Embed Size (px)
Citation preview

Pieces of time
Valerie Young RGN RMN PGDip. Health Visiting BA (Hons) MScSenior Teaching Fellow, University of Luton, Department of Health and Social Organizations, Aylesbury Vale Education Centre,Stoke Mandeville Hospital, Aylesbury, UK
Abstract Drawing on research data from a recent project, this paper reveals howcultural, organizational, professional and personal dimensions of timeaffect nurses’ availability to care and patients’ experiences of beingcared for. Here, I will philosophize these dimensions of time throughboth the philosophical stance of the research methodology used in thestudy – phenomenological hermeneutics – and by engaging in philo-sophical theory that explores and challenges nurse and patient talkduring interview. Patients’ experiences of time tend to be embodied,whereas nurses choose between a disembodied structure of linear clocktime or an embodied more spiritual experienced sense of time. Tocapture differences and their significance to caring, this paper firstexplores the way cursive time shapes and controls caring encounters.Following this, research data will be explored to demonstrate how anexpanded notion of time as both cursive and circular enables nurses tosense patients’ illness patterns and to move with the ebb and flow ofpatients’ life/illness experiences. Next, the moment or the act of caringis explored as a presence, as a moral stance or presencing of the nursefor the patient. Finally, the notion of timelessness or what Kristéva calls‘monumental time’ is explored in the context of the nurse/patient givingand gifting relationship, particularly their giving/gifting of voice andwords to each other. Sensual, cultural and historical appreciation ofthese time dimensions is invited through the use of visual imagery.Exposure of the limitations, locations and dislocations of languagereveals the therapeutic power of silence, quiet and stillness. Conse-quently, poetry will be used to expand the visual imagery and engagethe reader in the silence from which words emerge, and the silence
Correspondence: Valerie Young, 3 Ash Grove, Aylesbury, Bucks HP21 7 PU, UK. Tel.: + 44 (0) 1296 397881 (home), 01296 315580
(work); fax: + 44 1296315567; e-mail: [email protected]
Ori
gina
l Art
icle
90 © Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103

Pieces of Time 91
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
that lives between and within words, the silence of timelessness. OO’Donohue says ‘When we forget or neglect this silence we empty our world of its secret and subtle presences’.
Keywords: linear time, circular time, monumental time, deep time,presence, giving.
ence and unreflective habitual practices. The messagepermeates and transcends individual caring work andindividual lives and will echo through the paper toevoke both this continuous presence and the silencebetween words:
In order to arrive there,
To arrive where you are, to get from where you are not,
You must go by a way wherein there is no ecstasy.
In order to arrive at what you do not know
You must go by a way which is the way of ignorance.
In order to possess what you do not possess
You must go by the way of dispossession.
In order to arrive at what you are not
You must go through the way in which you are not.
(Eliot, 1959, p. 25)
Linear (cursive) and cyclical time orientations ofnurses determine the kind of care they provide.However, deep time (Kearney, 1996) and monumen-tal time orientations (Kristéva, 1986), though noteasily articulated, were revealed in the study and willbe analysed philosophically. Archetypal images frommythology connote diverse understandings of timeand though Jung holds that archetypal images are notrepresentable in the conscious, I hope that their usein this paper informs monumental and deep time andtheir importance to caring.
Shades and shapes of time
Most nurses in the study said that they were accul-turated to manage time in a linear, cursive way andon the whole felt comfortable with this relationship.However, they also complained that caring was jeop-ardized by linear time whose unidirectional flow –moving from beginning to the end of sequences such
Introduction
In a recent qualitative study that explored with nurseshow culture influenced their professional manage-ment of critical incidents (Young, 2000), nurses identified time as a major concern, and a powerfuldeterminant of their availability to care. Caringembraced cursive time, circular time, monumentaltime and deep time or timelessness. The study con-cluded that expert nursing was artistic, weaving dif-ferent time orientations together like a patchworkquilt to solve problems in caring. It was as though thefabrics of people’s lives, even when seemingly intatters, could be rendered further apart or could bemended or re-created to help patients continue theirlife work depending on professional artistry, avail-ability and presence.
The research methodology used in the project, phe-nomenological hermeneutics, calls attention to theresearcher’s need to honour and disturb the taken for granted, to appreciate the naïve reading, the historicity and the deferral of meaning involved ininterpretation. In the context of this research, itemphasized the need to attend to the many dimen-sions of time–space relationships involved in caring:the reflexivity that phenomenological hermeneuticsdemands consistently articulates time with place withpeople. This articulation engages the ethic dimensionby locating the researcher in the research question(Frid et al., 2000) and by requiring the researcher’sconcern for the utterer (co-participant) and the utter-ances (Ricoeur, 1981).
T.S Eliot’s Four Quartets is a powerful reminder ofuncertainty. It addresses the importance of reflexivity,the constancy of change, and the need for silence andstillness to honour the present. The poetry also dif-ferentiates between the notion of continuous pres-

92 Valerie Young
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
as a work shift or a task – trapped them in unsatis-factory practices.
Joanne, in talking of her work on a psychiatricward, said:
It is the whole set up – the time given and the number of
staff.There is so much to do and such little time to do it.You
are caring for [patients] as a group but not for an individual.
