Embed Size (px)
Citation preview

Pilot Study of Massage in Veteranswith Knee Osteoarthritis
Michael Juberg, BA,1 Kristin K. Jerger, MD, LMBT,1 Kelli D. Allen, PhD,2,3
Natalia O. Dmitrieva, PhD,4 Teresa Keever, BSN, RN,1 and Adam I. Perlman, MD, MPH1
Abstract
Objectives: To (1) assess the feasibility and acceptability of Swedish massage among Department of VeteransAffairs (VA) health care users with knee osteoarthritis (OA) and (2) collect preliminary data on efficacy ofSwedish massage in this patient group.Design: Experimental pilot study.Setting: Duke Integrative Medicine clinic and VA Medical Center, Durham, North Carolina.Patients: Twenty-five veterans with symptomatic knee OA.Interventions: Eight weekly 1-hour sessions of full-body Swedish massage.Outcome measures: Primary: Western Ontario and McMaster University Osteoarthritis Index (WOMAC) andglobal pain (Visual Analog Scale [VAS]). Secondary: National Institutes of Health Patient Reported OutcomesMeasurement Information System-Pain Interference Questionnaire 6b (PROMIS-PI 6b), 12-Item Short-FormHealth Survey (SF-12 v1) and the EuroQol health status index (EQ-5D-5L), knee range of motion (ROM), andtime to walk 50 feet.Results: Study feasibility was established by a 92% retention rate with 99% of massage visits and 100% ofresearch visits completed. Results showed significant improvements in self-reported OA-related pain, stiffnessand function (30% improvement in Global WOMAC scores; p = 0.001) and knee pain over the past 7 days (36%improvement in VAS score; p < 0.001). PROMIS-PI, EQ-5D-5L, and physical composite score of the SF-12also significantly improved ( p < 0.01 for all), while the mental composite score of the SF-12 and knee ROMshowed trends toward significant improvement. Time to walk 50 feet did not significantly improve.Conclusions: Results of this pilot study support the feasibility and acceptability of Swedish massage among VAhealth care users as well as preliminary data suggesting its efficacy for reducing pain due to knee OA. If resultsare confirmed in a larger randomized trial, massage could be an important component of regular care for thesepatients.
Introduction
Osteoarthritis (OA) affects nearly 27 millionAmericans, and its prevalence is expected to rise con-
siderably in the next several decades.1 Knee OA is particu-larly common, with a lifetime risk of 45%.2 OA in general,and knee OA in particular, is more common in U.S. militaryveterans than in the general population, and Department ofVeterans Affairs (VA) health care users are at particularlyhigh risk.3 In addition, VA health care users with arthritis
(most commonly knee OA) have more severe symptoms andactivity limitations.4 In veterans, OA (including knee OA)commonly co-occurs with other chronic pain conditions,post-traumatic stress disorder, and substance abuse.5
Currently, a variety of conventional treatment options forknee OA are available, including pain medication, cortico-steroid injections, physical therapy, exercise, weight man-agement, and joint replacement surgery.6 When traditionaltreatment approaches are used, many patients with knee OAcontinue to experience symptoms such as chronic pain and
1Duke Integrative Medicine, Duke University Medical Center, Durham, NC.2Department of Medicine, Division of Rheumatology, and Thurston Arthritis Research Center, University of North Carolina at Chapel
Hill, Chapel Hill, NC.3Health Services Research and Development Service, Durham Veterans Affairs Medical Center, Durham, NC.4Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham, NC.
THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINEVolume 21, Number 6, 2015, pp. 333–338ª Mary Ann Liebert, Inc.DOI: 10.1089/acm.2014.0254
333

functional limitations that reduce quality of life.7 Accord-ingly, there remains a pressing need to identify additionaleffective, conservative treatments for knee OA that improvepain, functioning, and overall well-being in these patients.
Massage therapy is effective for musculoskeletal disor-ders, such as chronic back and neck pain,8 and is an effec-tive treatment for managing pain associated with knee OA.9
For massage to be integrated into a comprehensive painmanagement program, a systematic approach and dosage ofmassage therapy needs to be established. A prior study dem-onstrated the efficacy of a specific manualized protocol ofSwedish massage for improving pain, stiffness, and func-tioning due to knee OA in non-veterans.9 A subsequent studyestablished an optimal dosage for the protocol: eight weekly1-hour sessions.10
Although there is promising evidence for massage as aneffective treatment for knee OA, further studies must evaluateits effectiveness in diverse patient groups. VA health careusers are an important patient group for studying this treat-ment for several reasons. First, given VA health care users’particularly high risk for activity-limiting knee OA, it is im-portant to identify effective interventions for this vulnerablepatient group. Second, the demographic profile of VA healthcare users differs substantially from that of participant sam-ples in previous studies of massage for knee OA.9,10 Most ofthese patients are men, and the acceptability of massage inthis group has not been sufficiently evaluated. Third, VAhealth care users with knee OA have higher levels of physicaland psychological comorbidities that could influence or beaffected by massage.5 This pilot study evaluated a previouslyestablished massage therapy protocol in a new population:VA health care users with knee OA. Core objectives of thisstudy were to (1) assess the feasibility and acceptability ofSwedish massage among VA health care users with knee OAand (2) collect preliminary data on the efficacy of Swedishmassage in this patient group.
Materials and Methods
This was a single group pilot study, with all participantsreceiving a 1-hour-per-week intervention of Swedish mas-sage for 8 weeks. Assessments were conducted before andafter the intervention. The institutional review boards ofDuke University and the Durham VA Medical Center re-viewed and approved the study.
Participants
Primary eligibility requirements included (1) VA healthcare users; (2) age ‡ 35 years; (3) written confirmation ofOA of the knee per American College of Rheumatologycriteria6 provided by the participant’s physician; (4) ra-diographically established OA of the knee; and (5) a pre-randomization score in a specified range on the VisualAnalog Scale (VAS; ‡ 40 mm and £ 90 mm on a 40–100 mmscale). For patients with bilateral knee involvement, the studyknee was determined by the patient as being the more prob-lematic/painful knee. Exclusion criteria included (1) any intra-articular knee depo-corticosteroid within the last 3 months, (2)intra-articular hyaluronate within the past 6 months, (3) ar-throscopy within the past year, (4) knee replacement surgery,(5) significant injury within the past 6 months, and (6) pres-ence of a rash or open wound over the knee. Participants
missing the research visit or three or more massage visitscould be withdrawn from the study at the discretion of thestudy principal investigator.
Patients with knee OA at the Durham VA Medical Centerwere recruited by using two methods. First, posters weredisplayed in clinic waiting rooms and other common areasof the medical center. Second, invitation letters were sentto patients who were identified as having knee OA fromDurham VA electronic medical records. These letters pro-vided basic information about the study and invited patientsto call if they were interested in participating. The first25 eligible participants to send a letter from their physicianverifying their diagnosis of knee OA were enrolled in thestudy. Participants meeting all criteria gave written informedconsent before enrolling in the study.
Study design and treatment
Participants received eight weekly 1-hour Swedish mas-sages at Duke Integrative Medicine’s clinical facilities, 1 milefrom the Durham VA Medical Center. Massage therapistswere certified by the National Certification Board forTherapeutic Massage & Bodywork adhered to a manualizedmassage protocol previously tested to treat OA of the knee.10
Therapists announced their next technique or position inorder to minimize potential client startle in a population withhigh prevalence of post-traumatic stress disorder. Each studytherapist signed a form attesting to adherence to the studyprotocol after each massage session.
The primary outcome measure used to assess OA-relatedpain, stiffness, and function was the Western Ontario andMcMaster University Arthritis Index (WOMAC) globalscore (VAS version). The WOMAC has been subject tonumerous validation studies to assess reliability and re-sponsiveness to change in therapy, including physical formsof therapy.11 In addition, participants were asked to respondto the question, ‘‘How much pain have you had because ofyour knee in the past week?’’ using a 100-point VAS.
Secondary outcomes included measures of other domainsof high relevance to patients with knee OA: the NationalInstitutes of Health Patient Reported Outcomes Measure-ment Information System-Pain Interference Questionnaire6b (PROMIS-PI 6b).12 This instrument consists of sixquestions that follow the format, ‘‘In the past 7 days, howmuch did pain interfere with [insert category]?’’ and allowsresponses on a 5-point scale (1 = not at all/never, 5 = verymuch/always). The six categories include enjoyment of life,ability to concentrate, day-to-day activities, enjoyment ofrecreational activities, doing tasks away from home (e.g.,getting groceries, running errands), and socializing withothers. Measures used to assess change in perceived healthstatus included EQ-5D-5L,13 a non–disease-specific instru-ment for describing and valuing health-related quality oflife, and the Short Form-12 (SF-12), version 1.14 The SF-12Health Survey is a 12-item subset of the SF-36 that mea-sures the same eight domains of health as the longer scale. Itis a brief, reliable measure of overall health status which isuseful in large population health surveys and has been usedextensively as a screening tool. Knee range of motion(ROM), measured manually with a goniometer to the onsetof stiffness, and 50-foot walk test were also measured.Maximal walking speed is a more reliable and predictive
334 JUBERG ET AL.

