Embed Size (px)
Citation preview
INTRODUCTION
METHODS
FIGURE 1
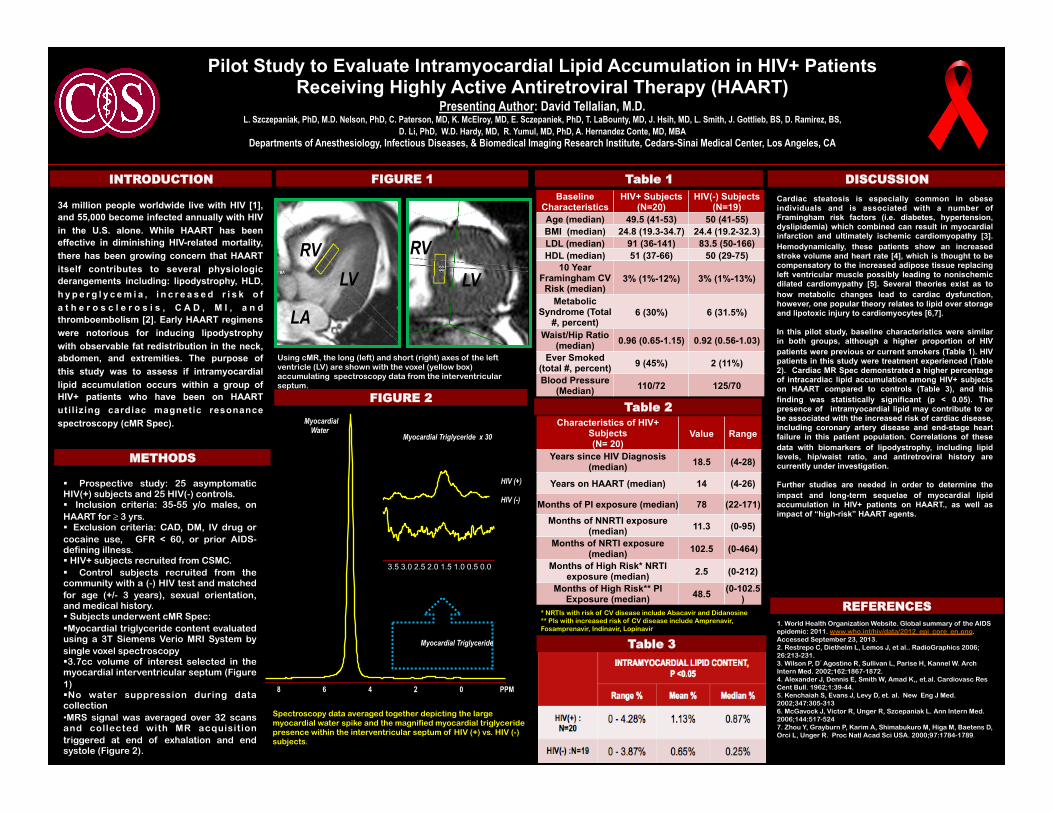
FIGURE 2
DISCUSSION
REFERENCES 1. World Health Organization Website. Global summary of the AIDS epidemic: 2011. www.who.int/hiv/data/2012_epi_core_en.png. Accessed September 23, 2013. 2. Restrepo C, Diethelm L, Lemos J, et al.. RadioGraphics 2006; 26:213-231. 3. Wilson P, D’Agostino R, Sullivan L, Parise H, Kannel W. Arch Intern Med. 2002;162:1867-1872. 4. Alexander J, Dennis E, Smith W, Amad K,, et.al. Cardiovasc Res Cent Bull. 1962;1:39-44. 5. Kenchaiah S, Evans J, Levy D, et. al. New Eng J Med. 2002;347:305-313 6. McGavock J, Victor R, Unger R, Szcepaniak L. Ann Intern Med. 2006;144:517-524 7. Zhou Y, Grayburn P, Karim A, Shimabukuro M, Higa M, Baetens D, Orci L, Unger R. Proc Natl Acad Sci USA. 2000;97:1784-1789.
Spectroscopy data averaged together depicting the large myocardial water spike and the magnified myocardial triglyceride presence within the interventricular septum of HIV (+) vs. HIV (-) subjects.
Using cMR, the long (left) and short (right) axes of the left ventricle (LV) are shown with the voxel (yellow box) accumulating spectroscopy data from the interventricular septum.