(Young, 2000)
Nurses related cursive time to hierarchy, and the lit-erature also relates it to masculinity (Zerubavel, 1979;Kristéva, 1986). When this time orientation aloneinformed practice, it put a bounded structure ofcaring in place that though sometimes scaffoldinginexperienced nurses by helping them structure theirday, at other times stilted the caring work of moreexperienced nurses. Cursive time distanced nursesfrom patients by objectifying caring in tasks ratherthan subjectifying caring within relationships. Nurses’talk of their working lives tended to be dominated by the linear or cursive, and was mostly described asunidirectional, moving from a to b, from the begin-ning to the end in a relentless, systematic, unstoppablejourney, which in western culture is also accepted tobe from left to right, from west to east (Lippincottet al., 1999). Bauman (1993), however, stresses that in our time-space linearity of modern memories,the past or what comes before is ‘lower’ or ‘inferior’in the vertical linear-space hierarchical movementbetween past, present and future (Bauman, 1993,p. 226). The implications of this for caring work will be discussed later. Within the study, the theme of dichotomies/relationships of lifetime/career timerevealed that a linear work structure limited women’s career opportunities and dislocated familylife because it would not accommodate patterns ofworking that fitted with patterns of women’s home lives. For example, a midwife who had left work to bring up a family said that she could notreturn to midwifery because of duty roster inflexi-bility in health care trusts. Instead she planned toresume a very different nursing career because shecould weave it more easily with her responsibi-lities at home. This example was typical of the con-flict between circular and linear time in nursing practice.
Circular, cyclical time is already perceived as femi-nine (Davies, 1990). One co-participant expressedcyclical time orientation in terms of an intricate motifcreated in a circular pattern by the waxing andwaning or natural rhythm (Kristéva, 1986; Bauman,1993) of patients’ symptoms and the nurse’s require-ment to be in that pattern with the patient. Severalnurses talked about the influence of intimate lifecycles on their ability to offer depth-caring.
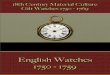
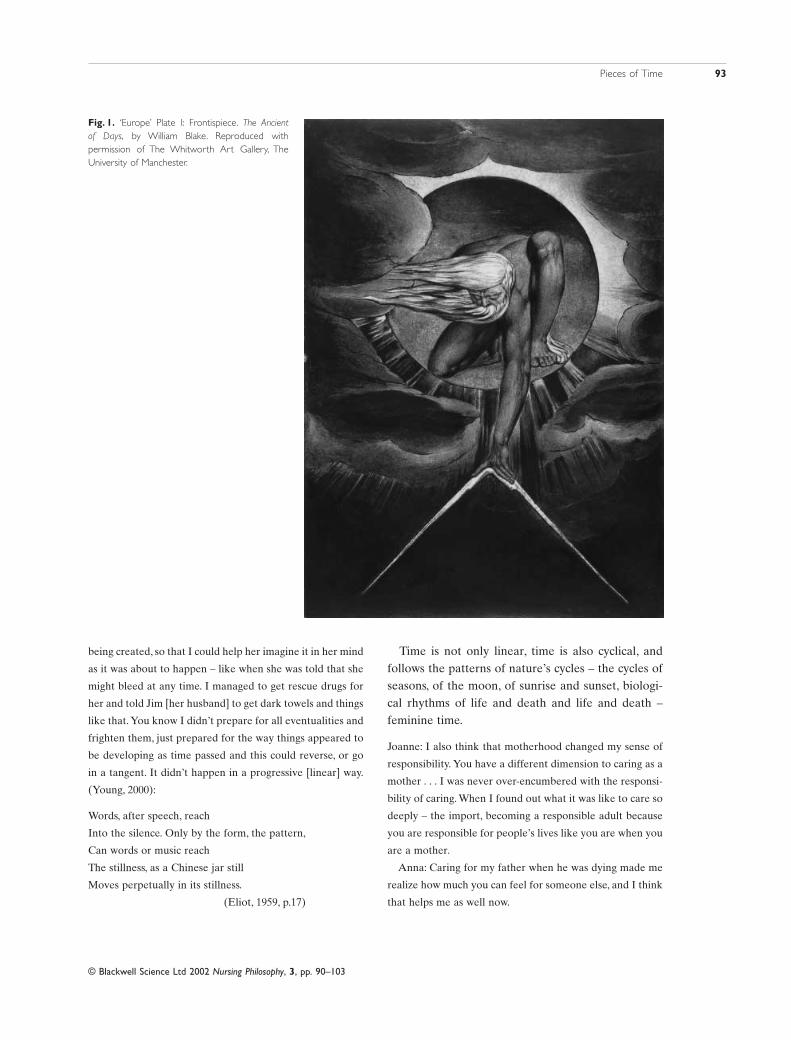
The Ancient of Days by William Blake (Fig. 1). Thisis a male God, Urizen, whose name is a play onreason. Urizen is holding a compass, a symbol of therational and the linear in a bid to overcome chaos andirrationality. The image has been interpreted as theeffort to crush man’s sense of depth and infinity, andto confine him within the narrow walls of his fivesenses (Lippincott, 1999) and in the context of thisdiscussion symbolizes nurse and patient strugglesbetween linear and circular time orientations. The following story from the research project outlines this tension.
Becci: The district nurse gave Mary, just diagnosed as having
disseminated carcinoma, a trajectory of the rest of her life,
warning ‘I’m here at the beginning, I’ll be here at the end’,
warning her that she would need a pressure mattress even-
tually and would probably need hospital care and indicating
how she [the district nurse] would intervene at different
times. Mary [the patient] did not want her life measured out
in a line like this. So she refused to see the district nurse
again. (Young, 2000):
And the end and the beginning were always there
Before the beginning and after the end.