measure of walking ability than walking at a comfortablepace.15,16 Participants were asked to walk as fast as theysafely could with or without a walking aid. They were timedfrom a standing start until the point at which they walkedthrough the 50-foot (15.24-meter) marker. Additional post-study questions were asked of all participants during thefinal visit to assess study acceptability (Appendix 1).
Statistical analysis
Paired-samples t tests were used to examine the effects oftreatment on change in outcomes at baseline and immedi-ately after the intervention. In all analyses, statistical sig-nificance is reported using a two-tailed a level of 0.05 orless, and the 95% confidence interval for all parameter es-timates are provided. All analyses were carried out by usingSAS software, version 9.3 (SAS Institute, Cary, NC).
Results
Feasibility and participant characteristics
Of the 104 potential participants completing the telephonescreening, 56 were determined to be eligible (41 were ineli-gible and 7 declined participation), and the first 25 (n = 25) tosubmit a letter from their physician confirming the diagnosisof OA by radiography were enrolled. Among the 25 studyparticipants, the mean age was 57.0 (standard deviation,12.0); most participants were men (68%), 52% were black or
African American, and 68% were not employed (Table 1).During the study, 1 participant withdrew, and another par-ticipant was withdrawn by the principal investigator aftermissing three consecutive appointments. The remaining 23participants (92%) completed the study. Study feasibility wasestablished by the 92% retention rate with 99% of massagevisits and 100% of research visits completed.
Primary outcome measures
Participants’ mean WOMAC global score improved by30% ( p = 0.001), as shown in Table 2. Significant improve-ment was observed on all subscales of the WOMAC index,including the pain subscale ( p < 0.001), stiffness subscale( p = 0.006), and the function subscale ( p < 0.001). Partici-pants’ VAS scores also showed an average improvement of36% ( p < 0.001).
Secondary outcome measures
Perceived health status as measured with the EQ-5D-5Land the SF-12 also improved significantly (Table 3). Im-provements in the SF-12 physical composite score reachedstatistical significance ( p < 0.01). However, improvementsin the SF-12 mental component score only exhibited a trendtoward improvement ( p = 0.080). The PROMIS-PI 6b(Table 3) showed a 15% improvement ( p < 0.01). A trendin the expected direction was observed for knee ROM, but thisdid not reach statistical significance ( p = 0.087). There wasno significant change in the 50-foot walk test ( p = 0.121).
Responses to post-study questions confirmed acceptabil-ity, feasibility, and a positive response to the treatment (fullquestions and responses listed in Appendix 1; n = 23 for allquestions). These questions were not part of a standardizedinstrument but were developed specifically for this study toassess aspects of patient satisfaction that were important toevaluate in the context of this pilot/feasibility study. Anoverwhelming majority of respondents answered ‘‘yes’’ tothe following questions: ‘‘Would you like to continue mas-sage as part of the on-going management of your knee ar-thritis?’’ (91%) and ‘‘Was the schedule of visits (60 minutes/week) convenient for you?’’ (96%).
When asked about the likelihood that other veterans wouldwant to try massage if it were offered at the VA, 87% re-sponded that it was very likely or somewhat likely, and 83% ofrespondents answered ‘‘yes’’ to the post-study question: ‘‘Didyou notice any other changes in your health or other aspects ofyour life since starting the massage?’’
Table 1. Patient Characteristics
Characteristic Value
Total sample (n) 25Mean age at baseline (yr) 56.96 – 11.98Mean BMI (kg/m2) 31.58 – 7.71Men, n (%) 17 (68)Hispanic ethnicity, n (%) 0 (0)
Race, n (%)American Indian/Alaska Native 0 (0)Asian 1 (4)Black or African American 13 (52)Native Hawaiian or other Pacific Islander 0 (0)White 11 (44)
Currently employed (working for pay), n (%) 8 (32)
Values are expressed as the mean – standard deviation or number(percentage) of patients.
BMI, body–mass index.
Table 2. Changes in Primary Outcome Measures
VariableMean
before (SD)Mean
after (SD)Mean paired difference
(95% CI) p-ValuePercent
improvement
WOMACGlobal 66.4 (13.8) 45.4 (22.6) - 21.0 ( - 32.2 to - 9.9) 0.001* 30Pain 63.0 (14.8) 42.0 (27.3) - 22.5 ( - 33.6 to - 11.4) < 0.001* 37Stiffness 69.1 (18.0) 52.8 (24.0) - 16.3 ( - 27.5 to - 5.2) 0.006* 21Function 65.0 (13.7) 41.5 (21.0) - 23.6 ( - 35.0 to - 12.2) < 0.001* 32VAS 69.4 (13.8) 43.0 (25.1) - 26.4 ( - 38.5 to - 14.2) < 0.001* 36
*Indicates significance at level p < 0.05.CI, confidence interval; SD, standard deviation; VAS, visual analog scale; WOMAC, Western Ontario and McMaster University
Osteoarthritis Index.
MASSAGE FOR KNEE OA IN VA HEALTH CARE USERS 335

Discussion
This pilot study confirmed the feasibility of delivering amanualized protocol of Swedish massage for treating VAhealth care users with knee OA, with no significant re-cruitment barriers and both retention and treatment sessioncompletion rates over 90%. Only two participants failed tocomplete the full massage intervention, and neither case wasdue to perceived inefficacy of the massage therapy. Ac-ceptability of the intervention was high in this largely maleveteran population, with over 90% of participants indicatingthey would like to continue to receive massage as part oftheir treatment plan for knee OA.
Although preliminary, the data strongly supported thepotential efficacy of this treatment protocol for improvingoutcomes in VA health care users with knee OA. Resultswere consistent with findings from our previous studies in ageneral population.9,10 Percentages of improvements inWOMAC scores were well above the minimal clinicallyimportant differences (17%–22%) reported by Angst et al. intheir prospective cohort study of 192 patients with lowerlimb OA,17 with a 30% improvement in the global score,37% improvement on the pain subscale, and 32% im-provement on the function subscale. Pain interference andperceived health status also significantly improved over thecourse of the study.
This study’s findings raise important considerations forfuture studies of massage therapy for chronic pain condi-tions, such as knee OA. Its strong recruitment, retention, andfeasibility outcomes suggest that veterans need and arelargely receptive to massage as an intervention for pain dueto knee OA. It appears that no study has demonstrated thefeasibility and acceptability of providing professional out-patient massage for veterans with chronic pain due to kneeOA (or OA in any other joint) and simultaneously providedstrong preliminary results of significant pain reduction.These combined findings warrant a large-scale randomizedcontrolled trial to establish the clinical efficacy of massagefor veterans’ knee OA.
Prior studies have also documented the strong interest ofVA patients, providers, and administrators to make massagetherapy available across the VA for patients with chronicpain. In one large-scale study (n = 401) conducted acrossfive VA primary care clinics, 202 participants reported
having sought massage for their chronic pain, and 387participants (97%) reported willingness to try massagetherapy; thus, massage was the most preferred of the com-plementary and alternative medicine modalities studied(massage therapy, chiropractic care, herbal medicines, andacupuncture).18,19 A recent qualitative study of 28 patientcare providers and administrators at a large VA facility ratedmassage as the top priority for promotion within the VAover 18 other modalities.19 In this same study, althoughmany participants saw lack of funding as a barrier to pro-viding massage within the VA, others thought funding wasavailable in response to a well-planned request.
Several strategies for reducing long-term cost of massagefor chronic pain warrant further study. Home-based massageprograms are cost-effective and have demonstrated signifi-cant reductions in self-reported pain and anxiety in veteransfor conditions that include a substantial mental componentin addition to chronic pain, such as cancer and reintegrationafter return from active duty in Iraq or Afghanistan.20,21
Another pilot study in non-veterans recently showed thathome-based massage resulted improved symptoms amongpatients with knee OA.22 Larger studies are needed toevaluate whether home-based massage, either alone or as anadjunct to professional massage therapy, has benefit forveterans and others with knee OA. In addition, it would beuseful to evaluate the potential combined effects of massagetherapy (professional or home-based) with other therapiesthat could help to sustain benefits, such as mindfulness-based stress reduction, which is more effective and longerlasting for mood improvement than massage therapy.23
Finally, this study has several limitations common to pilotstudies, including a small sample size (n = 25), relativelyshort intervention duration, and lack of control group.However, this study provides important preliminary dataabout the feasibility and efficacy of Swedish massage in avulnerable and understudied patient group. In addition, thisstudy was limited to Swedish massage techniques. Althoughthis precludes generalizability to other possible techniques,it confers the advantage of standardizing the intervention ina health care system such as the VA.
In conclusion, this pilot study supports the feasibility andacceptability of Swedish massage among VA health careusers with knee OA. Preliminary data suggest the potentialefficacy of 8 weeks of 1-hour weekly massage for reduced
Table 3. Changes in Secondary Outcome Measures
Variable Pre PostPatients
(n) p-ValueChange (95% confidence
interval)
EQ-5D-5L 0.60 – .16 0.68 – .15 23 0.002a 0.08 (0.03 to 0.1)SF-12, PCS 28.1 – 7.5 33.6 – 10.5 13b 0.002a 5.5 (2.4 to 8.6)SF-12, MCS 43.7 – 18.3 50.7 – 14.9 6b 0.080c 7.0 ( - 1.2 to 15.3)PROMIS-PI 20.1 – 5.0 17.0 – 5.9 23 0.005a - 3.2 ( - 5.3 to - 1.1)Knee range of motion (degrees) 113.9 – 13.0 117.5 – 15.0 23 0.087 3.6 ( - 0.6 to 7.8)50-ft walk (sec) 13.5 – 2.2 12.8 – 2.4 23 0.121 - 0.7 ( - 1.7 to 0.2)
Values expressed with a plus/minus sign are the mean – standard deviation. Negative values for mean paired difference for PROMIS PainInterference and time to walk 50 feet indicate improvement on these measures.
aSignificant at p < 0.05.bStandard scoring of the SF-12 specifies that participants with any missing data be dropped from the analysis.cTrend in expected direction at p < 0.10.EQ-5D-5L, the EuroQol health status index; SF-21, 12-Item Short-Form Health Survey; MCS, Mental Composite Score; PCS, Physical
Composite Score; PROMIS-PI, Patient Reported Outcomes Measurement Information System-Pain Interference.
336 JUBERG ET AL.