LV RV
LA
LV RV
8 6 4 2 0 PPM
Myocardial Triglyceride
Myocardial Water
3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0
Myocardial Triglyceride x 30
HIV (+) HIV (-)
Table 3
* NRTIs with risk of CV disease include Abacavir and Didanosine ** PIs with increased risk of CV disease include Amprenavir, Fosamprenavir, Indinavir, Lopinavir
Pilot Study to Evaluate Intramyocardial Lipid Accumulation in HIV+ Patients Receiving Highly Active Antiretroviral Therapy (HAART)
Presenting Author: David Tellalian, M.D. L. Szczepaniak, PhD, M.D. Nelson, PhD, C. Paterson, MD, K. McElroy, MD, E. Sczepaniek, PhD, T. LaBounty, MD, J. Hsih, MD, L. Smith, J. Gottlieb, BS, D. Ramirez, BS,
D. Li, PhD, W.D. Hardy, MD, R. Yumul, MD, PhD, A. Hernandez Conte, MD, MBA Departments of Anesthesiology, Infectious Diseases, & Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA
34 million people worldwide live with HIV [1], and 55,000 become infected annually with HIV in the U.S. alone. While HAART has been effective in diminishing HIV-related mortality, there has been growing concern that HAART itself contributes to several physiologic derangements including: lipodystrophy, HLD, h y p e r g l y c e m i a , i n c r e a s e d r i s k o f a t h e r o s c l e r o s i s , C A D , M I , a n d thromboembolism [2]. Early HAART regimens were notorious for inducing lipodystrophy with observable fat redistribution in the neck, abdomen, and extremities. The purpose of this study was to assess if intramyocardial lipid accumulation occurs within a group of HIV+ patients who have been on HAART uti l izing cardiac magnetic resonance spectroscopy (cMR Spec).
§ Prospective study: 25 asymptomatic HIV(+) subjects and 25 HIV(-) controls. § Inclusion criteria: 35-55 y/o males, on HAART for ≥ 3 yrs. § Exclusion criteria: CAD, DM, IV drug or cocaine use, GFR < 60, or prior AIDS-defining illness. § HIV+ subjects recruited from CSMC. § Control subjects recruited from the community with a (-) HIV test and matched for age (+/- 3 years), sexual orientation, and medical history. § Subjects underwent cMR Spec: § Myocardial triglyceride content evaluated using a 3T Siemens Verio MRI System by single voxel spectroscopy § 3.7cc volume of interest selected in the myocardial interventricular septum (Figure 1) § No water suppression during data collection • MRS signal was averaged over 32 scans and collected with MR acquisition triggered at end of exhalation and end systole (Figure 2).
Table 1
Cardiac steatosis is especially common in obese individuals and is associated with a number of Framingham risk factors (i.e. diabetes, hypertension, dyslipidemia) which combined can result in myocardial infarction and ultimately ischemic cardiomyopathy [3]. Hemodynamically, these patients show an increased stroke volume and heart rate [4], which is thought to be compensatory to the increased adipose tissue replacing left ventricular muscle possibly leading to nonischemic dilated cardiomypathy [5]. Several theories exist as to how metabolic changes lead to cardiac dysfunction, however, one popular theory relates to lipid over storage and lipotoxic injury to cardiomyocytes [6,7]. In this pilot study, baseline characteristics were similar in both groups, although a higher proportion of HIV patients were previous or current smokers (Table 1). HIV patients in this study were treatment experienced (Table 2). Cardiac MR Spec demonstrated a higher percentage of intracardiac lipid accumulation among HIV+ subjects on HAART compared to controls (Table 3), and this finding was statistically significant (p < 0.05). The presence of intramyocardial lipid may contribute to or be associated with the increased risk of cardiac disease, including coronary artery disease and end-stage heart failure in this patient population. Correlations of these data with biomarkers of lipodystrophy, including lipid levels, hip/waist ratio, and antiretroviral history are currently under investigation. Further studies are needed in order to determine the impact and long-term sequelae of myocardial lipid accumulation in HIV+ patients on HAART., as well as impact of “high-risk” HAART agents.
Table 2 Characteristics of HIV+
Subjects (N= 20)
Value Range
Years since HIV Diagnosis (median) 18.5 (4-28)
Years on HAART (median) 14 (4-26)
Months of PI exposure (median) 78 (22-171)
Months of NNRTI exposure (median) 11.3 (0-95)
Months of NRTI exposure (median) 102.5 (0-464)
Months of High Risk* NRTI exposure (median) 2.5 (0-212)
Months of High Risk** PI Exposure (median) 48.5 (0-102.5
)
Baseline Characteristics
HIV+ Subjects (N=20)
HIV(-) Subjects (N=19)
Age (median) 49.5 (41-53) 50 (41-55) BMI (median) 24.8 (19.3-34.7) 24.4 (19.2-32.3) LDL (median) 91 (36-141) 83.5 (50-166) HDL (median) 51 (37-66) 50 (29-75)
10 Year Framingham CV Risk (median)
3% (1%-12%) 3% (1%-13%)
Metabolic Syndrome (Total
#, percent) 6 (30%) 6 (31.5%)
Waist/Hip Ratio (median) 0.96 (0.65-1.15) 0.92 (0.56-1.03)
Ever Smoked (total #, percent) 9 (45%) 2 (11%)
Blood Pressure (Median) 110/72 125/70





