And all is always now. Words strain,
Crack and sometimes break, under the burden,
Under the tension, slip, slide, perish,
Decay with imprecision, will not stay in place,
Will not stay still. Shrieking voices
(Eliot, 1959, p.17)
Becci, the palliative care nurse tending Mary,said:
I had to manage this fine time line so tentatively. It was like
a delicate motif that we were creating together. I had to con-
sider what Mary needed to know next as it was emerging,
Pieces of Time 93
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
being created, so that I could help her imagine it in her mind
as it was about to happen – like when she was told that she
might bleed at any time. I managed to get rescue drugs for
her and told Jim [her husband] to get dark towels and things
like that. You know I didn’t prepare for all eventualities and
frighten them, just prepared for the way things appeared to
be developing as time passed and this could reverse, or go
in a tangent. It didn’t happen in a progressive [linear] way.
(Young, 2000):
Words, after speech, reach
Into the silence. Only by the form, the pattern,
Can words or music reach
The stillness, as a Chinese jar still
Moves perpetually in its stillness.
(Eliot, 1959, p.17)
Time is not only linear, time is also cyclical, andfollows the patterns of nature’s cycles – the cycles ofseasons, of the moon, of sunrise and sunset, biologi-cal rhythms of life and death and life and death – feminine time.
Joanne: I also think that motherhood changed my sense of
responsibility. You have a different dimension to caring as a
mother . . . I was never over-encumbered with the responsi-
bility of caring. When I found out what it was like to care so
deeply – the import, becoming a responsible adult because
you are responsible for people’s lives like you are when you
are a mother.
Anna: Caring for my father when he was dying made me
realize how much you can feel for someone else, and I think
that helps me as well now.
Fig. 1. ‘Europe’ Plate I: Frontispiece. The Ancient of Days, by William Blake. Reproduced with permission of The Whitworth Art Gallery, The University of Manchester.

94 Valerie Young
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
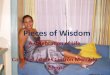
Motherhood by Jules Dalou (Fig. 2) represents thefeminine of caring. The statue is symbolic of the femi-nine archetype as life-giving, protective and nourish-ing. This particular sculpture is also a water fountain,suggestive that cyclical time precedes and accompa-nies linear time. In mythology the Goddesses of theMoon, Goddesses of Harvest and Goddess Psyche allsymbolize circular time. However, in contemporarysociety it is difficult to locate feminine mythologicalrepresentations, just as it is to recognize and affirmthe sensitivity of the feminine of caring to the circu-larity of the ebb and flow of illnesses: the districtnurse characterized Mary according to a partialmedical discourse that symbolically structured Mary’stime as waiting time. Mary’s role in this discoursemeant being forced to bear its meanings by the district nurse’s narrative control (Martin, 1998).However, Becci, the palliative care nurse, contested
this space through the application of a feminine nar-rative structure, which disconfirms a single linearityof cause (cancer) and effect (death). She created nar-rative space for different kinds of circular trajectoriesto emerge in the fluctuations of Mary’s symptoms,despite Mary’s prognosis.
Sensing time-lines in caring
The following example is from a pilot study con-ducted prior to the project. This example tentativelydraws on the sensuality of caring and thus to whatRussell (2000) calls the embodied conception ofethics.
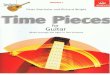
The Whisper by Andre Wallace (Fig. 3) is used here to symbolize the intimacy and connectionneeded for disclosure of the feared or denied secretsof illness.
Fig. 2. Motherhood, by Jules Dalou, is situated near the Royal Exchange,London.
Fig. 3. The Whisper, by Andre Wallace, is a large bronze sculpture positioned at the entrance to Milton Keynes Library, Milton Keynes,England.

Pieces of Time 95
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
Students and I established that we had all nursedsomeone with severe rheumatoid arthritis andtogether we created a sense of the embodiment ofrheumatoid arthritis and its possible individual mean-ings. I shared its visceral meaning to me in remem-bering a particular patient I had nursed: her fragileand transparent skin, the downy hair growing onpained arms and face as though attempting to caressthe pain away or protect her, her fragile hands andfeet, their distortion and the delicate ways we placedthem on surfaces.
We all have our images. One student, barely 3months into her nursing programme recalled a recentsituation where a staff nurse was escorting a womanwith painful arthritis to the bathroom. The staff nursewas in a hurry because it was time to do the druground. Her body language and use of body space andvoice reflected her impatience: she moved ahead ofthe patient, far enough ahead for the space betweenthem to become a distance for someone struggling tomove there. She also made tut-tutting sounds toemphasize her irritation at the woman’s slowness ofmovement into this distance created between them, aspace that became a tension, time tension, taut,tightrope, tut-tutting, violation of time, presence,space and voice.
Our ability to perceive this time-space (dis)con-nection, this actual moment of caring/uncaring isreflection in action. It acknowledges the emotional,reflective and sensual, aspects of ethical bodiesemphasized by Bauman (1993) and Irigaray (1985).We can recognize that the essential environment forcaring is always there. It is in the moment, in the timeand place and caring instant. We can revisit it andchange its dynamic because of our recognition of continuous presence.
Bauman (1993) draws attention to Levinas, whodiscussed the difference between ‘being for another’and ‘being with’ another. Interpreting the above situation in the light of Bauman’s work suggests thatthe staff nurse is with the patient. But being with
means being apart from her. She and the patient areontologically separate, ‘She [the patient] is but not[the staff nurse], the place [s]he occupies is a placewhere she [the staff nurse] is not’ (Bauman, 1993, p.70). However, Levinas’ theory of being for another
precedes ontology. It is transcendental because of itsability to rise above being and being with. Bauman(1993) calls this a moral responsibility because it isnot taken on as a contract but taken as though it isthere already and always as though it is ours withoutever being taken by us.This is what Bauman calls ‘face
to face’.
Le Baiser de l’aieule (The Grandmother’s Kiss) byJean Dampt (Fig. 4). (Bauman, 1993, p. 73) holds that:
. . . the face is what resists me . . . The absolute nakedness of
a face, the absolutely defenceless face without covering,
clothing or mask, is what opposes my power over it, my
violence.