pain and interference of pain on other aspects of one’s life.If results are confirmed in a larger randomized trial, massagecould be an important component of regular care for thesepatients.
Acknowledgments
Special thanks to Dr. Partap Khalsa and the NationalInstitutes of Health National Center for Complementary andAlternative Medicine for supporting this work via grant 3R01 AT004623-05S2. The authors are grateful to ProfessorCarl F. Pieper for providing his input on statistical analysis.
Author Disclosure Statement
No competing financial interests exist.
References
1. Lawrence RC, Felson DT, Helmick CG, et al. Estimates ofthe prevalence of arthritis and other rheumatic conditions inthe United States. Part II. Arthritis Rheum 2008;58:26–35.
2. Murphy L, Schwartz TA, Helmick CG, et al. Lifetime riskof symptomatic knee osteoarthritis. Arthritis Rheum 2008;59:1207–1213.
3. Cameron KL, Hsiao MS, Owens BD, et al. Incidence ofphysician-diagnosed osteoarthritis among active duty Uni-ted States military service members. Arthritis Rheum 2011;63:2974–2982.
4. Dominick KL, Golightly YM, Jackson GL. Arthritis prev-alence and symptoms among US non-veterans, veterans,and veterans receiving Department of Veterans AffairsHealthcare. J Rheumatol 2006;33:348–354.
5. David D, Woodward C, Esquenazi J, et al. Comparison ofcomorbid physical illnesses among veterans with PTSD andveterans with alcohol dependence. Psychiatr Serv 2004;55:82–85.
6. Hochberg MC, Altman RD, April KT, et al. AmericanCollege of Rheumatology 2012 recommendations for theuse of nonpharmacologic and pharmacologic therapies inosteoarthritis of the hand, hip, and knee. Arthritis Care Res(Hoboken) 2012;64:465–474.
7. Richmond J, Hunter D, Irrgang J, et al. Treatment of os-teoarthritis of the knee (nonarthroplasty). J Am Acad Or-thop Surg 2009;17:591–600.
8. Sherman KJ, Cook AJ, Wellman RD, et al. Five-weekoutcomes from a dosing trial of therapeutic massage forchronic neck pain. Ann Fam Med 2014;12:112–120.
9. Perlman AI, Sabina A, Williams AL, et al. Massage therapyfor osteoarthritis of the knee: a randomized controlled trial.Arch Intern Med 2006;166:2533–2538.
10. Perlman AI, Ali A, Njike VY, et al. Massage therapy forosteoarthritis of the knee: a randomized dose-finding trial.PLoS One 2012;7:e30248.
11. Bellamy N. The WOMAC Knee and Hip OsteoarthritisIndices: Development, validation, globalization and influ-ence on the development of the AUSCAN Hand Osteoar-thritis Indices. Clin Exp Rheumatol 2005;23:S148–153.
12. Broderick JE, Schneider S, Junghaenel DU, et al. Validityand reliability of patient-reported outcomes measurementinformation system instruments in osteoarthritis. ArthritisCare Res (Hoboken) 2013;65:1625–1633.
13. Fransen M, Edmonds J. Reliability and validity of theEuroQol in patients with osteoarthritis of the knee. Rheu-matology (Oxford) 1999;38:807–813.
14. Stewart AL, Ware JE Jr. Measuring Functioning and Well-Being: The Medical Outcomes Study Approach. Durham,NC: Duke University Press; 1992.
15. Gill S, McBurney H. Reliability of performance-basedmeasures in people awaiting joint replacement surgery ofthe hip or knee. Physiother Res Int 2008;13:141–152.
16. Fransen M, Crosbie J, Edmonds J. Reliability of gaitmeasurements in people with osteoarthritis of the knee.Phys Ther 1997;77:944–953.
17. Angst F, Aeschlimann A, Michel BA, et al. Minimal clinicallyimportant rehabilitation effects in patients with osteoarthritisof the lower extremities. J Rheumatol 2002;29:131–138.
18. Denneson LM, Corson K, Dobscha SK. Complementaryand alternative medicine use among veterans with chronicnoncancer pain. J Rehabil Res Dev 2011;48:1119–1128.
19. Fletcher CE, Mitchinson AR, Trumble EL, et al. Percep-tions of providers and administrators in the Veterans HealthAdministration regarding complementary and alternativemedicine. Med Care 2014;52:S91–96.
20. Collinge W, Kahn J, Soltysik R. Promoting reintegration ofNational Guard veterans and their partners using a self-directed program of integrative therapies: a pilot study. MilMed 2012;177:1477–1485.
21. Kozak L, Vig E, Simons C, et al. A feasibility study ofcaregiver-provided massage as supportive care for Veteranswith cancer. J Support Oncol 2013;11:133–143.
22. Atkins DV, Eichler DA. The effects of self-massage onosteoarthritis of the knee: a randomized, controlled trial. IntJ Ther Massage Bodywork 2013;6:4–14.
23. Plews-Ogan M, Owens JE, Goodman M, et al. A pilot studyevaluating mindfulness-based stress reduction and massagefor the management of chronic pain. J Gen Intern Med2005;20:1136–1138.
Address correspondence to:Kristin K. Jerger, MD, LMBT
Duke Integrative MedicineDuke University Medical Center
DUMC 102904Durham, NC 27710
E-mail: [email protected]
Adam I. Perlman, MD, MPHDuke Integrative Medicine
Duke University Medical CenterDUMC 102904
Durham, NC 27710
E-mail: [email protected]
(Appendix follows/)
MASSAGE FOR KNEE OA IN VA HEALTH CARE USERS 337

Appendix 1. Study Acceptability: Responses to Closed-Ended Post-Study Questions (n = 23)
Question No Yes % Yes
1. ‘‘Was the schedule of visits (60 minutes/week) convenient for you?’’ 1 22 962. ‘‘Would you like to continue massage as part
of the ongoing management of your knee arthritis?’’2 21 91
3. ‘‘Did you notice any other changes in your healthor other aspects of your life since starting the massage?’’
4 19 83
4. ‘‘If the VA were to offer massage for knee arthritis, howlikely do you think it is that other veterans you knowwould want to try this treatment?’’� Very likely 18 78� Somewhat likely 2 9� Not at all likely 0 0� Don’t know 3 13
VA, Department of Veterans Affairs.
338 JUBERG ET AL.

JOURNAL OF AMERICAN COLLEGE HEALTH, VOL. 62, NO. 4
Major Article
A Randomized Controlled Trial of Koru:A Mindfulness Program for College Students
and Other Emerging Adults
Jeffrey M. Greeson, PhD; Michael K. Juberg, BA; Margaret Maytan, MD;Kiera James; Holly Rogers, MD
Abstract. Objective: To evaluate the effectiveness of Koru, amindfulness training program for college students and other emerg-ing adults. Participants: Ninety students (66% female, 62% white,71% graduate students) participated between Fall 2012 and Spring2013. Methods: Randomized controlled trial. It was hypothesizedthat Koru, compared with a wait-list control group, would reduceperceived stress and sleep problems, and increase mindfulness,self-compassion, and gratitude. Results: As hypothesized, resultsshowed significant Group (Koru, Wait-List) × Time (Pre, Post) in-teractions for improvements in perceived stress (F[1, 76.40] = 4.50,p = .037, d = .45), sleep problems (F [1, 79.49] = 4.71, p = .033,d = .52), mindfulness (F [1, 79.09] = 26.80, p < .001, d = .95),and self-compassion (F[1, 74.77] = 18.08, p < .001, d = .75). Allsignificant effects were replicated in the wait-list group. Signifi-cant correlations were observed among changes in perceived stress,sleep problems, mindfulness, and self-compassion. Conclusions:Results support the effectiveness of the Koru program for emergingadults in the university setting.
Keywords: college health, emerging adulthood, meditation, mind-fulness, stress management
Dr Greeson and Mr Juberg are with Duke Integrative Medicineat Duke University Medical Center in Durham, North Carolina, andthe Department of Psychiatry and Behavioral Sciences at Duke Uni-versity School of Medicine in Durham, North Carolina. Dr Maytanis with the Department of Psychiatry and Behavioral Sciences atDuke University School of Medicine in Durham, North Carolina.Ms James is with Swarthmore College in Swarthmore, Pennsylva-nia. Dr Rogers is with the Department of Psychiatry and BehavioralSciences at Duke University School of Medicine in Durham, NorthCarolina, and Duke Counseling and Psychological Services at DukeUniversity in Durham, North Carolina.
Copyright © 2014 Taylor & Francis Group, LLC
A ccording to the 2012 National Survey of CollegeCounseling Centers, 92% of counseling centersare serving increasing numbers of students each
year, and 88% of directors report a continued trend towardsstudents presenting with increasing levels of psychopathol-ogy.1 Counseling centers are feeling this strain despite ev-idence that only a small percentage of struggling studentsseek treatment from university health centers.2,3 The levelof stress amongst students is alarming. About 50% of stu-dents report significant levels of anxiety and depression,2,4
and 16.5% report a history of suicidal or self-harm behavior.2
Moreover, sleep disturbance is prevalent in college studentsand has been proposed as a transdiagnostic risk factor forpoor mental health.5,6 The effects of mental health problemsfor students are not insignificant, as students with mentalhealth challenges have difficulties with campus engagement,personal relationships, and graduation rates.7 Because of themagnitude of the problem and the limitations on availableresources, those working in student health and wellness needcreative, developmentally targeted, evidenced-based strate-gies to effectively reduce stress and improve well-being instudent populations. Mindfulness-based interventions mayplay a role in filling this important need.
Mindfulness, the skill of learning to pay attention, with-out judgment, to one’s present-moment experience, offers away to improve well-being in diverse populations.8 Mindful-ness meditation training has been shown to reduce stress andimprove mood and academic performance in both collegeand graduate students.9–12 In the United States, mindfulness-based stress reduction (MBSR) and variants of MBSR arethe most commonly used methods of teaching mindful-ness meditation to adults. MBSR was developed by JonKabat-Zinn13 and is effective for improving psychological
222
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

