Embed Size (px)
Citation preview
2017-02-06
1
The Use of PICCs Within Critical Care
Lynn Hadaway, M.Ed., RN-BC, CRNI
Disclosure
• Lynn Hadaway is a paid consultant for BBraun of Canada, Ltd
• Development and delivery of thispresentation was commissioned by B Braunof Canada, Ltd
2017-02-06
2
Disclosures
• Speaker and/or consultant for:– 3M– Atrion Corp– B Braun Medical, Inc– B Braun of Canada,
Ltd– Bard Access Systems– Baxter– BD Medical– Covidien/Medtronic
– Elcam– Excelsior– Fresinius Kabi– Gayco Healthcare– LineGard Medical– Lippincott Williams
Wilkins– Terumo– VATA– Velano Vascular
Learning Objectives
• Identify the current standards and guidelines applicable to PICC insertion and management.
• Describe the clinical considerations for PICCs used in critical care.
• Analyze PICC complications associated with critical care patients.
2017-02-06
3
Standards and Guidelines
• CDC– Prevention of Intravascular Catheter-Related Infections,
2011– https://www.cdc.gov/hicpac/pdf/guidelines/bsi-guidelines-2011.pdf
• Safer Healthcare Now– Preventing Central Line Infections, 2012– www.saferhealthcarenow.ca
• Canadian Vascular Access Association– Occlusion Management Guideline for Central Venous
Access Devices, 2013– http://cvaa.info/PUBLICATIONS/OcclusionManagementGuideline(O
MG)/tabid/229/Default.aspx
Standards and Guidelines
• Department of Health, England
– Epic3: National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospital in England, 2013
– https://www.his.org.uk/files/3113/8693/4808/epic3_National_Evidence-Based_Guidelines_for_Preventing_HCAI_in_NHSE.pdf
• Society for Healthcare Epidemiology of America (SHEA)
– Strategies to Prevent Central Line-Associated , 2014 Update
– http://journals.cambridge.org/action/displayAbstract?fromPage=online&aid=10312269&fulltextType=RA&fileId=S0899823X00193870
2017-02-06
4
Standards and Guidelines
• Canadian Hemodialysis Access Coordinators Network