Alone, the Other, the patient is weak, and it is pre-cisely that weakness that makes the nurse’s act ofpositioning her as a face a moral act. Bauman (1993,p. 79) speaks of the silence of the face of the Other,the authority that commands caring:
How troublesome is facing up, instead to that preontologi-
cal demand which conventions help us to conveniently
forget. That demand is Unspoken. The Other, as we remem-
ber, is not a force, but a face: The Other resists me simply by
being the Other, by her opposition - does not oppose me by
her resistance (resistance is something I am prompted to
fight against and overcome; it is the lack of resistance that
truly disarms). The Other is ‘only’ authority, and authority
does not need force. So the command to care, to ‘be for’, had
been given before it was spoken, and it would have been
given even if it was never spoke and was to remain silent
forever.
Bauman then asserts that had the patient asked thestaff nurse to be patient, to give her time, she wouldhave uncovered the staff nurse’s immorality. Thecommand to be responsible was there before wordsin a continuous presence, in the face, denied by thenurse in her hurry towards the future.
In terms of caring work Mayeroff (1990, p. 69) con-siders the relationship between place and time andhelps explain Bauman’s notion of being for in rela-tion to space/time. He says:
. . . place is not something I have, as if it were a possession.
Rather I am in-place because of the way I relate to others.
And place must be continually renewed and reaffirmed; it is

96 Valerie Young
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
not assured once and for all, for it is our response to the
need of others to grow which gives us place. In-place is as
much temporal as spatial, just as time is as much spatial as
temporal.
Nurses’ stories reveal their struggle to be in-placein terms of being in right relation with self and otherin time. So many nurses tread the line of linear time and their place is inscribed by clock-regulatedroutines of institutional place. In response to themechanics of linear time, they can so easily becomemechanical in their work and perceive both time andplace as immutable, as was evident in the aboveresearch examples.
However, Kali Striding Over the Corpse of Shiva
(Fig. 5) plays out the tension between power of
time that passes and time as eternal/continuous. TheGoddess Kali according to Hindu belief is an aspectof Shiva. In Indian mythology Shiva is usuallydepicted as a dancer who embodies eternal energy.Kali is Shiva’s consort, the destructive, all-pervadingpower of time to destroy. She is symbolized as thedestroyer who activates the creative powers of Shiva.Here, she is represented as the active usherer ofdeath, whereas Shiva is represented as passive.As shetreads on him, however, he returns to life and beginsto swing his drum, thus calling all life into being (Lippincott, 1999). The cyclical life-death-life-deathunity of the couple in this sculpture challenges thedissonance of time dimensions evoked in The Ancientof Days. The prioritization of clock-time in profes-sional practice diminishes cyclical and deep-time.
Fig. 4. Le Baiser de l’aieule (Grandmother’s Kiss),1892, marble bust, by Jean Dampt. Reproduced by permission of Musée d’Orsay, © Photo RMN.

Pieces of Time 97
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
Being present and presencing:honouring the silent patient
Nurses are encouraged to expand their caring poten-tial through reflection. Caring potential is enhancedby time-sensitive reflection, such as reflection in andon action or reflection in the moment. Generallythough, reflection even at its most imaginative callson the past to help manage the present and anticipatethe future. But Løgstrup (1971) warns that not all ofcaring can call on the past. Being present is an activeprinciple, it means ‘presencing’ or doing presence.Presencing is a skill that emerges in relation with thepatient. Presencing is risky, imaginative, intuitive andspontaneous. Both risk and potential are connoted in
the sculpture Kali Striding Over the Corpse of Shiva:
there are times when carers embrace and advocatefor the silent and passive patient, re-calling them tolife or facilitating deep, soul time (Kearney, 1996).This aesthetics of the time/space occupied by bothpatient and carer will be explored more fully later. Ithink that patients more than nurses recognize thisvisceral dimension of being cared for. Professionalcarers don’t always recognize their embodied caringpotential, the potential that is energized by theirbodies by being present, because they are not presentwith their bodies nor with the bodies of patients: theyare ahead or behind because of hurry or worry.Dynamism and sensitivity with the use of space, theuse of our voices in the air, recognizing that my voice
Fig. 5. Kali Striding Over the Corpse of Shiva,late 19th century, painted clay. Reproduced bypermission of British Museum, © The BritishMuseum.

98 Valerie Young
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
moves to another in the air, and the words, a word, orsilence at the right time can make a difference. Howmuch time does this presencing take?
Open-heartedness enlarges the present and thusthe future and past. Mayeroff (1990, p. 24) again:
Patience is an important ingredient in caring: I enable the
other to grow in [her] own time and in [her] own way . . .
By being patient I give time and thereby enable the other
to find [herself] in her own time. The impatient [person],
on the other hand, not only does not give time, but . . .
often takes time away from the other. If we know that
someone is impatient with us, or if we are impatient with
ourselves, even the time that we might have had is often
reduced.
Dreyfus & Rabinov (1982) argue that humanthought operates within whole, intuitive imaginedconfigurations, rather than by breaking down units ofinformation by units of time. We can accept impre-cise, ambiguous and unordered information that doesnot follow normal scripts. We can attend to the textand margin together without neglecting one for theother. We can interpret by being both focused andlateral. In general terms Husserl, Heidegger andGadamer indicated that thought becomes aware of ahorizon, aims at a noema, a kind of object or picturethat configures or images an intuitive grasp of a situation and presents to the mind a spectacle orpanoramic field of orientation and expectation(Gergen, 1999).