A Randomized Controlled Trial of Koru
health, with meta-analyses documenting medium-to-large ef-fect sizes.14,15 Although there has been work on developingprograms specifically for children and teens,16 there has beenlittle discussion about targeting mindfulness training specif-ically towards other critical developmental stages, such asemerging adulthood.
Emerging adulthood is the developmental stage from thelate teens through the 20s, which includes most college stu-dents.17 In 2011, 68.2% of graduating high school studentsenrolled in postsecondary education, and in the fall of 2011there were nearly 21 million students enrolled in either 2-or 4-year degree-granting institutions.18 College-attendingand non–college-attending emerging adults (EAs) have sim-ilar developmental characteristics,19 and the overall rate ofpsychiatric disorders is roughly equivalent between college-attending individuals and their non–college-attending peers.4
Because the primary emphasis in emerging adulthood is onidentity exploration, this life stage is associated with frequentchanges and uncertainty in all life spheres.19
Mindfulness meditation offers a promising tool for man-aging the stress that may be associated with the challengesof emerging adulthood. However, there are no objective dataabout what pedagogical methods may be effective for train-ing EAs in mindfulness. Due to their unique developmentalstage, EAs may not engage readily in training programs thatare designed for older adults due to time constraints, skepti-cism about the potential benefits, and difficulty maintainingmotivation to effect behavior change.20 To address this dis-parity, Rogers and Maytan21 have developed Koru, a manual-ized training program in mindfulness, meditation, and othermind-body skills, that specifically targets EAs.
Koru is the New Zealand Maori word for the unfurling fernfrond, which symbolizes balanced growth. Koru differs frommindfulness programs developed for more general popula-tions of adults in several key ways. First, the program trainsEAs in certain mind-body skills, such as abdominal breathingand guided imagery, as well as insight meditation practice.These mind–body skills, for which studies show a positiveeffect on stress and anxiety,22,23 give participants tools forquickly reducing distress, which in turn builds their motiva-tion to continue practicing stress management and self-carein daily life. Second, Koru is relatively brief, with only four75-minute sessions and 10 minutes of required daily medita-tion practice. The course is highly structured and attendanceat all 4 classes is required. Third, the program is taught ina small-group format to capitalize on peer interactions thatEAs value. Fourth, the teaching is very active, addressingskepticism and building motivation quickly. Finally, the lan-guage and metaphors used are designed to resonate withthe interests and concerns of EAs. In addition to teachingmindfulness skills to cope with stress, Koru also empha-sizes cultivating positive emotions such as self-compassionand gratitude. Both compassion and gratitude are consideredcore qualities of mindfulness,24 and have been associatedwith lower levels of stress and psychological symptoms andgreater well-being in prior studies.25,26 Koru has been verypopular with students and those who have participated report
positive outcomes on course evaluations.20,21 However, untilnow, Koru has not been subjected to rigorous quantitativeevaluation.
The present randomized controlled trial (RCT), therefore,aimed to evaluate the effectiveness of Koru for EAs in auniversity setting. We hypothesized that college and graduatestudents who participate in Koru, when compared with acontrol group, would show reduced stress, improved sleep,and increased mindfulness, self-compassion, and gratitude.
METHODS
Study DesignThe RCT had 2 study arms: (1) Koru, the active interven-
tion, and (2) a wait-list control. We chose to use a wait-listcontrol condition to control for the effects of time, becauselevels of stress, sleep problems, and even self-concept canchange during an academic semester. Students who wererandomly assigned to the wait-list control group were of-fered an opportunity to participate in Koru later the samesemester. We felt that this design struck a balance betweenscientific rigor, by benefitting from an experimental designwith random assignment to groups, with the use of a cultur-ally normal wait-list process for the Koru program, whichshould optimize motivation and retention.
Following online informed consent, study participantscompleted standardized self-report questionnaires via a sur-vey Web site within 1 week before and after participatingin the 4-week Koru program. The study protocol was con-ducted between Fall 2012 and Spring 2013. Full approvalby the university’s Institutional Review Board was obtainedprior to data collection.
Students were eligible for the study if they were (a) cur-rently enrolled as an undergraduate, graduate or professionalstudent; (b) at least 18 years of age; (c) proficient in En-glish; (d) able to use a computer with internet access; and(e) willing to be randomized to either the Koru group orthe wait-list control group. Blocked randomization (blocksize = 2) was used to ensure balanced study groups afterevery 2 students enrolled. The randomization schedule wascreated using Research Randomizer (www.randomizer.org)and was performed by the study coordinator who kept groupassignments blinded from other study staff who performedstatistical analyses. Following randomization, the study co-ordinator contacted students to inform them of their group as-signment. Subsequently, the Koru instructors contacted stu-dents enrolled in Koru with an introductory e-mail and arequest to begin reading the required text, Wherever You Go,There You Are by Jon Kabat-Zinn. To protect against socialdesirability bias and potential evaluation bias, Koru courseinstructors were not directly involved in subject recruitment,consent, randomization, or data collection procedures.
Power analyses (G∗Power version 3.1.5; Kiel, Germany)based on a difference between 2 independent means (2groups) at a significance level of .05, a desired power of.80, and a medium-to-large effect size (ie, Cohen’s d = .6)based on prior meta-analyses, indicated that 45 students per
VOL 62, MAY/JUNE 2014 223
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

Greeson et al
group would be required to detect a significant difference forthe Koru versus wait-list control group.27
ParticipantsParticipants were 90 undergraduate, graduate, and profes-
sional students (Mage = 25.4, SD = 5.7; range = 18–59).Two graduate students, one who was 59 years old and an-other who was 42, provided baseline survey data but droppedout before attending the Koru group to which they were ran-domly assigned. The oldest student who provided completepre- and postsurvey data was 31 years old. Seventy-four stu-dents provided data on the post-Koru survey, a response rateof 82%.
As shown in Table 1, the sample comprised mostly women(66%) who were predominantly white (62%) and non-Hispanic (85%). Half of students reported having no reli-gious affiliation or being atheist. Nearly three-quarters werein graduate or professional school. The 2 randomized studygroups did not differ on any demographic characteristics,except average hours of sleep per night. The Koru group re-ported sleeping half an hour less per night, which was statis-tically significant but still within the normal range of healthysleep. We defined program completion as attending at least 3of the 4 Koru classes. There were no significant differences atbaseline between students who completed Koru versus thosewho did not. The only outcome variable that differed sig-nificantly was the Isolation subscale of the Self-compassionScale; the group of students that completed the Koru programreported a mean decrease in their sense of isolation, whereasthe group that attended 2 or less Koru classes reported a meanincrease in their sense of isolation post intervention.
ProcedureThe secure, online survey was administered using Qual-
itrics software (Provo, Utah) and included basic demographicinformation and a battery of standardized self-report ques-tionnaires. The questionnaires assessed symptoms of stress,sleep problems, mindfulness of thoughts and feelings, self-compassion, and gratitude. Participants were not offered fi-nancial compensation for completing the surveys.
InterventionAs detailed in a recently published treatment manual,21 the
Koru program is offered at a large university through Coun-seling and Psychological Services and consists of 4 required75-minute classes. The classes include 12 to 14 studentstaught by 1 or 2 teachers. Students typically participate inKoru because they are seeking training in mindfulness andmeditation to help reduce stress and enhance psychologicalwell-being. The Koru program is free of charge, voluntary,not graded, and students do not receive course credit for par-ticipating. In addition to attending all 4 weekly small-groupsessions, the Koru program requires a commitment to prac-ticing meditation for at least 10 minutes daily, completingand returning a daily meditation log, as well as reading therequired chapters in the course book, Wherever You Go, There
You Are. The meditation log includes space for daily docu-mentation of 2 things for which the student feels grateful.During each class, students learn and practice mindfulnessmeditation and 1 or 2 mind–body skills, including breathingexercises, walking meditation, guided imagery, and eatingmeditation.
Measures
Perceived Stress Scale (PSS)The 10-item Perceived Stress Scale (PSS) measures per-
ceived stress over the past month, defined by the degreeto which one feels like life has been unpredictable, uncon-trollable, or overwhelming. The PSS scores have demon-strated reliability and construct validity in student samplesand EAs.28 Cronbach’s α was .83 for PSS scores at both timepoints.29
Medical Outcome Study Sleep Scale (MOS SLP9)The sleep scale is one subscale of the Medical Outcomes
Study (MOS) health status measure.30 It consists of 12 itemsto measure 6 sleep dimensions: initiation (time to fall asleep),quantity (hours of sleep each night), maintenance, respira-tory problems, perceived adequacy of sleep, and somnolence(daytime sleepiness). The time frame for the responses is“the past 4 weeks.” The 9-item summary scale (Sleep Prob-lems Index II) was used for analysis.30 Higher scores indicategreater sleep problems. Cronbach’s α was .88 for sleep qual-ity scores at both time points.29
Cognitive and Affective Mindfulness Scale–Revised(CAMS-R)
The 12-item Cognitive and Affective MindfulnessScale–Revised (CAMS-R) was used to measure 4 aspectsof trait mindfulness, including attention, awareness, accep-tance, and present-focus. Previous psychometric evaluationof the CAMS-R found scores to be reliable and valid,31 anda recent outcome study found that the CAMS-R was sensi-tive to change following MBSR training.32 Cronbach’s α forCAMS-R scores was .88 at baseline and .80 post interven-tion.29
Self-compassion Scale (SCS)The 26-item Self-compassion Scale (SCS)33 was used to
assess participants’ tendency to treat themselves with kind-ness and understanding rather than harsh judgment and criti-cism during difficult times, to perceive difficult experience aspart of common humanity, and to consider difficult thoughtsand experiences as separate from the core self. The SCS has6 subscales (Self-judgment, Self-kindness, Isolation, Com-mon Humanity, Mindfulness, Over-identification) that canbe summed to attain a total score. SCS scores have beenshown to be reliable and valid in previous studies of col-lege students.33 The SCS was also sensitive to change with amindful self-compassion (MSC) training program.34 Higherscores on all scales indicate higher levels of self-compassion.
224 JOURNAL OF AMERICAN COLLEGE HEALTH
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