– Nursing Recommendations for the Management of Vascular Access in Adult Hemodialysis Patients: 2015 Update
– http://www.cannt.ca/files/CANNT-VA%20Guidelines-2016Jan4-NP.pdf
• Infusion Nurses Society
– Infusion Therapy Standards of Practice, 2016– https://www.ins1.org/Store/ProductDetails.aspx?productId=241097
Clinical Considerations
• Vascular Access Planning (Gorski, 2016)– Preservation of peripheral veins!!
– Most appropriate VAD selection• Collaborative process among the interprofessional
team, the patient, and caregivers
• Least invasive device, Smallest outer diameter, Fewest number of lumens needed for prescribed therapy
– PICCs are NOT an infection prevention strategy!
2017-02-06
5
Clinical Considerations
• Hemodynamically UNstable patients– Recommendations from the MAGIC study
• Centrally inserted central catheter (CICC) for therapy of 14 days or less
• PICC for 15 days or more, but CICC is preferred
• PICCs preferred in critical patient with coagulopathies or sepsis (Chopra, 2015)
Clinical Considerations
• Avoid PICCs in – Stage 4 or 5 Chronic Kidney Disease
– Patients with abnormal creatinine or eGFR (CANNT, 2016)
• Use with caution in oncology and critical care patients– Risk of venous thrombosis and infection (Gorski, 2016)
• PICC outer diameter should consume 45% or less of vein diameter (Gorski, 2016)
2017-02-06
6
Clinical Considerations
• Mid-upper arm circumference (Gorski, 2016)– Before inserting PICC for baseline
– When clinically indicated
– Measure 10 cm above antecubital fossa
• Presence of pacemaker (Gorski, 2016)– Place PICC on opposite side, if possible
– Evaluate pacemaker function before and after PICC insertion
Clinical Considerations
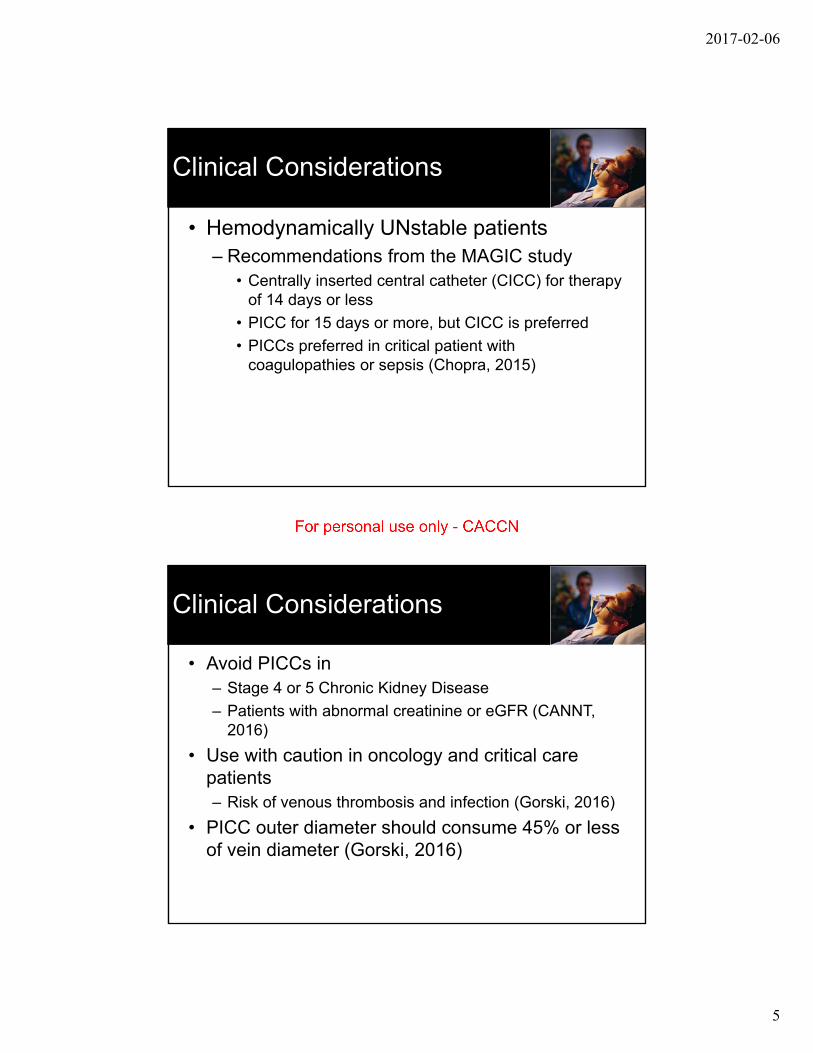
• Ultrasound guidance for vein selection and insertion
• Maximum barriers– Full body drape
– Long sleeve gown
– Gloves
– Hair and face cover