John Constable’s paintings draw our attention to the notion of an intuitive horizon. His paint-ing – Study of Clouds Above a Wide Landscape
(not shown) – attempted to express the changingnature of the sky. Constable recognized that the skycannot be represented in a fixed, idealistic wayfavoured by artists of his time. Rather, as the sourceof light in nature and expression of emotion and sentiment, the sky needed to be understood and theessence was in appreciating and knowing how itchanged (Lippincott, 1999). This recognition con-notes a kind of organized search in which thoughtmoves towards what it looks for by ‘choosing’, that is,by discarding and recombining the data it needs, butnone the less without the prescription that deter-mines in advance what is appropriate to choose and
what is appropriate to see. To quote Watson (1999,p. 270):
One learns a landscape not by knowing the name or iden-
tity of everything in it but by perceiving the relationships in
it, by grasping the whole. It is through this tacit knowledge
that we engage in a quality of consciousness transformation
brought about by art, ritual, myth, metaphor and symbol.
Caring practice demands imagination and creativ-ity. (Bauman, 1993, p. 81) extends the horizon furtherin saying that moral practice ‘must hold the saintli-ness of the saints for its only horizon . . . must setitself standards that it cannot reach’.
Gifting: the voice of patients’ truths,a caring gift
Peter’s story
Peter too was silenced by medical words. When hefirst met his Macmillan nurse, she asked him to tellher about his understanding of his illness. In talkingabout his diagnosis he said: ‘The GP read aloud to mefrom his notes but I couldn’t make out the words. Ithink they were medical words . . . I didn’t under-stand. I was thinking to myself that I just didn’t knowwhat he was saying, when he looked up from thenotes, looked at me straight in the eye and said, ‘‘We’lldo the best we can to prolong your life” ’ (Young,2000).
Peter then looked at the nurse and said: ‘I supposewe’ll have to talk about this cancer but I don’t likeusing that word’. She replied: ‘If you don’t like usingthat word what word would you like to use?’ In amore confident voice he said: ‘My tumour doesn’tseem so frightening’ (Young, 2000). It doesn’t matterthat Peter also chose a clinical terminology, whatmatters was his comfort with this. During the initialmeeting between Peter and his Macmillan nurse sheobserved how his insular life and his sparse homemight be inhospitable to the normalization, by whichshe meant the institutionalization, expected by manycommunity nurses for home deaths. Peter’s eccen-tricity was difference, difference that could marsupport. His passion for his garden, its view andnature that surrounded him also indicated the inhos-pitality of a hospice death for someone like Peter.

Pieces of Time 99
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
Jean-Francois Lyotard (1988) reminds us that data,information we need to care, are not given but aregivable. This reminds us of the fragility, the creative-ness and precariousness of knowledge that informscaring. Lyotard warns that if you think you’re describ-ing thought when you describe a selecting and tabu-lating of data, you’re silencing truth. The art ofthinking, and caring, is almost no more than letting a givable come towards you. Lyotard & Watson(1999), thinkers in the postmodern, and Anderson &Goolishian (1992) explain this kind of attending toanother when they in their different ways emphasizethe sort of emptiness or rather suspension and still-ing of ordinary intentions of mind and receivedknowledge required to be open to the givable, thegifts of openness. The Whisper (Fig. 3) also suggeststhe attention and intimacy needed to appreciate
another. London Pride (Fig. 6) suggests the need foremptiness in order to fill up.
The nurse caring for Peter adapted a ‘not knowingstance’ (Anderson & Goolishian, 1992) and Peterfilled the space with gifts of honesty and disclosuresof his aloneness. At one point he asked: ‘What dopeople in my position do now? Do we commitsuicide?’ Despite the appearance of Peter’s alonenessin his home, he had a sense of belonging with himselfin his environment that his nurse intuited and workedwith. O’Donohue (1997, p. 114) talks of the strengthof belonging in your own interiority.
If you belong there, and if you are in rhythm with yourself
and connected to that deep unique source within, then you
will never be vulnerable when your outside belonging is
qualified, relativised or taken away.
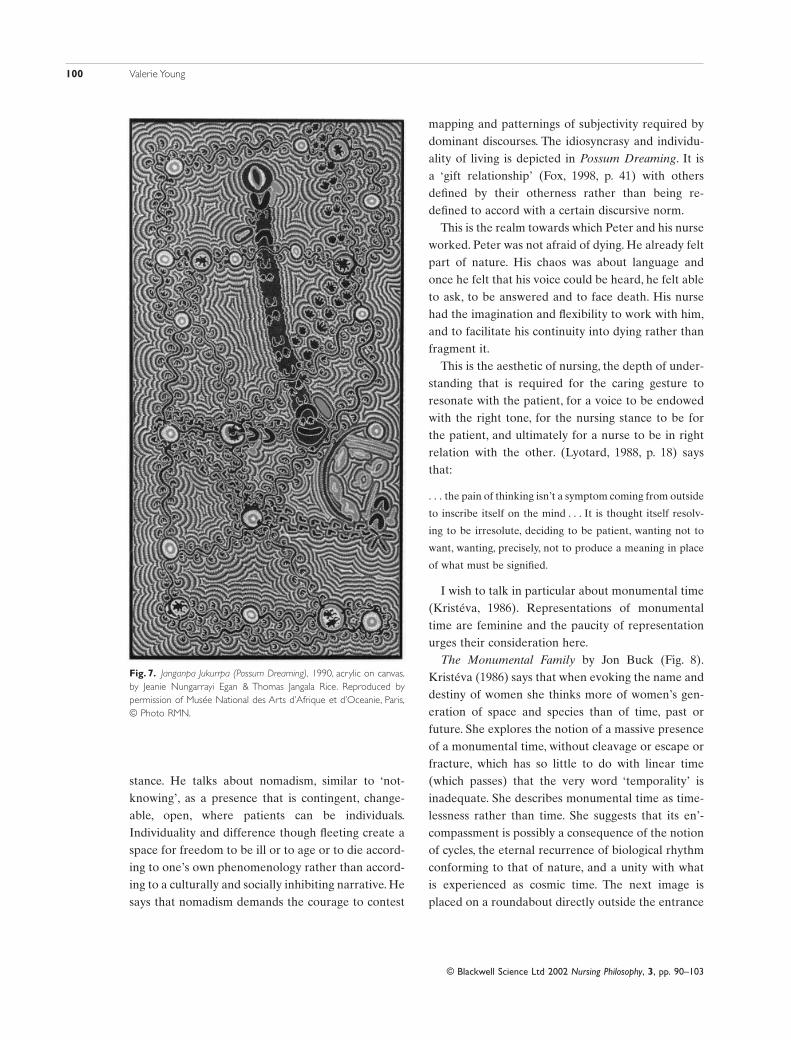
Janganpa Jukurrpa (Possum Dreaming) by JeanieNungarrayi Egan and Thomas Jangala Rice (Fig. 7).
