-
8/20/2019 Pi is 0002934399803544
1/3
BRIEF CLINICAL OBSERVATIONS
Nondilated Obstructive
Uropathy Due to a
Ureteral Calculus
Aaron Spital, MD, Robert Spataro, MD,
Departments of Medicine and Radiology, University of
Rochester School of Medic ine, The Genesee Hospital,
Rochester, New York
U
trasunography has become the standard ap-
proach for investigating suspected urinary tract
obstruction because of its safety and high sensitivity.lJ
However, it is important to understand that ultra-
sonography does not detect obstruction directly, but
rather its usual consequence: dilatation of the renal
collecting system. Unforhmately, urinary tract ob-
struction is not always accompanied by detectable
dilatation36 In these unusual cases of nondilated ob-
structive uropathy, the results of conventional ultra-
sonography will be falsely negative, thereby mislead-
ing the physician and possibly delaying diagnosis and
therapy. Most previously reported cases have been the
result of retroperitoneal or pelvic malignancy or fi-
brosis, or have followed pelvic surgery.56 Here we re-
port a case of nondilated obstructive uropathy caused
by a ureter-al calculus in order to alert physicians to
the possibility that on occasion, even obstruction due
to a urinary stone may be missed by ultrasonography.
While this presentation has been noted previously by
radiologists,5~7-~ it has not been emphasized in the gen-
eral medical literature.
CASE REPORT
A Wyear-old white male was admitted to The
Genesee Hospital with a Z-day history of intermittent
left-sided flank pain radiating to the groin. His past
medical history included mild renal insufficiency
with a baseline serum creatinine of 1.7 mg/dL, an id-
iopathic lupus anticoagulant, multiple deep venous
thromboses of the legs, and pulmonary emboli.
Medications included coumadin, vitamins, and
herbal preparations. On exarntiation the patient was
found to have new hypertension and left-sided ab-
dominal tenderness. Laboratory data revealed a
serum creatinine of 2.5 m@lL and mild microscopic
hematuria. The patient was thought to have renal
colic, although no stone was seen on abdominal
roentgenography.
The following day, a renal ultrasound was obtained
that was completely normal with no evidence of hy-
dronephrosis (Figure IA). Recause of this surpris-
ing finding and the history of a hypercoagulable state,
occlusive vascular causes of renal dysfunction were
sought. A radionuclide renal scan showed decreased
blood f low to the left kidney with minimal excretion
and a normal-appearing right kidney. Selective left
renal arteriography and venography were performed,
but no evidence of vascular obstruction was found.
The patient’s pain persisted and the serum creati-
nine remained elevated at 2.3 mg/dL. Therefore, the
renal ultrasound was repeated 3 days after the initial
study. Again, no hydronephrosis was detected
(Figure 1B). Nonetheless, because of an increasing
index of suspicion for urinary tract obstruction, an
intravenous pyelogram (IVP) was obtained the fol-
lowing day. It showed delayed excretion on the left
side with mild dilatation of the collecting system and
obstruction at t,he left ureteral vesicle junction
(Figure 2).
On the evening fol lowing the IVP, the patient passed
a small stone that was composed of calcium oxalate.
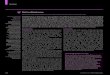
Figure
1A.
First ultrasound of the left
kidney showing no evidence of
hydronephrosis.
May 1995 The American Journal of Medicine@ Volume 98
509
-
8/20/2019 Pi is 0002934399803544
2/3
BRiEF CLlNlCAL OBSERVATIONS
Intravenous pyelography has long been consid-
ered the most valuable study for the evaluation of re-
nal colic.277 However, there are several potential com-
plications of this procedure including allergic
reactions, contrast-induced renal failure, precipita-
tion of renal colic, and the consequences of expo-
sure to ionizing radiation. In contrast, ultrasonogra-
phy of the urinary tract is noninvasive and virtually
risk free. Nloreover, some investigators have found
ultrasonography so reliable in the evaluation of re-
nal colic that they have recommended it (rather than
an IS&‘) as the initial study of choice for the investi-
gation of suspected renal paii~.~,~ However, as the pre-
sent case illustrates, this approach will occasionally
be misleading.
