-
Effects of a$xed magnetic appliance on the dentofa/ciaZ
complex
Varun Kalra, BDS, MDS, D. Orth., MS,* Charles J. Burstone, DDS,
MS,** and Ravindra Nanda, BDS, MDS, PhD*** Farmington, Corm.
The purpose of the study was to design and evaluate the effects
of a fixed magnetic appliance that hinged the mandible open and
exerted an intrusive force on the teeth. Ten patients between the
ages of 8 years and 10 years 6 months, with Class II, Division 1
malocclusion associated with mandibular retrusion and increased
lower facial height, were treated with this appliance. The length
of treatment was 4 months, after which the appliance was removed
and the patients were followed up for 4 months. Ten children with
similar age, sex, and dentofacial characteristics acted as controls
and did not receive any appliance therapy. Changes in morphology of
the dentofacial complex were evaluated by use of lateral
cephalograms and study models. In addition temporomandibular joint
and muscle functions were assessed. During treatment mandibular
length increased 3.2 mm, angle of facial convexity decreased 2.8,
the upper and lower teeth intruded an average of 1.5 mm each, and
the mandibular plane angle decreased 1.3. In the follow-up period,
some rebound eruption was noted; however, all other changes were
stable. (AM J ORTHOD DENTOFAC ORTHOP 1989;95:467-78.)
I t has been estimated that two thirds of the patients treated
by orthodontists in the United States have mandibular retrusion
characteristics. Some of these patients also have an increased
lower facial height and large interlabial gap. In such patients
treatment with conventional orthodontic appliances may lead to
Class I occlusion. However, this often does not provide a
satisfactory result in terms of stability and facial es- thetics.
At present the only definitive method of im- proving dentofacial
harmony in these patients is by means of surgical superior
repositioning of the maxilla. This procedure increases the
interocclusal space and allows upward and forward autorotation of
the man- dible, thereby decreasing lower facial height and facial
convexity. Often concomitant with superior reposition- ing of the
maxilla, the mandible also is surgically ad- vanced to further
reduce mandibular retrusion. Recently Dellinger reported on the use
of a magnetic appliance to treat patients with skeletal open bite.
This appliance resulted in intrusion of posterior teeth and an
upward and forward autorotation of the mandible.
There were two hypotheses for this study. (1) If all erupted
teeth in the upper and lower arches could be
From the University 3f Connecticut School of Dental Medicine.
Supported in part by NIH Grant DE-03953-12. *.ksistant Professor.
Department of Orthodontics. **Professor and Chairman. Departmenr of
Orthodontics. ***Professor. Department of Orthcdomics.
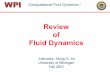
LINGUAL WIRE
Fig. 1. Schematic drawing of appliance.
intruded with an appliance, the mandible would auto- rotate
upward and forward into the interocclusal space created. (2) If
this appliance could displace the condyle downward and forward,
away from the posterior part of the glenoid fossa, stimulation of
condylar growth might occur. Both these effects, an increase in
length of the mandible and an upward and forward autorotation of
the mandible, would be beneficial in treating Class II
malocclusions associated with increased lower facial height and a
retrusive mandible. The objectives of this study therefore were to
(1) design an appliance that hinges the mandible open and exerts an
intrusive force
467
-
466 Kalra, But-stone, and Nanda Am. J. Orrhod. Denrofuc. Orthop.
June 1989
Fig. 2. Occlusal view of appliance.
Table I. Force produced by the appliance
Distance between upper Repelling force and lower splints (mm)
fgm)
0.5 3500 1.0 2640 1.5 2040 2.0 1630 2.5 1315 3.0 1080 3.5 890
4.0 730 4.5 600 5.0 480 6.0 330
appliances were removed and the patients observed for an
additional 4 months. Subjects in the control group were studied for
8 months.
Appliance design
on the teeth and (2) evaluate the effects of this appliance on
the morphology and function of the dentofacial complex.
MATERIALS AND METHODS
The subject pool in the study consisted of 20 boys and girls who
were between the ages of 8 years and 10 years 6 months and who had
Class II, Division 1 malocclusion associated with mandibular
retrusion. The angle of facial convexity, lower facial height, and
interlabial gap were greater than normal. The permanent first
molars and incisors had erupted; the overjet ranged from 6 to 10 mm
and the overbite varied from 0 to 3 mm. The 10 subjects in the
treatment group and the 10 subjects in the control group were
closely matched with regard to age, sex, and dentofacial
characteristics.
The working bite was taken with the mandible in centric relation
and opened 7 to 8 mm in the permanent first molar region. The
appliance consisted of upper and lower acrylic splints that were
bonded on the occlusal halves of the permanent first molars,
deciduous molars or premolars, and canines (Figs. 1 through 3).
Samar- ium cobalt magnets measuring 20 X 8 x 2 mm were encased in a
stainless steel case 0.007-inch thick and embedded into the upper
and lower acrylic splints in a repelling mode. In addition a
0.028-inch wire was embedded in the acrylic. This wire rested on
the lingual surfaces of the four permanent incisors and was indi-
vidually bonded to them; thereby intrusive forces were transmitted
to the entire arch. The size and shape of the magnets were designed
in collaboration with Re- coma Inc.* The steel cases were
fabricated in coop- eration with the Bioengineering Department,
University of Connecticut Health Center. The forces produced by the
appliance are listed in Table I.