A Randomized Controlled Trial of Koru
TABLE 1. Baseline Characteristics of Study Participants
Characteristic Koru group (n = 45) Wait-list group (n = 45) Difference statistic
Age t(84) = 0.81, p = .423M years 25.75 24.76SD 6.84 4.15
Gender χ 2(1) = 0.05, p = .842Male 15 16Female 30 29
Ethnicity See noteHispanic 4 1Non-Hispanic 38 38Prefer not to answer 3 5
Race χ 2(1) = 0.79, p = .375White 30 26African American 3 2Asian American 10 13Other 1 3Prefer not to answer 1 1
Religion χ 2(2) = 2.14, p = .343No religious affiliation 14 19Atheist 5 7Buddhist 1 0Christian 13 7Jewish 1 2Hindu 2 1Muslim 0 2Unitarian/Universalist 1 1Other 2 1Prefer not to Answer 6 5
Education χ 2(2) = 0.32, p = .852Undergraduate 1st yr 0 3Undergraduate 2nd yr 6 2Undergraduate 3rd yr 4 3Undergraduate 4th yr 2 5Undergraduate 5th yr 0 1Graduate student 20 20Professional Student 13 11
Sleep t(88) = 2.26, p = .027M hours per night 7.56 8.09SD 1.09 1.16
Sleep medication χ 2(1) = 0.34, p = .561n yes 8 6% 18% 13%
Note. Chi-square could not be computed for ethnicity due to less than 5 Hispanic students per group. Other demographic categories with less than5 students each were collapsed as follows. Race: white, racial minority. Religion: no religious affiliation, atheist, religious affiliation. Education:undergraduate, graduate, professional student.
Cronbach’s α for SCS total scores was .94 at baseline and.95 post intervention.29
Gratitude Questionnaire (GQ-6)Dispositional gratitude was measured using the GQ-6,35
which has demonstrated good convergent validity with rele-vant constructs such as positive affect and prosocial traits.36
Cronbach’s α for GQ-6 scores was .88 both pre and postintervention.29
Other MeasuresDemographic characteristics were assessed at the end of
the online survey, and are reported in Table 1.
Data AnalysisAll statistics were performed using IBM SPSS version 20
(Armonk, New York). Variables were screened for distribu-tional assumptions prior to analysis. All continuous outcomevariables approximated a normal distribution with skewnessand kurtosis less than 2.0. Primary analyses of between-group effects were tested using linear mixed-effects models,which provide several statistical advantages over traditionalrepeated-measures analysis of variance (ANOVA).37 Groupassignment was treated as a fixed effect and outcome vari-ables were treated as random effects that could vary within-person and across time. This analytic strategy, based on
VOL 62, MAY/JUNE 2014 225
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

Greeson et al
restricted maximum likelihood estimation, allowed all sub-jects to be included in the models, even those with missingdata. Therefore, mixed-effects models were consistent withintent-to-treat principles without requiring imputation, suchas last observation carried forward, which can bias parame-ter estimates. Mixed-effects modeling also provided the ad-vantage of accounting for dependence of observations in arepeated-measures design, a phenomenon that frequently vi-olates an assumption of traditional ANOVA using the generallinear model.
The primary hypothesis of a significant difference betweengroups over time was tested using a Group × Time interactioneffect, which indicated the effectiveness of Koru comparedwith a wait-list control. Within the same model runs, t testswere used to test hypotheses about planned contrasts betweenpre- and postintervention scores within the Koru and controlgroups, and to test for differences between-groups at base-line and at the postintervention time point. Effect sizes forbetween-group differences over time were calculated usingCohen’s d and η2.38 Secondary analyses included within-group mixed-effects models to replicate the effects of Koruamong wait-listed students who took the program later inthe same semester. Secondary analyses also included corre-lations among changes in outcomes measures as a functionof randomized group assignment. Consistent with recom-mendations for clinical trials, statistical significance for allparameter estimates was set at z = 1.96, α = .05, 2-tailed.39
RESULTS
Baseline Characteristics and Preliminary AnalysesBaseline levels of perceived stress fell more than 1 stan-
dard deviation above the norm for adults between ages 18and 34 and for adults with an advanced degree.28 Baselinesleep problems fell nearly 1 standard deviation above thegeneral population norm.30 Mindfulness scores fell approx-imately 1 standard deviation below a published norm forcollege students,31 and was comparable to a sample of adultswho participated in an 8-week, self-pay MBSR program.32
Self-compassion fell nearly 1 standard deviation below thecollege student norm33 and the mean gratitude score wascomparable to the mean reported by scale developers forcollege students.35 t tests revealed no significant differencesbetween groups on primary outcome variables at baseline,except gratitude, which was significantly higher in the Korugroup (see Table 2). One subscale of the SCS (Common Hu-manity) was higher in the Koru group at baseline. Data wererelatively normally distributed with all z scores for skewnessand kurtosis less than 2.0.
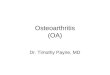
Figure 1 provides a flow diagram for recruitment and re-tention throughout the trial. Overall, 90% of students whoenrolled in the study completed the baseline survey andwere randomized. Over 82% of randomized students wereretained. Of the 45 students initially randomized to Koru,33% attended all 4 classes, 38% attended 3 or more classes,18% attended 2 classes, and 4% attended only 1 class. Seven
percent (n = 3) did not attend any Koru classes after theywere initially assigned to the group. Of the 45 students whoparticipated in Koru after being randomized to the wait-listgroup, 33% attended all 4 classes, 27% attended 3 or moreclasses, 11% attended 2 classes, and 2% attended only 1 class.Twenty-seven percent of students (n = 12) initially assignedto the wait-list did not attend any Koru classes when theywere offered the opportunity later in the semester. Consistentwith intent-to-treat, all students who were randomized wereanalyzed. No adverse events were reported by any participantduring the study.
Primary AnalysesAs hypothesized, there was a significant Group × Time
interaction for change in perceived stress scores (see Table 2).Whereas perceived stress scores for the control group didnot change over time (t = 0.71, p = .48), perceived stressdecreased significantly in the Koru group (t = 3.62, p =.001). A medium effect size on perceived stress was observedfor Koru compared with the wait-list control (Table 2), asevidenced by a half standard deviation larger reduction inperceived stress scores (d = .45), with 5% of the variance inperceived stress scores over time explained as a function ofgroup assignment (η2 = .048).
There was also a significant Group × Time interaction forchange in sleep problems (see Table 2). Whereas sleep qualityscores for the control group did not change over time (t =0.03, p = .98), overall sleep quality improved significantlyin the Koru group (t = 3.04, p = .003). A medium effect sizeon sleep problems was observed for Koru compared with thewait list control (Table 2), as evidenced by a half–standarddeviation larger reduction in sleep quality scores (d = .52),with 6% of the variance in sleep quality scores over timeexplained as a function of group assignment (η2 = .063).
A significant Group × Time interaction was observed forchange in mindfulness scores (see Table 2). Whereas mind-fulness scores for the control group did not change over time(t = 0.59, p = .56), mindfulness increased significantly inthe Koru group (t = −6.60, p < .001). A large effect sizeon mindfulness of thoughts and feelings was observed forKoru compared with the wait-list control (Table 2), as evi-denced by a 1 standard deviation larger increase in CAMS-Rmindfulness scores (d = −.95), with 18% of the variancein mindfulness scores over time explained as a function ofgroup assignment (η2 = .184).
A significant Group × Time interaction was also observedfor change in self-compassion scores (see Table 2). Whereasself-compassion total scores for the control group did notchange over time (t = −0.20, p = .84), they improved sig-nificantly in the Koru group (t = −6.38, p < .001). A largeeffect size on total self-compassion scores was observed forKoru compared with the wait-list control (Table 2), as evi-denced by a three-quarter standard deviation larger increasein total self-compassion scores (d = −.75), with 12% of thevariance in total self-compassion scores over time explainedas a function of group assignment (η2 = .123).
226 JOURNAL OF AMERICAN COLLEGE HEALTH
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

