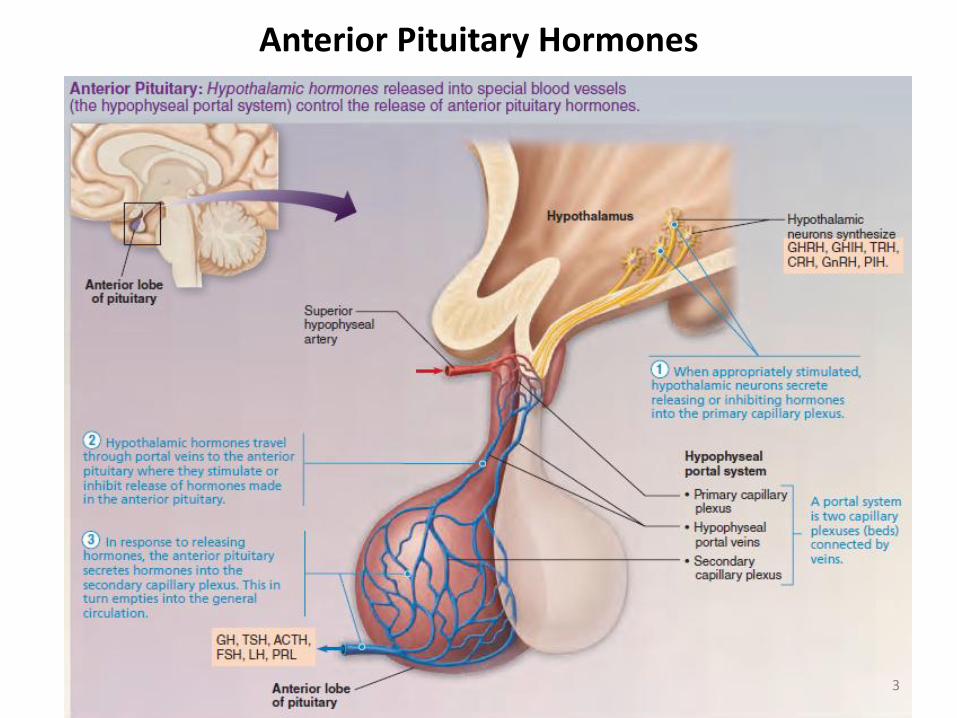
Anterior Pituitary Hormones
3
4

Hormones of the hypothalamus
5
1. Agents Affecting Growth Hormone (Somatotropin)
– Growth hormone-releasing hormone (GHRH)
• Released from the hypothalamus
• Binds to specific membrane GHRH receptors on pituitary.
• GHRH rapidly elevates serum growth hormone (somatotropin)
levels with high specificity.
6
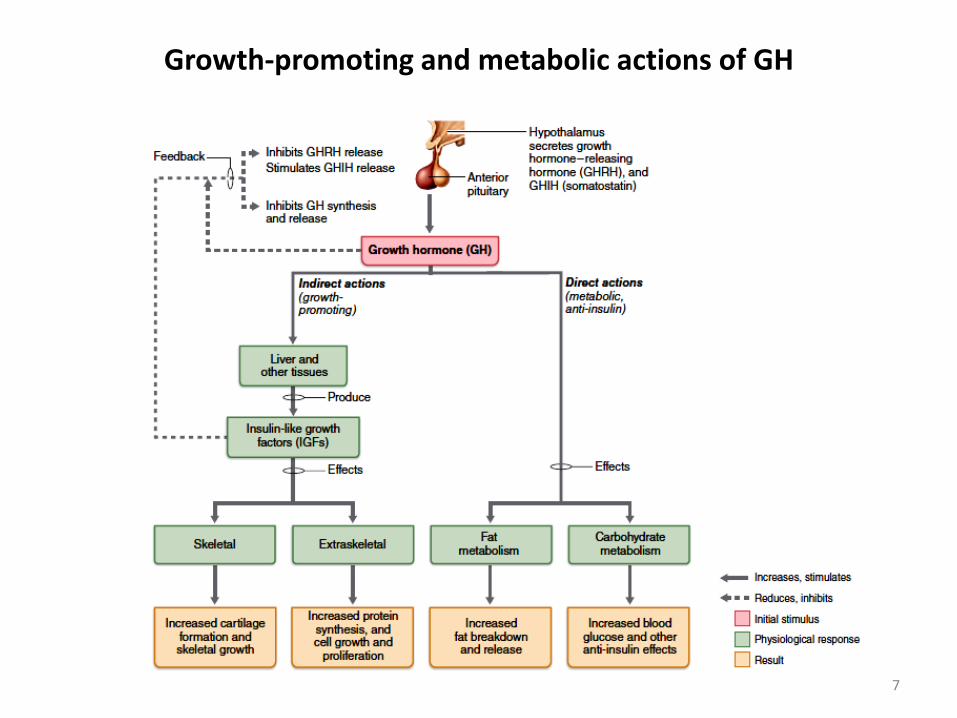
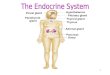
Growth-promoting and metabolic actions of GH
7
Growth hormone (GH)
• Hypersecretion causes gigantism in children and acromegaly in adults
• Hyposecretion in children causes pituitary dwarfism.
8
1. Agents Affecting Growth Hormone (Somatotropin)
– Somatotropin release-inhibiting hormone (SST, somatostatin)
• Inhibits the release of Somatotropin & TSH from the pituitary and the release of glucagon and insulin from the pancreas.
• Inhibits the secretion of a number of gut peptides such as vasoactiveintestinal polypeptide (VIP), and gastrin, and it inhibits the growth and proliferation of many cell types.
• Example of SST analogue: Octreotide
9
1. Agents Affecting Growth Hormone (Somatotropin)
• Octreotide is an SST analog administered by SC, IM, or IV injection.