Cephalometric analysis
Changes in craniofacial morphology caused by growth and
treatment were determined from a set of lateral cephalometric head
films. A set consisted of two cephalograms, one taken with the
mandible in centric relation and the other with the mouth wide open
to
The active treatment time was 4 months, after which *Recoma
Inc., Fairfield, N.J.
-
Vo/ume 9s Numhrr 6
Fig. 3. Buccal view of appliance.
facilitate visualization of the condyles. For each patient in
the treatment group, the first set of head films was taken before
treatment, the second set of films after 4 months active treatment,
and the third set 4 months posttreatment. In the control group, an
initial set and a final set of cephalograms were taken 8 months
apart. Changes between the two sets of films in the control group
were divided by two to obtain changes throughout a 4-month period.
Subsequent cephalograms were su- perimposed on the anterior cranial
base of the previous cephalogram as described by Baumrind, Miller,
and Molthen. Vertical and horizontal positional changes of certain
landmarks were measured in relation to two Cartesian coordinate
systems. In the first system, the originally constructed Frankfort
horizontal (FH) plane (constructed by subtracting 7 from the
sella-nasion line) served as the X axis and a line perpendicular to
it through sella served as the Y axis. In the second system, the
original natural occlusal plane formed the X axis and a line
perpendicular to it through sella formed the Y axis. The two
coordinate systems were transferred from the first tracing to the
next. In addition certain other linear and angular measurements
were as- sessed (Figs. 4 through 6). Separate maxillary and man-
dibular tracings were superimposed3 to determine changes in the
position of the teeth within the maxilla and the mandible. Changes
in the position of the teeth were measured in relation to the
original occlusal plane (X axis) and a line perpendicular to it
through sella (Y axis). The length of the mandible, condylion-
prognathion (Co-Pgn), was measured from the open mouth
cephalogram.
J cos co* COP
N FH
Fig. 4. Cephalometric landmarks and linear measurements used in
the study. (1) N-ANS, Upper anterior facial height mea- sured
perpendicular to Frankfort horizontal (FH) plane. (2) ANS- Me,
Lower anterior facial height measured perpendicular to FH plane.
(3) A-El to occlusal plane. (4) Condylion-pogonion (Co- Pg), Length
of mandible parallel to FH plane. (5) Co-Go, Pos- terior facial
height measured perpendicular to FH plane.
Assessment of temporomandibular joint and muscle function
An assessment of the function of the masticatory system was
conducted to ascertain the status of any signs and symptoms of
dysfunction that were present or that might develop. The assessment
was based on a
-
470 Kalra, Burstone, and Nanda Am. J. Orthod. Dentofac. Orthop.
June 1989
Fig. 5. Mandibular length, condylion-prognathion (Co-Pgn),
measured from wide open mouth cephalogram.
clinical dysfunction examination and on anamnestic dysfunction
as described by Helkimo.4
For the treatment group, assessments were made at the following
time intervals: before treatment, 3 days after insertion of
appliance, 3 months after insertion of appliance, on removal of
appliance, and 4 months post- treatment. For the control group,
assessments were made at the start of the examination period and 8
months later.
Results of the cephalometric and study model analyses were
statistically analyzed. To assess the significance of differences
between the treatment and control groups, mean and standard
deviation were calculated and Students t tests were performed. The
null hypothesis was rejected at the 0.05% level of confidence.
The size of the combined error in locating, super- imposing, and
measuring the changes in different land- marks was calculated with
the following. formula:
J Zd2 SE measurement = - 2n The combined standard error did not
exceed 0.6 mm in the horizontal and vertical dimensions.
RESULTS
The effects of the magnetic appliance during treat- ment and
during the follow-up period are given in Tables II and III.
Mandible
During treatment the length of the mandible,
condylion-prognathion (Co-Pgn) , increased 3.2 mm as compared with
0.8 mm in the control group (p < 0.001). In the follow-up
period, no difference was seen in growth rates of the treatment and
control groups (Fig. 7).
Fig. 6. Angular measurements used in the study. (6) 1 to-FH
plane. (7) Y axis. (8) N-A-Pg, Angle of facial convexity. (9) 1 to
mandibular plane. (10) FH-MP, Mandibular plane angle.
In the treatment group, the mandible autorotated upward and
forward as judged by the mandibular plane angle and Y axis. The
mandibular plane angle decreased 1.3 and 0.3; the Y axis decreased
1.1 and 0.3 in the treatment and follow-up periods, respectively.
These changes were small but statistically significant.
Overall facial form
Downward and forward displacement of2 the max- illa, as
represented by anterior nasal spine and point A, did not show any
significant differences between the treated and control groups.
There was a significant decrease in the angle of facial
convexity (p < 0.001) (Fig. 8) and improvement in the
relationship of A-B to occlusal plane (p < 0.001) (Fig. 9).