Dreamtime paintings symbolize Peter’s sense of timeand place as a concept of time related to place. Thepaintings are like maps that synthesize all of apeople’s history: past, present and future. Time wascreated through the transformation of ancestralbeings into place. They (Peter) ‘sat down’ and, how-ever briefly they (he) stayed, they became part of the place forever. In Yolngu terms they (he) ‘turnedinto’ the place. The dreaming encompasses within itother temporalities: it integrates processes, personalmemories and historical events within its frame (Lippincott, 1999).
Or say that the end precedes the beginning
And the end and the beginning were always there
Before the beginning and after the end.
And all is always now.
(Eliot, 1959, p. 17)
Such reflections are also evident in Native Ameri-can culture. The features of a place such as a waterhole or a mountain would be described as a placewhere the ancestors live. In this image, the possum are travelling north looking for gum leaves. Everytime they stopped they were expressed on the formof the landscape and became present (Lippincott,1999).
Fox (1998) draws attention to this moving/stilling
Fig. 6. London Pride, by Frank Dobson. This sculpture is positionedoutside the National Theatre, Southbank, London.
100 Valerie Young
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
stance. He talks about nomadism, similar to ‘not-knowing’, as a presence that is contingent, change-able, open, where patients can be individuals.Individuality and difference though fleeting create aspace for freedom to be ill or to age or to die accord-ing to one’s own phenomenology rather than accord-ing to a culturally and socially inhibiting narrative. Hesays that nomadism demands the courage to contest
mapping and patternings of subjectivity required bydominant discourses. The idiosyncrasy and individu-ality of living is depicted in Possum Dreaming. It is a ‘gift relationship’ (Fox, 1998, p. 41) with othersdefined by their otherness rather than being re-defined to accord with a certain discursive norm.
This is the realm towards which Peter and his nurseworked. Peter was not afraid of dying. He already feltpart of nature. His chaos was about language andonce he felt that his voice could be heard, he felt ableto ask, to be answered and to face death. His nursehad the imagination and flexibility to work with him,and to facilitate his continuity into dying rather thanfragment it.
This is the aesthetic of nursing, the depth of under-standing that is required for the caring gesture to resonate with the patient, for a voice to be endowedwith the right tone, for the nursing stance to be forthe patient, and ultimately for a nurse to be in rightrelation with the other. (Lyotard, 1988, p. 18) saysthat:
. . . the pain of thinking isn’t a symptom coming from outside
to inscribe itself on the mind . . . It is thought itself resolv-
ing to be irresolute, deciding to be patient, wanting not to
want, wanting, precisely, not to produce a meaning in place
of what must be signified.
I wish to talk in particular about monumental time(Kristéva, 1986). Representations of monumentaltime are feminine and the paucity of representationurges their consideration here.
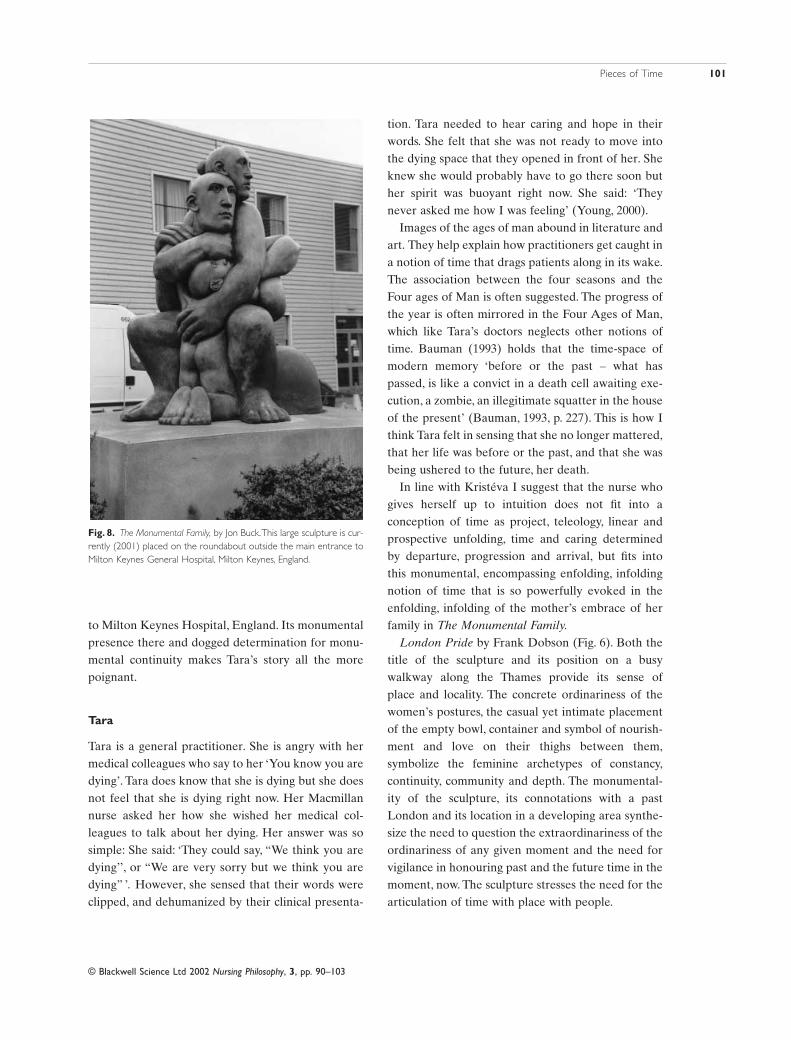
The Monumental Family by Jon Buck (Fig. 8).Kristéva (1986) says that when evoking the name anddestiny of women she thinks more of women’s gen-eration of space and species than of time, past orfuture. She explores the notion of a massive presenceof a monumental time, without cleavage or escape orfracture, which has so little to do with linear time(which passes) that the very word ‘temporality’ isinadequate. She describes monumental time as time-lessness rather than time. She suggests that its en’-compassment is possibly a consequence of the notionof cycles, the eternal recurrence of biological rhythmconforming to that of nature, and a unity with what is experienced as cosmic time. The next image is placed on a roundabout directly outside the entrance
Fig. 7. Janganpa Jukurrpa (Possum Dreaming), 1990, acrylic on canvas,by Jeanie Nungarrayi Egan & Thomas Jangala Rice. Reproduced by permission of Musée National des Arts d’Afrique et d’Oceanie, Paris,© Photo RMN.
Pieces of Time 101
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
to Milton Keynes Hospital, England. Its monumentalpresence there and dogged determination for monu-mental continuity makes Tara’s story all the morepoignant.
