Embed Size (px)
Citation preview

Physiotherapy support for children with Spina Bifida & Hydrocephalus
Bronwen Warner

• What SHINE does
• Anatomical & physiological ins and outs of spina bifida, hydrocephalus plus a couple more interesting conditions
• Discuss possible effects of conditions on child/young person
• Orthopaedic concerns
• Our role and influence on development & function
• What is effective mobility & how we can promote it
Happy to make it as practical & interactive as you like!
A loose agenda

Established in 1966, Shine is a National Charity working across England, Wales and
NI.We provide vital practical support, information and
advice on many aspects of Hydrocephalus and Spina
Bifida. SHINE offers life long assistance to enable people
to get the best out of life.
Who are we?

• Provides specialist health and education support and advice to our members to help them to better manage their conditions
• Holds regional and national groups and events• Campaigns for improved services for individuals with spina bifida and
hydrocephalus• Works with members, families, local service providers to achieve person
centred goals• Provides training and advice for professionals on the conditions • Supports with claiming benefits and signposting to other organisations • Campaigns for folic acid supplementation and fortification• Completes holistic assessment & very specific health related support in our
health hubs e.g. physio, OT, continence
What does Shine do

• Medical conditions and treatment• Diagnosis• Staying healthy & managing condition/s• Mental health• Bowel and bladder issues• Benefits, finances and funding• Education• Living independently• Folic acid and pregnancy• Relationships and social life• Local services• Local/national groups and peer support
….. And much more!
Help, advice and information on…

• 1 in 756 pregnancies are affected by a neural tube defect (NTD) such as spina bifida (source: EUROCAT, 2017).
• There is no cure for spina bifida or hydrocephalus.• Not all babies born with spina bifida have
hydrocephalus- around 80% do.
Did you know?.......

Anencephaly

• Genetic component• Family history on either side• Lack of folate/ vitamin B12- contraceptive pill depletes folate
levels and women with diabetes/ a BMI over 30/ taking certain epilepsy medication need more folate• Previous NTD pregnancy
Why does Spina Bifida occur?
Taking a 400mcg folic acid supplement every day for at least 8
weeks before falling pregnant reduces chance of NTD affected
pregnancy by up to 70%

• Gap or split in the spine• Fault in the development of the spinal cord & surrounding nerves• Neural tube fails to fully close• Congenital condition• Often diagnosed during the 20-week scan, but not always• The lower on the spine and the smaller the lesion, the less severe
the resulting impairments are likely to be
Spina Bifida

www.flipper.diff.org

Folic acid campaign: Folic for Life
• ~70% of NTDs are preventable through folic acid supplementation• 90% of UK women do not have high enough levels of folate in their
blood to protect against NTDs and ~45% of pregnancies are not planned. • ~1:750 UK pregnancies are affected by an NTD

Folic for Life - core ideas:1) Contraception isn't as effective as most people believe2) People often discover they are pregnant too late for folic acid to be of benefit3) Folic acid supplements are a cheap and easy way to reduce the chances of NTD's and improve the mothers health in the event of pregnancy

www.folicforlife.com

Types of Spina Bifida
Open spina bifida – 2 typesVisible sac/cyst on the back
Myelomeningocele• Most common and serious of the two
types of open SB • Outer part of vertebrae is split, spinal
cord & meninges are damaged and pushed out through opening
• Cyst contains tissue, CSF, nerves and part of the spinal cord
• Paralysis and loss of sensation• Bladder and bowels often affected• Hydrocephalus often associated with
this form
Edited from www.stanfordchildrens.org

Types of Spina Bifida
Open spina bifida Visible sac/cyst on the back
Meningocele• Least common type of SB• Outer part of vertebrae is split. SC is
normal but meninges are damaged & pushed out through opening
• Sac contains meninges (tissue that covers the brain and spinal cord, CSF but no spinal tissue)
• Impairment usually less severe than myelomeningocele
Edited from www.stanfordchildrens.org
Types of Spina Bifida
Closed spinal lesions
Spina bifida occulta• Outer part of vertebrae is not
completely joined• Spinal cord and meninges are
undamaged• Often hair and/or dimple at site of
defect
Edited from www.stanfordchildrens.org