Even though the mandible autorotated upward and forward,
increased mandibular growth was responsible for an increase in
anterior (ANS-Me) and posterior (Co- Go) facial heights (p <
0.001). Fig. 10 shows the change in overall facial form in the
treatment group as compared with the control group.
Dentition
During treatment the upper and lower incisors in- truded
approximately 1.3 mm each and the molars 1.6 mm each. During this
period, in the control group, these teeth erupted 0.3 and 0.4 mm,
respectively (Fig. 11). In the follow-up period, the posterior
teeth reerupted until they achieved occlusal contact with their
antago- nists (Fig. 12). However, overall the lower incisor
-
Volume 95 Number 6
ESfects of fired magnetic appliance on dentofacial complex
471
Table II. Comparison of changes between treatment and control
groups during treatment period
Measurements
Treatment p-oup Control group (N = IO) (N = IO)
Mean SD Mean SD Mean
difference p value
Mandible Length
Co-Pgn (mm) Co-Pg parallel to FH (mm)
Displacement in relation to FH Pg horizontal (mm) Pg vertical
(mm)
Rotation MP-FH () Y axis ()
Maxilla Displacement in relation to FH
Point A horizontal (mm) Point A vertical (mm) ANS horizontal
(mm) ANS ven:ical (mm)
Facial height ANS-Me perpendicular to FH (mm) Co-Go
perpendicular to FH (mm)
Facial convex,@ N-A.-Pg () A-B perpendicular to OP (mm)
Dentitinn Overjet (mm) Overbite (mm) Molar relation (mm)* Upper
incisor to FH () Lower incisor to MP ()
+3.2 0.5 +2.1 0.6
+0.8 0.2 2.4 1-0.5 0.2 1.6
< 0.001 < 0.001
+2.6 + 1.9
+0.5 +0.5
< 0.001 < 0.01
0.9 I.1
0.2 0.3
2.1 1.4
- 1.3 - 1.1
0.8 0.5
0.2 0.1
1.3 1.1
< 0.001 < 0.001
0 0
+0.5 +0.3 +0.5 +0.2
0.2 0.2 0.3 0.2
+0.4 +0.2 +0.4 +0.2
0.3 0.2 0.2 0.3
0.1 NS 0.1 NS 0.1 NS 0 NS
+ 1.8 1.1 +2.6 0.9
+0.4 0.2 +0.6 0.2
1.4 2.0
i 0.01 < 0.001
-2.8 0.9 +2.3 0.9
-0.1 +0.1
0.1 0.1
2.7 2.2
< 0.001 < 0.001
-2.1 0.7 -3.8 0.9 +2.0 0.8 +0.2 0.6 -0.1 0.7
-0.1 0.2 +0.1 0.2 -0.1 0.1 +0.2 0.5 +0.1 0.6
2.0 < 0.001 3.9 < 0.001 2.1 < 0.001 0 NS 0.2 NS
Changes in tooth position within the maxilla and mandible
(measured from maxillary and mandibular su- perimposition
tracings)** Vertical displacement
Upper molar (mm) - 1.6 0.3 +0.2 0.1 1.8 < 0.001 Lower molar
(mm) + 1.6 0.3 -0.3 0.2 1.9 < 0.001 Upper incisor (mm) - 1.4 0.4
+0.4 0.3 1.8 < 0.001 Lower incisor (mm) + 1.2 0.2 -0.3 0.1 1.5
< 0.001
Horizontal displacement Upper molar (mm) +0.1 0.4 +0.1 0.2 0 NS
Lower mlolar (mm) +0.2 0.2 0 0.3 0.2 NS Upper incisor (mm) 0 0.4
+0.1 0.1 0.1 NS Lower incisor (mm) 0 0.5 0 0.3 0 NS
+ Denotes downward or forward displacement of landmark. -
Denotes upward or backward displacement of landmark. * + Denotes
imprcvement of molar relationship toward Class I. **The maxilla was
superimposed on the hard palate and the anterior maxillary
structures with main consideration being given to the region
between point A ar,d the anterior nasal spine with the images of
the superior surfaces of the hard palate aligned. The mandible was
superimposed on the inner tables of the symphysis and the line of
distal extension of the mandible.
(p < O.OOl), upper incisor (p < O.Ol), and upper mo- lar
(p < 0.05) showed less eruption in the treated group than in the
control group as seen in Table IV and Fig. 13.
In the treatment period, the overjet was reduced 2.1
mm and the molar relationship improved 2.0 mm to- ward Class I
occlusion as a result of increased forward displacement of the
mandible in relation to the maxilla; this remained unchanged during
the follow-up period.