A Randomized Controlled Trial of Koru
TAB
LE
2.C
han
ges
inO
utc
om
eV
aria
ble
sfo
rK
oru
and
Wai
t-L
ist
Co
ntr
olG
rou
ps
Kor
ugr
oup
Wai
t-lis
tcon
trol
Mix
ed-m
odel
AN
OV
APr
ePo
stPr
ePo
st(G
roup
×T
ime)
Out
com
eM
SDM
SDM
SDM
SDF
pd
η2
Perc
eive
dst
ress
23.7
15.
6520
.43∗
6.20
25.6
65.
6525
.04
5.96
76.4
0.0
4.4
5.0
48Sl
eep
prob
lem
s41
.36
16.2
132
.52∗
18.0
642
.91
16.2
142
.84
17.2
379
.49
.03
.52
.063
Min
dful
ness
28.6
95.
6333
.77∗
6.06
27.2
25.
6326
.79
5.87
79.0
9.0
0−.
95.1
84Se
lf-c
ompa
ssio
n(t
otal
)2.
730.
663.
25∗
0.70
2.61
0.66
2.62
0.68
20.0
7.0
0−.
75.1
23Se
lf-k
indn
ess
2.64
0.77
3.20
∗0.
842.
470.
772.
550.
809.
20.0
0−.
06.0
83C
omm
onH
uman
ity2.
790.
843.
14∗
0.90
2.41
0.84
2.65
†0.
870.
51.4
8−.
13.0
04M
indf
ulne
ss3.
070.
763.
46∗
0.82
2.86
0.76
2.85
0.80
8.03
.01
−.51
.061
Self
-jud
gmen
t2.
670.
793.
28∗
0.87
2.74
0.79
2.64
0.83
15.3
9.0
0−.
86.1
56Is
olat
ion
2.54
0.88
3.16
∗0.
952.
550.
882.
460.
9117
.56
.00
−.79
.135
Ove
r-id
entifi
catio
n2.
680.
853.
30∗
0.91
2.61
0.85
2.60
0.88
16.8
1.0
0−.
72.1
15G
ratit
ude
35.9
36.
9636
.32
7.51
32.5
86.
9632
.31
7.26
0.24
.62
−.09
.002
Not
e.Pr
ean
dpo
stsc
ores
from
mix
ed-e
ffec
tsm
odel
sar
esh
own
ases
timat
edm
argi
nal
mea
ns(S
D).
Stat
istic
sar
esh
own
for
Gro
up×
Tim
eef
fect
,w
hich
test
edfo
rth
eef
fect
iven
ess
ofK
oru
over
time
com
pare
dw
ithth
ew
ait-
listc
ontr
ol.C
ohen
’sd
=di
ffer
ence
betw
een
pre-
post
chan
gein
Kor
uan
dpr
e-po
stch
ange
inw
ait-
listd
ivid
edby
pool
edSD
.Ran
ge:.
20=
smal
l,.5
0=
med
ium
,.80
=la
rge.
38η
2
rang
efo
rpe
rcen
tvar
ianc
eex
plai
ned
inou
tcom
edu
eto
grou
pas
sign
men
t:.0
1=
smal
l,.0
6=
med
ium
,.14
=la
rge.
38H
ighe
rsc
ores
for
alls
elf-
com
pass
ion
scal
esin
dica
tehi
gher
leve
lsof
self
-com
pass
ion.
∗ p<
.005
;†p
<.0
5fo
rw
ithin
-gro
upch
ange
sby
pair
edtt
est(
see
text
).
VOL 62, MAY/JUNE 2014 227
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

Greeson et al
Assessed for Eligibility/Enrolled(n = 101)
Excluded (n = 11) Lost to Follow-Up (n = 11) Not meeting inclusion criteria (n = 0) Declined to participate (n = 0)
Analyzed (n = 45)
Lost to Follow-Up (n = 0) Discontinued Intervention due to
Scheduling Conflicts (n = 6)
Assigned to Koru Group (n = 45) Received allocated intervention
(n = 42) Did not receive allocated intervention (n = 3)
Lost to Follow-Up (n = 7) Discontinued Intervention due to
Scheduling conflicts (n = 7) Missed Survey Deadline (n = 1)
Assigned to Wait-List Control (n = 45) Received allocated intervention later
(n = 33) Did not receive allocated intervention
(n = 12)
Analyzed (n = 45)
Allocation
Analysis
Follow-Up
Randomized (n = 90)
Enrollment
FIGURE 1. CONSORT flowchart of participants retained at each phase of the trial (color figure available online).
To examine the sources of change in overall levelsof self-compassion, we ran separate mixed-effects modelson each of the self-compassion subscales (see Table 2).Whereas the wait-list control group only reported a sig-nificant pre–post change on 1 subscale, Common Human-ity, the Koru group reported significant pre–post changeson all 6 subscales: increased Self-kindness, Common Hu-manity, and Mindfulness, and decreased Self-judgment, Iso-lation, and Over-identification (see Table 2). Effect sizes
for SCS subscales fell in the medium range for Self-kindness and Mindfulness, and in the large range for Self-judgment, Isolation, and Over-identification. The CommonHumanity subscale, which improved significantly for bothgroups, showed a small effect size in favor of Koru (seeTable 2).
The Group × Time interaction for change in gratitudewas not statistically significant. Neither group reported asignificant pre–post change in gratitude (see Table 2).
228 JOURNAL OF AMERICAN COLLEGE HEALTH
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

A Randomized Controlled Trial of Koru
Secondary AnalysesMixed-effects models on students originally assigned to
the wait list (n = 45) who took Koru later in the semesterreplicated all significant effects observed among studentswho were randomized to take Koru first. Within-subjectsanalyses modeled change over 3 time points: baseline, postwait-list, and post Koru. Significant effects of time (all p val-ues < .005) were accounted for by significant changes fromtime 2 to time 3 for the following variables: PSS (t = 3.56,p = .001), sleep problems (t = 12.75, p < .001), mindful-ness (t = 5.08, p < .001), self-compassion total (t = 6.24, p< .001), self-judgment (t = 4.37, p < .001), isolation (t =4.70, p < .001), over-identification (t = 4.10, p < .001), self-kindness (t = 3.68, p < .001), and mindfulness (t = 4.14, p< .001). Consistent with students randomized to take Korufirst, students randomized to take Koru later in the semesterhad large effects sizes (within-subjects Cohen’s d = t/
√n) for
changes in mindfulness (d = .76) and total self-compassionscores (d = .93), and medium effect sizes for perceived stress(d = .53) and most self-compassion subscales (d = .55–.70).The effect size for improvement in sleep problems was sub-stantially larger (d = 1.90), and the effect on an increasedsense of common humanity was marginally significant (t =1.96, p = .054) with a small effect size (d = .29).
As expected, numerous significant correlations were ob-served between changes in perceived stress, sleep problems,mindfulness, and self-compassion among students originallyrandomized to Koru (see Table 3). Notably, changes in mind-fulness, self-compassion total scores, self-judgment, andover-identification were significantly correlated with all otheroutcome variables (except gratitude) in the Koru group. Incontrast, compared with students randomly assigned to Koru,students assigned to the wait-list group reported fewer thanhalf as many significant correlations (see Table 3). Thesefindings are consistent with the hypothesis that improvementsin stress, sleep, mindfulness, and compassion are interrelatedduring Koru.
COMMENTEmerging adulthood, the transitional stage between high
school and adulthood, has been defined as a distinct de-velopmental stage with unique needs and challenges.17,19
This age group struggles with concerning levels of stress-related psychological conditions, including anxiety,40 depres-sion,2 and sleep disturbance.5 Mindfulness-based interven-tions have proved effective for reducing stress in universitystudents.41 The main results from this RCT found that Koru,a new mindfulness training program designed specifically forEAs, produced significant improvements in perceived stress,sleep quality, mindfulness, and self-compassion in a univer-sity student cohort of EAs. Gratitude was not measurablyaffected. Koru was well liked by students as reflected byhigh enrollment and retention in the study.
The results of this trial replicate and extend previous stud-ies of meditation and mindfulness training for university stu-dents. For example, the significant effect on lowering per-
ceived stress was similar in magnitude to a published RCT oncollege students that compared the effect of 2 meditation pro-grams with a wait-list control group.9 Lower perceived stressfollowing participation in Koru is also consistent with anotherwait-list controlled trial with medical students.10 Other RCTsthat found significant reductions in perceived stress and psy-chological distress included a 6-week mind–body programbased on the relaxation response and cognitive-behavioraltherapy skills42 and a 3-arm trial that compared 5 sessions ofmindfulness meditation training, somatic relaxation training,and a wait-list control.43 Thus, the significant stress reducingeffect of Koru in this study was comparable to other, oftenlonger, stress management and skill building programs forstudents.
Koru also produced a significant decrease in sleep prob-lems, an effect that has previously been limited to uncon-trolled studies.44 Whereas RCTs of MBSR and mindfulness-based cognitive therapy (MBCT) have recently documentedimprovements in objective measures of sleep quality amongadult populations with insomnia45 and depression,46 thepresent study adds to the literature by demonstrating thatimprovement in subjective sleep quality among universitystudents is directly correlated with increased levels of mind-fulness and self-compassion.
Consistent with a recent meta-analysis of over 12,000participants in mindfulness-based therapies, Koru producedclinically significant effect sizes on multiple measures of psy-chological well-being.14 The largest effect sizes in this studywere seen for increases in mindfulness and self-compassion.The increase in mindfulness with Koru was comparable toincreases in mindfulness seen with an 8-week MBSR pro-gram,32 an 8-week MBCT program,47 and an 8-week MSCprogram.34 Although Koru’s relatively large effect size forself-compassion (d = .75) was substantially less than that forMSC (d = 1.67), it had somewhat stronger effects on mind-fulness and stress. This difference may reflect that Koru doesnot specifically target self-compassion, but rather mindfulattention, awareness, relaxation, and self-regulation. Nev-ertheless, changes in self-compassion in this study werecomparable to those seen in other primary mindfulness in-terventions such as MBSR.48 Given the association betweenhigher levels of self-compassion and better psychologicalwell-being,25,34 this study suggests that Koru may promotestudent health, in part, by helping EAs develop a health-ier way of relating to themselves in difficult times—a waymarked by greater self-kindness and less self-judgment; agreater sense of connection through common humanity andless isolation; and better emotional balance through greatermindfulness and less over-identification with one’s problems.
Secondary findings demonstrated that all of the signif-icant effects observed in a group of students randomizedto receive Koru could be replicated in wait-listed studentslater in the same semester. Moreover, correlations amongimprovements in perceived stress, sleep problems, mindful-ness, and self-compassion were predominantly significantin the Koru group. This finding indicates that Koru-relatedbenefits in mental and behavioral health are interdependent.
VOL 62, MAY/JUNE 2014 229
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