Our patient’s initial renal ultrasound was inter-
preted as being completely normal. Even after the di-
agnosis had been made j a retrospective review of this
study still failed to show any abnormality. The nor-
mal findings on ultrasonography, along with reno-
graphic evidence of unilateral poor function and a his-
tory of hypercoagulability, led the physicians to
perform unnecessary
invasive
procedures to exclude
vascular obstruction as the cause of this patient’s dis-
order. A repeat renal ultrasound several days later
was again norm@ but an IVP clearly showed ob-
struction at the left ureteral vesicle junction.
This unusual presentation of renal calic secondary
to an obstructing
stone
with
no
detectable dilatation
on ultrasonography has been previously alluded to
in the radiological literature.1~G~“8 In most cases, the
reporting physicians concluded that the obstruction
was very recent and proximal dilatation had not yet
had time to occur. However, our case suggests that
.,., ._ ., .,
F@re 13. Second ultrasound o f the left kidney again
show&
no
hydronephrosis.
The next day, the serum creatinine returned to its pre-
vious baseline value of 1.7 mgML. Three weeks later
a repeat radionuclide renal scan was normal
Figure 2. Thirty-minute oblique radiograph from the
intravenous
pyelogram showing blunted fornices with mildly dilated
calyces,
renal pelv is, and proximal ureter of the left kidney,
consistent
with ureterai obstruction. The right side is normal.
there are other causes of nondilatation in obstruc-
tive nephrolithiasis. Our patient had more than 2 full
days of renal colic before his initial normal sono-
graphic study. The process had been present for 5
days at the time of his second study. These results
are even more impressive when one considers that
the degree of obstruction was severe, as evidenced
by the renographic and urographic findings as well
as the elevation in serum creatinine. The explanation
for this remarkable presentation is unknown.
Previously proposed mechanisms include: impaired
peristalsis; for&al rupture with decompression of
the pelvicalyceal system; atypical anatomy of the col-
lecting system (such as a small intrarenal pelvis)
which resists dilatation; and a severely depressed
glomerular filtration rate secondary to underlying re-
nal disease or volume depletion.1~3-5~BJ0
Regardless of the mechanism, the message is clear.
When a patient presents with renal colic and an ob-
structing urinary
stone
is suspected, the physician
should not be dissuaded by negative findings on ul-
tmsonography. In such cases, an IVP should be per-
formed. Indeed, because of the possibility of nondi-
latation and because the IW can
better define the site
510 May 1995 T he American Journal of Medicine@ Volume 98
-
8/20/2019 Pi is 0002934399803544
3/3
BRIEF CLINICAL OBSERVATIONS
and cause of obstruction, many authors still believe
that
the
IVP is the diagnostic procedure of choice in
t.he evaluation of renal colic.‘a”,g In those rare situa-
tions where urography is contraindicated and ultra-
sonography is normal, retrograde and even antegrade
pyelography should be considered.
REFERENCES
1. Cronan JJ. Contemporary concep ts for lmaglng urinary tract
obstruction.
UroiRadiol. 1992;14:8-12.
2. Webb JAW . Ultrasonography In the dlagno sls of renal
obstruction. EIMJ.
1990;301:944-946.
3. Gornish M, Lune Y, Wysenbeek AJ. Nondilated obstructive
uropathy causing
acute renal failure. Isr J Med SC;. 1990;26:50-52.
4. Lyons K, Matthews P, Evans C. Obstructive uropathy without
djlatabon: a
potential dlag nostlc pitfall. BMJ. 1988;296:1517-1518.
5. Malllet PJ, Pelle-Francoz 0, Laville M, et al. NondIlated
obstructive acute
renal failure: diagnos tic procedures and therapeutic
management. Radiology.
1986;160:659-662.
6. Spital A, Valve JR, Segal AJ. Nondilated obstructive
uropathy. Urology.
1988:31:478-482.
7. Erwin BC, Carroll BA, Sommer FG. Renal COIIC: the role of
ultrasound In initial
evaluation. Radiology. 1984;152:147-150.
8. Haddad MC, Sharlf HS , Shahed MS, et al. Renal colic:
dlagnosrs and
outcome. Radiology. 1992;184:83-88.
9. Spencer J, Lindse ll 0, Mastorakou I. Ultrasonography
compared with
Intravenous urography in the investigation of adults with
hematurla. BMJ.