Magnets used in the repelling mode produce lateral
-
472 Kalra, Burstone, and Nanda Am. J. Orthod. Dentofac. Orthop.
June 1989
Tabie III. Comparison of changes between treatment and control
groups during follow-up period
Measurements
Treatment group (N = 10)
Mean SD
Control group (N = 10)
Mean SD Mean
difference p value
Length Co-Pgn (mm) Co-Pg parallel to FH (mm)
Displacement in relation to FH Pg horizontal (mm) Pg vertical
(mm)
Rotation MP-FH () Y axis ()
Maxilla
+0.7 +os
0.2 0.3
+0.6 0.2 +0.4 0.2
-0.4 -0.3
0.2 0.2
Displacement in relation to FH Point A horizontal (mm) Point A
vertical (mm) ANS horizontal (mm) ANS vertical (mm)
Facial height ANS-Me perpendicular to FH (mm) Co-Go
perpendicular to FH (mm)
Facial convexity N-A-Pg () A-B perpendicular to OP (mm)
Dentition
+0.3 +0.4 +0.4 +0.2
0.2 0.4 0.2 0.3
+0.2 +0.5
0.2 0.2
-0.3 +0.3
0.2 0.2
Overjet (mm) 0 0.3 Overbite (mm) +2.8 0.4 Molar relation (mm)*
+0.1 0.2 Upper incisor to FH () +0.4 0.6 Lower incisor to MP ()
-0.4 0.5
i-O.8 0.2 +0.5 0.2
0.1 NS 0 NS
+0.5 +0.5
0.2 0.3
0.1 NS 0.1 NS
0 0
0.2 0.1
0.4 0.3
< 0.05 < 0.05
+0.4 +0.2 +0.4 +0.2
0.3 0.2 0.2 0.3
0.1 NS 0.2 NS 0 NS 0 NS
to.4 0.2 +0.6 0.2
0.2 NS 0.1 NS
0.1 0.1
-0.1 +0.1
0.2 0.2
< 0.05 < 0.05
-0.1 0.2 +0.1 0.2 -0.1 0.1 +0.2 0.5 to.1 0.6
0.1 NS 2.1 < 0.001 0.2 NS 0.2 NS 0.5 NS
Changes in tooth position within the maxilla and mandible
(measured from maxillary and mandibular su- perimposition
tracings)** Vertical displacement
Upper molar (mm) Lower molar (mm) Upper incisor (mm) Lower
incisor (mm)
Horizontal displacement Upper molar (mm) Lower molar (mm) Upper
incisor (mm) Lower incisor (mm)
+ 1.8 0.4 -2.1 0.5 +1.4 0.5 - 1.4 0.3
+0.2 0.1 1.6 -0.3 0.2 1.8 +0.4 0.3 1.0 -0.3 0.1 1.1
< 0.001 < 0.001 < O.ctOl < 0.001
+0.1 +0.2 +0.2 -0.1
0.4 0.3 0.2 0.4
+0.1 0
+0.1 0
0.2 0.3 0.1 0.3
0 NS 0.2 NS 0.1 NS 0.1 NS
+ Denotes downward or forward displacement of landmark. -
Denotes upward or backward displacement of landmark. * + Denotes
improvement of molar relationship to Class I. **The maxilla was
superimposed on the hard palate and the anterior maxillary
structures with main consideration given to the region between
point A and the anterior nasal spine with the images of the
superior surface of the hard palate aligned. The mandible was
superimposed on the inner tables of the symphysis and the line of
distal extension of the mandible.
forces as they are moved toward each other. This re- stilted in
buccolingual tipping of the teeth in the pos-, terior segments. It
was found that in centric relation, seven patients had a molar
crossbite on one side and
an increased buccal overjet on the other side. However, during
the follow-up period, the teeth uprighted to their original
inclinations, thereby correcting the cross- bite on one side and
the increased buccal overjet on
-
Volume 95
Number 6 EfJects of,fixed magnetic appliance on dentofacial
complex 473
Co-Pgn H Treatment Group q Control Group
(MM) 0
1 Treatment Period Follow-up Perlod
Fig. 7. Change in mandibular length (Co-Pgn).
the other side. The intermolar width remained un- changed.
Function
None of the patients in the treatment or control groups
complained of difficulty in opening the mouth maximally, of
stiffness of jaws, locking, luxation or pain on movement of the
mandible, pain in the region of the temporomandibular joint, or
pain of the masti- catory musculature during any stage of the
study. Sim- ilarly clinical examination of the muscles of
mastication and temporomandibular joint function showed that pa-
tients in the treatment group did not experience any discomfort,
pain, or temporomandibular joint dysfunc- tion at any stage of
treatment.
The appliance was accepted extremely well by the children and,
apart from initial awkwardness, none complained of discomfort nor
difficulty in speech and eating. Patients used a fluoride rinse
daily and main- tained good oral hygiene; as a result neither
caries nor decalcification was noted during treatment.
DISCUSSION
The two most important findings in the study were that the
length of the mandible increased significantly in the treated group
and the entire upper and lower arches intruded during
treatment.