• Alcoholic chlorhexidine skin antiseptic
2017-02-06
7
Clinical Considerations
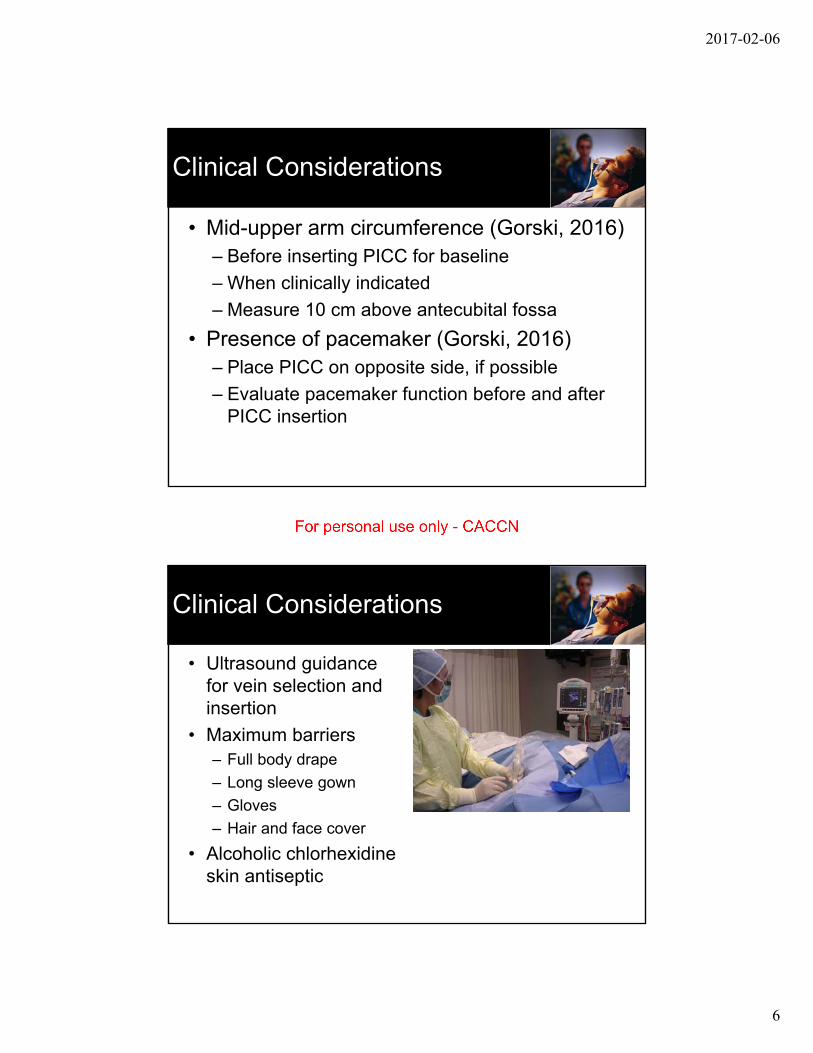
• Tip location for all Central VADs– Location with greatest safety profile is
cavoatrial junction (CAJ)
– Body movement will mean PICC tip moving into right atrium
Clinical Considerations
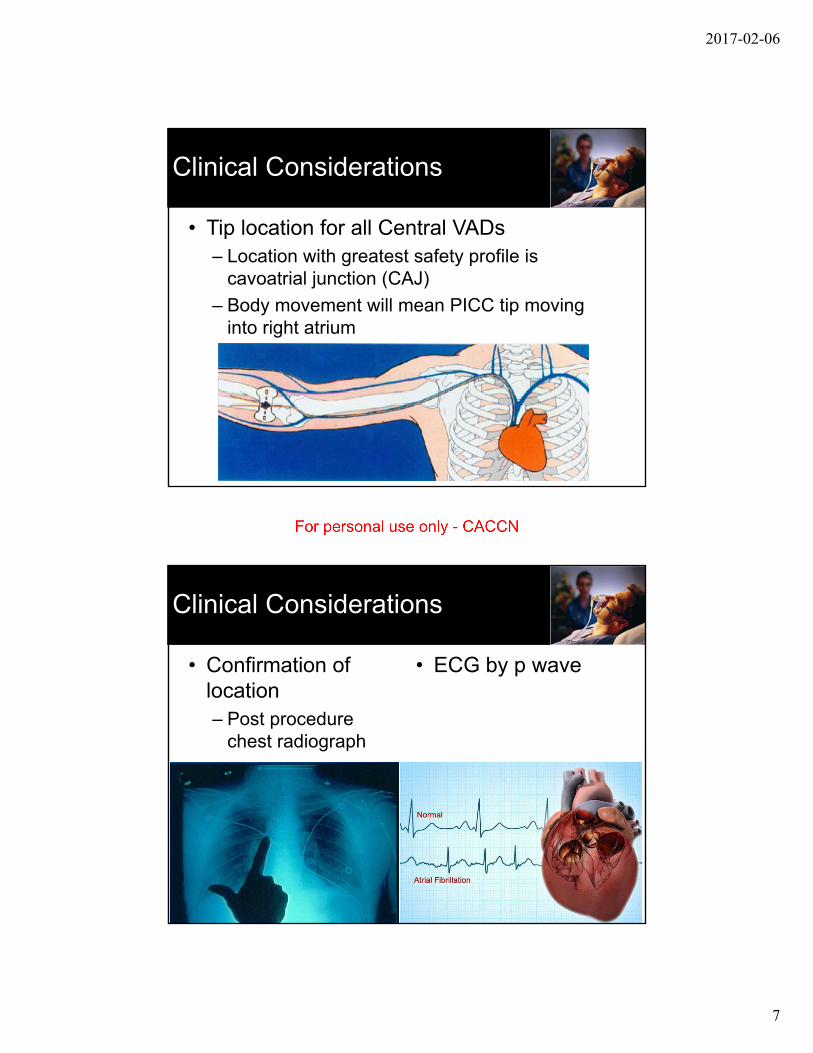
• Confirmation of location– Post procedure
chest radiograph
• ECG by p wave
2017-02-06
8
Clinical Considerations
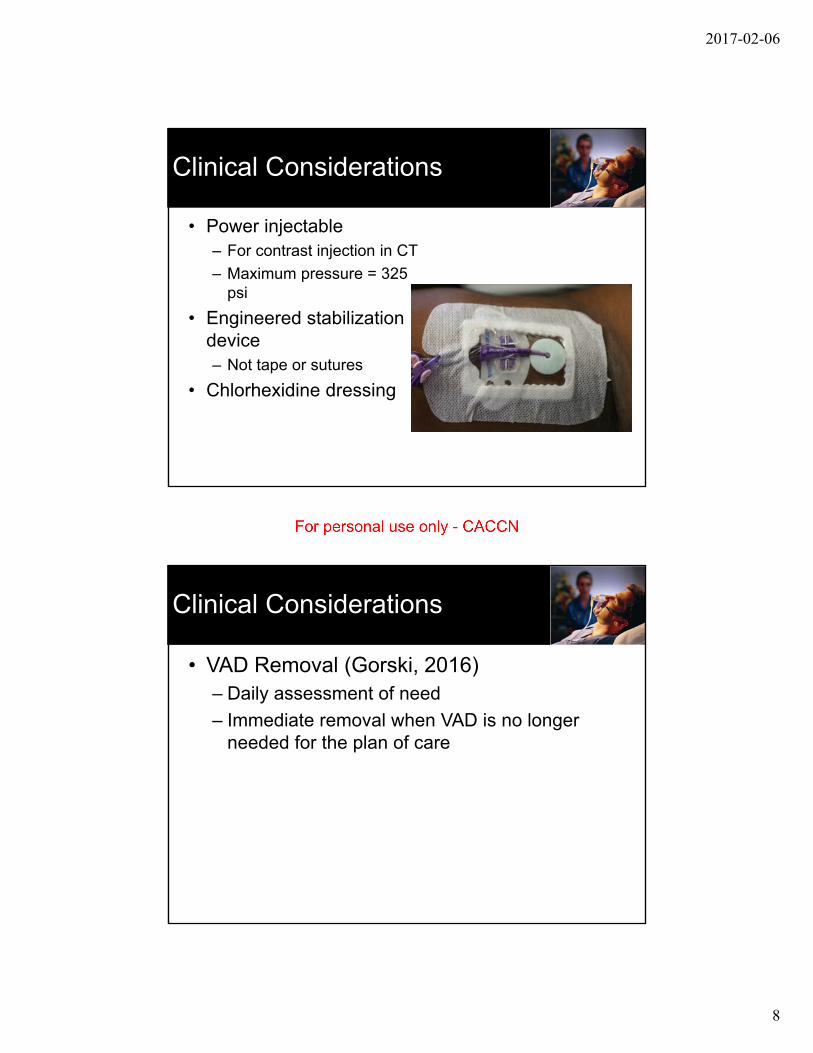
• Power injectable– For contrast injection in CT
– Maximum pressure = 325 psi
• Engineered stabilization device – Not tape or sutures
• Chlorhexidine dressing
Clinical Considerations
• VAD Removal (Gorski, 2016)– Daily assessment of need
– Immediate removal when VAD is no longer needed for the plan of care
2017-02-06
9
PICC Complications
• Critical care patients– Mechanical problems
– Bloodstream infection
– Vein thrombosis
PICC Complications
• Mechanical problems– Tip malposition (Gorski, 2016)
• Primary malposition – occurs on insertion and corrected immediately
– Intracardiac by more than 2 cm from CAJ
• Secondary malposition – occurs during dwell– Also known as tip migration
– Original tip location high in SVC or brachiocephalic vein
– Changes in intrathoracic pressure
– Body movement – neck, arm, shoulder
– Vein thrombosis
– Power injection in CT
2017-02-06
10
PICC Complications
• Mechanical problems– Tip malposition (Gorski, 2016)
• Intravascular– Jugular
– Contralateral subclavian
– Azygos
– Small tributary veins
– Aberrant venous anatomy such as persistent left SVC
• Extravascular– Erosion of catheter tip through vein wall
– Fistula between vein and artery
– Cardiac tamponade
PICC Complications
• Mechanical problems– Tip malposition
• Withhold infusion through PICC
• Develop plan for identification of tip and repositioning or removal
• A major reason for the importance of a blood return!!