• Octreotide is used to treat:
– Acromegaly
– Severe diarrhea associated with hypersecretory states such as VIP-secreting tumors (VIPomas)
– Gastrinoma
– Glucagonoma
– Variceal and upper GI bleeding
– TSH-secreting adenomas
10
• GnRH Analogs
– GnRH Receptor Agonists
• Leuprolide
• Gonadorelin
• Triptorelin
• Nafarelin
• Goserelin
• Histrelin
11
2. Gonadotropin-releasing Hormone (GnRH) and Analogs
2. Gonadotropin-releasing Hormone (GnRH) and Analogs
Pulsatile administration
– Short-term or pulsatile administration of GnRH agonists (every 1–4 h) increases the synthesis and release of both LH & FSH
– Treatment of certain types of infertility
12
Chronic administration
– 2–4 weeks of daily administration of GnRH inhibits the release of both LH & FSH by causing a reduction in the number of GnRH receptors on the anterior pituitary.
– Leads to reduced production of gonadal steroids; Androgens & Estrogens (chemical castration).
– Useful in the treatment of precocciuos puberty and hormone-dependent cancers and hyperplasias such as prostate cancer, breast cancer, endometriosis, and fibroids.
– Available as implantable formulation
13
2. Gonadotropin-releasing Hormone (GnRH) and Analogs
Adverse effects in Women:
– Hot flushes and sweating
– Diminished libido and depression
– Ovarian cysts
– Contraindicated in pregnancy and breast-feeding
14
2. Gonadotropin-releasing Hormone (GnRH) and Analogs
Adverse effects in Men:
– Hot flushes and edema
– Bone pain due to initial rise in testosterone levels
– Diminished libido
– Gynecomastia
15
2. Gonadotropin-releasing Hormone (GnRH) and Analogs
– Common example:
• Ganirelix
• Abarelix
• Cetrorelix
• GnRH antagonists competitively and reversibly bind to GnRH receptors in the pituitary gland, blocking the release of LH and FSH from the pituitary.
16
GnRH Receptor Antagonists
• In men, the reduction in LH subsequently leads to rapid suppression of testosterone release from the testes
• In women it leads to suppression of estrogen release from the ovaries.
• Unlike the GnRH agonists, which cause an initial surge in testosterone or estrogen levels, GnRH antagonists have an immediate onset of action, rapidly reducing sex hormone levels without an initial surge
17
GnRH Receptor Antagonists

• Prostate cancer
• Hormone-sensitive breast cancer and some benign disorders such as endometriosis and uterine fibroids
• Some cases of infertility: Prevents premature LH surge
18
Clinical Uses of GnRH Receptor Antagonists
3. Prolactin-releasing factor (PRF) and prolactin-inhibiting factor (PIF)
– Secretion of prolactin from the pituitary is controlled by both:
• Stimulation (mediated by PRF)
• Inhibition (mediated by PIF = dopamine)
19
Prolactin-releasing factor (PRF)
• Drugs that reduce CNS dopaminergic activity cause an increase in prolactinsecretion:
₋ Antipsychotics
₋ Antidepressants
₋ Anti-anxiety
Drugs that promote prolactin secretion are used to treat lactation failure.
20
Prolactin-inhibiting factor (PIF)
• Inhibition of prolactin secretion can be produced by a number of dopamineagonists:
– Bromocriptine acts as an agonist of dopamine D2-receptors and an
antagonist of D1-receptors.
– Cabergoline is a potent D2 agonist with greater D2 selectivity. It is more
effective in reducing hyperprolactinemia than bromocriptine and has a
long half-life that permits twice-weekly dosing.
21
Prolactin-inhibiting factor (PIF)
– Therapeutic uses of PIF:
• Inhibition of prolactin secretion in amenorrhea, galactorrhea, and prolactin-secreting tumors
• The correction of female infertility secondary to hyperprolactinemia
• Treatment of Parkinson disease.
22

23
Hormones of the anterior pituitary
Growth hormone
– Growth hormone agonists (GH, somatotropin), methionyl-growth hormone (somatrem)
– GH is released in a pulsatile manner, with the highest levels during sleep
– GH secretion decreases with increasing age
– Administered SC or IM
– Half-life: 25 min, but sufficient to induce IGF-1 release by the liver, which is responsible for the GH-like actions
24
– Therapeutic uses of GH:
• Replacement therapy in children with GH deficiency before
epiphyseal closure
• Growth failure due to Prader-Willi syndrome
• To stimulate growth in patients with Turner syndrome
• Other approved uses include long-term replacement of GH
deficiency in adults, treatment of cachexia and AIDS wasting
25
Growth hormone

– Side effects of GH:
• Edema
• Arthralgias and myalgias
• Flue-like symptoms
• Increase the risk of Diabetes
• Should not be given to children with closed epiphysis
26
Growth hormone
Growth hormone antagonists
– Pegvisomant
• Pegvisomant is a GH receptor antagonist
• Blocks the action of endogenous GH
• Used specifically for the treatment of acromegaly
• Pegvisomant is administered SC
27
Gonadotropins (LH & FSH)
• Gonadotropins (Luteinizing hormone and follicle-stimulating hormone)
– Actions and pharmacologic properties:
• In women,
– LH increases estrogen production in the ovary and is required for progesterone production by the corpus luteum after ovulation
– FSH is required for normal development and maturation of the ovarian follicles
• In men,
– LH induces testosterone production by the interstitial (Leydig) cells of the testis
– FSH acts on the testis to stimulate spermatogenesis and the synthesis of androgen-binding protein
28
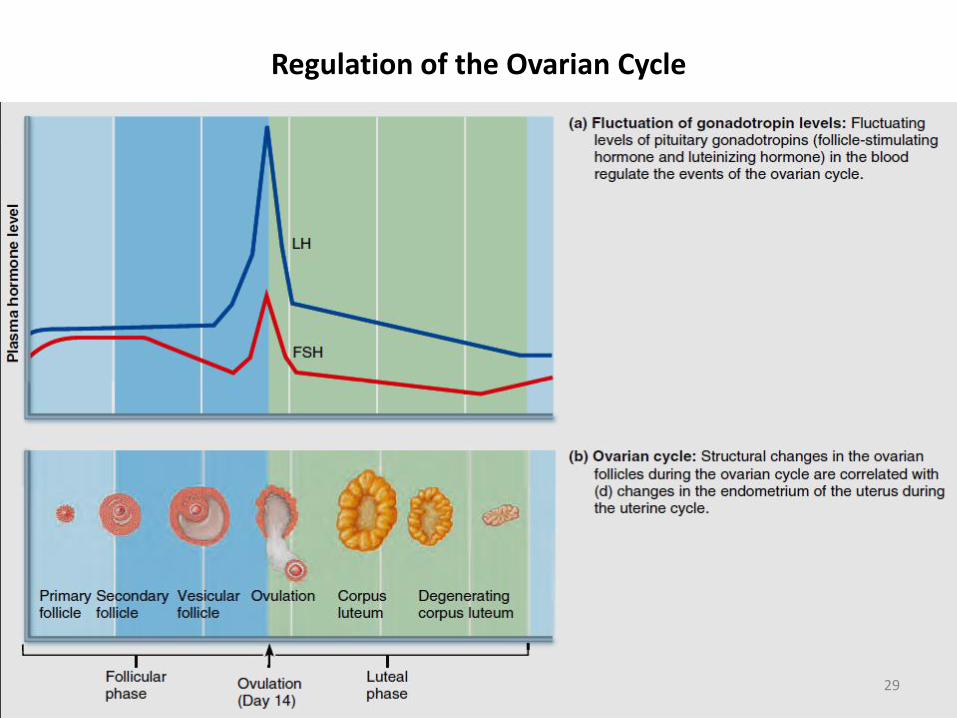
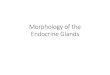
Regulation of the Ovarian Cycle
29
– FSH and LH of pituitary origin are not used pharmacologically.
– Menotropins (human menopausal gonadotropins, hMG) :
• Isolated from the urine of postmenopausal women
• Contain a mixture of LH and FSH
• Urofollitropin (Bravelle) is immunologically purified FSH from the urine of pregnant women.
– Follitropin α/β are recombinant FSH products
30
Gonadotropins (LH & FSH)
– hCG:
• Produced by the placenta and can be isolated and purified from the urine of pregnant women
• The alpha subunit is made by recombinant DNA technology (choriogonadotropin α)
• hCG is nearly identical in activity to LH
– All of these hormones must be administered parenterally (SC or IM)
31
Gonadotropins (LH & FSH)
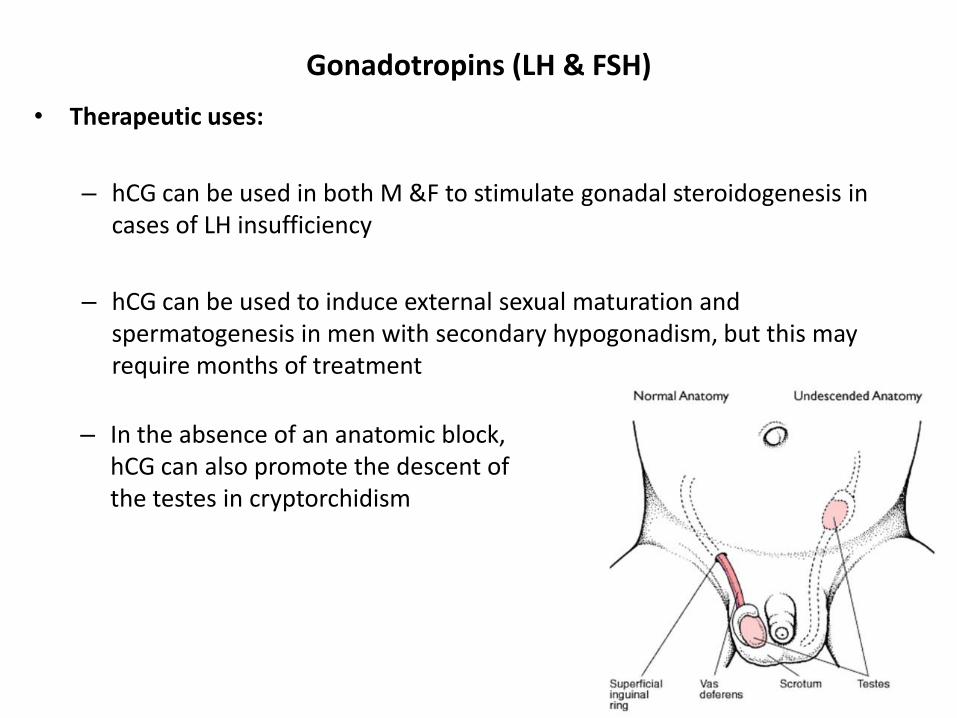
• Therapeutic uses:
– hCG can be used in both M &F to stimulate gonadal steroidogenesis in cases of LH insufficiency
– hCG can be used to induce external sexual maturation and spermatogenesis in men with secondary hypogonadism, but this may require months of treatment
32
Gonadotropins (LH & FSH)
– In the absence of an anatomic block, hCG can also promote the descent of the testes in cryptorchidism
• Therapeutic uses:
– Menotropins (hMG) are used in concert with hCG to stimulate ovulation in women with functioning ovaries:
Injection of hMG or FSH products over a period of 5-12 days causes ovarian follicular growth and maturation, then hCG is injected one day after the last dose of FSH to induce ovulation.