Types of Spina BifidaSpina Bifida Occulta (SBO)• Effects usually appear during times of rapid growth in children or during
middle age. Very occasionally, effects are present from birth. Look out for:• Turning in of the feet ( talipes)• Back pain• ‘Growing pains’, pain, weakness or fatigue during walking• Cramp or pins and needles in the feet and legs• Thinning of the calf muscles• Numbness or lack of sensation on the skin of the feet• Bladder and/or bowel problems.
www.spinabifida.net www.ispn.guide

Types of Spina BifidaLipomyelomeningocele
• Part of the spinal cord & nerves tangles in a benign fatty tumor. Fat prevents the spinal bones from closing completely, leaving a gap
• 90% have markers on their back- fatty lumps, birthmarks, deep dimples. Often seen at birth as a skin covered lump
• 15% of cases of spina bifida.• Learning & development should follow typical
patterns• 5% of those with lipo have a condition which can
lead to hydrocephalus• Usually not detected at the antenatal scan. Brain and
skull will usually look normal so the changes to the spine may not be detected
www.sciencedirect.com
www.ispn.guide

Pop Quiz J

#2 J

#3 J

ClassificationSpinal level determined by careful examination of sensation & motor function
• Thoracic
• High level (L1 or L2)
• Mid lumbar (L3)
• Low lumbar (L4 or L5)
• Sacral
NB in predicting mobility & orthotic needs & also gives baseline to determine whether neurologic
deterioration from tethering is occurring

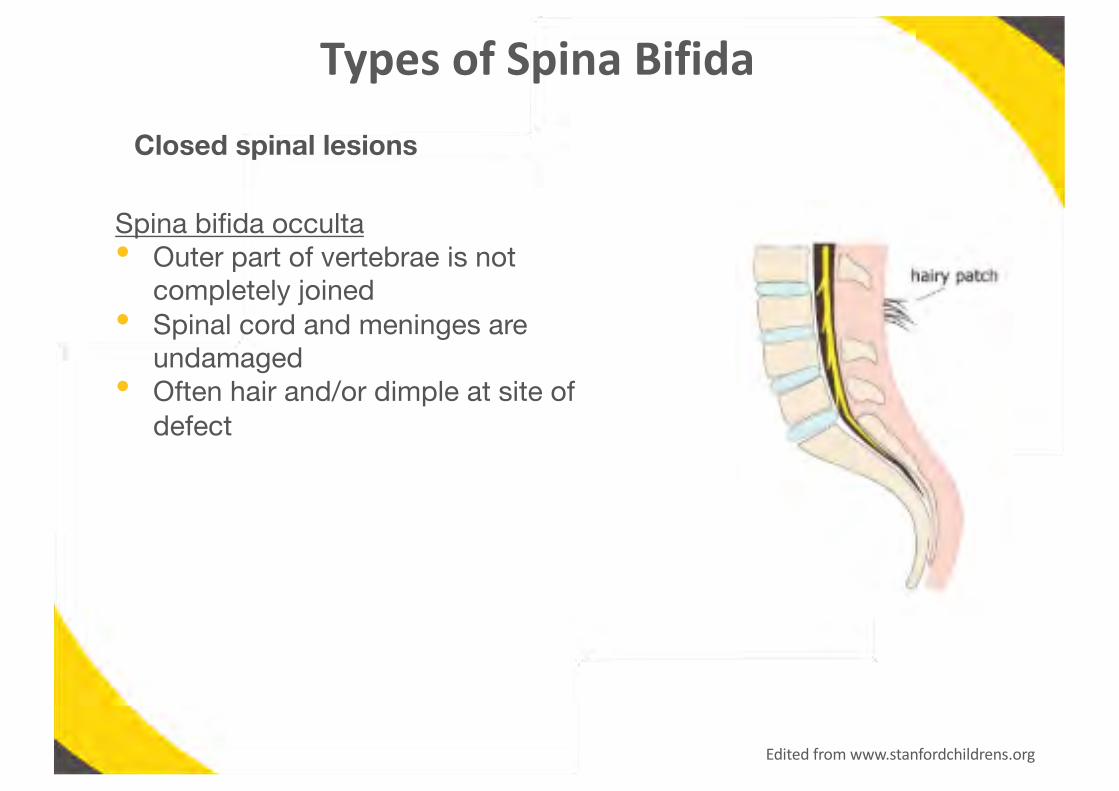
1 pair of coccygeal nerves
Muscle innervation list
JHow many pairs &
what general muscles/body parts do they innervate?
1 pair of coccygeal nerves
Muscle innervation list