2017-02-06
11
PICC Complications
• Know signs and symptoms of malposition– No blood return
– Pulsatility of blood return
– Resistance when flushing
– Alteration in waveform when transducer is attached
– Dyshythmias
– Changes in vital signs
– Pain and/or edema in chest, shoulder, neck, back
– Complaints of hearing a running stream on ipsilateral side
– Neurological problems
PICC Complications
• Bloodstream Infection– Retrospective audit of medical records for all
hospitalized patients with PICC insertion over a 3-year period (Chopra, 2014)
• 966 PICCs, 171 (18%) in ICU patients
• 58 (6%) with PICC-associated BSI over 1156 catheter days
• 2.16 per 1000 catheter days
• Median time to infection = 10 days
• Greatest risk factors by multivariate analysis:– Hospital length of stay
– ICU status
– Number of lumens
2017-02-06
12
PICC Complications
• Bloodstream Infection– Systematic literature review and meta-analysis
in hospitalized patients (Chopra, 2013)• CLABSI rates with PICCs statistically the same as
other CICCs
• Rates for both catheters similar for critical care patients
PICC-CLABSI CICC-CLABSI
Incidence 5.2% 5.8%
# of CLABSI (# of patients)
76 (1473) 76 (1302)
Sources of Microbes
• Skin – Insertion site
– Hands of caregivers
• Hub
• Infusate
• Seeding from other infection sites
2017-02-06
13
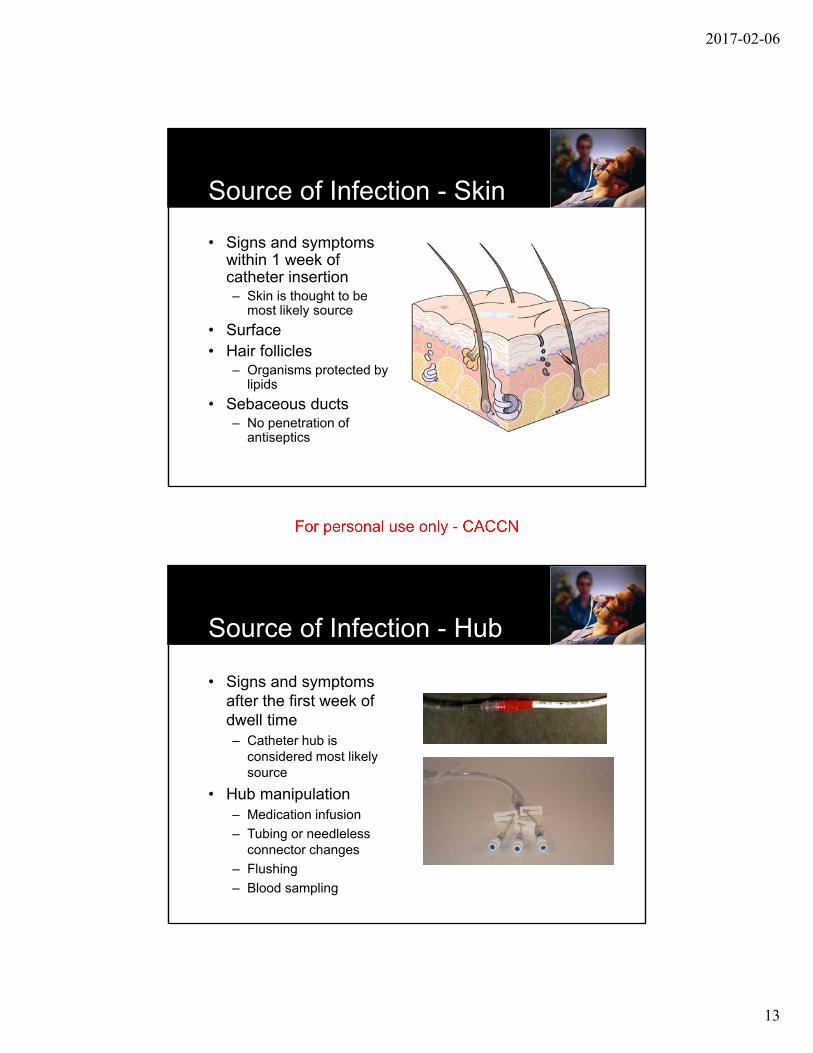
Source of Infection - Skin
• Signs and symptoms within 1 week of catheter insertion– Skin is thought to be
most likely source
• Surface• Hair follicles
– Organisms protected by lipids
• Sebaceous ducts– No penetration of
antiseptics
Source of Infection - Hub
• Signs and symptoms after the first week of dwell time– Catheter hub is
considered most likely source
• Hub manipulation – Medication infusion
– Tubing or needleless connector changes
– Flushing
– Blood sampling