33
Gonadotropins (LH & FSH)
• Adverse effects
– Menotropins and hCG cause ovarian enlargement in about 20% of treated women
– Menotropins and hCG may cause ovarian life-threatening hyperstimulationsyndrome in up to 1% of patients:
– Acute respiratory distress
– Ascites
– Hypovolemia and shock
34
Gonadotropins (LH & FSH)
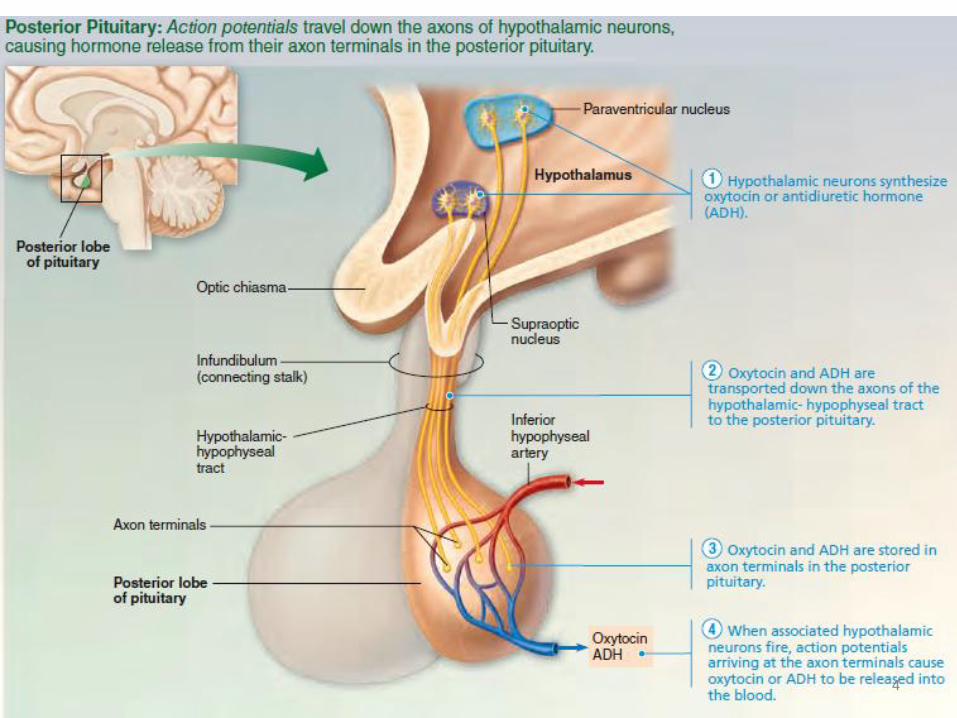
Hormones of the posterior pituitary
35

Anti-diuretic Hormone (ADH, Vasopressin)
– ADH is synthesized in the hypothalamus and stored in the posterior pituitary
– ADH is released in response to increasing plasma osmolarity or a fall in blood pressure
– The actions of ADH are mediated by three types of specific receptors:
• V1a: located in vascular smooth muscle, myometrium, and kidney
• V1b: located in the CNS and adrenal medulla
• V2: located in renal tubules
36
Anti-diuretic Hormone (ADH, Vasopressin)
• In renal tubules, ADH causes the permeability of water to increase and also increases the transport of urea in the inner medullary collecting duct, which increases the urine-concentrating ability of the kidney
• ADH causes vasoconstriction at higher doses
• ADH stimulates the hepatic synthesis of coagulation factor VIII and von Willebrand factor.
37
– ADH preparations
• Aqueous vasopressin (Pitressin), a short-acting preparation that acts on both V1 and V2 receptors, is administered parenterally and lasts 2–6 hours
• Desmopressin acetate (DDAVP, Stimate) is a longer lasting (10–20 h) preparation administered intranasally, parenterally, or orally
38
Anti-diuretic Hormone (ADH, Vasopressin)

– Therapeutic uses
• Desmopressin is the most effective treatment for severe central diabetes insipidus because its V2 activity is 3,000 times greater than its V1 activity; but it is not effective in the nephrogenic form of the disease
• Vasopressin is included in the advanced cardiac life support protocol as a substitute for epinephrine in cardiac arrest with asystole
• Desmopressin is useful in nocturnal enuresis by reducing nighttime urine production
39
Anti-diuretic Hormone (ADH, Vasopressin)
Oxytocin
– Oxytocin is synthesized in the hypothalamus and secreted by the posterior pituitary.
– Actions and pharmacologic properties
• Elicits milk ejection from the breast.
• Stimulates contraction of uterine smooth muscle.
• The plasma t1/2 of oxytocin is 5–10 minutes.
– Therapeutic uses
• Is used for induction and maintenance of labor.
• Stimulates milk ejection from the breast.
• Postpartum uterine bleeding.