Tara
Tara is a general practitioner. She is angry with hermedical colleagues who say to her ‘You know you aredying’. Tara does know that she is dying but she doesnot feel that she is dying right now. Her Macmillannurse asked her how she wished her medical col-leagues to talk about her dying. Her answer was sosimple: She said: ‘They could say, “We think you aredying’’, or “We are very sorry but we think you aredying” ’. However, she sensed that their words wereclipped, and dehumanized by their clinical presenta-
tion. Tara needed to hear caring and hope in theirwords. She felt that she was not ready to move intothe dying space that they opened in front of her. Sheknew she would probably have to go there soon buther spirit was buoyant right now. She said: ‘Theynever asked me how I was feeling’ (Young, 2000).
Images of the ages of man abound in literature andart. They help explain how practitioners get caught ina notion of time that drags patients along in its wake.The association between the four seasons and theFour ages of Man is often suggested. The progress ofthe year is often mirrored in the Four Ages of Man,which like Tara’s doctors neglects other notions oftime. Bauman (1993) holds that the time-space ofmodern memory ‘before or the past – what haspassed, is like a convict in a death cell awaiting exe-cution, a zombie, an illegitimate squatter in the houseof the present’ (Bauman, 1993, p. 227). This is how Ithink Tara felt in sensing that she no longer mattered,that her life was before or the past, and that she wasbeing ushered to the future, her death.
In line with Kristéva I suggest that the nurse whogives herself up to intuition does not fit into a conception of time as project, teleology, linear andprospective unfolding, time and caring determined by departure, progression and arrival, but fits into this monumental, encompassing enfolding, infoldingnotion of time that is so powerfully evoked in theenfolding, infolding of the mother’s embrace of herfamily in The Monumental Family.
London Pride by Frank Dobson (Fig. 6). Both thetitle of the sculpture and its position on a busywalkway along the Thames provide its sense of place and locality. The concrete ordinariness of thewomen’s postures, the casual yet intimate placementof the empty bowl, container and symbol of nourish-ment and love on their thighs between them,symbolize the feminine archetypes of constancy,continuity, community and depth. The monumental-ity of the sculpture, its connotations with a pastLondon and its location in a developing area synthe-size the need to question the extraordinariness of theordinariness of any given moment and the need forvigilance in honouring past and the future time in themoment, now. The sculpture stresses the need for thearticulation of time with place with people.
Fig. 8. The Monumental Family, by Jon Buck.This large sculpture is cur-rently (2001) placed on the roundabout outside the main entrance toMilton Keynes General Hospital, Milton Keynes, England.

102 Valerie Young
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
Conclusion
In considering the ways that different notions of timereflect and command ways of caring, this paper relatesaesthetic thinking with the aesthetics of caring. Aes-thetic thinking has been discussed as a mode of think-ing according to which what doesn’t yet exist, a word,a reassurance, a whisper, a touch, caring, will emerge.This kind of reflective thinking challenges the way weare used to thinking according to the already-thought,the inscribed. This kind of reflective thinkingdemands holistic understanding of time that expandsthe linear to embrace circular and monumental time.This is the kind of thinking and working required to‘be for’ patients. Undoubtedly we habitually think ina world of prescriptions. Consequently, we find it verydifficult to be patient, to leave something hanging inabeyance or take it up again in a different way sowhat hasn’t been thought yet can emerge. Yet, theimpact of superficial narrative on the lives of nursesand patients outlined above emphasizes the need toquestion routine and repetitive practices.
To arrive where you are, to get from where you are not,
You must go by a way wherein there is no ecstasy.
In order to arrive at what you do not know
You must go by a way which is the way of ignorance.