1990;301:1074-1076.
10. Platt JF, RubIn JM, EIIIs JH. Acute renal obstruction:
evaluation with
lntrarenal duplex doppler and conventional US. Radiology.
1993;186:685688.
Manuscript submltted April 20, 1994
and accepted June 22, 1994.
Trousseau’s Syndrome With
Nonbacterial Thrombotic
Endocarditis: Pathogenic
Role of Antiphospholipid
Syndrome
Didier Bessis, MD, Albert Sotto, MD, t @ital
Saint-
E/o;,Montpellier,Jean-Paul Viard, MD, HbpitalNecker,
Paris,Madeleine Bbard, PhD, HdpitalSaint-Louis,
Paris,
Albert-Jean Ciurana, MD,
/ pita/ Saint-E/o;,
Montpellier,
Marie-Claire Boffa, MD, PhD,
&pita/
Saint-Louis, aris,France
N
onbacterial thrombotic endocarditis (NBTE)
with Trousseau’s syndrome is a common mani-
festation of malignant diseases, particularly in lung,
gastrointestinal, and pancreatic adenocarcinomas.’
The pathophysiologic mechanisms of these malig-
nancy-associat.ed thromboses are still
not
clear. We
describe a case of NBTE with Trousseau’s syndrome
in a patient with lung adenocarcinoma. The patient
was positive for antiphosphatidylinositol antibodies
and anti-@ glycoprotzin I (anti-PBGPI) antibodies; to
the best of our knowledge, this combination has
never been reported in this pathology.
CASE REPORT
In
July 1992, a previously healthy 48-year-old white
man
presented with aphasic right palsy that re-
gressed within a fe w minutes. Five days later, he
complained of severe pain in his left calf and apha-
sic left facial palsy. Digital subtraction angiography
of
the
abdominal aorta and lower limbs revealed
em-
bolic obliteration of the left tibioperoneal artery. A
cerebral computed tomographic (CT) scan showed
vascular ischemic in&uy of the right temporal and bi-
lateral occipital lobes and t,he left internal capsule.
The patient was given intravenous heparin for I1
days followed by warfar in. One week later,
he
had a
fever of 38.5”C and complained of cramps in his left
leg. A superficial venous thrombosis was noted in
the
upper left arm. Venography of the lower limbs re-
vealed thromboses of the bilateral popliteal and tib-
ial veins.
On admission to Hepital Saint-Eloi (Montpellier,
France) 1 month later, the physical examination re-
vealed a systolic murmur in the mitral region and
aphasia with confusional syndrome. The white blood
cell count was 16 X log/L with 68% polymorphonu-
clear leukocytes. No thrombopenia or fibrinopenia
was observed. Nine blood cultures were sterile.
Serologic tests for HIV-l and HIV-2, Q fever,
Chlamydia~, Mycoplasma,
and Rmtcellu species were
negative. Venereal Disease Research Laboratory test,
Coombs’ test, rheumatoid factor, antibodies to nu-
clear components and native DNA, and antineu-
trophil cytoplasmic autoantibodies were negative.
Lupus anticoagulant was detected with a pro-
longed partial activated thromboplastin time (49 sec-
onds versus 32 seconds for
the
control), uncorrected
by mixing with normal plasma, and confirmed by
measuring prothrombin time using diluted thrombo-
plastin. The levels of coagulation proteins (factors II,
V, VII, VIII,
IX, X,
XI, XII), antithrombin III, protein
C, and protein S were normal.
Antiphospholipid antibody (aPLA) levels were de-
termined (INSERM U353 and Dr. Pascale Laroche,
Biomedical Diagnostics, Marne-la-Vallke, France)
using
an
enzyme-linked immunosorbent assay
(ELISA) on plates coated with different: phospho-
lipids: cardiolipin,
phosphatidylinositol, phos-
phatidylserine, phosphatidylethanolamine, either
alone or in combination (Table). The aPLA levels
were expressed as GPL or MPL units using a stan-
dard curve obtained with serially diluted selected
positive sera. Ten unit,s, which corresponded to the
97th percentile of the distribution of 100 healthy
blood donors, was arbitrarily chosen as the thresh-
old above which aPLA levels were considered to be
May 1995 The American Journal of Medicinea Volume 98
511