40

41
The Thyroid Gland
Synthesis of thyroid hormones
• Thyroid hormones:
Triiodothyronine (T3)
Tetraiodothyronine (T4, thyroxine)
• Sythesis materials: iodine & tyrosine
42
Synthesis of thyroid hormones
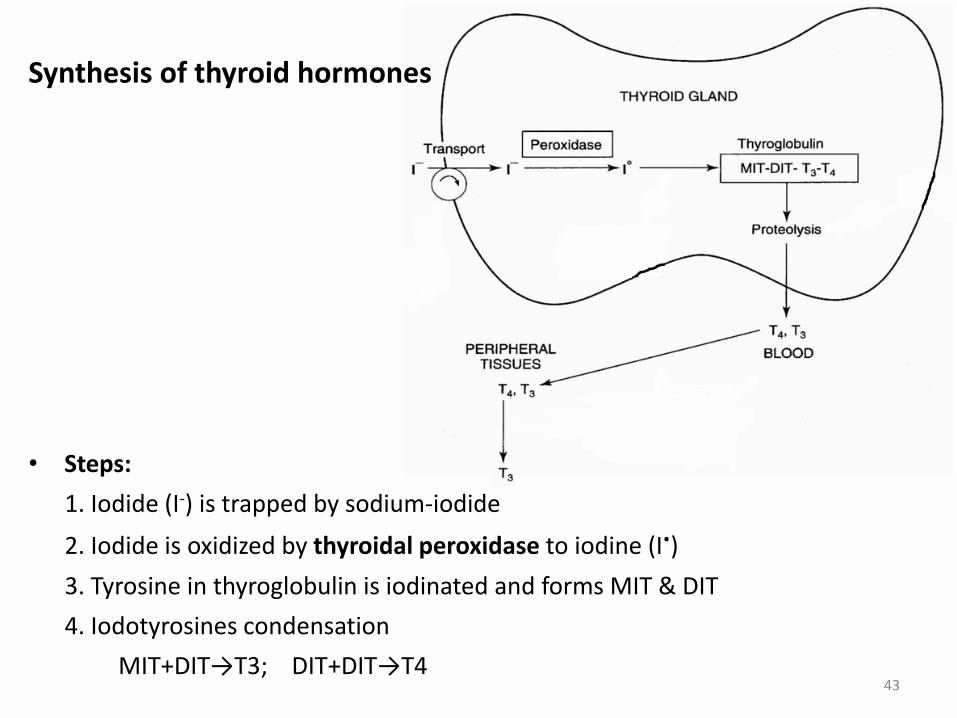
• Steps:
1. Iodide (I-) is trapped by sodium-iodide
2. Iodide is oxidized by thyroidal peroxidase to iodine (I.)
3. Tyrosine in thyroglobulin is iodinated and forms MIT & DIT
4. Iodotyrosines condensation
MIT+DIT→T3; DIT+DIT→T443
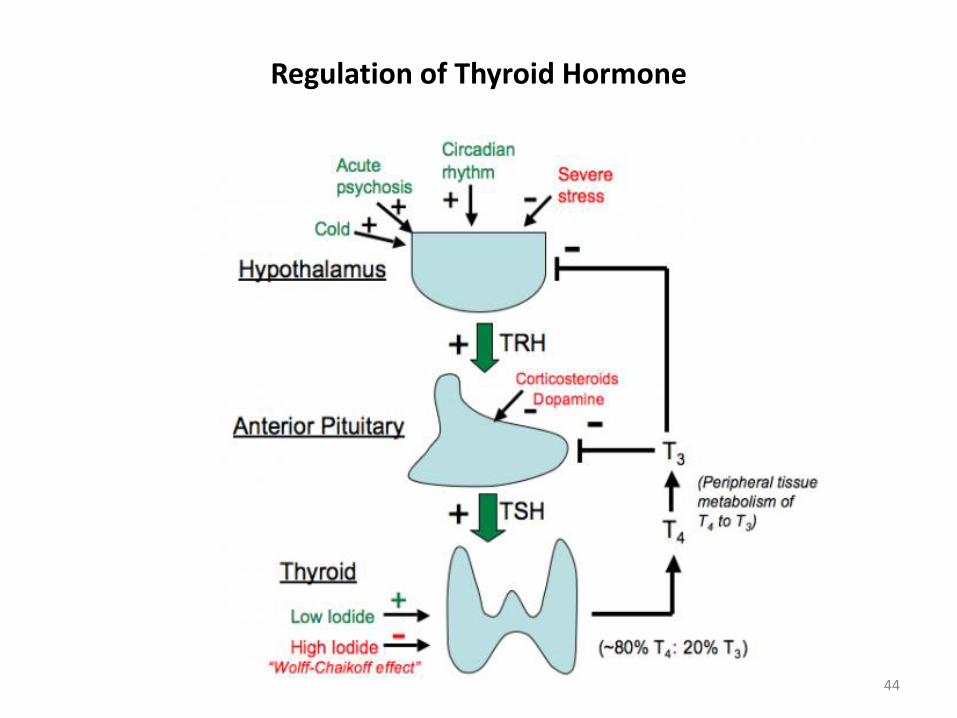
Regulation of Thyroid Hormone
44
Physiological actions of thyroid hormones
• To normalize growth and development, body temperature, and energy levels
• Eitiology of hypothyroidism:
Hashimoto disease
Simple goiter
After surgery and ablation of thyroid after surgery
Congenital
• Insufficiency (Hypothyroidism) causes:
Cretinism (infant & child)
Myxedema (adult)
45
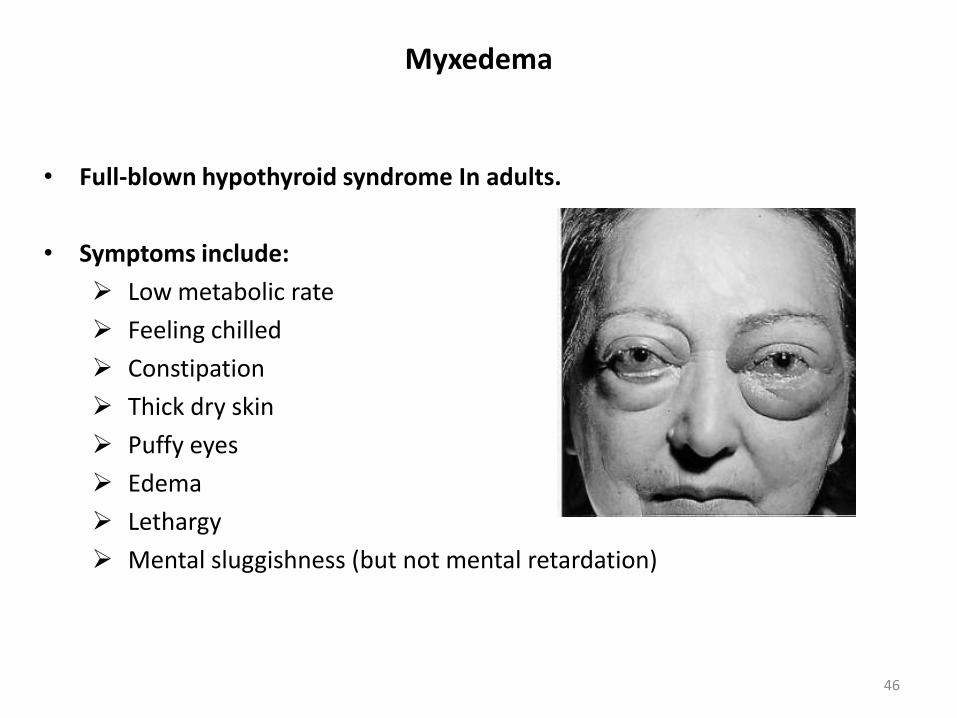
• Full-blown hypothyroid syndrome In adults.