In 4 months of treatment, the length of the mandible in the
treated group increased 3.2 mm as compared with 0.8 mm in the
control group. The specially con- structed magnetic appliance held
the mouth open 7 to
8 mm in the first molar region when the upper and lower splints
were in contact, and 10 to 11 mm open when the mandible was in the
acquired rest position. This caused the condylar heads to rotate
and translate forward, away from the posterior aspect of the
glenoid fossa. A number of researchers5-7 have shown increased
condylar growth in animal studies with appliances that caused
protraction or hyperpropulsion of the condyles. Reports on the use
of functional appliances, either a form of activator or the Frankel
FR, present contradic- tory results. Some studies*-* show increase
in man- dibular growth; others22-28 find that mandibular growth is
not increased with the use of either type of appliance. Conflicting
results with the use of removable functional appliances could be
attributed to the fact that they are dependent on patient
cooperation and clinical expertise and at best are worn only part
of the day.
It is possible that in growing persons there is stim- ulation of
condylar growth when the condyles are pro- tracted by the
functional appliance, but this ceases when the appliance is removed
from the mouth. All ani- ma15- and human studies29-33 that use
fixed splint-like devices to hold the mandible forward 24 hours a
day show an increase in mandibular growth. It could be that the
determining factor is the amount of time the appli- ance is worn
each day. Moss and Salentijn34 claim that growth at the condyle
appears to take place as a sec- ondary phenomenon to fill the space
left by the man- dible as it is displaced forward by the tissues
around it. Enlow also reports condylar growth to be of a
compensatory nature rather than a primary process.
-
474 Kalra, Burstone, and Nanda Am. J. Orthod. Dentofac. Orthop.
June 1989
N-A-Pg q Treatment Group b9 Control Group
-4' Treatment Period Follow-up Period
Fig. 8. Change in the angle of facial convexity (N-A-Pg).
A-B (OP) S Treatment Group RI Control Group
MN 0
-1' Treatment Period Follow-up Period
Fig. 9. Change in the relationship of A-B to occlusal plane.
Petrovi? and McNamara, Connelly, and McBride12 at- tributed
increased condylar growth to increased activity in the lateral
pterygoid muscles. Later studies3-7 in- dicated that the effect of
the lateral pterygoid muscles may be mediated to the condyles via
the stretch of the posterior portion of the capsule, the
meniscotemporal ligament as the condyles come forward. Whetten and
JohnstonJ6 have shown that severing the lateral ptery- goid msucle
did not affect growth of the condyle on the affected side. Recently
McNamara and Carlson noted that the adaptive changes in the
temporomandib-
ular region may be caused by alteration in the biome- chanical
or biophysical environment of the joint that may be produced by
muscular or nonmuscular forces. With the magnetic appliance in the
mouth, the condyles moved down the articular slope about 10 mm away
from the posterior aspect of the glenoid fossa. This could cause
articular tissue strain with increased con- dylar growth as a
fill-in process. However, the present state of knowledge precludes
a definite answer to the mechanism of increased condylar
growth.
After removal of the appliances, the rate of growth
-
V&me 95 Number 6
Ejfects ofjked magnetic appliance on dentofacial comple?r
475
_ , , u :
q R I : ! , i ,-- I Y. I , , =._ .* I , , I ,I I -._* a. / ,,;,
;;
v
--.* ,/ . *. *..* : : -*. : : a a......, Fig. 10. Composite
tracing of lateral cephalograms showing the mean differences in
dentofacial form between the treatment and control groups.
Differences between the two groups are inter- preted as changes
caused by treatment. -, Pretreatment; - - -, 4 months
posttreatment. The lateral cephalogram was superimposed on the
anatomic structures of the floor of the anterior cranial fossa with
primary consideration given to the region between the anterior
clinoid process and crista galli.
of the mandible was found to be similar to that in the control
group. Petrovic3 and McNamara3 have re- ported a decrea.sed amount
of growth for a period fol- lowing removal of hyper-propulsion
appliances in an- imals. However, human studies29-33 with the
Herbst ap- pliance have shown normal mandibular growth after
removal of the appliance. The results of this study con- cur with
those of the latter.
It was decided to use magnets to provide the intru- sive force
on the teeth since any other form of me- chanical device would
either interfere with function or not provide such an efficient
system. The size and shape of the magnets were dictated by space
available in the mouth, patient comfort, and the force that they
could generate. Samarium cobalt magnets were chosen since they have
an excellent ratio of magnetic force to size.3g4 In addition they
are far superior in resisting loss of magnetic energy with time and
are safe to use in the mouth.394 However, samarium cobalt is
suscep- tible to corrosion in the oral environment39; therefore
Fig. 11. Composite of maxillary and mandibular superimposition
tracings showing the mean differences in the position of the teeth
between the treatment and control groups during the treat- ment
period. Differences between the two groups are inter- preted as
changes caused by treatment. -, Pretreatment; - - -, posttreatment.
The maxilla was superimposed on the hard palate and the anterior
maxillary structures with main considera- tion given to the region
between point A and the anterior nasal spine with the images of the
superior surfaces of the hard palate aligned. The mandible was
superimposed on the inner tables of the symphysis and the line of
distal extension of the mandible.
the magnets were encased in a stainless steel case and embedded
in the acrylic splints so that they were not exposed to the oral
environment.