1 pair of coccygeal nerves
Muscle innervation list

1 pair of coccygeal nerves
Muscle innervation list

1 pair of coccygeal nerves
Muscle innervation list

Classification of SB• Asymmetry of sensory loss or weakness is common
• Typical presentation of myelomengingocele
Thoracic • Issues with abdominals & trunk• Complete LL paralysis
L1 or L2 • May have some hip flexion & adduction but no quads strength to extend knees
L3 • May have knee flexion but paralysis of ankles & feet
L4 or L5 • Absent sensation around anus, perineum & feet• Quads strength (knee extension), some hamstring
(knee flexion) & anterior tibialis (ankle dorsiflexion)
Sacral • May have no detectable sensory loss• May have functioning glutei (hip extension) &
gastrocs (ankle plantarflexion)
Classification- GMFCSGross Motor Function Classification System
• 5 level system describing gross motor function of children & youth with CP – helpful with SB
• Looks at self – initiated movement with particular emphasis on sitting, walking & wheeled mobility
• Distinctions between levels based on functional abilities, need for assistive technology including hand held mobility devices (walkers, crutches, canes etc) or wheeled mobility
• Quality of movement much less taken into account
• Based on usual performance at home, school and in community
• 4 age bands (under 2, 2-4, 4-6, 6-12 years)

Tethered cordCan cause neurologic deterioration & why classification & careful assessment is NB
• During normal growth, spinal cord ascends within canal so conus moves from L4 to L2 between birth & puberty
• In SB, abnormal cord may be tethered to scar tissue or bony deformities leading to ischaemic damage
• Clinical signs most common 6 – 12 years and can include:
- deterioration of walking - back pain - leg pain - spasticity - increasing scoliosis - progressive foot deformity - deterioration in bladder & bowel function
*key findings: progressive weakness over time on manual testing & changes in bowel & bladder function*• Back pain typically worsened with activity & relived with rest
• Generally diagnosed on clinical grounds +/- MRI, urodynamics, electrophysiologic testing
• Surgical release of cord effectively relieves pain & may arrest neurologic deterioration

Hydrocephalus
“Water” “Head”
Types of hydrocephalus:• congenital – present at birth (e.g. spina bifida)• acquired – develops after birth (e.g. head injury, infection)• normal pressure hydrocephalus* – usually only develops in older people
*clinically distinct condition. Link relates to the brain structures and fluids involved.

What is hydrocephalus?
https://kidshealth.org/en/parents/hydrocephalus.html

Treatment for Hydrocephalus

Hydrocephalus treatments
VA shunt VP shunt
http://o.quizlet.com/Z2ObiRu02LmB4UkW2LkFtg.jpg
Endoscopic Third Ventriculostomy
http://neuros.net/en/endoscopic_ventriculostomy/
Shunts

• bulging at the soft spots• gapping between skull bones• increased head circumference• prominent veins • downward cast of the eyes (called "sunsetting")
Symptoms of hydrocephalusSigns in babies:
• nausea/vomiting (may be worse in the morning)• drowsiness• head &/or neck pain• balance problems• confusion• problems with motor skills• double-vision• squinting &/or repetitive eye movements• urinary incontinence / bowel incontinence
Signs in older children & adults:https://quizlet.com/45510950/step-2-neurology-uworld-flash-cards/
• rapidly enlarging head circumference• swelling or redness along shunt track
Signs of shunt failureSigns in babies:
• acute headache • irritability• lethargy• vomiting
Signs in young children:
Shunt malfunction signs often more subtle and insidious:- mild drowsiness- impaired attention & co – ordination