• Symptoms include:
Low metabolic rate
Feeling chilled
Constipation
Thick dry skin
Puffy eyes
Edema
Lethargy
Mental sluggishness (but not mental retardation)
Myxedema
46
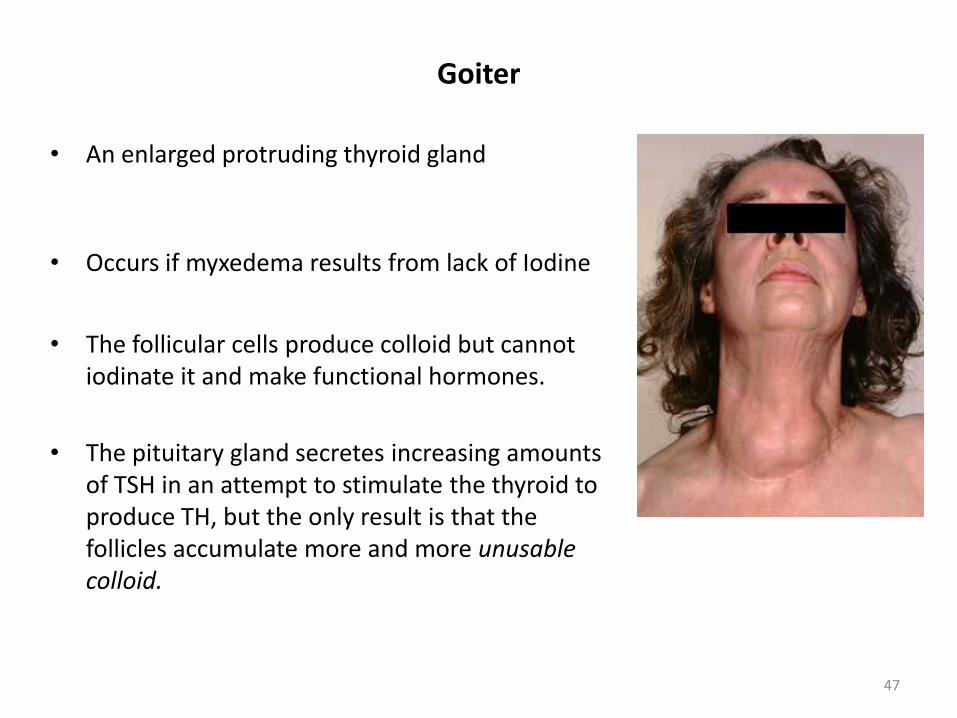
Goiter
• An enlarged protruding thyroid gland
• Occurs if myxedema results from lack of Iodine
• The follicular cells produce colloid but cannot iodinate it and make functional hormones.
• The pituitary gland secretes increasing amounts of TSH in an attempt to stimulate the thyroid to produce TH, but the only result is that the follicles accumulate more and more unusable colloid.
47
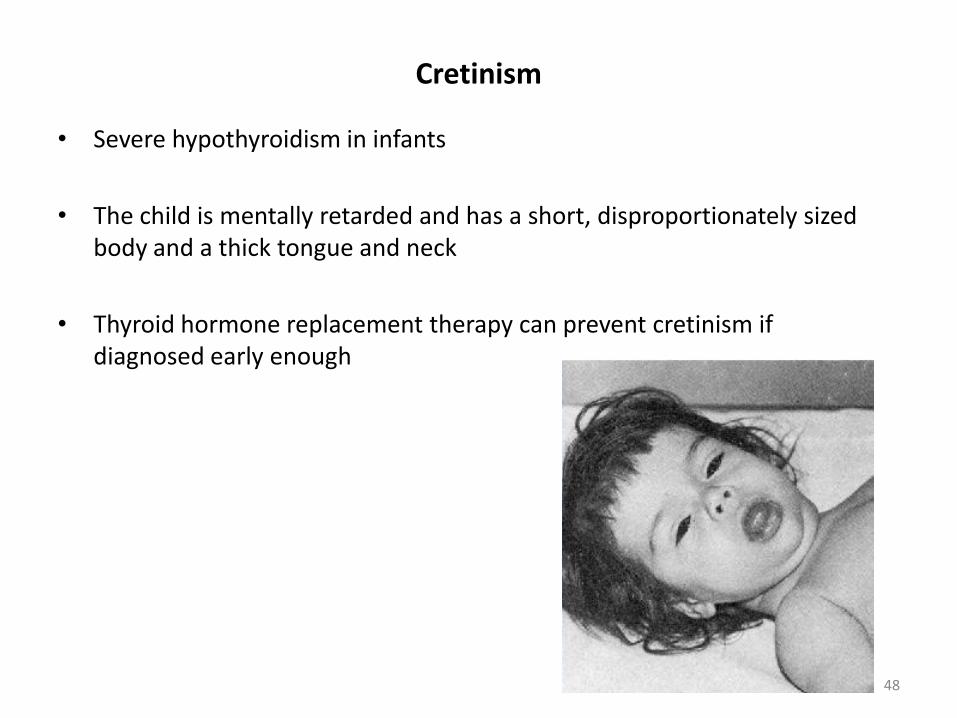
Cretinism
• Severe hypothyroidism in infants
• The child is mentally retarded and has a short, disproportionately sized body and a thick tongue and neck
• Thyroid hormone replacement therapy can prevent cretinism if diagnosed early enough
48
Physiological actions of thyroid hormones
• Excess secretion of thyroid hormone (Hyperthyroidism) most commonly results from: Graves disease and toxic goiter
• Severe Hyperthyroidism: results in thyrotoxicosis (thyroid storm)
49
Graves’ disease
• The most common hyperthyroid disease
• It is an autoimmune condition, where abnormal antibodies are directed against thyroid follicular cells.