Greeson et al
TAB
LE
3.C
orr
elat
ion
sA
mo
ng
Stu
dy
Var
iab
les
for
Ko
ruG
rou
p(n
=35
)B
elo
wD
iag
on
alan
dW
ait-
Lis
tC
on
tro
l(n
=39
)A
bov
eD
iag
on
al
12
34
56
78
910
11
1.Pe
rcei
ved
stre
ss(P
SS)
—.3
22∗
−.14
2.1
99−.
094
.161
.241
−.27
5†−.
267
−.24
3−.
164
2.Sl
eep
prob
lem
s(M
OS)
.313
†—
.059
−.25
0−.
238
−.02
1−.
019
−.13
8.0
13−.
334∗
.100
3.M
indf
ulne
ss(C
AM
S)−.
611∗∗
∗−.
450∗∗
—.4
96∗∗
.454
∗∗.1
23.3
61∗
.187
.098
.315
†.0
574.
Self
-com
pass
ion
(tot
al)
−.45
9∗∗−.
405∗
.711
∗∗—
.661
∗∗.0
60.5
65∗∗
.731
∗∗.4
26∗∗
.536
∗∗.2
395.
Self
-kin
dnes
s(S
CS)
−.32
2†−.
335∗
.613
∗∗.8
21∗∗
—.0
39.5
37∗∗
.253
−.09
6.2
07−.
070
6.C
omm
onH
uman
ity(S
CS)
−.24
3−.
309†
.523
∗∗.6
28∗∗
.416
∗—
.191
−.35
4∗−.
145
−.19
2−.
277†
7.M
indf
ulne
ss(S
CS)
−.25
5−.
262
.594
∗∗.7
99∗∗
.657
∗∗.5
53∗∗
—.1
45−.
052
.024
−.02
58.
Self
-jud
gmen
t(SC
S)−.
486∗∗
−.33
4∗.5
82∗∗
.881
∗∗.6
42∗∗
.487
∗∗.5
68∗∗
—.4
56∗∗
.459
∗∗.4
17∗∗
9.Is
olat
ion
(SC
S)−.
388∗
−.19
6.4
62∗∗
.642
∗∗.3
96∗
.077
.400
∗.5
63∗∗
—.0
48.2
6610
.Ove
r-id
entifi
catio
n(S
CS)
−.37
8∗−.
444∗∗
.505
∗∗.8
25∗∗
.624
∗.4
27∗
.593
∗∗.6
91∗∗
.508
∗∗—
.293
†
11.G
ratit
ude
(GQ
-6)
−.20
3−.
286†
.276
.241
.143
.329
†.1
18.2
22.1
74.1
17—
Not
e.PS
S=
Perc
eive
dSt
ress
Scal
e;M
OS
=M
edic
alO
utco
mes
Stud
y;C
AM
S=
Cog
nitiv
ean
dA
ffec
tive
Min
dful
ness
Scal
e;SC
S=
Self
-com
pass
ion
Scal
e;G
Q-6
=G
ratit
ude
Que
stio
nnai
re.
† p<
.10;
∗ p<
.05;
∗∗p
<.0
1;∗∗
∗ p<
.001
.
230 JOURNAL OF AMERICAN COLLEGE HEALTH
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

A Randomized Controlled Trial of Koru
Taken together, the significant changes in perceived stress,sleep, mindfulness and self-compassion with Koru suggestthat tailoring mindfulness training to emerging adulthood byincorporating other mind–body skills, using fewer class ses-sions, requiring shorter but mandatory home practice as wellas a course text, and contextualizing mindfulness training toreflect common interests and concerns of EAs is an effectivestrategy.
The relative brevity of the training model may contributeto the high retention rates and thus effectiveness of Koru. Stu-dents identify time pressures as one of the primary reasonsfor not seeking help for mental health concerns.3 Thus, Koruwas designed to be as efficient as possible. Koru involves5 hours of class time over 4 weeks, plus the expectation of10 minutes of practice/day. In comparison, MBSR involves27 hours of class time over 8 weeks, plus the expectation of45 minutes/day of meditation practice.49 The decreased timerequirement of Koru appears to work well for young adultswho are juggling competing pressures. The present studydemonstrates that significant results can be achieved within arelatively short, 4-week time frame. Others have found bene-fits with brief exposure to mindfulness training. For example,one 5-session training model that included a daylong med-itation retreat found significant decreases in psychologicaldistress and rumination, and significant increases in positivemood, among undergraduate and graduate students reportingdistress.43 Another recent study found reductions in anxietyand associated neural correlates with only 4 20-minute mind-fulness trainings.50 The relatively high retention rate of 82%in our study may reflect the appeal of Koru for EAs.
Strengths and LimitationsThe strengths of the study included a randomized experi-
mental design, adequate statistical power provided by a rela-tively large sample size, inclusion of all available data fromall randomized subjects, and relatively high levels of programadherence and survey completion. Limitations included re-liance on self-report surveys for primary outcome measures,which are susceptible to recall bias; limited diversity in thestudent sample, which precludes broader generalizability;and use of pre- and postintervention measures, which lim-its understanding of when beneficial effects started to occurand how long beneficial effects might last after Koru train-ing. Future research can build on the present study by usingan objective measure of mindfulness, such as monitoringbreaths or heart beat while practicing meditation,51 enrollinga more diverse group of students, and including both interimand follow-up assessments to better describe the process anddurability of change following Koru.
ConclusionCollege students make up a substantial fraction of the
EA demographic.18 A large proportion of college studentsreport significant stress-related mental health concerns, in-cluding anxiety and depression.41 These types of mentalhealth concerns impact students both interpersonally and
academically.7 Mindfulness-based interventions are knownto provide significant improvement in anxiety, depression,and stress reactivity in adults and university student popu-lations.41,52 Only a small percentage of struggling studentsreceive treatment from university health centers2,3; therefore,it is critical that a broader range of mental-health outreachservices be provided for students. The results of this studyshow that Koru, a relatively brief, developmentally targetedmindfulness program, was effective at reducing symptoms ofstress, enhancing psychological well-being, and promotingsleep—a key health behavior—for EAs who are students in auniversity setting. These findings support Koru as a viable in-tervention for student counseling centers and other agenciesthat seek to provide cost-effective, low-stigma interventionsfor students suffering from unmanageable levels of stress.Further research is needed to explore the effectiveness ofKoru in other EA populations in community colleges, his-torically black colleges and universities, and nonacademicsettings.
ACKNOWLEDGMENTSWe thank the staff at Duke Counseling and Psychological
Services, including the director of outreach services GaryGlass, PhD, and the administrative assistant for outreach ser-vices, Mary Cicinnati. We also thank all of the undergraduate,graduate, and professional students who volunteered theirvaluable time to participate in the trial and complete our sur-vey. Finally, we thank Karen Caldwell, PhD, for assistancewith SPSS code for the mixed-effects models, and DennisCarmody, BA, for technical assistance with randomizationprocedures and database management.
FUNDINGThis work was supported by grant R00 AT004945 from
the National Center for Complementary and AlternativeMedicine (NCCAM) to JMG. The contents of this articleare solely the responsibility of the authors and do not neces-sarily represent the official views of the National Institutesof Health (NIH).
CONFLICT OF INTEREST DISCLOSUREAfter completing the current research study, Dr Rogers
co-founded the Koru Center for Mindfulness, of which shehas an ownership share; if Koru is found to be an effectiveintervention, she could benefit financially. Dr Maytan hasreceived compensation for teaching from the Koru Centerfor Mindfulness. Dr Greeson, Mr Juberg, and Ms James,who were responsible for collecting and analyzing the datafor this study, report no financial relationship relevant to thesubject of this article. The authors confirm that the researchpresented in this article met the ethical guidelines, includingadherence to the legal requirements, of the United States andreceived approval from the Institutional Review Board ofDuke University.
VOL 62, MAY/JUNE 2014 231
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