2017-02-06
14
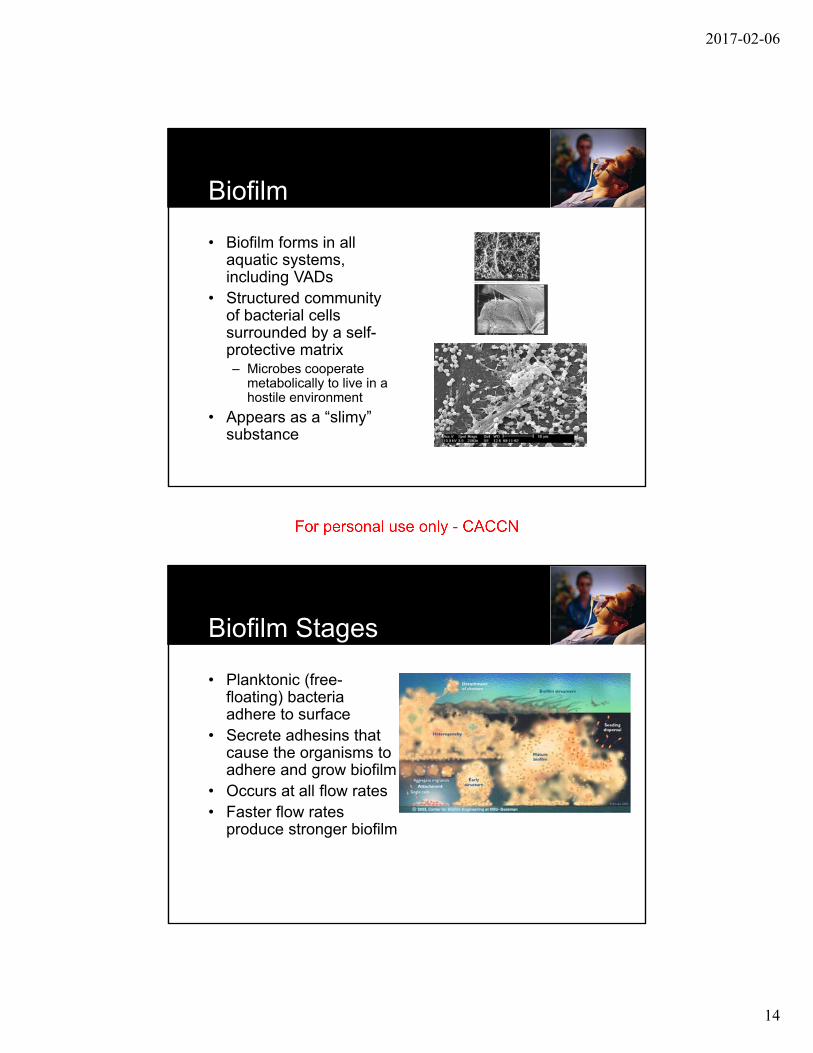
Biofilm
• Biofilm forms in all aquatic systems, including VADs
• Structured community of bacterial cells surrounded by a self-protective matrix– Microbes cooperate
metabolically to live in a hostile environment
• Appears as a “slimy”substance
Biofilm Stages
• Planktonic (free-floating) bacteria adhere to surface
• Secrete adhesins that cause the organisms to adhere and grow biofilm
• Occurs at all flow rates• Faster flow rates
produce stronger biofilm
2017-02-06
15
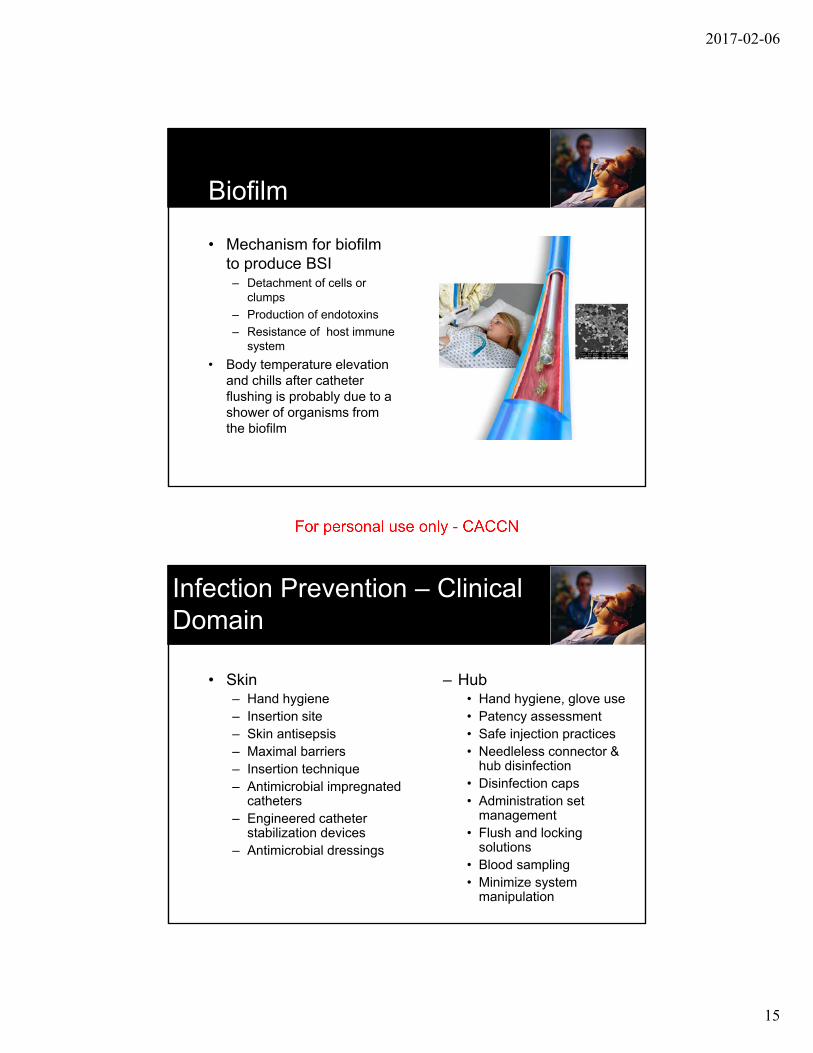
Biofilm
• Mechanism for biofilm to produce BSI– Detachment of cells or
clumps
– Production of endotoxins
– Resistance of host immune system
• Body temperature elevation and chills after catheter flushing is probably due to a shower of organisms from the biofilm
Infection Prevention – Clinical Domain
• Skin– Hand hygiene– Insertion site– Skin antisepsis– Maximal barriers– Insertion technique– Antimicrobial impregnated
catheters– Engineered catheter
stabilization devices– Antimicrobial dressings
– Hub• Hand hygiene, glove use• Patency assessment• Safe injection practices• Needleless connector &
hub disinfection• Disinfection caps• Administration set
management• Flush and locking
solutions• Blood sampling • Minimize system
manipulation
2017-02-06
16
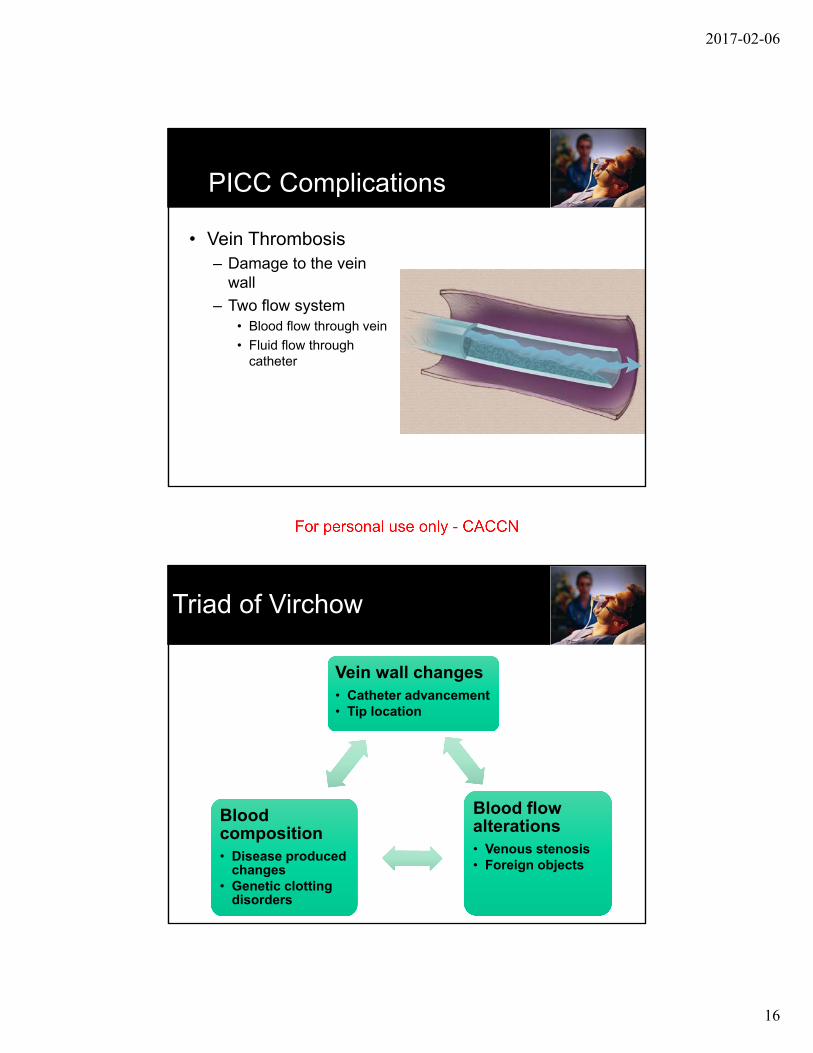
PICC Complications
• Vein Thrombosis– Damage to the vein
wall
– Two flow system• Blood flow through vein
• Fluid flow through catheter
Triad of Virchow
Vein wall changes• Catheter advancement• Tip location
Blood flow alterations• Venous stenosis• Foreign objects
Blood composition• Disease produced
changes• Genetic clotting
disorders
2017-02-06
17
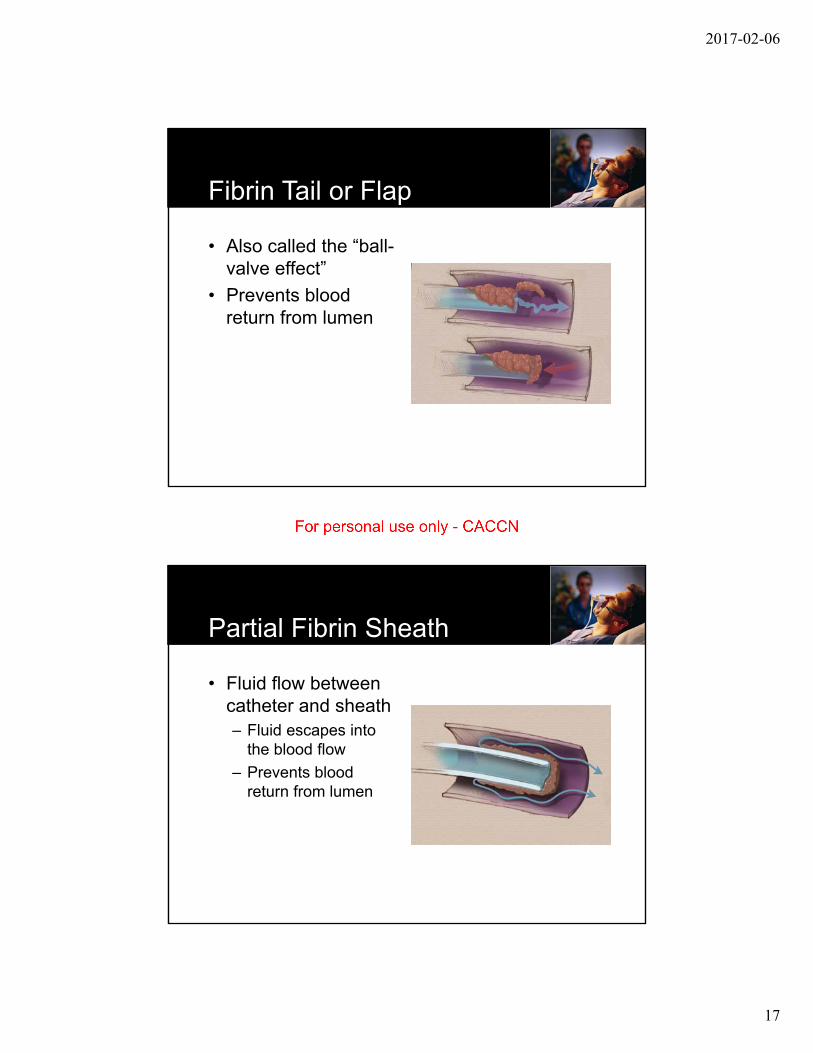
Fibrin Tail or Flap
• Also called the “ball-valve effect”