• Most people with hydrocephalus will lead “normal lives”.• Acknowledge hydrocephalus but don’t let it dominate life• Can take part in most activities and sports
• Teenagers must learn to take responsibility for shunt health• Affects everyone differently- many people with have no challenges, others will
have some challenges and some will have challenges in many areas of their life
Hydrocephalus
Challenges can include:Ø ConcentrationØ Working memoryØ Information processingØ Co-ordinationØ Organisational skillsØ Visual problemsØ Early puberty

• Often with myelomeningocele • Malformation of hindbrain & cerebellum whereby cerebellar ‘tonsils’ protrude
down into spinal cord• Usually obstructs flow of CSF – shunting in 80-90%
• Cerebellum - fine motor functions & gateway for cognitive skills involving attention, planning, learning procedures
• ??impact on balance & co – ordination / ataxia???
Arnold – Chiari II Malformation
*Red flags*May present with neck pain, progressive spasticity, ataxia
Less well known but common with myelomeningocele• Partial agenesis - parts of corpus callosum may be missingThis is the major fibre pathway connecting the 2 cerebral hemispheres so damage causes reduced communication between the 2 and significant problems with spatial & motor skills• Hydrocephalus itself has significant effects on the brain including stretching of
white matter fibres such as the corpus callosum & selective thinning of posterior brain regions associated with development of spatial skills
Other congenital brain abnormalities

• CNS changes in children with myelomeningocele are associated with problems in development of cognitive & motor skills, and behavioural difficulties that reflect the effects of these cognitive problems
• Despite the extent to which CNS is altered, few children are mentally affected or even characterised as slow learners. They typically have strengths and weaknesses in their learning profiles
• Often learning deficiencies are in more non – verbal skills including motor, perceptual – motor and visual – spatial skills.
• These non – verbal learning disabilities often tend to be associated with social problems particularly as child enters adolescence
It all impacts on the way we are ableto engage with and therefore treat and help
children and their families
Why we need to know


So how can SB affect people?
So how can SB affect people?
Mobility (typically below lesion is affected)
Bladder & Bowels
Precocious puberty
Cognition
Latex allergy
Loss of feeling in feet/legs
Sleep apnoea
Anxiety & Depression
Orthopaedic concerns (Congenital & acquired)
Impaired sexual functions
Hydrocephalus & associated complications
Seizures
Sensory processing difficulties
Pain
Skin integrity issues

Pain protects us from harmMany people with spina bifida have a loss of sensation to their legs and feet.Pressure sores are more likely to result when lack of sensation and reduced mobility are present together.Healing takes longer with reduced mobility so really NB to avoid. Damage can be from:• Shoes• Splints• Wheelchairs• BurnsChange position frequently, keep skin clean& dry, check skin frequently and treat anywounds to prevent further breakdown.
Skin care

Mobility concern – PUPIS work
- Vests- Pressure mapping- Risk mapping wrt age

Orthopaedic Issues
• Congenital deformities (present at birth)e.g. kyphosis, hemivertebrae, hip dislocation, clubfoot
• Acquired developmental deformities - related to level of involvement & caused by muscle imbalance,
paralysis, decreased sensation- iatrogenic injury such as postop tethered cord

Common Ortho Concerns• Hip deformities (contracture, subluxation, dislocation)• Knee joint problems (knee flexion or extension contracture, knee
valgus deformity, late knee instability & pain)• Rotational deformities (internal & external torsion of femur and/or
tibia – often much more of a concern in SB as reduced mobility does not naturally ‘unwind’ femoral torsion & clubfoot can increase tibial torsion))
• Clubfoot and ankle contractures• Pathologic fractures (more prevalent in people with higher level
neurological involvement due to presence of osteopaenia related to relative lack of mobility)
“The main goal of orthopaedic care ….. Is to correct deformities that may prevent the patient from using orthoses to ambulate during
childhood. In addition, the orthopaedic surgeon must monitor spinal balance & deformity & assist in monitoring the neurological status”
(2008) Neuromuscular disorders. In: Herring J (ed) Tachdjian’s pediatricorthopaedics. Saunders Elsevier, Philadelphia, pp 1405–1453

Orthoses & Equipment
Indications for use include:• Maintenance of alignment• Prevention of deformity• Correction of flexible deformity• Facilitation of independent mobility• Protection for insensate limb
Examples: scoliosis brace, HKAFO, KAFO, AFO, *with twister cables*?Use of aids to help as well incl walkers & crutchesStanding frames, specialist seating, sleep systems