• Rather than marking these cells for destruction as antibodies normally do, these antibodies mimic TSH and continuously stimulate TH release.
50
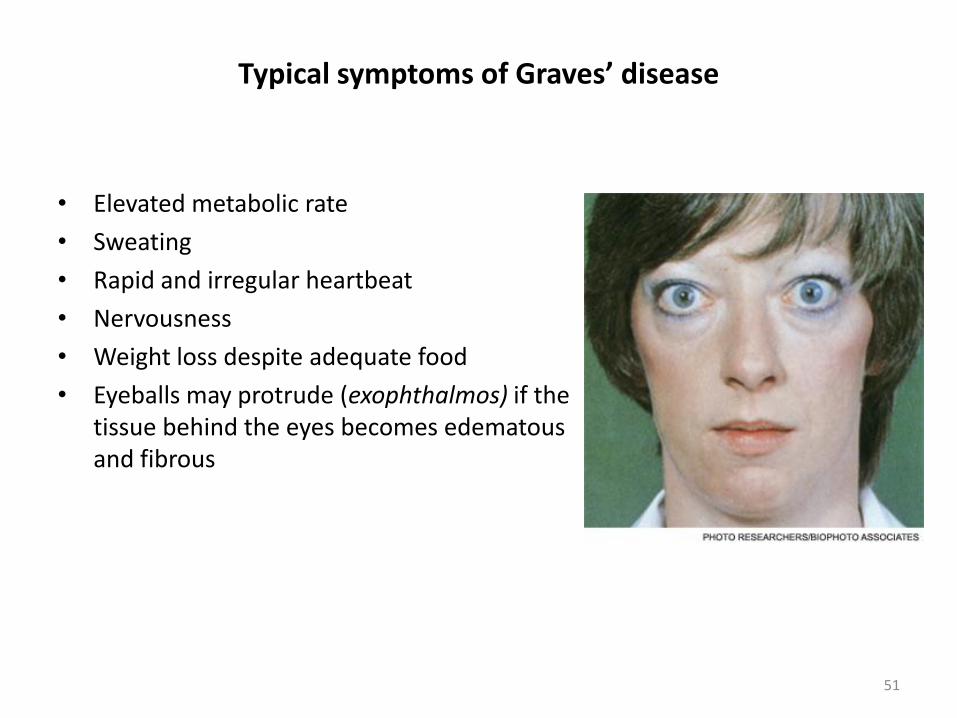
Typical symptoms of Graves’ disease
• Elevated metabolic rate
• Sweating
• Rapid and irregular heartbeat
• Nervousness
• Weight loss despite adequate food
• Eyeballs may protrude (exophthalmos) if the tissue behind the eyes becomes edematous and fibrous
51
52
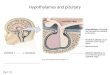
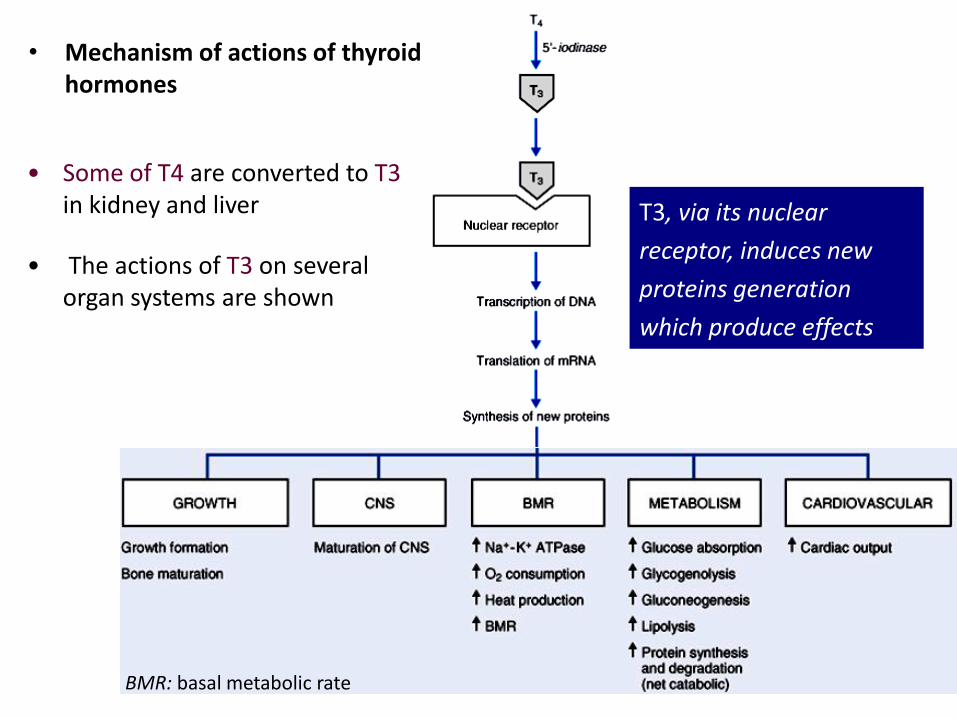
• Some of T4 are converted to T3in kidney and liver
• The actions of T3 on several organ systems are shown
• Mechanism of actions of thyroid hormones
T3, via its nuclear
receptor, induces new
proteins generation
which produce effects
BMR: basal metabolic rate
Thyroid drugs
53
• Representative drugs: levothyroxine (L-T4), liothyronine (T3)
Clinical use:
1. Hypothyroidism: cretinism & myxedema;
2. simple goiter
3. Others
Adverse reactions:
Overdose leads to thyrotoxicosis and angina or MI (usually in ageds)
Anti-thyroid drugs
54
Class Representative
Thioamides Propylthiouracil (PTU)
Methimazole
Iodides KI, NaI
Radioactive iodine 131I
β-adrenoceptor blockers Propranolol
Thioamides
55
Mechanism of action: All thioamides inhibit
Peroxidase-catalyzing reactions
Iodine organification
Iodotyrosines condensation
Propylthiouracil also inhibit T4 conversion into T3
Pharmacological action: They inhibit thyroid hormone synthesis
Thioamides
56
Thioamaides have no effects on thyroglobulin already stored in the gland, as a