With the appliance in the mouth, the subject tended to maintain
an interocclusal space of about 3.0 mm between the upper and lower
splints. At this distance the magnets produce a repelling force of
1080 gm, thereby subjecting each tooth in the arch to an intrusive
force of approximately 90 gm. Burstone recommends an intrusive
force of 20 gm for incisors. Dellingep3 showed that a force of 100
gm was adequate to intrude premolars in dogs. However, an optimum
force value has not been established for intrusion of posterior
teeth or large segments of teeth. Since some of the teeth covered
by the appliance had large root surfaces, a force in the range of
90 gm per tooth was considered ade- quate, though perhaps
excessive, for intrusion. More research is needed in this area to
determine an optimum intrusive force.
In a repelling mode, when the magnets are moved toward each
other, lateral forces are generated. In most patients this caused
the mandible to deviate about 2 mm to one side in the acquired rest
position. This shearing force generally caused both upper buccal
segments to be tipped to the right side of the patient and both
lower buccal segments to be tipped to the left side. This re-
-
476 Kalra, Burstone, and Nanda Am. J. Orthod. Dentofac. Orthop.
June 1989
Fig. 12. Composite of maxillary and mandibular superimposition
tracings showing the mean difference in the position of the teeth
between the treatment and control groups during the follow-up
period. Differences between the two groups are interpreted as the
amount of relapse. -, Posttreatment; - - -, 4 months post-
treatment. The maxilla was superimposed on the hard palate and the
anterior maxillary structures with main consideration given to the
region between point A and the anterior nasal spine with the images
of the superior surfaces of the hard palate aligned. The mandible
was superimposed on the inner tables of the symphysis and the line
of distal extension of the mandible.
Fig. 13. Composite of maxillary and mandibular superimposition
tracings showing the mean differences in the position of the teeth
between the treatment and control groups during treat- ment plus
follow-up. Differences between the two groups are interpreted as
overall additional change in the treated group. -, Pretreatment; -
- -, 4 months posttreatment. The maxilla was superimposed on the
hard palate and the anterior maxillary structures with main
consideration given to the region between point A and the anterior
nasal spine with the images of the superior surfaces of the hard
palate aligned. The mandible was superimposed on the inner tables
of the symphysis and the line of distal extension of the
mandible.
Table IV. Comparison of changes in tooth position between
treatment and control groups during treatment plus follow-up
(measured from maxillary and mandibular superimposition
tracings)*
Treatment group Control group (N = IO) (N = 10)
Mean Measurements Mean SD Mean SD difference p value
Dent&ion Vertical displacement
Upper molar (mm) +0.2 0.2 +0.4 0.2 0.2
-
Volume 95 Number 6
.Effects of @fixed magnetic appliance on dentqfizcial complex
477
segments in the lower tipped to the other side, there were no
significant changes in the upper and lower intermolar arch widths.
In an effort to minimize or prevent the occurrence of crossbites,
it is proposed that the amount of repelling force produced by the
magnets be reduced, thereby also reducing the lateral forces
generated. If buccal crossbites still occurred, they would be mild
in nattire and self-correcting once the appliance was removed.
Treatment with the magnetic appliance is followed by a phase of
fixed appliance treatment to correct dental relationships;
therefore cor- rection of any buccolingual tipping, were it to
remain, could readily be achieved at this stage.
On removal of appliances, it was noticed that since the teeth
had intruded, occlusion occurred only on the gum pads covering the
unerupted second molars, leav- ing the posterior teeth about 4.0 mm
out of occlusion. In retrospect examination of pretreatment study
models and x-ray films showed that even though the upper and lower
second molars were not close to eruption, the clearance between the
soft tissues of the upper and lower pads averaged only about 1.0
mm. When the appliances were removed, upward and forward a&o-
rotation of the mandible was limited by the gap between these
pads.
Autorotation of the mandible occurs when the free- way space is
increased after surgical superior reposi- tioning of the maxilla.A7
In such instances the man- dible acquires a new rest position,
which appears sta- b1e.4s-47 [t could therefore be assumed that if
the gum pads had not caused obstruction, the mandible would have
autorotated further and acquired a new, potentially stable rest
position. Dellinge? reported on cases in which intrusion of
posterior teeth had been achieved with the use of an Active
Magnetic Vertical Corrector. He found that both intrusion of teeth
and the ensuing autorotation of the mandible were stable 3 years
later. In this study the teeth were prevented from achieving
occlusal contact, resulting in reeruption until full oc- clusion of
the posterior teeth was obtained. Neverthe- less, throughout the
entire treatment and follow-up pe- riod, the teeth in the treated
group underwent statisti- cally significant intrusion as compared
with the control group. The limited autorotation of the mandible
that was achieved was stable. In fact during the follow-up period,
the mandible autorotated further. The appliance may have caused
mild inflammation of the soft tissues distal to the first molars;
once the appliances were re- moved, the inflammation gradually
subsided and this allowed the mlandible to close a littler further.