• Prevents blood return from lumen
Partial Fibrin Sheath
• Fluid flow between catheter and sheath– Fluid escapes into
the blood flow
– Prevents blood return from lumen
2017-02-06
18
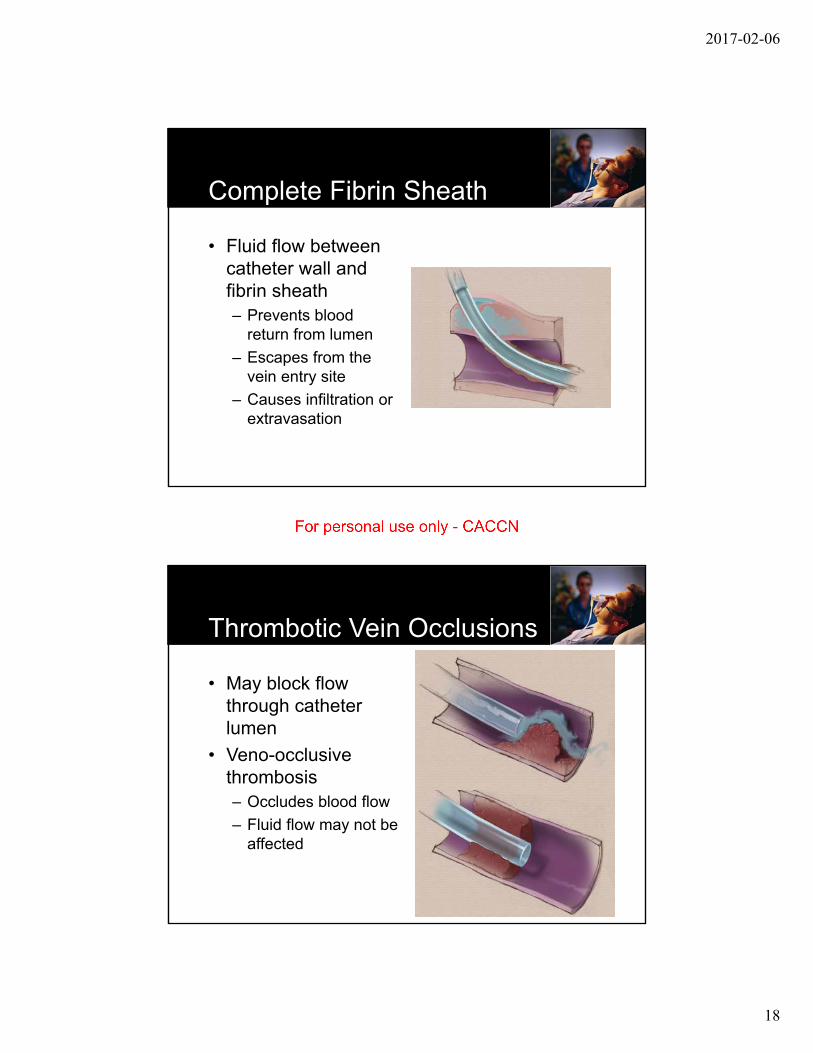
Complete Fibrin Sheath
• Fluid flow between catheter wall and fibrin sheath– Prevents blood
return from lumen
– Escapes from the vein entry site
– Causes infiltration or extravasation
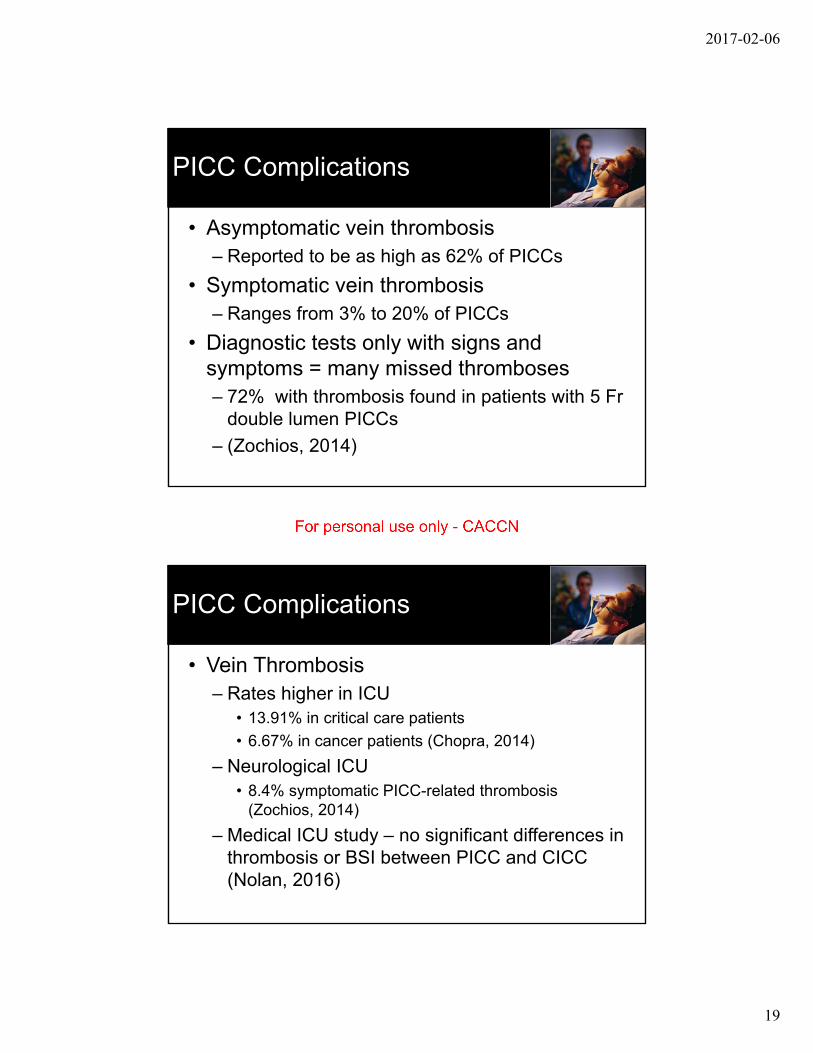
Thrombotic Vein Occlusions
• May block flow through catheter lumen
• Veno-occlusive thrombosis– Occludes blood flow
– Fluid flow may not be affected
2017-02-06
19
PICC Complications
• Asymptomatic vein thrombosis– Reported to be as high as 62% of PICCs
• Symptomatic vein thrombosis– Ranges from 3% to 20% of PICCs
• Diagnostic tests only with signs and symptoms = many missed thromboses– 72% with thrombosis found in patients with 5 Fr
double lumen PICCs
– (Zochios, 2014)
PICC Complications
• Vein Thrombosis– Rates higher in ICU
• 13.91% in critical care patients
• 6.67% in cancer patients (Chopra, 2014)
– Neurological ICU• 8.4% symptomatic PICC-related thrombosis
(Zochios, 2014)
– Medical ICU study – no significant differences in thrombosis or BSI between PICC and CICC (Nolan, 2016)
2017-02-06
20
PICC Complications
• Vein Thrombosis
• Bigger is NOT better with PICCs!– 4 Fr with 0.4% symptomatic thrombosis vs 8.8% with 6
Fr PICCs• Single lumen = 0.6%
• Double lumen = 2.9%
• Triple lumen = 8.8% (Zochios, 2014)
• PICC should consume less than 45% of vein lumen (Sharp, 2013)– 4 Fr PICC requires a minimum vein diameter of 4 cm
PICC Complications
• Pulmonary embolism– Occurs in 1.3% of all PICCs
– 15% of PICCs with symptomatic thrombosis (Zochios, 2014)
• Lower extremity deep vein thrombosis reported in 9/966 PICCs (1%) (Chopra, 2014)

2017-02-06
21
PICC Complications