Greeson et al
NOTEFor comments and further information, address corre-
spondence to Jeffrey M. Greeson, PhD, Duke Integra-tive Medicine, Duke University Medical Center, DUMCBox 102904, Durham, NC 27710, USA (e-mail: [email protected]; [email protected]).
REFERENCES1. Gallagher RP. National Survey of Counseling Center Di-
rectors. Alexandria, VA: International Association of CounselingServices; 2004.
2. Garlow SJ, Rosenberg J, Moore JD, et al. Depression, des-peration, and suicidal ideation in college students: results fromthe American foundation for suicide prevention college screeningproject at Emory University. Depress Anxiety. 2008;25:482–488.
3. Downs MF, Eisenberg D. Help seeking and treatmentuse among suicidal college students. J Am Coll Health. 2012;60:104–114.
4. Blanco C, Okuda M, Wright C, et al. Mental health of col-lege students and their non-college-attending peers: results fromthe national epidemiologic study on alcohol and related conditions.Arch Gen Psychiatry. 2008;65:1429–1437.
5. Gaultney JF. The prevalence of sleep disorders in collegestudents: impact on academic performance. J Am Coll Health.2010;59:91–97.
6. Harvey AG. Insomnia, psychiatric disorders, and thetransdiagnostic perspective. Curr Dir Psychol Sci. 2008;17:299–303.
7. Salzer MS. A comparative study of campus experiencesof college students with mental illnesses versus a general collegesample. J Am Coll Health. 2012;60:1–7.
8. Keng S, Smoski MJ, Robins CJ. Effects of mindfulness onpsychological health: a review of empirical studies. Clin PsycholRev. 2011;31:1041–1056.
9. Oman D, Shapiro SL, Thoresen CE, Plante TG, FlindersT. Meditation lowers stress and supports forgiveness among col-lege students: a randomized controlled trial. J Am Coll Health.2008;56:569–578.
10. Warnecke E, Quinn S, Ogden K, Towle N, Nelson MR.A randomised controlled trial of the effects of mindfulnesspractice on medical student stress levels. Med Educ. 2011;45:381–388.
11. Franco C, Manas I, Cangas AJ, et al. The applicationsof mindfulness with students of secondary school: results onthe academic performance, self-concept and anxiety. In: LytrasMD, Ordonez De Pablos P, Ziderman A, et al, eds. Knowl-edge Management, Information Systems, E-Learning, and Sus-tainability Research. Berlin, Germany: Springer-Verlag; 2010:83–97.
12. Mrazek MD, Franklin MS, Phillips DT, Baird B, SchoolerJW. Mindfulness training improves working memory capacity andGRE performance while reducing mind wandering. Psychol Sci.2013;24:776–781.
13. Kabat-Zinn J. An outpatient program in behavioral medicinefor chronic pain patients based on the practice of mindfulness medi-tation: theoretical considerations and preliminary results. Gen HospPsychiatry. 1982;4:33–47.
14. Khoury B, Lecomte T, Fortin G, et al. Mindfulness-based therapy: a comprehensive meta-analysis. Clin Psychol Rev.2013;33:763–771.
15. Eberth J, Sedlmeier P. The effects of mindfulness medita-tion: a meta-analysis. Mindfulness. 2012;3:174–189.
16. Burke CA. Mindfulness-based approaches with children andadolescents: a preliminary review of current research in an emergentfield. J Child Fam Stud. 2010;19:133–144.
17. Arnett JJ. Emerging adulthood: a theory of develop-
ment from the late teens through the twenties. Am Psychol.2000;55:469–480.
18. Aud S, Hussar W, Johnson F, et al. The Condition of Educa-tion 2012. Washington, DC: National Center for Education Statis-tics, US Department of Education; 2012.
19. Arnett JJ. Emerging Adulthood: The Winding Road From theLate Teens Through the Twenties. New York, NY: Oxford UniversityPress; 2004.
20. Rogers HB. Koru: teaching mindfulness to emerging adults.New Direct Teach Learn. 2013;2013(134):73–81.
21. Rogers H, Maytan M. Mindfulness for the Next Generation:Helping Emerging Adults Manage Stress and Lead Healthier Lives.New York, NY: Oxford University Press; 2012.
22. Finkelstein C, Brownstein A, Scott C, Lan Y. Anxiety andstress reduction in medical education: an intervention. Med Educ.2007;41:258–264.
23. Saunders PA, Tractenberg RE, Chaterji R, et al. Promot-ing self-awareness and reflection through an experiential mind-body skills course for first year medical students. Med Teach.2007;29:778–784.
24. Shapiro S, Schwartz G, Santerre C. Meditation and pos-itive psychology. In: Snyder CR, Lopez SJ, eds. Handbook ofPositive Psychology. New York, NY: Oxford University Press;2002:632–645.
25. Neff KD, Rude SS, Kirkpatrick KL. An examination of self-compassion in relation to positive psychological functioning andpersonality traits. J Res Pers. 2007;41:908–916.
26. Fredrickson BL, Cohn MA, Coffey KA, Pek J, Finkel SM.Open hearts build lives: positive emotions, induced through loving-kindness meditation, build consequential personal resources. J PersSoc Psychol. 2008;95:1045–1062. doi: 10.1037/a0013262.
27. Faul F, Erdfelder E, Lang A, Buchner A. G∗ power 3: aflexible statistical power analysis program for the social, behavioral,and biomedical sciences. Behav Res Methods. 2007;39:175–191.
28. Cohen S, Janicki-Deverts D. Who’s stressed? Distribu-tions of psychological stress in the united states in probabil-ity samples from 1983, 2006, and 2009. J Appl Soc Psychol.2012;42:1320–1334.
29. Cronbach, L. J. Coefficient alpha and the internal structureof tests. Psychometrika. 1951;16:297–334.
30. Spritzer KL, Hays RD. MOS Sleep Scale: A Manual for Useand Scoring. Version 1.0. Los Angeles, CA: RAND; November2003.
31. Feldman G, Hayes A, Kumar S, Greeson J, Laurenceau JP.Mindfulness and emotion regulation: the development and initialvalidation of the cognitive and affective mindfulness scale-revised(CAMS-R). J Psychopathol Behav Assess. 2007;29:177–190.
32. Greeson JM, Webber DM, Smoski MJ, et al. Changesin spirituality partly explain health-related quality of life out-comes after mindfulness-based stress reduction. J Behav Med.2011;34:508–518.
33. Neff KD. The development and validation of a scale to mea-sure self-compassion. Self Identity. 2003;2:223–250.
34. Neff KD, Germer CK. A pilot study and randomized con-trolled trial of the Mindful Self-compassion program. J Clin Psy-chol. 2013;69:28–44.
35. McCullough ME, Emmons RA, Tsang JA. The grateful dis-position: a conceptual and empirical topography. J Pers Soc Psychol.2002;82:112–27.
36. McCullough ME, Tsang J, Emmons RA. Gratitude in in-termediate affective terrain: links of grateful moods to individualdifferences and daily emotional experience. J Pers Soc Psychol.2004;86:295–309.
37. Singer JD, Willett JB. Applied Longitudinal Data Analysis:Modeling Change and Event Occurrence. New York, NY: OxfordUniversity Press; 2003.
38. Cohen J. Statistical Power Analysis for the Behavioral Sci-ences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum; 1988.
232 JOURNAL OF AMERICAN COLLEGE HEALTH
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4

A Randomized Controlled Trial of Koru
39. Friedman LM, Furberg CD, DeMets DL. Fundamentals ofClinical Trials. New York, NY: Springer; 1998.
40. Keyes CL, Eisenberg D, Perry GS, Dube SR, Kroenke K,Dhingra SS. The relationship of level of positive mental healthwith current mental disorders in predicting suicidal behavior andacademic impairment in college students. J Am Coll Health.2012;60:126–133.
41. Regehr C, Glancy D, Pitts A. Interventions to reduce stressin university students: a review and meta-analysis. J Affect Disord.2013;148:1–11.
42. Deckro GR, Ballinger KM, Hoyt M, et al. The evalua-tion of a mind/body intervention to reduce psychological dis-tress and perceived stress in college students. J Am Coll Health.2002;50:281–287.
43. Jain S, Shapiro SL, Swanick S, et al. A randomized con-trolled trial of mindfulness meditation versus relaxation training:effects on distress, positive states of mind, rumination, and distrac-tion. Ann Behav Med. 2007;33:11–21.
44. Winbush NY, Gross CR, Kreitzer MJ. The effects ofmindfulness-based stress reduction on sleep disturbance: a system-atic review. Explore (NY). 2007;3:585–591.
45. Gross CR, Kreitzer MJ, Reilly-Spong M, et al. Mindfulness-based stress reduction versus pharmacotherapy for chronic primaryinsomnia: a randomized controlled clinical trial. Explore (NY).2011;7:76–87.
46. Britton WB, Haynes PL, Fridel KW, Bootzin RR.Polysomnographic and subjective profiles of sleep continuity before
and after mindfulness-based cognitive therapy in partially remitteddepression. Psychosom Med. 2010;72:539–548.
47. Kuyken W, Watkins E, Holden E, et al. How doesmindfulness-based cognitive therapy work? Behav Res Ther.2010;48:1105–1112.
48. Birnie K, Speca M, Carlson LE. Exploring self-compassionand empathy in the context of mindfulness-based stress reduction(MBSR). Stress Health. 2010;26:359–371.
49. Kabat-Zinn J. Full Catastrophe Living: Using the Wisdomof Your Body and Mind to Face Stress, Pain, and Illness. New York,NY: Delacorte Press; 1990.
50. Zeidan F, Martucci KT, Kraft RA, McHaffie JG, Coghill RC.Neural correlates of mindfulness meditation-related anxiety relief[published online ahead of print April 24, 2013]. Soc Cogn AffectNeurosci. doi:10.1093/scan/nst041.
51. Sauer S, Walach H, Schmidt S, et al. Assessment ofmindfulness: review on state of the art. Mindfulness. 2013;4:3–17.
52. Hofmann SG, Sawyer AT, Witt AA, Oh D. The effectsof mindfulness-based therapy on anxiety and depression: a meta-analytic review. J Consult Clin Psychol. 2010;78:169–183.
Received: 22 June 2013Revised: 12 January 2014
Accepted: 20 January 2014
VOL 62, MAY/JUNE 2014 233
Dow
nloa
ded
by [
98.1
15.1
43.1
86]
at 1
1:48
09
May
201
4