result the clinical effects appears slowly until thyroglobulin stores are depleted.
Methemazole is preferred over PTU because it has a longer t1/2 (given once
daily)
PTU is recommended during the first trimester of pregnancy, due to a greater
risk of teratogenecity associated with methimazole.
Clinical use of Thioamides
• Mild hyperthyroidism and for those surgery & 131I are not permitted;
• Operation preparation
• Thyroid crisis (comprehensive therapy).
57
Adverse effects of Thioamides
• Long-term use leads to thyroid hyperplasia
• Pruritic maculopapular rash is the most common adverse reaction
• Agranulocytosis
58
Iodides (NaI, KI)
• Pharmacological action (Wolff-Chaikoff effect): Inhibition of T3 & T4
release and synthesis.
• This effect lasts only for few weeks
• Decrease of size & vascularity of the hyperplastic gland
59
Iodides (NaI, KI)
Clinical use
• Treatment of Thyroid Storm
• Prior to surgery (Decrease of size & vascularity of the gland)
60
Adverse reactions
• Acneiform rash
• Swollen salivary glands and mucous membrane ulcerations
Radioactive iodine (131I)
• 131I is the only isotope for treatment of thyrotoxicosis.
• Its therapeutic effect depends on emission of β rays with an effective half-
life of 5 days & a penetration range of 0.4-2 mm.
• Woman in pregnancy or lactation is forbidden!
61
β-adrenoceptor blockers
• βblockers are effective in treatment of thyrotoxicosis.
• Propranolol is the most widely studied and used.
62
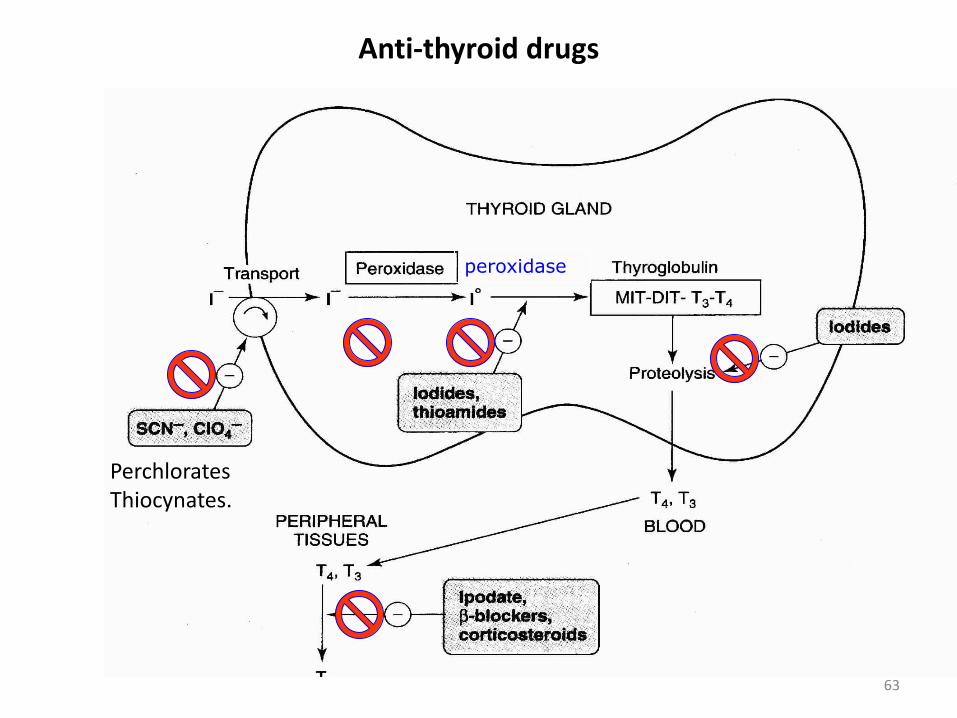
Anti-thyroid drugs
peroxidase
PerchloratesThiocynates.
63