• Thrombotic Risk factors– Suboptimal tip locations
– Mechanical ventilation• Increases pulmonary coagulopathy leading to
systemic coagulopathy
– Immobility in ICU
– End-stage renal disease
– Sepsis
– Platelet transfusion
– Use of vasopressors (Zochios, 2014)
PICC Complications
• Clinical Signs and Symptoms (Gorski, 2016)– Pain, edema in arm, shoulder, neck or chest
– Erythema in extremity
– Engorged superficial veins of extremity, shoulder, neck or chest
– Difficulty with neck or extremity movement
2017-02-06
22
PICC Complications
• Vein Thrombosis Diagnosis (Gorski, 2016)– Color-flow Doppler ultrasound preferred
• Not invasive, no radiation exposure
– Venography with contrast, CT, or MRI may be needed for viewing veins obscured by clavicle or ribs
PICC Complications
• “Do not remove a CVAD in the presence of CVAD-associated vein thrombosis when the catheter is correctly positioned at the cavoatrial junction, is functioning correctly with a blood return, and has no evidence of any infection. The decision to remove the CVAD should also consider the severity of DVT related symptoms, presence of contraindications for systemic anticoagulation, and the continued need for infusion therapy requiring a CVAD.” – INS VAD Removal Standard 44
• Based on Kearon, 2012
2017-02-06
23
PICC Complications
• Take Away Messages– PICCs are not the best choice for many critical
care patients – Use with caution!
– Use smaller PICCs with fewer lumens• May not be possible with critical care infusion needs
– Careful attention to tip location at or close to cavoatrial junction!
– Rigorously employ ALL infection prevention techniques
Questions
2017-02-06
24
References
• Sharp R, Gordon A, Mikocka-Walus A, et al. Vein measurement by peripherally inserted central catheter nurses using ultrasound: a reliability study. Journal of the Association for Vascular Access. 2013;18(4):234-238.