J Question for you
Does/should 24 hour postural management play a role in the management plan of a child with spina bifida? • Consider the different levels discussed earlier. • How could different equipment, orthoses etc impact on specific
ortho concerns (+ve and –ve)


Movement
• The act or process of movement; Change of place or position or posture
• A particular instance or manner of moving(Merriam – Webster)

The Building Blocks of Movement
• Internal motivation - awareness/ understanding/ internal drive
• Sensory awareness- body and space awareness (proprioception)- tolerance to movement of head (vestibular)- touch - sensory motivation (visual, auditory, smell, taste cues)
• Physical skills - stages of development
We need all 3 to be effective movers & shakers!

Potential Challenges to Movement
• Internal motivation - may have difficulties with initiating movement- internal motivation sometimes decreased
• Sensory awareness- decreased or complete loss of sensation - altered body awareness - remember 8 senses
• Physical skills - muscle weakness/ complete paralysis- weight shift, balance & co – ordination challenges- medical/ orthopaedic reasons
Lots of things that can be done and people who can help toidentify, manage & overcome challenges

Physiotherapy• Helps with all 3 areas (NB don’t forget sensory please!)
• Identify ‘missing’ or weaker components
• Person and family centred goals, treatment & care plans
• Hands on therapy
• Education & advice for all involved
• Maintain alignment (24 hour postural management is NB)
• Promote independent mobility

7 Specific positions for play & strengthening
1) Prone position aka tummy time
2) Rolling & getting into sitting
3) Sitting
4) 4 – point kneeling (crawling position)
5) Kneeling
6) Half – kneeling
7) Standing

Always #1: Prone position aka tummy time

Rolling & getting into sitting• All about transitions
• Rotation is key for movement & 3 dimensional view of world
• Vital component of sensory development
• Often just takes some ‘roll – playing’! **hydroceph babies especially

Sitting• Different types with different effects• Want rotation & ability to move out of base of
support• Long sitting very useful for hamstring stretch• Side sitting for weight shift, UL weight bearing,
transition posture

4 – point/crawling position• Pre-cursor for crawling (bilateral co-ordination, fine motor skills)• Strengthens core, shoulder & hip complexes• Weight bearing (joint development), weight shifting (balance)

Kneeling
• Weight bearing through hip joints• Strengthens core • Hip co-contraction (glutes++)• Weight through arms• Weight shift & balance
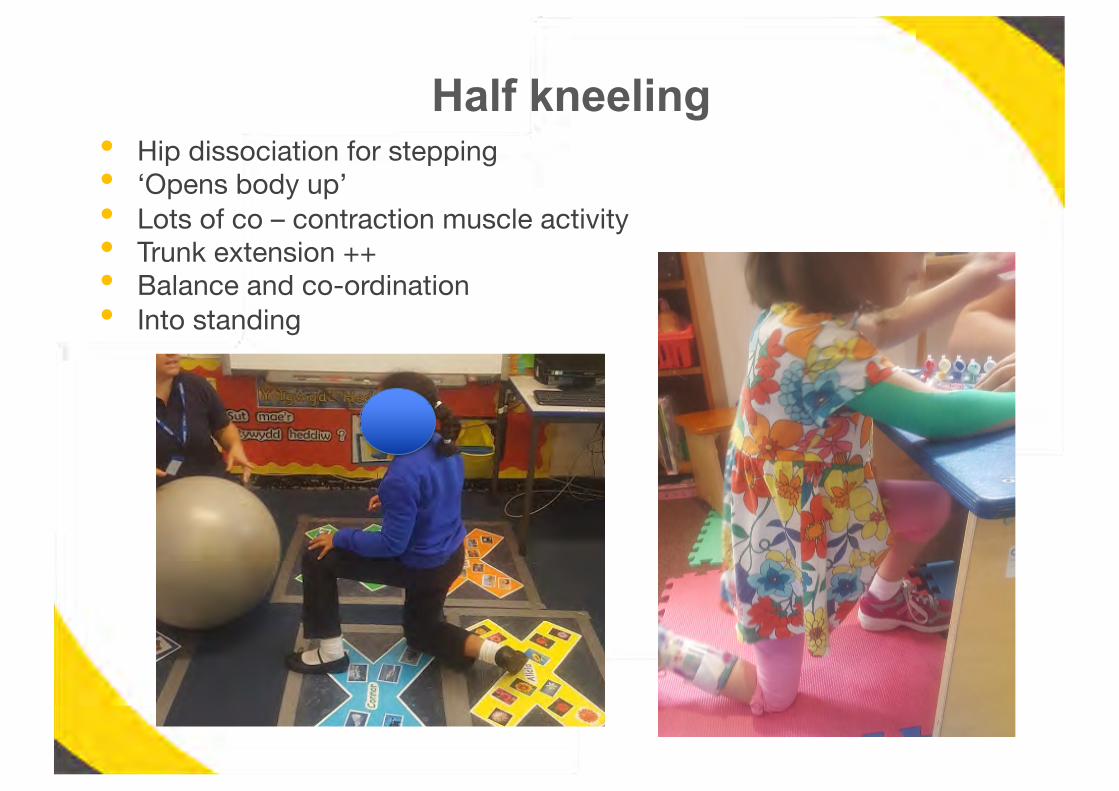
Half kneeling• Hip dissociation for stepping• ‘Opens body up’• Lots of co – contraction muscle activity• Trunk extension ++• Balance and co-ordination • Into standing