Since the slight intrusion and autorotation achieved were both
stable, it can be hypothesized that if the gum pads had not
prevented further autorotation, the enhanced auto-
rotation achieved would also have remained stable and the teeth
would not have reerupted to the extent they did. In the future it
is proposed that removal of the tissue overlying the upper and/or
lower second molars about a week before removal of appliances would
be beneficial. This would allow autorotation of the man- dible as
determined by the amount of intrusion.
CONCLUSIONS
A fixed magnetic appliance was designed that hinged the mandible
open and exerted an intrusive force on the teeth. Treatment with
this appliance resulted in:
1. An increase in length of the mandible 2. Intrusion of teeth
3. Upward and forward autorotation of the man-
dible 4. Reduction of A-B to occlusal plane 5. Improvement in
the angle of facial convexity 6. Creation of temporary buccal
crossbite caused
by the shearing force of repelling magnets During follow-up
there was some rebound eruption
of teeth; however, all other changes were stable. This appliance
presents a promising mode of im-
proving facial harmony in patients with Class II, Di- vision 1
malocclusion associated with mandibular re- trusion, increased
lower facial height, and increased interlabial gap. In addition
reduction in overjet and improvement in molar relationship toward
Class I oc- clusion make the second stage of conventional ortho-
dontic treatment less demanding. Further research and development
of the appliance are advocated.
REFERENCES I.
2.
3.
4.
5.
6.
Graber TM. Orthodontics: principles and practice. 3rd ed. Phil-
adelphia: WB Saunders Company, 1972:205. Dellinger EL. A clinical
assessment of the Active Vertical Cor- rector-a nonsurgical
alternative for skeletal open bite treat- ment. AM J ORTHOD
1986;89:428-36. Baumrind S, Miller D, Molthen R. The reliability of
head film measurements. 3. Tracing superimposition. AM J ORTHOD
1976; 70:617-44. Helkimo M. Studies on function and dysfunction of
the masti- catory system. II. Index for anamnestic and clinical
dysfunction and occlusal state. Sven Tandlak Tidskr 1974:67: 101-Z
1. Petrovic A, Stutzmann J, Oudet C. Control processes in the
postnatal growth of the mandibular condylar cartilage. In: McNamara
JA Jr, ed. Determinants of mandibular form and growth. Ann Arbor,
1975. Center for Human Growth and De- velopment. University of
Michigan. Stockli PW, Willert HG. Tissue reactions in the
temporoman- dibular joints resulting from anterior displacement of
the man- dible in the monkey. AM J ORTHOD 1971:60:142-55.
7. Baume LJ, Derichsweiler H. Is the condylar growth center re-
sponsive to orthodontic therapy? An experimental study in Ma- caca
mulatta. Oral Surg Oral Med Oral Path01 1961;14: 1371.
8. Petrovic A, Stutzmann JJ, Gasson N. The final length of the
mandible: Is it genetically predetermined? In: Carlson DS, ed.
-
478 Kalra, Burstone, and Nanda
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
Craniofacial biology. Monograph 10, Craniofacial Growth Se-
ries. Ann. Arbor: 1981. Center for Human Growth and Devel- opment,
University of Michigan. McNamara JA Jr, Hinton RJ, Hoffman DL.
Histologic analysis of temporomandibular joint adaptations to
protrusive function in young adult rhesus monkeys (Macaca mulatta).
AM J ORTHOD 1982;82:288-98. Charlier JP, Petrovic A,
Herrmann-Stutzmann J. Effects of man- dibular hyperpropulsion on
the prechondroblastic zone of young rat condyle. AM J ORTHOD
1969;55:71-4. Graber TM, Rakosi T, Petrovic AG. Dentofacial
orthopedics with functional appliances. St. Louis: The CV Mosby
Company, 1985.. McNamara JA Jr, Connelly T, McBride MC.
Histological studies of temporomandibular joint adaptations. In:
McNamara JA Jr, ed. Determinants of mandibular form and growth. Ann
Arbor: 1975. Center for Human Growth and Development, University of
Michigan. Petrovic AG, Stutzmann JJ. Further investigation into the
func- tioning of the peripheral comparator of the servosystem (re-
spective positions of the upper and lower dental arches) in the
control of the condyle cartilage growth rate and of the lengthening
of the jaw. In: McNamara JA Jr, ed. The biology of occlusal
development. Ann Arbor: 1977. Center for Human Gmwth and
Development, University of Michigan. Petrovic A, Stutzmann J.
Tierexperimentelle Untersuchungen uber das Gasichtsschadelwachstum
and seine Beeinflunssung: eine biologische Erklarung der
songenannte Wachstumsrotation des Unterkiefers. Fortscbr
Kieferorthop 1979;40: 1. McNamara JA Jr, Carlson DS. Quantitative
analysis of tempo- romandibular joint adaptations to protrusive
function. AM J ORTHOD 1979;76:593-611. Petrovic A. An experimental
and cybernetic approach to the mechanism of action of functional
appliances on the mandibular growth. In: McNamara JA Jr, ed.