• Gorski L, Hadaway L, Hagle M, McGoldrick M, Orr M, Doellman D. Infusion Therapy Standards of Practice. Journal of Infusion Nursing. 2016;39(1S):159.
• Chopra V, Flanders SA, Saint S, Woller S, O'Grady NP, N S. The Michigan appropriateness guidel for intravenous catheers (MAGIC). 2015;in press.
• Chopra V, Ratz D, Kuhn L, Lopus T, Lee A, Krein S. Peripherally inserted central catheter‐related deep vein thrombosis: contemporary patterns and predictors. Journal of Thrombosis and Haemostasis. 2014;12(6):847-854.
References
• Chopra V, Anand S, Hickner A, et al. Risk of venous thromboembolism associated with peripherally inserted central catheters: a systematic review and meta-analysis. The Lancet. 2013;382(9889):311-325.
• Chopra V, O'Horo JC, Rogers MA, Maki DG, Safdar N. The risk of bloodstream infection associated with peripherally inserted central catheters compared with central venous catheters in adults: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2013;34(9):908-918.
• Chopra V, Ratz D, Kuhn L, Lopus T, Chenoweth C, Krein S. PICC-associated bloodstream infections: prevalence, patterns, and predictors. Am J Med. 2014;127(4):319-328.
2017-02-06
25
References
• Zochios V, Umar I, Simpson N, Jones N. Peripherally inserted central catheter (PICC)-related thrombosis in critically ill patients. The journal of vascular access. 2014;15(5):329-337.
• Nolan ME, Yadav H, Cawcutt KA, Cartin-Ceba R. Complication rates among peripherally inserted central venous catheters and centrally inserted central catheters in the medical intensive care unit. Journal of critical care. 2016;31(1):238-242.
• Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians evidence-based clinical practice guidelines. CHEST Journal. 2012;141(2_suppl):e419S-e494S.