Standing
• Supported to independent (perch, leaning with hands etc)• Sit to stand important • Change variables like stance, step, weight shift, surface etc)• Squatting • Dynamic vs static activity• Use aids as appropriate (splints, standing frames, sticks etc)
Top issues
• Weak anti – gravity extensor muscles • Followed closely by weak abdominals = hinging spine• Tight hamstrings• Proactive prevention of hip dislocations and spinal
deformity• Concerns with foot splints• High functioning/independently mobile kids needing fine –
tuning e.g. end range quad strengthening, hamstring tightening with growth spurts, eversion/dorsiflexion work, single leg standing for better balance etc
? Thoughts on….??
- soft tissue work (massage)- abduction standers- early standing (12 months)- AFO provision

Top issuesPLEASE PROMOTE EARLY MOBILITY
• Prone on scooter boards • Small mobility devices e.g. scooot from firefly, whizzybug
Please consider
- Cognition often typical for age- Not affected by tone like with CP - Need to become aware of legs if affected by sensory loss- What’s learnt in early years will be for life
TRANSITIONS AND TRANSFERS PLEASE


Movement & the potential costs
How did you travel here today?
• Energy expenditure
• Speed
• Exhaustion

Costs of walking
• People walk at a speed that is most efficient in terms of energy expenditure. To maintain this level, persons with disabilities move more slowly
• The more abnormal the gait pattern, the greater the energy expenditure & the slower the speed
• Using aids greatly increases energy expenditure & slows speed• Any aid that increases effort is likely to be abandoned• Wheelchairs allow travel at speed comparable to that of
unimpaired walkers with equivalent energy expenditure

Costs of walking
• When prolonged exercise is performed at more than 50% of individuals max aerobic capacity, available O2 is insufficient to meet energy demands of muscles & activity cannot be sustained without exhaustion
- Children with thoracic & upper lumbar lesions walking without aids = max aerobic capacity
- Lower lumbar lesions = 85% compared with unimpaired walkers 30%
- Walking with myelomeningocele twice as strenuous as propelling chair
- Average speed of free walking (26m/minute) much slower than peers (69 – 73m/minute)

Costs of walking
• In unimpaired people, rate of energy expenditure decreases with age while aerobic & physical working capacities increase. Opposite is true for children with abnormal gait – their rate of energy expenditure increases while aerobic & physical working capacities decrease…..
…….. The child or teenager who complains of fatigue or difficulty with keeping up is not ‘lazy’. They are experiencing extreme physical exertion
• Think about what it means for both individual and family to go from walking to wheelchair at later stage