Malocclusion and the peri- odontium. Monograph 15, Craniofacial
Growth Series. Ann Ar- bor: 1984. Center for Human Growth and
Development, Uni- versity of Michigan. Petrovic AG, Stutzmann JJ,
Lavergne J. Effects of functional appliances on the mandibular
condylar cartilages. In: Graber TM, ed. Physiologic principles of
functional appliances. St. Louis: The CV Mosby Company, 1985.
McNamara JA Jr, Bookstein FL, Shaughnessy TG. Skeletal and dental
changes following function regulator therapy on Class II patients.
AM J ORTHOD 1985;88:91-110. Marschner JF, Harris JE. Mandibular
growth and Class II treat- ment. Angle Orthod 1966;36:89-93.
Friinkel R, Reiss W. Zur Problematik der Unterkiefermach-
entwicklung bei Distalbissfallen. Forts&r Kieferorthop 1970;
31:345-55. Righellis EG. Treatment effects of Fr&kel activator
and extraoral traction appliances. Angle Orthod 198353: 107-21.
Bjijrk A. ,The principle of the Andresen method of orthodontic
treatment, a discussion based on cephalometric x-ray analysis of
treated cases. AM J ORTHOD 1951;37:437-58. Jakobsson SO.
Cephalometric evaluation of the treatment effect on Class II,
Division 1 malocclusions. AM J ORTHOD 1967; 53446-7. Harvold EP,
Vargervik K. Morphogenic response to activator treatment. AM J
ORTHOD 1971;60:478-90. Ahlgren J. Late results of
activator-treatment: a cephalometric study. Br J Orthod
1976;3:181-7.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
Am. J. Orthod. Dentofac. Orthop. June 1989
Schulhof RJ, Engel GA. Results of Class II functional appliance
treatment. J Clin Orthod 1982;16:587-99. Creekmore TD, Radney ,LJ.
Fr%nkel appliance therapy: ortho- pedic or orthodontic? AM J ORTHOD
1983;83:89-108. Robertson NRE. An examination of treatment changes
in chil- dren treated with the function regulator of Frlnkel. AM J
ORTHOD 1983;83:229-310. Pancherz H. Treatment of Class I
malocclusions by jumping the bite with the Herbst appliance: a
cephalometric investigation. AM J ORTHOD 1979;76:423-41. Pancherz
H. The effect of continuous bite jumping on the den- tofacial
complex: a follow-up study after Herbst appliance treat- ment of
Class II malocclusions. Eur J Orthod 1981;3:49-60. Pancherz H. The
mechanism of Class II correction in Herbst appliance treatment. A
cephalometric investigation. AM J ORTHOD 1982;82:104-13. Wieslander
L. Intensive treatment of severe Class II malocclu- sions with a
headgear-Herbst appliance in the early mixed den- tition. AM J
ORTHOD 1984;86:1-13. Kalra V, Be&man M, Sachdeva R, Nanda R.
Effects of anterior repositioning of the mandible on the
dentofacial complex. J Dent Res 1985;64:344. Moss ML, Salentijn L.
The capsular matrix. AM J ORTHOD 1969;56:474-90. Enlow DM. Handbook
of facial growth. Philadelphia: WB Saun- ders Company, 1982:122-3.
Whetten LL, Johnston LE Jr. The control of condylar growth: an
experimental evaluation of the role of the lateral pterygoid
muscle. AM J ORTHOD 1985;88:181-90. Petrovic A. Control of
postnatal growth of secondary cartilages of the mandible by
mechanisms regulating occlusion: cybernetic model. Trans Eur Orthod
Sot 197469-75. McNamara JA Jr. Functional adaptations in the
temporoman- dibular joint. Dent Clin North Am 1975;19:457-71.
Tsutsui H, Konouchi Y, Sasaki H, Shiota M, Ushita T: Studies on the
SmCo magnet as a dental material. J Dent Res 1977;58:1597-1606.
Blechman AM. Magnetic force system in orthodontics. AM J ORTHOD
1985;87:201-10. Blechman AM, Smiley M. Magnetic forces in
orthodontics. AM J ORTHOD 1978;74:435-43. Burstone CJ. Deep
overbite correction by intrusion. AM J ORTHOD 1977;72:1-22.
Dellinger EL. A histologic and cephalometric investigation of
premolar intrusion in the Macaca speciosa monkey. AM J ORTHOD
1967;53:325-54. Bell WH, Creekmom TD, Alexander RG. Surgical
correction of the long face syndrome. AM J ORTHOD 1977;71:40-67.
Schendell SA, Eisenfeld J, Bell WH, Epker BN. Superior re-
positioning of the maxilla: stability and soft-tissue osseous re-
lations. AM J ORTHOD 1976;70:663-74. Fish LC, Wolford LM, Epker BN.
Surgical-orthodonic correction of vertical maxillary excess. AM J
ORTHOD 1978;73:241-57. Wessberg GA, Washburn MC, LaBanc JP, Epker
BN. Effect of surgical superior repositioning of the maxilla in
mandibular rest- ing posture. AM J ORTHOD 1982;81:465-72.
Reprint requests to: Dr. Varun Kalra Department of Orthodontics
University of Connecticut Health Center School of Dental Medicine
Farmington, CT 06032