Michael Kearney (1996) establishes that carersneed to create a holding environment, or empathic,skilled, aesthetic caring for the surface needs ofpatients to enable those who are in total pain, soulpain, to be in right relation with depth and this depthtemporality, this relation with soul or psyche can befrightening because of its unfamiliarity.This relates totribal connections with earth and soul such as NativeAmerican Ain-dah-ing or home to self, or celticunderstandings of the body as clay that returns toclay. Many of these relationships depict a sense ofplace and presence and time that is beyond words butwhich can be connoted in art.
A Wish to Touch the Sky by Hollis Sigler (Fig. 9).The artist, Hollis Sigler, attempted to be present inthe moment by representing her cancer experience bydrawing, painting and journaling her feelings andthoughts in one depth sitting as they occurred. Thevibrancy of this depth consideration of the present is
evoked in the powerful colours and movement in herwork. Here, the pegs that could hold her spirit in placeappear to become birds that carry her to freedom.Her caption beneath this painting says: ‘Cancer is aturning point when you can become free. It is to fulfila dream that can no longer wait. It is to understandthe moment’ (Sigler, 1999, p. 62). The present, themoment, the art of presencing oneself as a carer inthe actual moment of caring also demands a turningpoint, demands a change of rhythm from one that ishabitual, or one prescribed by work routine, to onethat is original and inspired. The newness, the poten-tial of each caring moment is evoked in differentkinds of reflective thinking that challenge the habitsof the past, and can also when appropriate invoke therisk of spontaneity and imagination. Hollis Sigler’spaintings tell of temporality, impermanence and dispossession.
You say I am repeating
Something I have said before. I shall say it again.
Shall I say it again? In order to arrive there,
To arrive where you are, to get from where you are not,
You must go by a way wherein there is no ecstasy.
In order to arrive at what you do not know
You must go by a way which is the way of ignorance.
In order to possess what you do not possess
You must go by the way of dispossession.
In order to arrive at what you are not
You must go through the way in which you are not.
(Eliot, 1959, p. 25)
Fig. 9. A Wish to Touch the Sky, 1994, oil pastel on paper, by Hollis Sigler.Reproduced from Hollis Sigler’s Breast Cancer Journal by permission ofthe publisher, Hudson Hills Press, New York, © 1999 Hollis Sigler.

Pieces of Time 103
© Blackwell Science Ltd 2002 Nursing Philosophy, 3, pp. 90–103
References
Anderson H. & Goolishian H. (1992) The client is theexpert: a not-knowing approach to therapy. In: Therapyas Social Construction (eds S. McNamee & K. Gergen),pp. 25–39. Sage, New York.
Bauman Z. (1993) Postmodern Ethics. Blackwell, Oxford.Davies K. (1990) Women, Time and the Weaving of the
Strands of Everyday Life. Avery, England.Dreyfus H.L. & Rabinov P. (1982) Michel Foucault:
Beyond Structuralism and Hermeneutics. HarvesterPress, Brighton.
Eliot T.S. (1959) Four Quartets. Faber & Faber,London.
Fox N. (1998) The promise of postmodernism for the sociology of health and medicine. In: Modernity,Medicine and Health (eds G. Scambler & P. Higgs),pp. 29–45. Routledge, London.
Frid I., Ohlen J. & Bergbom I. (2000) On the use of narra-tives in nursing research. Journal of Advanced Nursing,32(3), 695–703.
Gergen K.J. (1999) An Invitation to Social Construction.Sage, London.
Irigaray L. (1985) This Sex Which is not One. Cornell University Press, New York.
Kearney M. (1996) Mortally Wounded. Stories of SoulPain, Death and Healing. Marino Press, Dublin.
Kristéva J. (1986) Women’s time. In: The Kristeva Reader(ed. T. Moi), pp. 187–213. Blackwell, Oxford.
Lippincott K., Eco U., Gombrich E.H. et al. (1999) TheStory of Time. Merrell Hoberton, London.
Logstrup K.E. (1971) The Ethical Demand. Fortress Press,Philadelphia.
Lyotard J.-F. (1988) The Inhuman. Polity Press, Cambridge.Martin G.W. (1998) Empowerment of dying patients: the
strategies and barriers to patient autonomy. Journal ofAdvanced Nursing, 28(4), 737–744.
Mayeroff M. (1990) On Caring. HarperPerennial, NewYork.
O’Donohue J. (1997) Anam Cara: Spiritual Wisdom fromthe Celtic World. Bantam Press, London.
Ricoeur P. (1981) Hermeneutics and the Human Sciences.Cambridge University Press, New York.
Russell R. (2000) Ethical bodies. In: The Body, Culture andSociety: an Introduction (eds P. Hancock, B. Hughes,E. Jagger, K. Paterson, R. Russell, E. Tulle-Winton & M. Tyler), pp. 101–116. Open University Press,Buckingham.
Sigler H. (1999) Breast Cancer Journal. Hudson Hills Press,New York.
Watson J. (1999. Postmodern Nursing and Beyond.Churchill Livingstone, London.
Young V. (2000) Good enough nursing: an exploration ofthe ways that nurses negotiate interprofessional rela-tionships in managing critical incidents. Unpublisheddissertation, University of Luton, Luton.
Zerubavel E. (1979) Patterns of Time in Hospital Life.University of Chicago Press, Chicago.







![JamSpace: A Networked Real-Time Collaborative Music ... · collaborative composition, artificially-synchronized pseudo-real-time performance [14], or real-time pieces ... icon from](https://img.pdfslide.us/doc/110x75/5f0512ab7e708231d4111ffa/jamspace-a-networked-real-time-collaborative-music-collaborative-composition.jpg)