Costs of walking
• Exercise induced fatigue has significant impact on child- classroom performance suffers (risk increases with accelerated growth, large school grounds, students moving throughout day)- heart rate increases - significant decline in visual - motor performance test measures(these both improved in study with wheelchair use)
• these risks are in addition to already identified problems with cognitive skills, visual – perceptual problems etc that we talked about earlier
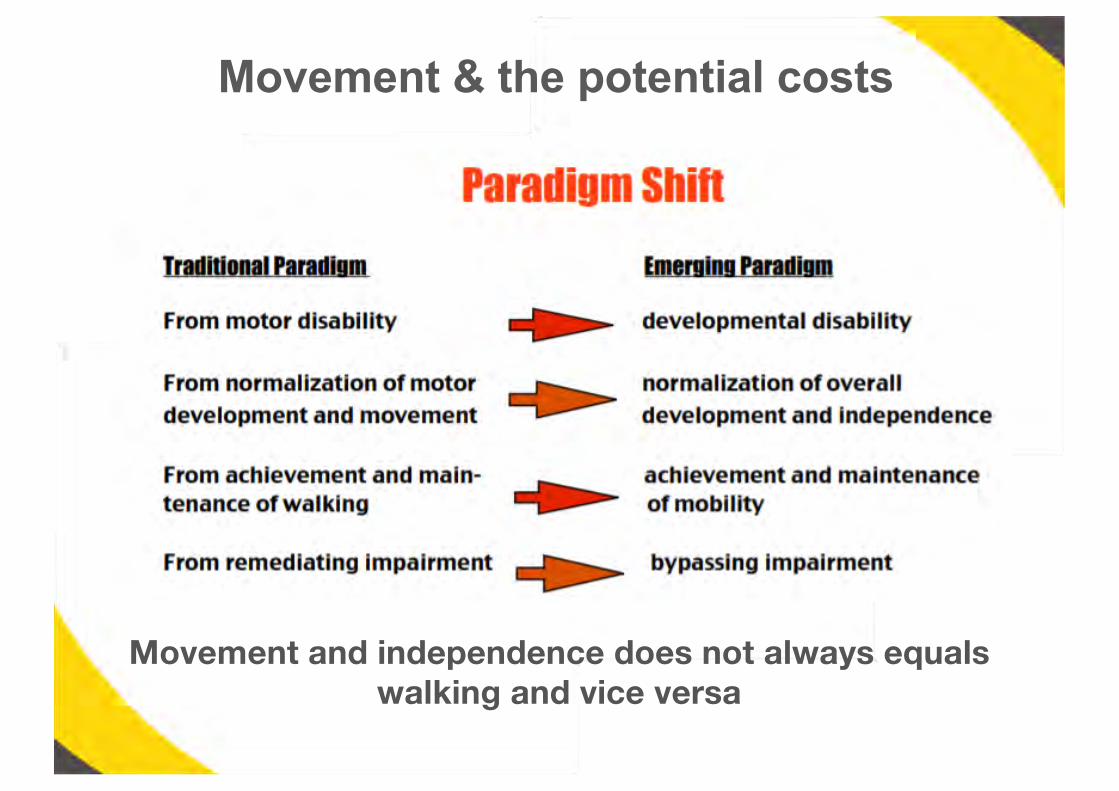
Movement & the potential costs
Movement and independence does not always equals walking and vice versa
• Provide opportunity for development in all areas which are reliant on each other • Mobility is key - through motor skills, very young children learn about
things and people in their world – they cause things to happen. • Become initiators rather than passive recipients of experience, in turn
promoting development of attention, motivation and intelligence • When motor skills are restricted, all areas of child development are at
risk
Purpose of Mobility

• Widen motor independence• Reduce excessive energy expenditure• Avoid early physiological burnout• Reduce risk of joint deterioration and pain
Purpose of Mobility Devices

Thank you for your attention!
Any Questions?


![Neuropsychology and Spina Bifida [Read-Only]spinabifidant.org/wp-content/...Full-Neuropsychology-and-Spina-Bifida.pdf · NEUROPSYCHOLOGY AND THE PSYCHOLOGICAL ASPECTS OF SPINA BIFIDA](https://img.pdfslide.us/doc/110x75/5d59960688c9933d7a8b8165/neuropsychology-and-spina-bifida-read-only-neuropsychology-and-the-psychological.jpg)